
Abstract
The current study quasi-experimentally assessed the outcome of high-intensity inpatient sex offender treatment in the Netherlands in terms of sexual and violent (including sexual) recidivism. It was hypothesized that treated sex offenders would show lower recidivism rates than untreated sex offenders of the same risk level. In line with the risk principle of the Risk, Need, Responsivity (RNR) model, we predicted that this would especially hold true for offenders of higher risk levels. The study sample consisted of 25% of all convicted Dutch sex offenders not referred to any form of treatment and discharged from prison between 1996 and 2002, and all convicted Dutch sex offenders referred to inpatient treatment who were discharged between 1996 and 2002. Static-99R risk levels of these 266 offenders were retrospectively assessed and survival curves regarding sexual and violent (including sexual) recidivism were compared between treated and untreated offenders, controlling for level of risk. Mean follow-up was 148.0 months (SD = 29.6) and the base rate of sexual recidivism was 15.0% and 38.4% for violent (including sexual) recidivism. Cox regression survival analyses showed marginally significant lower failure rates regarding sexual recidivism for treated high-risk offenders only, and significantly lower failure rates regarding violent (including sexual recidivism) for treated sex offenders of moderate-high and high-risk levels. No treatment effects for low and low-moderate risk offenders were found. Results underscore the risk principle of the RNR model: Treatment is more effective when its dosage is attuned to risk level.
The effectiveness of sex offender treatment is subject to ongoing debate (Furby, Weinrott, & Blackshaw, 1989; Gallagher, Wilson, Hirschfield, Coggeshall, & MacKenzie, 1999; Hall, 1995; Hanson, Bourgon, Helmus, & Hodgson, 2009; Hanson et al., 2002; Harris, Rice, & Quinsey, 1998; Kenworthy, Adams, Brooks-Gordon, & Fenton, 2004; Lösel & Schmucker, 2005; Rice & Harris, 2003). Conclusions derived from systematic reviews and meta-analyses about the effectiveness of treatment for sex offenders appear to be contingent on their respective inclusion criteria: Those limited to randomized studies tend to conclude that there is insufficient evidence for treatment efficacy (e.g., Kenworthy et al., 2004; Rice & Harris, 2003), whereas those with wider inclusion criteria tend to conclude that treatment does exert a positive effect (e.g., Hanson et al., 2002; Lösel & Schmucker, 2005). The most recent meta-analysis (Hanson et al., 2009) was based on 23 recidivism outcome studies meeting the basic criteria for study quality as defined in the guidelines of the Collaborative Outcome Data Committee (CODC; 2007a, 2007b), rejecting 81% of all available studies but not limiting analysis to randomized studies. Results showed significantly lower sexual recidivism rates (10.9% vs. 19.2%) for treated offenders, but not significantly lower violent (including sexual) recidivism rates (22.9% vs. 32.0%). More importantly, however, Hanson et al. (2009) found that the Risk, Need, Responsivity (RNR 1 ) principles of effective correctional treatment (Andrews, Bonta, & Hoge, 1990; Bonta & Andrews, 2007) likewise apply to sex offenders. In addition, only treatment programs adhering to all three RNR principles showed substantial and significant reduction in recidivism, consistent over all included outcome measures (sexual, violent including sexual, and any recidivism).
In keeping with the risk principle, these results imply that the largest treatment effect is to be expected from (adequate) treatment of high-risk sex offenders. A recent study from Olver, Nicholaichuk, Gu, and Wong (2013) supported that notion as they compared treatment effects for a national cohort of Canadian federally incarcerated sex offenders of various risk levels and found a significant reduction in recidivism only in the subgroups of moderate and high-risk offenders but not for low risk offenders. An earlier study (Hanson, Broom, & Stephenson, 2004) found no treatment effect even after controlling for risk level. Neither study used the Static-99(R) but instead relied on specifically constructed static scales to control for differences in risk level. The reported mean risk scores suggest that the sample of the Hanson et al. study was of a considerably lower risk level (M = 1.7, out of a possible 10) than the Olver et al. study (M = 1.9, out of a possible 5). Overall, findings indicate that evaluation of the treatment of high-risk sex offenders is specifically essential in the debate on treatment efficacy.
While randomized effect studies are the gold standard for treatment evaluation, their specific use for sex offender treatment evaluation has been disputed (Marshall & Marshall, 2007). Most importantly, randomization is not always practically feasible; for example, when it would involve the deliberate release into society of untreated sex offenders at risk to reoffend, and even more so when the studied offenders are considered at high risk to reoffend. If randomization is not feasible, researchers are encouraged to use the CODC guidelines to achieve acceptable study quality without randomization (CODC, 2007a; Hanson et al., 2009). The CODC guidelines specifically stress the importance of taking into account four factors when conducting a non-randomized evaluation: (a) risk levels (by scoring actuarial measures for all subjects), (b) dropouts (by reporting intent-to-treat analysis), (c) follow-up time (by using fixed follow-up periods or survival analysis), and (d) potential confounding variables (by controlling statistically).
The current study, while aiming to adhere to the CODC guidelines, takes a quasi-experimental approach to the evaluation of inpatient sex offender treatment in the Netherlands, specifically targeted to high-risk sex offenders in terms of sexual and violent (including sexual) recidivism. It was hypothesized that the offenders discharged from this treatment would show significantly lower recidivism rates than untreated sex offenders of the same actuarial risk levels. In addition, in keeping with the RNR principles and mindful of the high intensity of the provided treatment, larger treatment effects were expected for offenders with higher actuarial risk scores.
Method
Participants
The study sample consisted of two subsamples of men convicted for a contact sexual offense in the Netherlands. The first subsample included all offenders who were discharged from high-intensity inpatient treatment between 1996 and 2002 (n = 106). The second subsample consisted of a random selection of 25% of adult male sex offenders who were discharged from prison between 1996 and 2002, without being referred to any form of treatment (n = 188). This subsample was obtained by selecting half of all Dutch jurisdictions, stratified for urban and rural areas, and subsequently randomly selecting half of the obtainable files from each selected jurisdiction. Both samples added up to a total of 294 sex offenders. These subsamples correspond to the inpatient and no treatment subsamples as described in Smid, Kamphuis, Wever and Van Beek (2014) and overlap with the inpatient and no treatment subsamples described in Smid, Kamphuis, Wever, and Van Beek (2013).
A total of 28 records were discarded for a diversity of reasons: Six offenders deceased before discharge, two (illegal immigrant) offenders were extradited directly after discharge, and six offenders were not actually discharged but left the treatment facility to return to prison as result of a new conviction. For 14 offenders (five inpatients and nine prisoners), we were unable to find a new extract of criminal records to assess new offenses; 12 of those deceased before 2006, and their record was deleted from the judicial system, as was customary up to that date. Follow-up data for the two remaining offenders was missing for unknown reasons. This resulted in a final sample of 266 offenders who were included in the subsequent analyses, 34% discharged inpatients (n = 90) and 66% discharged from prison (n = 176). The mean age at discharge for the total sample was 37.48 (SD = 11.74), with a minimum age of 18 and a maximum age of 78. Of all offenders, 70.3% (n = 187) had a prior criminal charge/conviction (n = 167) and 28.9% (n = 77) had a previous charge/conviction for a sexual offense. The mean Static-99R score of the total sample was 3.20 (SD = 2.46). The distribution of offenders over Static-99R risk levels differed significantly between the two subgroups, χ2(3, N = 266) = 39.74, p < .001, with inpatient offenders more often showing moderate-high and high-risk levels and untreated offenders more often showing low-moderate and low-risk levels (see Table 1). On average, higher risk offenders were selected for inpatient treatment, but offenders of all risk levels were present in both groups. No cells showed an expected count of less than 5 and only one cell (low-risk inpatient treatment) showed an observed count (9) below the minimum expected count (15.2).
Static-99R Risk Levels Compared Between Untreated and Inpatient Sex Offenders.
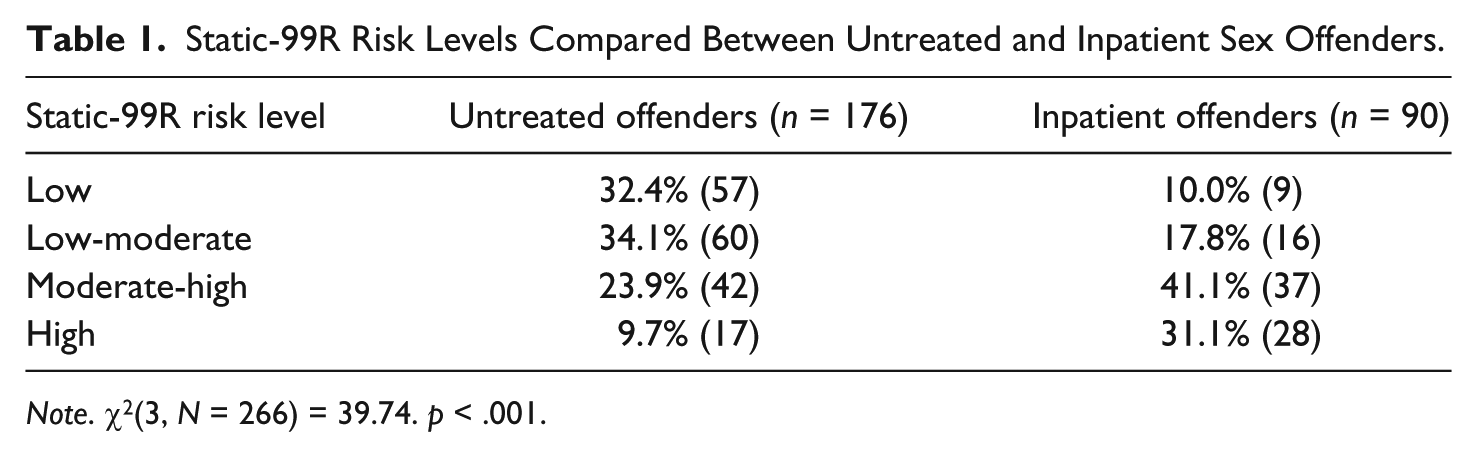
Note. χ2(3, N = 266) = 39.74. p < .001.
Setting
Pretrial psychological assessment for sex offenders is not a standard procedure in the Netherlands. Instead, judges can order discretionary psychological assessment by an independent psychologist or psychiatrist (or both). In approximately 5% of all sex offender convictions, a consulted examiner advises the court to refer a sex offender to mandatory inpatient treatment (Brouwers & Smit, 2005). This form of treatment is referred to as “ter beschikking stelling” (TBS) which translates as “put at the disposition of the government” meaning the treatment is imposed by the state for as long as the state sees fit. This treatment was primarily designed to protect society against reoffending and is imposed on offenders who are considered to be at serious risk to reoffend. It is of indefinite length, but each individual case is reevaluated in court every two years. Though treatment was intended to end when treatment providers determine that the offender has made sufficient progress, judges regularly decide to end treatment against the advice of the treatment providers: the so-called “contrarian rulings.”
The referral of sex offenders to this and other forms of treatment has for the longest time been guided by unstructured clinical procedures. Prior research has shown that this practice resulted in a situation in which sex offenders, irrespective of their actuarial risk levels, were referred to inpatient treatment, or to prison without any form of treatment (Smid et al., 2013). This indiscriminate treatment allocation provided the opportunity to compare the recidivism rates of released inpatients with untreated offenders of comparable actuarial risk levels (consistent with the CODC guideline to take risk levels into account). Offenders who were discharged based on contrarian rulings can be regarded as dropouts, and prior research has shown these offenders to be at considerably higher risk to reoffend than those who completed treatment (De Vogel, De Ruiter, Hildebrand, Bos, & Van de Ven, 2004). These dropouts were included in the treatment group to provide intention-to-treat analysis, consistent with the CODC guideline to take into account dropouts. The prematurely discharged offenders constituted 45% of all discharged offenders, and their treatment duration (M = 91.87 months, SD = 38.53) did not differ significantly from the regularly discharged offenders (M = 104.83 months, SD = 42.12, t = 1.42, p = .16).
The six offenders who recidivated during treatment and were reincarcerated during the time frame of the current study were excluded from this study sample because they had not been discharged yet, and thus fell out of our sample frame. Of note, the data in this study included all offenders who were discharged between 1996 and 2002, as opposed to offenders who were convicted during that time frame. Although their recidivism could clearly be regarded as a form of treatment failure, their inclusion would also have required the inclusion of all offenders still in treatment who did not recidivate during treatment, which was beyond the scope and frame of this study. Generally, offenders who recidivated during inpatient treatment would return to treatment after their reconviction and any served prison time. Accordingly, our sample did include seven offenders who recidivated during treatment, returned to treatment, and were eventually discharged between 1996 and 2002. The mean Static-99R scores of the six excluded non-discharged inpatient offenders was very similar to the Static-99R scores of the seven included discharged inpatient offenders who had recidivated during an earlier stage of treatment, M = 6.17 (SD = 0.98) versus M = 6.14 (SD = 2.12), p = .98.
Procedure
Participants’ criminal files, as compiled by the legal system for their index conviction (index files), were studied to retrospectively code the items of the Static-99R. The index files generally contained offenders’ criminal record at the time of conviction, 2 minutes concerning the index offense (with statements of both offenders and victims), and the exact indictment, verdict, and sentence, including any imposed treatment measures. The majority (69.9%) of the files contained a report concerning some sort of pretrial assessment (100% of the inpatient files and 55.1% of the prisoner files). All assessments were unstructured, and none of the offenders was assessed for risk level with an actuarial instrument at the time of conviction. A total of 10 trained coders scored the items based on the file information in the 266 files. The age-related Static-99R item was scored according to the offenders’ age at the time of discharge.
After the coding of the Static-99R, the offenders’ current criminal records were requested to acquire data on their reoffending. The current criminal records were coded by two independent raters who were blind to the initial risk assessment results. The outcome measure “sexual recidivism” was defined as any charge or conviction for a new offense that was sexual in name (e.g., rape, abuse, child pornography possession). “Violent recidivism” was defined as any charge or conviction for a new offense that involved any actual, attempted, or threatened physical harm to the victim and included all sexual offenses. Violent offenses included explicit display of violence, such as assault, murder, or robbery, and also included more covert forms of violence, such as threats, extortion, and stalking. Follow-up time was counted from the day of discharge to the day that the follow-up criminal record was retrieved, or, in case of deceased subjects, from the date of discharge to the date of death.
To test whether the quasi-experimental design resulted in comparable groups, demographic and clinical characteristics were compared between the treated and untreated offenders at each of the four risk levels, consistent with the CODC guideline to take into account potential confounding variables. Some demographic and legal variables were assessable for all subjects, that is, offender age, number of children, education level, relationship history, employment, ethnicity, prison sentence, and age of victim(s). Other, more psychological variables were only available for offenders with pretrial assessment reports, that is, for all of the treated offenders and for 55% (n = 97) of the untreated offenders. In these cases, more extensive information was documented and the reporting social worker, psychologist, or psychiatrist generally assessed more psychological information. The included variables were coded according to recorded statements of the offender or assessment by the reporter. These variables included general cognitive ability (e.g., mention of mental retardation); sexual orientation toward adults; mention of any major mental disorder, current or in the past; mention of any personality disorder (PD) or traits of PD; mention of substance abuse; mention of prior psychological/psychiatric treatment; and mention of childhood abuse.
Treatment
The Dutch mandatory inpatient sex offender treatment was provided after completion of any prison sentence by several Dutch health care facilities. These facilities, although closed, were not prison-like, and treatment was delivered in a generally supportive non-punishing atmosphere. Specific treatment programs varied among the 13 different facilities providing this treatment, but always included psychotherapy (individual, in groups, or both), most often a relapse prevention program, and adjunctive job/study orientation and pharmacotherapy when indicated. No treatment differentiation was made according to risk levels, but treatment was extensively tailored to the offenders’ individual responsivity. Treatment targets included the established criminogenic need factors (e.g., antisocial attitudes, offense supportive attitudes, substance abuse), as well as other factors not directly linked to recidivism risk (e.g., major mental disorder, empathy, social skills). The average treatment duration for the offenders included in the study sample was 8 years and 4 months (SD = 42.6 months). This duration refers to the total time they spent in and under supervision of the TBS clinic; this period involved participation in coordinated sex offender programming as well as participation in more general treatment-relevant programs. During the course of the treatment, the offenders progressively gained more extended forms of leave. For most offenders, their resocialization included a so-called “transmural” phase (halfway houses), when they were living outside the facility while still under supervision. Some offenders were transferred between facilities during treatment. For a more detailed description of TBS treatment, see Feldbrugge (2007). For an example of a treatment program of a specific treatment facility, see Van Binsbergen, Keune, Gerrits, and Wiertsma (2007).
Instruments
The Static-99 (Hanson & Thornton, 2000) is the most widely used and most extensively researched actuarial risk assessment instrument for sex offenders (Hanson & Morton-Bourgon, 2009). It consists of 10 items yielding a score between “0” and “12,” referring to four risk levels. The most recent meta-analysis (Hanson & Morton-Bourgon, 2009) summarized 63 findings from published and unpublished studies that included more than 20,000 subjects: A median Cohen’s d = .74 (mean d = .67) for sexual recidivism and a median Cohen’s d = .51 (mean d = .57) for any violent (including sexual) recidivism were observed. Recent research found age to add incrementally to the predictive validity of the Static-99, resulting in a revised scoring system (Helmus, Thornton, Hanson, & Babchishin, 2012). The Static-99R age item distinguishes four age categories yielding a score between “–3” and “+1.” Total scores of the Static-99R range between −3 and +13, referring to four risk levels: low (−3 to +1), low-moderate (2 or 3), moderate-high (4 or 5), or high (6 or higher). The Static-99R significantly predicted sexual and violent (including sexual) recidivism for a national Dutch sex offender sample (Smid et al., 2014), which the current sample is a subgroup of; Static-99R area under the curve (AUC) values varied between .71 and .74 for the various follow-up periods and outcome measures. In the current sample, the Static-99R predicted both sexual (AUC = .78) and violent (including sexual) recidivism (AUC = .73) significantly over a 10-year fixed follow-up period. For the subgroup of untreated offenders, the respective AUC values for sexual and violent (including sexual) recidivism were .83 and .78. For the subgroup of inpatient offenders, the AUC values for sexual and violent (including sexual) recidivism were .66 and .71. An earlier study also found lower predictive accuracy of static risk factors regarding treated offenders (Langton et al., 2007), indicating that treatment may render some static risk factors less valid.
Statistical Analysis
First, to assess baseline differences between the treatment and no-treatment group, comparisons of characteristics were conducted at each Static-99R risk level separately, by means of t test for the age-related variables, Mann−Whitney U tests for the ordinal variables, and chi-square analyses for categorical variables. No Bonferroni corrections were applied, as we aimed to conduct a stringent test of equivalence. Second, to assess their relationship to recidivism, variables showing significant a priori differences between the treated and untreated offenders were entered in a Cox regression survival analysis, with both risk level and treatment as covariates.
Third, Cox regression survival analyses were used to compare sexual and violent (including sexual) recidivism rates of treated and untreated offenders, while controlling for Static-99R score and individual differences in follow-up time (consistent with the CODC guideline to take into account follow-up time). Survival time was defined as the time between the date of discharge from treatment or prison to the date of perpetration of the first sexual or violent (including sexual) reoffense. If no new sexual or violent reoffense occurred, survival time was calculated as the time between discharge date and the retrieval date of the new criminal record, or date of death when indicated. To control for risk level, the Static-99R total score was included as a covariate. Seven offenders recidivated with a violent offense before they recidivated with a sexual offense, and their survival time for sexual recidivism was adjusted for the estimated time spent in prison for the earlier violent offense.
Finally, to assess differences in recidivism rates between treated and untreated offenders at each risk level, Cox regression survival analyses were conducted for each outcome measure including treated and untreated offenders stratified by the four Static-99R risk levels (low, low-moderate, moderate-high, and high).
Results
Mean follow-up in the total sample was 148.0 months (12 years and 4 months, SD = 29.6 months), with a minimum of 51 months (4 years and 3 months) and a maximum of 201 months (16 years and 9 months). The base rate for sexual recidivism was 15.0% and 38.4% for violent (including sexual) recidivism.
Analyses yielded few significant a priori differences between offenders of the same risk levels across treatment groups (see Tables 2 and 3). High-risk inpatient offenders were significantly younger at the time of conviction, t(43) = 3.72, p = .001, whereas low-moderate, t(74) = 2.26, p < .03, and moderate-high, t(77) = 5.17, p < .001, offenders were significantly older at the time of discharge. Moreover, untreated moderate-high, χ2(1, N = 79) = 23.85, p < .001, and high-risk, χ2 (1, N = 45) = 7.99, p < .01, offenders were significantly more often of non-European descent.
Demographic Variables Compared Between Untreated and Inpatient Sex Offenders at Each Static-99R Risk Level.
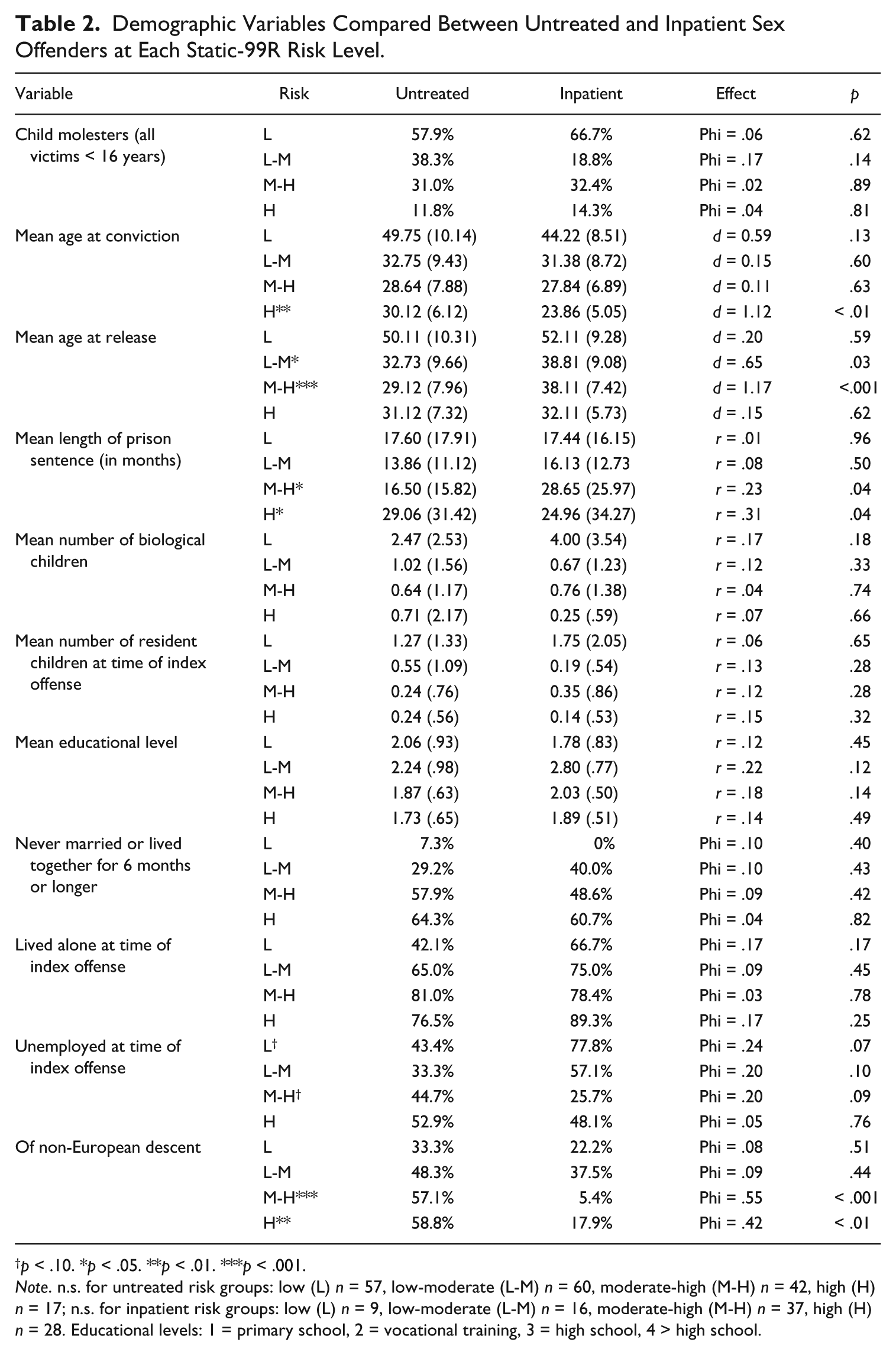
p < .10. *p < .05. **p < .01. ***p < .001.
Note. n.s. for untreated risk groups: low (L) n = 57, low-moderate (L-M) n = 60, moderate-high (M-H) n = 42, high (H) n = 17; n.s. for inpatient risk groups: low (L) n = 9, low-moderate (L-M) n = 16, moderate-high (M-H) n = 37, high (H) n = 28. Educational levels: 1 = primary school, 2 = vocational training, 3 = high school, 4 > high school.
Psychological Variables Compared Between Untreated and Inpatient Sex Offenders at Each Static-99R Risk Level.

p < .01.
Note. n.s. for untreated risk groups: low (L) n = 49, low-moderate (L-M) n = 50, moderate-high (M-H) n = 35, high (H) n = 14; n.s. for inpatient risk groups: low (L) n = 9, low-moderate (L-M) n = 16, moderate-high (M-H) n = 37, high (H) n = 28.
Cox regression survival analysis, controlling for risk level and treatment, showed no significant effects on sexual recidivism or violent (including sexual) recidivism for either age at conviction, age at release, or ethnicity (see Tables 4 and 5).
Cox Regression Survival Analysis: Sex Offender Treatment Outcome for Sexual Recidivism Controlling for Static-99R Total Score, Age, and Ethnicity (N = 266).

Note. CI = confidence interval.
p < .001.
Cox Regression Survival Analysis: Sex Offender Treatment Outcome for Violent (Including Sexual) Recidivism Controlling for Static-99R Total Score, Age, and Ethnicity (N = 266).
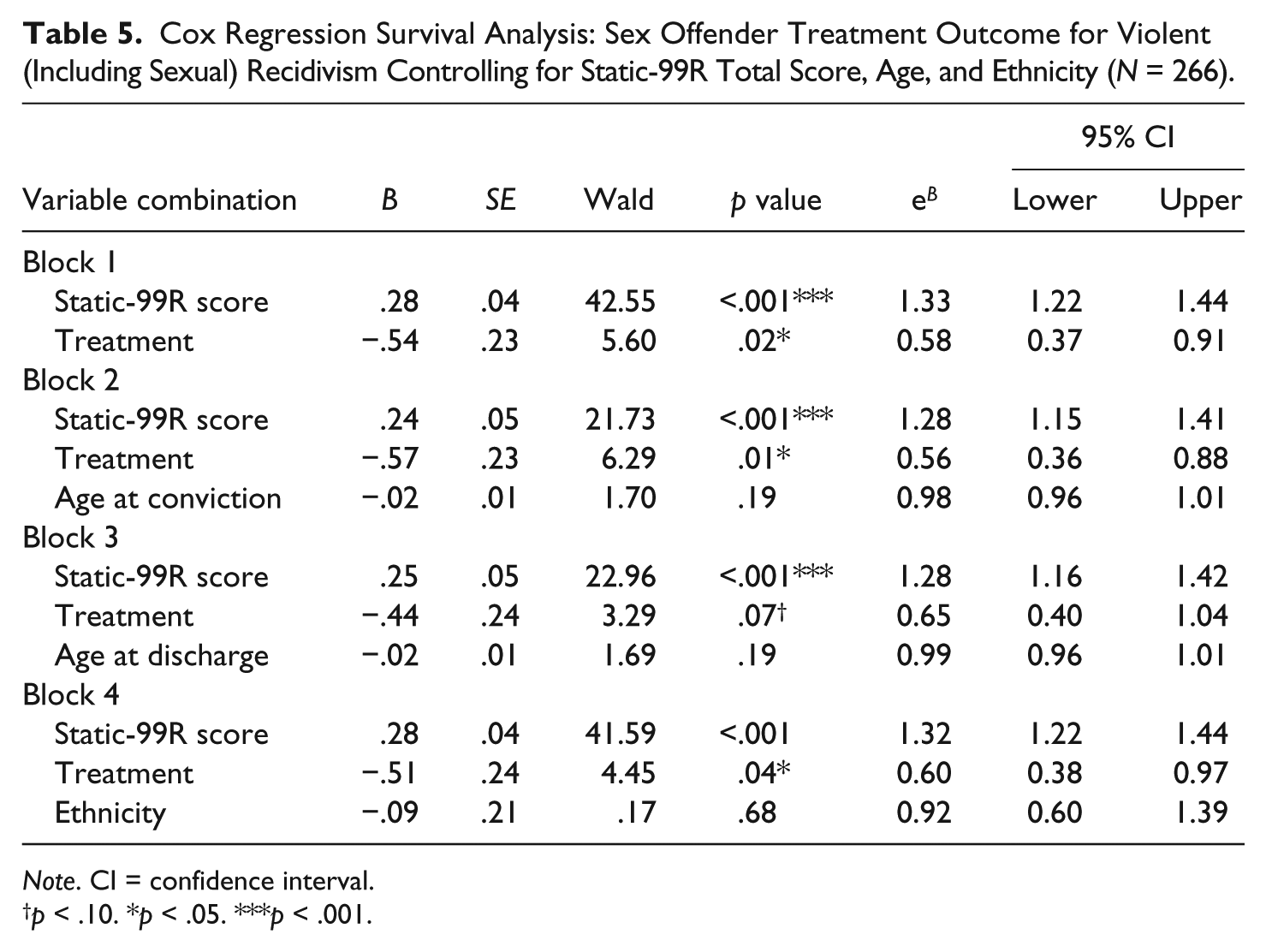
Note. CI = confidence interval.
p < .10. *p < .05. ***p < .001.
Regarding sexual recidivism, Cox regression survival analysis showed that, controlling for the Static-99R total score, treated sex offenders did not significantly differ from untreated sex offenders in terms of recidivism (see Table 4). Stratified by the four Static-99R risk levels however, treated high-risk offenders recidivated at a marginally significant lower rate than their untreated counterparts (B = −.88, SE = .45, Wald = 3.79, p = .05). No significant differences were found at the low, low-moderate, and moderate-high risk levels (see Figure 1).
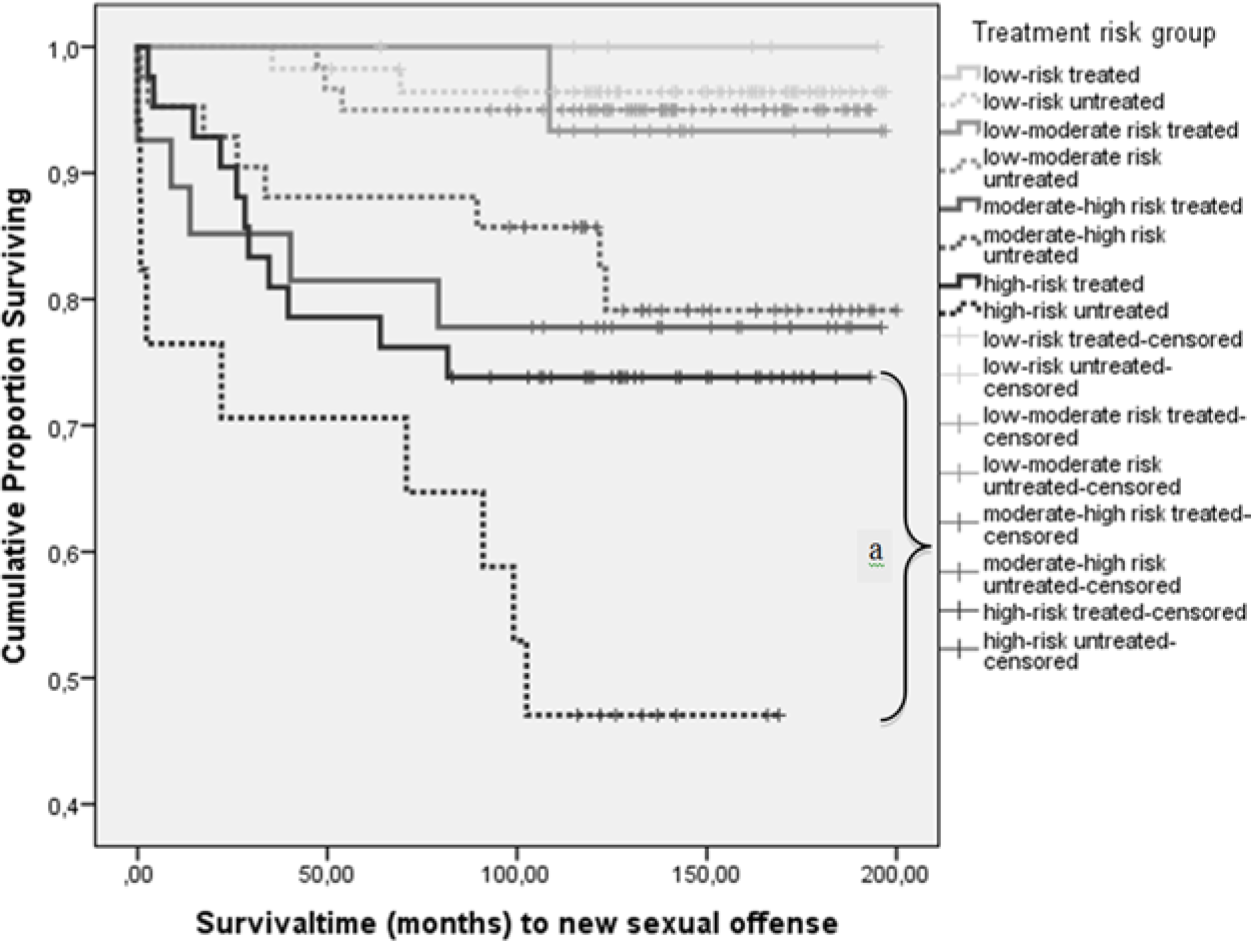
Survival analysis: Sexual recidivism failure rates among treated and untreated sex offenders as a function of Static-99R risk level (low, low-moderate, moderate-high, high).
Regarding violent (including sexual) recidivism, Cox regression survival analysis showed that, controlling for the Static-99R total score, treated sex offenders recidivated at a significantly lower rate than untreated sex offenders (see Table 5). Stratified by the four Static-99R risk levels, treated moderate-high (B = −.86, SE = .39, Wald = 4.84, p = .03) and high-risk sex offenders (B = −.76, SE = .35, Wald = 4.70, p = .03) recidivated at a significantly lower rate than their untreated counterparts, while no significant differences were found at the low and low-moderate risk levels (see Figure 2).
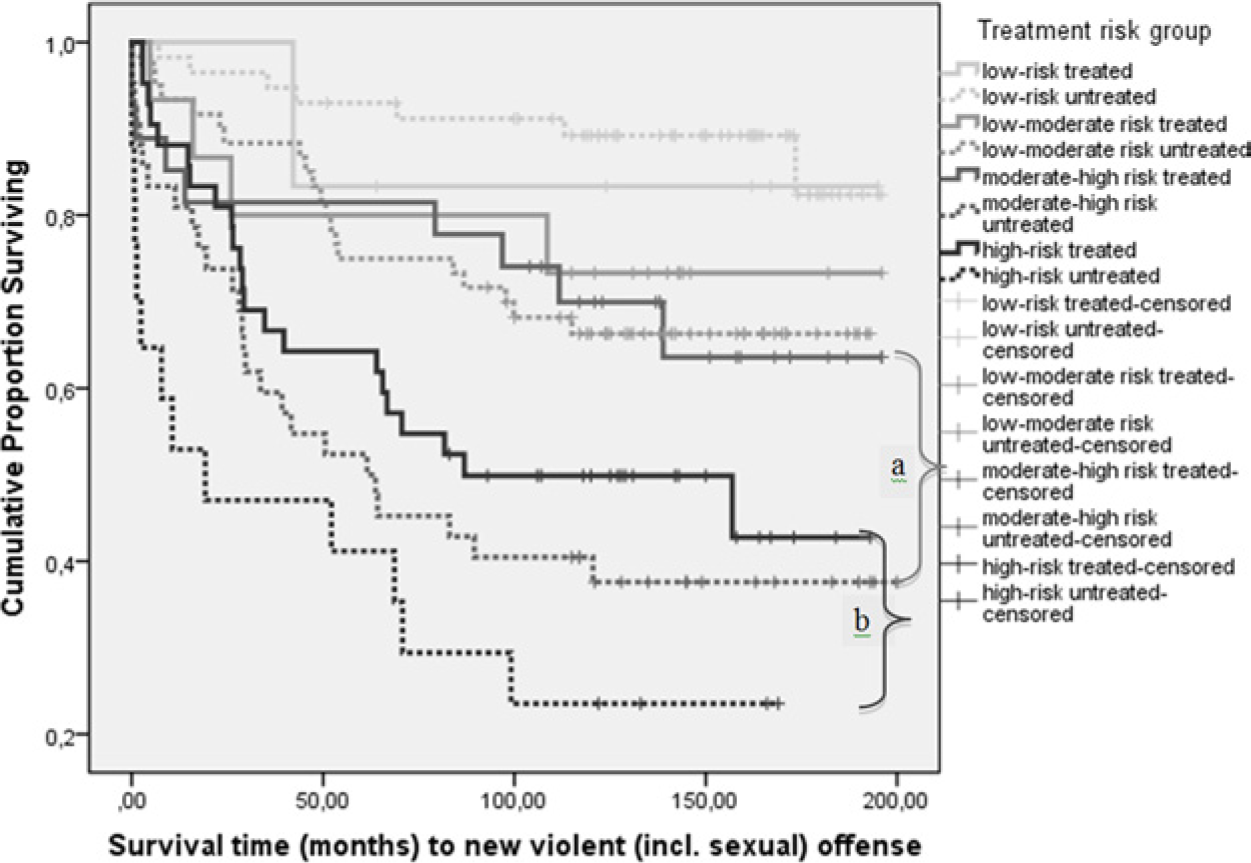
Survival analysis: Violent (including sexual) recidivism failure rates among treated and untreated sex offenders a function of Static-99R risk level (low, low-moderate, moderate-high, high).
Discussion
The current study quasi-experimentally assessed the effect of high-intensity inpatient treatment for sex offenders. The base rate for sexual reoffending was relatively low (15.0%), which may have impeded the power to detect differences between treated and untreated sex offenders. Only among high-risk offenders, for whom recidivism was more common (40.0%), a marginally significant treatment effect was found. We observed a significant effect of treatment on the more prevalent violent (including sexual) reoffending, especially for the moderate-high and high-risk offenders. These results are similar to recent research among Canadian federally incarcerated sex offenders (Olver et al., 2013) and again underscore the risk principle of the RNR model: Treatment is most effective when treatment levels are attuned to risk levels.
In contrast to treatment efficacy studies on non-sexual offenders but again in line with Olver’s findings (Olver et al., 2013) in incarcerated sex offenders, we did not find higher recidivism rates for (over)treated low risk offenders, (Bonta, Wallace-Capretta, & Rooney, 2000; Lowenkamp & Latessa, 2002). A possible explanation for these inconsistent findings is that the non-sexual offender studies included general recidivism as outcome measure (reconviction, arrest, incarceration for any offense), while both Olver et al. and the current study only included sexual and/or violent recidivism as outcome measure. This type of recidivism has a lower base rate in general, and even more so among low risk offenders, which renders effects among low risk offenders hard to detect. To date however, results seem to indicate that the effect of “overtreatment” does not apply to sex offenders with regard to sexual or violent (including sexual) recidivism. On the other hand, it should be noted that no clear positive effect of treatment was noted either, and (intensive) treatment for low risk offenders implies suboptimal use of resources. Overall, our results should be interpreted with caution, keeping in mind the limitations of the quasi-experimental design, and the modest power to detect differences in the subsamples after the stratification. Cross validation in larger samples is clearly indicated.
Second, the quasi-experimental design of the current study carries the possibility that treatment and control conditions differed in ways not captured by our efforts. Although the current study controlled for actuarial risk level, no dynamic risk measure was included (similar to prior studies, e.g., Hanson et al., 2004; Olver et al., 2013), and it is possible that risk-related group differences remained. However, given the selection criteria for inpatient treatment, it is safe to assume that any remaining pretreatment differences would have indicated higher risk for the inpatient offenders compared with the untreated offenders. This is also reflected by the existence of separate Static-99R recidivism tables for forensic psychiatric offenders: the “high-risk/high-need” norm group, displaying higher expected recidivism rates at equal Static-99R scores. Higher initial risk levels for inpatient offenders would not attenuate the effects observed in the current study but if anything, make them more pronounced instead. Statistical comparison of numerous variables, however, showed very few consistent differences between treated and untreated offender groups of comparable risk levels yielded only age and ethnicity as variables of interest, neither of which showed any statistical contribution to the treatment effect. Moreover, differences in age (partly unavoidable due to extensive treatment duration) were already discounted in the Static-99R score. This leaves the finding that sex offenders of non-European descent (in our sample consisting mostly of Moroccan, Surinamese, and Antillian sex offenders) were considered less eligible for inpatient treatment; a finding that certainly deserves further inquiry. Although only minimal baseline differences were found for the assessed variables in this study, the possibility always remains that other factors, not included here, differed between the groups and impacted the outcome.
Third, methodological limitations of this study prevent conclusive inferences regarding successfulness of the therapeutic treatment per se. Given the indefinite length of the treatment, selection effects cannot be ruled out. In other words, it is possible that only the less-at-risk offenders were discharged and that offenders who would have recidivated remained in treatment indefinitely. Such a selection effect may have been more prominent for high-risk offenders, who one might assume to have been regarded with greater scrutiny, thus explaining the stronger treatment effect in this subgroup. However, there is ample reason to question that the high-risk inpatients in this study were recognized as such at the time. Of note, no formal risk assessment was ever performed prior nor during the treatment, and the average treatment duration was equal for offenders of low (M = 89.2 months, SD = 31.2) and high-risk levels (M = 86.8 months, SD 37.5; p = .86). It is also unlikely that dangerous offenders were kept in treatment indefinitely because during the time frame studied “long-stay” (civil commitment) facilities did not exist and indefinite stay in inpatient treatment was extremely rare. Most importantly, the data in this study included all offenders who were discharged during a certain time frame (as opposed to offenders who were convicted during a specific time frame), the sample therefore also included (high-risk) inpatients who were discharged after prolonged periods of treatment as well as inpatients who recidivated during treatment, returned to treatment, and were eventually discharged.
In sum, be it by effective treatment, effective selection, or a combination thereof, our study provides evidence supporting that the Dutch TBS treatment system is (partially) successful in fulfilling its mandate: (higher risk) sex offenders eligible for discharge recidivated at significantly lower rates than comparable offenders who did not progress through the TBS system.
Finally, Hanson et al. (2009) stated that instead of applying the risk principle within individual treatment programs, it is also possible to have the system adhere to the risk principle by referring offenders of certain risk levels to certain forms of treatment. Such a risk-oriented system in the Netherlands should consistently refer sex offenders of moderate-high and high actuarial risk levels to high-intensity inpatient treatment to optimize treatment effect and reduce violent (including sexual) reoffending.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.