
Abstract
Emerging research highlights the role of self-regulation in the treatment of sexual offenders. Safe Offender Strategies (SOS) is a manualized sex offender treatment program that emphasizes the role of self-regulation and self-regulatory skills development in sex offender treatment, particularly for offenders with serious mental illness and intellectual/developmental disabilities. The current study involves 156 adult male sexual offenders in an inpatient psychiatric setting who received SOS treatment for a period ranging from 6 months to 1 year. Participants’ baseline and treatment data were obtained from archival medical records describing 1 year pre-treatment and up to 2 years of treatment participation. Dependent variables included monthly count rates of verbal and physical aggression and contact and noncontact sexual offending, as well as sexual deviancy attitudes, self-regulatory ability, and cooperation with treatment and supervision, as measured by the Sex Offender Treatment Intervention and Progress Scale (SOTIPS). Data were examined via paired-samples t tests, regression, and multilevel modeling, examining the impact of overall percentage of SOS groups attended over time, comparing participants’ baseline measures to data from 2 years of treatment. The impact of predicted risk was also evaluated. Significant treatment dose effects were identified for improvements in aggression, sexual offending, and indicators of treatment compliance and change. These findings suggest that the skills-based, self-regulation approach utilized in SOS may be effective in improving clients’ aggressive and sexual behaviors, attitudes toward their offenses and treatment, and self-regulatory ability over time. Implications for further research and treatment generalizability are discussed.
Sex offender treatment is ever evolving, reflecting changes in the way we view sexual behavior, variations in our understanding of the etiology of sexual violence, breakthroughs in empirical science, and also social and political influence in managing a controversial public concern. Within the broader context of the psychosocial treatment literature, the history of sex offender treatment research is comparatively brief, with initial studies emerging only decades ago and rapidly driving us to where we find treatment today.
Early behavioral treatments focused almost exclusively on decreasing deviant sexual arousal, as it was believed that this was the primary motivation for deviant sexual behavior. Although empirical research noted a moderate relationship between deviant or offense-specific sexual arousal and sexual recidivism among known sexual offenders (e.g., Hanson & Bussiere, 1998; Hanson & Morton-Bourgon, 2005), some early treatment outcome studies failed to uniformly demonstrate that changes in sexual arousal patterns could sufficiently or effectively reduce sexual recidivism (e.g., Rice, Quinsey, & Harris, 1991). In addition, only a minority of offenders may show sexual arousal specific to their victims, and some groups of offenders may be less likely to demonstrate a link between deviant sexual arousal and sex offending behavior (e.g., juvenile sexual offenders; Hunter, Goodwin, & Becker, 1994). It is likely that there are significant moderators and mediators in this process, and deviant or offense-specific sexual arousal is only one component of a sexual offense.
Subsequent clinical attention focused on cognitive and affective processes in the development of sexual behavior problems and the treatment of sex offenders. With this shift, techniques such as social skills training, anger management, empathy training, sex values clarification, and developing age appropriate sexual relationships were incorporated into standard sex offender treatment programs that had previously emphasized the reduction of deviant sexual arousal (e.g., Abel, Mittelman, & Becker, 1985; Marshall, Anderson, & Fernandez, 1999; Marshall, Laws, & Barbaree, 1990). Empirical evaluation has demonstrated that cognitive-behavioral treatments are generally effective at reducing sexual recidivism (e.g., Hanson et al., 2002), although little is yet understood about specific treatment mechanisms that may facilitate client improvement.
Many of these cognitive-behavioral treatment components were later incorporated under the broad rubric of relapse prevention, an intervention that was initially developed to assist substance abusers with maintaining treatment gains, controlling urges, and managing drug and alcohol problems. Relapse prevention was applied to sex offender treatment in the seminal works by Pithers, Marques, Gibat, and Marlatt (1983); Laws (1989); and Laws, Hudson, and Ward (2000), and quickly became one of the most dominant forms of sex offender treatment in North America (i.e., Marshall, 1999; see also McGrath, Cumming, & Burchard, 2003; McGrath, Cumming, Burchard, Zeoli, & Ellerby, 2010). The major focus of these treatment programs was to eliminate or reduce recidivism by preventing a “relapse,” or another incident of sex offending behavior, through the identification of offense-relevant triggers, and the subsequent use of avoidance and escape behaviors associated with these triggers. Preliminary studies of relapse prevention suggested it to be successful in reducing sexual recidivism (Marques, 1999; Marques, Day, Nelson, Miner, & Laws, 1989; Marques, Day, Nelson, & West, 1994), although later evaluation of the same randomized control trial revealed few differences between experimental groups (Marques, Wiederanders, Day, Nelson, & van Ommeren, 2005). Since that time, the number of programs in North America using relapse prevention as a primary sex offender treatment modality has declined (McGrath et al., 2010).
Newly emerging sex offender treatment approaches have incorporated changes from other aspects of correctional treatment literature, positive psychology, and the science of self-regulation. Risk-Needs-Responsivity, a framework for the delivery of treatment of offenders emphasizing individual risk, empirically supported treatment needs, and mediators that affect treatment response (Andrews, Bonta, & Hoge, 1990) was introduced to correctional and community offender treatment programs as a way to enhance treatment success. Although not a specific treatment for sex offending, sex offender programs providing treatment in a manner consistent with the principles of Risk-Needs-Responsivity have demonstrated greater effectiveness in reducing sex offender recidivism (Hanson, Bourgon, Helmus, & Hodgson, 2009a, 2009b). The Good Lives Model, originating from theories of self-regulation, incorporates elements of positive psychology shown to be critical to making and maintaining important life changes (Ward & Brown, 2004; Ward & Gannon, 2006; Ward, Mann, & Gannon, 2007). This represents a departure from the traditional, deficits- or risk-based approaches to treatment and addresses offender goals in a more comprehensive, holistic way.
Similarly, Safe Offender Strategies (SOS), described in Stinson and Becker (2012), is a skills-based approach to sex offender treatment that targets the role of dysregulation and self-regulatory deficits in the initiation and maintenance of sexual behavior problems, as well as other treatment foci such as aggression, illicit substance use, and impoverished social relationships. Ultimately ascribing to the Risk-Needs-Responsivity frame, SOS emphasizes individualized treatment planning, identifying and addressing responsivity factors that often interfere with treatment effectiveness, and identifying, self-monitoring, and addressing relevant self-regulatory skills deficits that may have precipitated sexual offending and other criminogenic problems. This treatment model was developed for clinicians treating often-overlooked clients with complex psychiatric, behavioral, and sex offender treatment needs, including those offenders with serious mental illness and intellectual/developmental disabilities. These are persons for whom traditional approaches may be insufficient or inaccessible, whether due to the complexity of the problem, interfering mental health needs, or limited cognitive resources (Stinson & Becker, 2011).
SOS is delivered primarily as a group-based treatment. Ten modules are provided that combine didactic learning and experiential processing. The initial module of treatment involves client motivation and commitment to change, moving later into client-derived goals and expectations of treatment. Subsequent modules focus on specific areas of dysregulation and self-regulatory deficits (i.e., emotional, cognitive, interpersonal, and behavioral regulation), with each module concluding with a review and practice of relevant adaptive self-regulatory skills or strategies. Clients complete most assignments within the context of group discussion, thus accommodating those with intellectual or other disabilities that limit their ability to meaningfully complete homework independently. Clients are, however, expected to complete weekly self-monitoring sheets to identify self-regulation problem areas that contribute to continued sexual, behavioral, or other problems. Within this structure, clients identify their own individualized patterns of dysregulation and self-regulatory deficit that may have precipitated their sexual offending and other maladaptive or problematic behaviors. For one client, this may involve self-monitoring and using adaptive skills for difficulties such as anger, entitlement, unrealistic expectations of others, and hostility toward women related to acts of rape and physical aggression, whereas for another client, this may be the identification of problems with loneliness, anxiety, isolation from others, poor self-esteem, and impulsivity related to sexual acts with children. Thus, although the underlying theoretical conceptualization of the problem is similar across clients, the individualized or specific factors related to maladaptive behaviors will vary, requiring clients and treatment providers to develop individualized treatment plans for the development of more adaptive coping skills in these domains.
SOS was initially piloted in two different inpatient forensic psychiatric hospitals, one of which is the focus of the current study. In this analysis, we examine the effectiveness of SOS in reducing incidents of verbal, physical, and sexual aggression in an inpatient psychiatric sample during the first 2 years of treatment. We also determine whether or not SOS has an impact on client treatment engagement, self-regulatory ability, and offense-related beliefs. The current study was premised on the following hypotheses:
Method
Participant Characteristics
This study included 156 adult males residing in an inpatient forensic psychiatric hospital in the Midwestern United States. All men had been deemed eligible for sex offender treatment services by treatment providers at the facility, either due to a history of arrest for a sexual offense in the community or another institution, or due to behavior within the current institution that met legal criteria for a sexual offense (i.e., attempted or actual sexual assault, groping the breasts or genitals of male or female staff persons, or exposing their genitals or masturbating in public areas). Participants were identified for inclusion regardless of whether or not they participated in sex offender treatment during the time of the study period. Any individual meeting treatment inclusion criteria who resided within the facility for at least 6 months prior to treatment eligibility (i.e., the start date of SOS on that client’s ward or program, or the date at which the client became legally eligible to receive treatment) and for at least 6 months during the implementation of SOS on his program was identified as a study participant. Optimally, client data were included for 1 year pre-treatment and 2 years during treatment. Data collection was discontinued at the end of 2 years of treatment, as the majority of clients receiving SOS had been transferred out of the facility at that time. Therefore, available data for analysis ranged from 6 months to 1 year pre-treatment, and 6 months to 2 years while receiving inpatient SOS.
Demographic characteristics
Participant age at the time of study treatment conclusion (i.e., up to 2 years of completed treatment) ranged from 21 to 75 years, with a mean of 42.2 years (SD = 12.8). Participants were somewhat ethnically diverse, with 54.5% (n = 85) Caucasian, 39.7% African American (n = 62), 2.6% Hispanic (n = 4), 1.9% self-identified as of mixed racial heritage (n = 3), and 1.2% who declined to affiliate with a particular racial or ethnic heritage (n = 2). The majority of the participants had never been married (n = 121, 77.6%), whereas the remainder were divorced (n = 28, 17.9%), currently married (n = 2, 1.3%), or marital status was unknown (n = 5, 3.2%). Of those currently or previously married, most had been married only once (n = 23, 65.7%), with others reporting 2 (n = 8, 22.97%), 3 (n = 3, 8.6%), or 4 marriages (n = 1, 0.3%). Most participants had no known children (n = 121, 77.6%), but of those who did report fathering children (n = 35, 22.4%), they ranged from 1 to 6 children, or an average of 2.2 children each. It should be noted that some of these characteristics, including age and the infrequency with which they had been married or fathered children, are likely a function of their psychiatric characteristics and history, described further below.
Psychiatric characteristics
Study participants evidenced a wide range of serious psychiatric illness and prior history of psychiatric hospitalization. Psychiatric diagnoses were assigned by treating psychiatrists at the facility, and these data reflect those most currently assigned at the time of initiation into SOS treatment. Data related to psychiatric diagnosis were aggregated into “yes/no” categories reflective of major symptoms to describe co-morbidity of symptoms and also to attenuate the impact of clinician variability in inter-category diagnosis. For example, major depressive disorder, dysthymic disorder, depressive disorder not otherwise specified, bipolar disorders, schizoaffective disorder, and adjustment disorder with depressed mood would have all been coded as “yes” for mood disorder. Similarly, schizoaffective disorder, any type of schizophrenia, major depressive disorder with psychotic features, or psychotic disorder not otherwise specified would have been coded “yes” for psychotic disorder. All participants met criteria for at least one psychiatric disorder, as is reported in Table 1. The most frequently diagnosed symptom categories were cognitive disorder (including a range of intellectual/developmental disabilities and autism spectrum disorders; n = 99, 63.5%), mood disorder (n = 80, 51.3%), psychotic disorder (n = 80, 51.3%), and substance use disorder (n = 74, 47.4%). Given that participants were all persons with histories of sexual offending, it is perhaps not surprising that a fair number of them met diagnostic criteria for a paraphilia (n = 33, 22.2%).
Psychiatric Diagnoses, by Category.
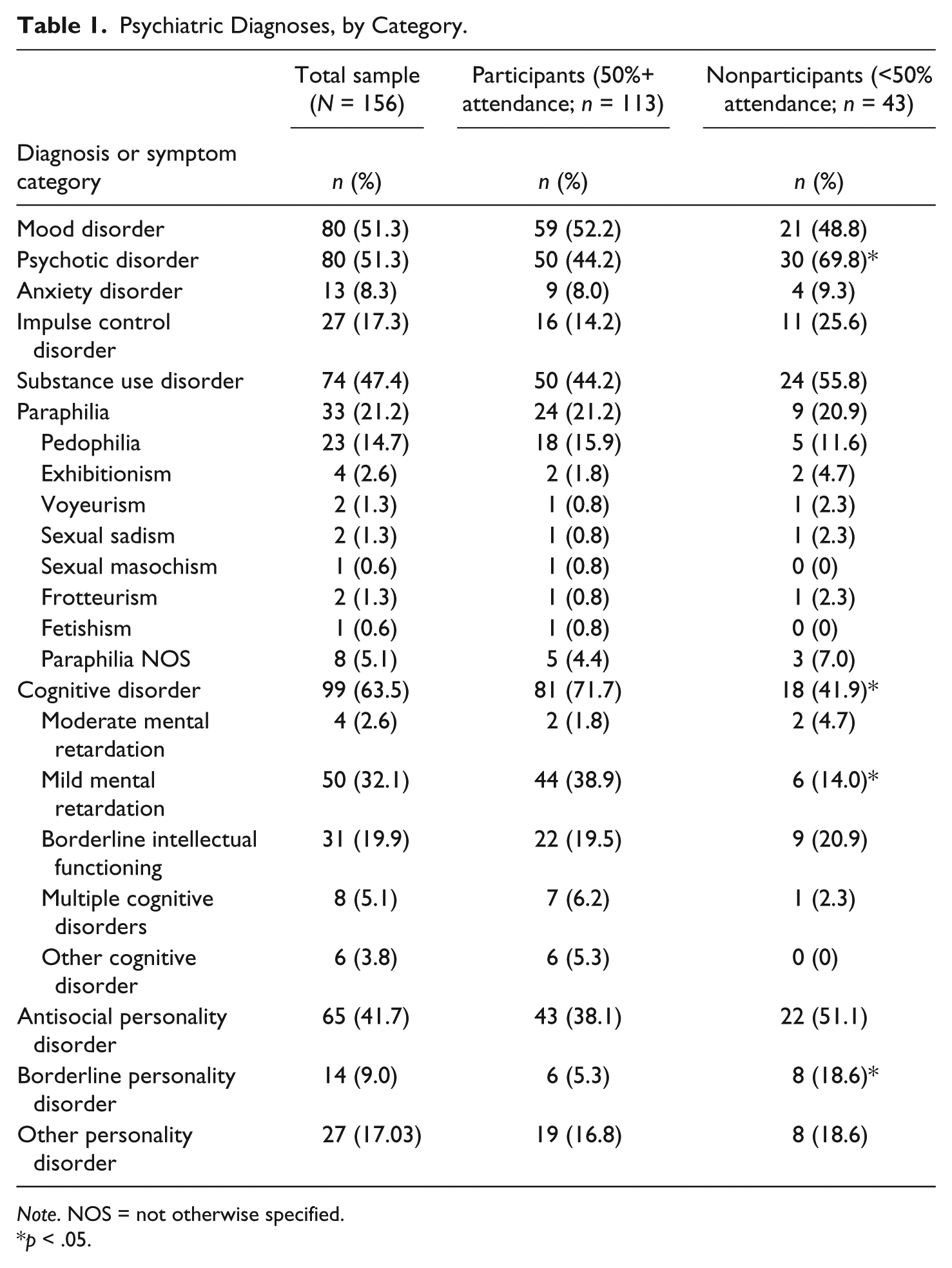
Note. NOS = not otherwise specified.
p < .05.
There was substantial diagnostic co-morbidity within the sample. Only 7.1% of the sample (n = 11) did not meet criteria for any Axis I disorders, as defined by the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000), whereas 26.3% (n = 41) only met criteria for one Axis I disorder, and the remaining 66.7% (n = 104) met criteria for two or more Axis I disorders. In comparison, 44.9% did not meet criteria for any Axis II personality disorders, but 52.6% (n = 82) met criteria for both an Axis I disorder and an Axis II personality disorder.
Previous episodes of inpatient psychiatric hospitalization were common (n = 121, 77.6%), and the age at first psychiatric hospitalization ranged from 5 to 62, with a mean age of 21.1 years (SD = 10.5). Also with regard to other areas of psychiatric concern, 35.3% of the participants (n = 55) endorsed a history of at least one suicide attempt that necessitated medical care or intervention, and 36.5% (n = 57) demonstrated a similar history of self-harm behavior. In many cases, these incidents precipitated prior episodes of inpatient psychiatric care.
Related to their current inpatient psychiatric admissions, most participants were civil commitments (n = 83, 53.2%), reflecting the state’s tendency to place people who had been found permanently incompetent to proceed to trial under a “voluntary by guardian” civil commitment status. Thus, current civil commitments often reflected initial forensic admissions. The remainder were not guilty by reason of insanity (n = 45, 28.8%), renewable court commitments (n = 2, 1.3%), or admissions as incompetent to proceed at the start of the project (n = 26, 16.7%) that changed to reflect a civil commitment status. The average length of admission at the time of the study (taking into account that many remained hospitalized following completion of their first 2 years of SOS sex offender treatment) was 10.5 years (SD = 6.7), ranging from 1 to 45 years.
Criminal and sexual offending history
Participants’ records revealed substantial histories of prior arrest, as well as histories of sexual and violent (nonsexual) behaviors. Overall, 93.5% (n = 146) evidenced a prior history of at least 1 arrest, with a mean of 5.2 arrests per person. These arrests were for violent (nonsexual) offenses (n = 70, 44.9%; M = 1.8 arrests), sexual offenses (n = 117, 75%; M = 2.6 arrests), property offenses (n = 71, 45.5%; M = 2.7 arrests), drug offenses (n = 32, 20.5%; M = 2.4 arrests), and other arrests (n = 42, 26.9%; M = 2.1 arrests), which included trespassing, resisting arrests, and status offenses. Despite the frequency of arrest, only 32.1% (n = 50) of the participants had a prior history of incarceration, which is likely indicative of their status as offenders within the forensic mental health system. In addition, records noted a history of physical, nonsexual aggression for 89.1% of the participants (n = 139).
Of the 75% of participants with a history of arrest for sexual offenses (M = 2.6 sexual arrests), 59% (n = 69) had been convicted or found not guilty by reason of insanity for a sexual offense, with an average of 1.5 convictions each. Of the 25% who had never been arrested for a sexual offense, they or family members reported one or more community offenses for which they had not been arrested (i.e., genital exposure or public masturbation = 5.4%, voyeurism = 2.7%, bestiality = 2.7%, attempted rape or unwanted sexual touching = 24.3%, child sexual abuse = 29.7%, adult sexual assault = 16.2%), or they had engaged in sexual offending within residential care settings (i.e., explicit sexual threats or stalking behaviors = 36.1%, genital exposure or public masturbation = 55.6%, attempted rape or unwanted sexual touching = 66.7%, adult sexual assault = 36.1%). As can be inferred from these numbers, among those who had not been previously arrested, there was often overlap between community and residential behaviors that would qualify as illegal or criminal sexual acts. Other data related to their sexual offenses were collected from archival documentation, family reports, or participant self-report. Participants were an average of 24 years of age (SD = 11.06; range = 8-62) at their first known or reported sexual offense (n = 128, 82.1%), and the first offense typically involved either a sexual act against a child (n = 82, 52.6%) or an aggressive sexual act against a nonconsenting adult (n = 39, 25%). Data presented in Table 2 describe the characteristics of their victims, with many participants offending against persons in multiple categories. Data were categorized as “any” offense in this category to permit reporting of multiple victim types per participant. Overall, these data reflect the psychiatric and behavioral severity of the sample utilized for this study.
Number of Participants Who Sexually Offended in Different Victim Categories.
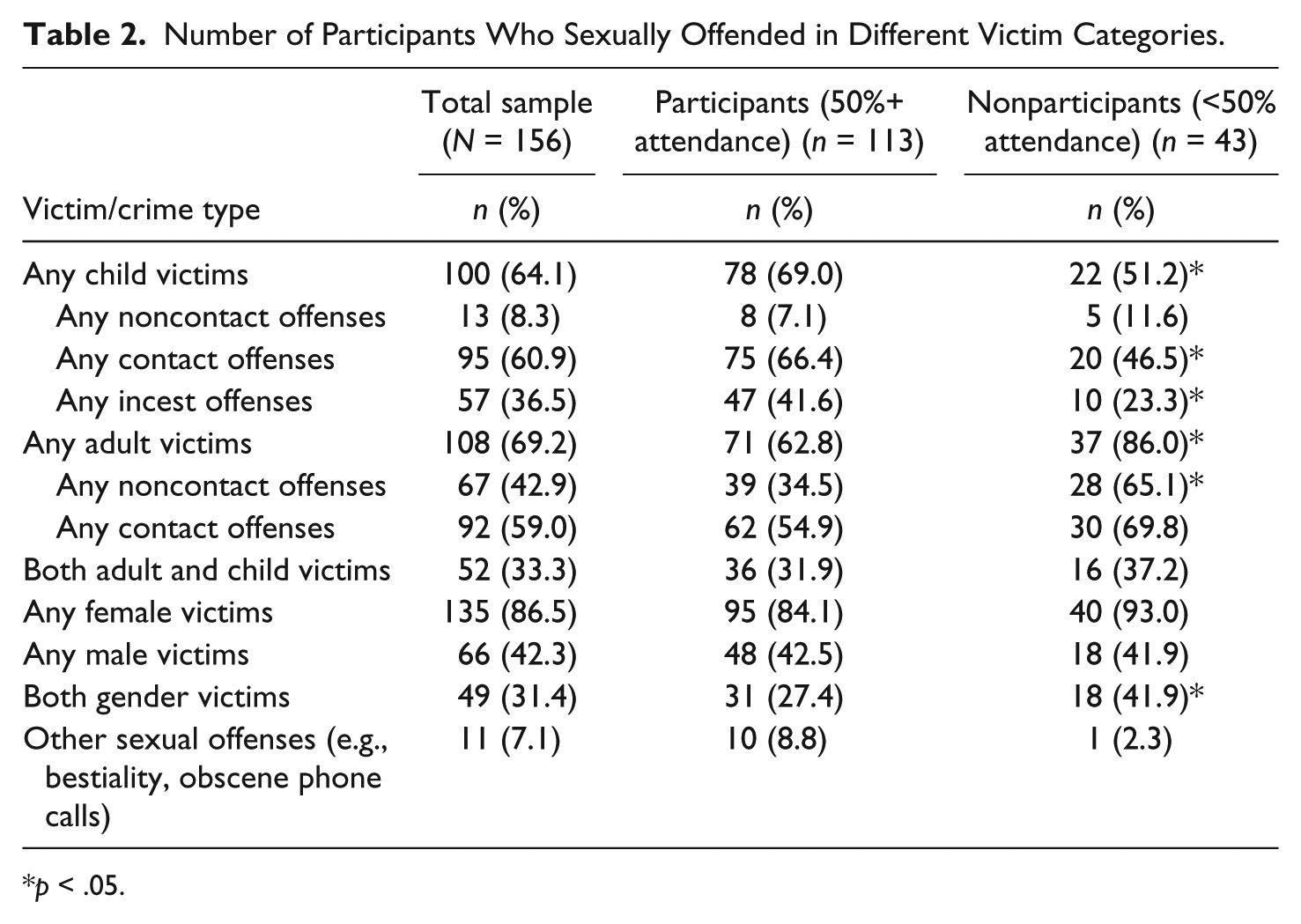
p < .05.
Participants’ scores on the Static-99R (Helmus, Thornton, Hanson, & Babchishin, 2012) were available from archival client medical records. Scores were available for all 156 participants and reflected their most recent estimates of risk at the time of study completion and data collection. For some, this included a risk assessment conducted immediately prior to their release or transfer from the facility. Scores ranged from −3 to 9, with a mean of 2.72 (SD = 1.982). Overall, 41 participants (26.3%) scored within the low risk range on this instrument (i.e., scores of −3 to 1). Sixty-three participants (40.4%) were classified in the low-moderate risk range (i.e., scores of 2 to 3). Among the remainder, 40 participants (25.6%) were moderate-high risk (i.e., scores of 4 or 5), and 12 participants (7.7%) were high risk (i.e., scores of 6 or higher).
Measures
Archival data were collected as part of a program and treatment evaluation project at the sponsoring facility. No individual participants were contacted or interviewed for the purposes of the current research. Permissions and approvals for human participants research were obtained through an Institutional Review Board affiliated with the facility and the first author of this article at the time of project implementation, as well as the professional research review committees of the facility and the state Department of Mental Health. No adverse events or negative participant consequences occurred as the result of this research. Data collection procedures did not adversely affect the care and treatment provided to any of the participants involved.
Treatment programming
Sixteen total SOS groups, averaging five to eight participants each, began at the research site in late 2007 to early 2008. Group membership remained open to accommodate new admissions to the facility. Group therapists were extensively trained in September and October of 2007 and then supervised by one of the developers of the SOS manual throughout the duration of the study. Monthly adherence checks were done to facilitate supervision and ensure compliance with the philosophy of treatment and implementation of SOS activities and discussions. Clients were selected for SOS by their ward team leaders and program coordinators based on a known or admitted history of illegal sexual behavior either in the community or while in residential care. Group facilitators were a part of each program and often conducted not only SOS but other core program groups. Frequency of group sessions were minimally expected to be once per week, but this was not always possible due to holidays, staff absences, or other programmatic demands. Clients continued to participate in SOS groups until such time as they were transferred from the facility either into community homes or other secure forensic residences.
Sources of information
Data were compiled from archival medical records maintained by the facility as part of a client’s care and treatment. Documents reviewed included admission psychiatric and social service assessments, available psychological testing, arrest and court records describing offense histories, annual psychiatric and social service reviews, sex offender group and other group progress notes written by treatment providers, daily documentation of behavior and treatment progress by treatment providers and direct care staff, and archived database reports indicating overall program progress (including group attendance, infractions or program violations earned, and systematic promotions or demotions in client stage or level). Additional data related to client progress was recorded from conversations with treatment providers and clinical supervisors within the sex offender treatment program at the facility.
Behavioral data
For the purposes of this analysis, data were coded “per incident” tallies of the following incidents in 6-month incremental periods: (a) verbal aggression (i.e., making a specific verbal threat of intended bodily harm toward another person); (b) physical aggression (i.e., acts of bodily harm toward another person); (c) noncontact sexual offending (i.e., acts of voyeurism, exposure of genitalia in a public location, or masturbating through the clothes or with genitals exposed when in a public location); and (d) contact sexual offending (i.e., unwanted sexual contact, sexually aggressive contact behavior, or sexual contact toward a person incapable of providing consent). These data were coded from daily progress notes by direct care staff and treatment providers on the participants’ wards. Data were coded for time periods ranging from 6 months to 1 year pre-SOS, and also for periods ranging from 6 months to 4 years during SOS implementation for that participant. Individual incidents were tallied into 5-month increments to allow for sufficient variability in number of incidents in a given time period.
In addition, client group attendance was coded from treatment provider group notes during these same periods. It was noted how many groups were available during the up-to-2-year period of SOS implementation from per-group progress notes, and notes were written for each participant indicating whether or not they attended the offered group, level of participation, topic discussed, and estimated progress. Data were tallied for groups offered and groups attended to calculate the percentage of SOS groups each participant attended during a given treatment year.
Sex Offender Treatment Intervention and Progress Scale
Individual participant progress in sex offender and other psychosocial treatment during the pre-SOS period and up to 2 years of SOS implementation were measured in 6-month increments using earlier versions of the Sex Offender Treatment Intervention and Progress Scale (SOTIPS; McGrath, Lasher, & Cumming, 2012), namely, the Sex Offender Treatment Needs and Progress Scale (McGrath & Cumming, 2003) and the Treatment Intervention and Progress Scale for Sexual Abusers With Intellectual Disabilities (SOTIPS-IDD; McGrath, 2005). These original research versions of the SOTIPS were utilized for consistency, as those were the versions available at the time of study initiation. Research on this instrument demonstrates good inter-class correlations and inter-rater reliability, ranging from .59 to .84 for independent items and .91 for total SOTIPS score (McGrath, Cumming, & Livingston, 2005). For the purposes of this analysis, SOTIPS subscale scores were coded for each participant for the time periods of interest by a team of persons including their SOS group treatment providers, case managers, and program director. These subscale scores included (a) Sexual deviancy or sex offense responsibility, (b) Criminality, (c) Self-regulation, (d) Cooperation with treatment and supervision requirements, (e) Lifestyle stability, and (f) Social supports. For this study, we were most interested in outcomes on subscales reflective of attitudes and behaviors related to sexual offending (with a possible SOTIPS score range = 0-18), self-regulatory ability (possible score range = 0-15), and cooperativeness with treatment and supervision requirements (possible score range = 0-9 for the SOTIPS and 0-15 for the SOTIPS-IDD version).
Research Design
Participant outcomes were examined with regard to both behavioral data and treatment progress data, first with paired-samples t tests to establish significant changes from pre-treatment to 2-years post treatment, and also as a function of both the percentage of SOS groups attended and the length of time involved in SOS during the first 2 years of treatment implementation. Participant data were separated into pre-treatment and in-treatment periods to inform our hypotheses regarding the impact of ongoing skills-based SOS treatment on individual participant behavior. We did not separate participants into treatment versus control groups but instead used participant pre-treatment behavior and progress as a baseline control, and examined treatment-related changes both within and between participants as a function of time and treatment dose (i.e., percentage of available groups attended). It should be noted that all participants were offered the same amount and dose of treatment opportunity (i.e., number of groups) on their respective programs, regardless of the nature and persistence of their offending behavior, in accordance with facility policy. All procedures were performed using SPSS, Version 21, and Mplus, Version 13.1.
Initial analyses were performed using paired-samples t tests of 121 participants who had complete data for the 6 months prior to treatment initiation and 24 months of treatment participation. For this analysis, participants were divided in groups of 83 persons who attended 50% or more of available SOS groups during that time, and 38 persons who attended fewer than 50% of available SOS groups. In subsequent analyses, stepwise multiple regression was used to identify variables that were predictive of significant change from pre-treatment to 18-month and 24-month endpoints of SOS treatment for verbal, physical, and sexual aggression, as well as subscales of the SOTIPS indicative of sexual offense responsibility, self-regulatory ability, and cooperation with treatment and supervisory requirements. Independent variables entered into the regression included pre-treatment baseline measures, Static-99R scores, and the percentage of groups attended during the first 2 years of treatment, with outcome at the end of Treatment Year 2 as a dependent variable. The 2 SOS endpoints of 18 and 24 months were used to account for the number of clients who were successfully transferred from the facility during that time frame. In other words, as only 121 of the original 156 participants (77.6%) remained in the facility at 24 months, data were also analyzed after 18 months of treatment. At 18 months, 138 of the original 156 participants (88.5%) were still residing in the facility and involved in SOS treatment.
As noted, the paired-samples t tests and regression analyses excluded or systematically dropped cases with missing data at specified endpoints. Only 121 of the 156 participants had a full 3-year data set, as those who made the most treatment progress and demonstrated behavioral improvement were likely to be transferred prior to the end of 2 years in treatment. We felt it important to not exclude those participants, as their data reflected significant positive treatment effects. A second issue involved the data describing change in sex offending behaviors during the course of treatment. Those who were most likely to exhibit improvement in this area were also the most likely to be transferred out of the facility into less restrictive placements. This makes inherent sense, as the majority of these participants were directly admitted as the result of a sexual offense. Thus, the remaining participants at the end of 2 years had disproportionately high rates of continued sexual offending. In addition, there was more limited variability with regard to rates of sexual offenses in the sample, as other variables (i.e., verbal and physical aggression) have typically higher base rates in samples such as this one.
To account for these concerns, we ran an additional analysis utilizing multilevel modeling in which observations were nested within subjects over time, and expected trajectories of change over time were extrapolated so that cases with missing data could still be included in the analysis (e.g., Raudenbush & Bryk, 2002). For this part of the analysis, time and percent of groups attended were entered as independent variables along with the Static-99R estimations for each of the outcome variables described above. We used this same multilevel modeling technique on indicators of treatment progress on the SOTIPS, given the limited range of variability in scores across time points, and also because those with the most improvement on these measures were typically transferred or released prior to the end of Treatment Year 2, thus dropping them from the paired-samples t tests and regression analysis. All case sets were included for this analysis.
Results
Of the 156 participants, all of whom were eligible to receive sex offender treatment during the study period, only 10 (6.4%) refused to attend any SOS treatment groups during the first year, and 13 (8.3%) refused to attend any SOS treatment groups during the second year. Of these, 8 participants refused to attend any SOS groups in both Years 1 and 2, 2 persons who refused attendance in the first year attended during the second, and 5 participants who attended during the first year dropped out during the second. In the first year, 73.7% of study participants attended more than 70% of available treatment groups, with 27.6% overall attending all available sex offender treatment programming. In the second year, 76.1% of the remaining 138 clients (i.e., 18 had already been transferred to other facilities) attended more than 70% of groups, with 20.3% of the remaining participants attending all available groups. On average, 32.8 SOS treatment groups were offered during the first year (range = 5-63) with a mean of 77.7% attendance (including those 6.4% of clients who refused to attend), and during the second year, an average of 30.1 SOS treatment groups were offered (range = 3-49) with a mean of 75.9% attendance (including those 8.3% who refused to attend). It should be noted that in some cases, few groups were offered to participants due to either transfer from the facility during that particular year, or group cancellations due to staff shortages or a lack of sufficient group members to run the group on an assigned day. Interestingly, risk scores on the Static-99R were not significantly correlated with group attendance (r = .10, p = .25), suggesting that risk level had little impact on treatment participation for this sample. To some degree, participant characteristics varied by group, such that persons in the participant group were less likely to evidence psychosis and borderline personality disordered characteristics and demonstrated a higher rate of cognitive impairments (see Table 1), while being also more likely to have engaged in sexual offenses against children (see Table 2).
Participants’ average rates of physical, verbal, and sexual aggression, as well as SOTIPS subscale scores for 6 months pre-treatment and 2 years in-treatment are presented in Table 3. Despite the transfer or release of 35 of the most successful or behaviorally stable participants by the end of 24 months of SOS treatment, as can be seen from these tables, target behaviors and treatment progress scores incrementally improved on average across the groups, regardless of whether or not persons who only minimally participated in treatment were included. Paired-samples t tests revealed significant treatment effects for persons attending 50% or more of SOS groups during the first 24 months for all measures, with the exception of contact sexual offenses, which neared significance (see Table 4). Group means for persons attending fewer than 50% of available SOS groups during that time did not significantly change, with the exception of contact sexual offenses, which improved for the minimal treatment group. It was determined that this was due to an outlier within that subsample (i.e., a participant whose sexually aggressive behaviors were so severe that facility administration intervened to limit his behavior).
Average Frequencies of Aggression and Average SOTIPS Subscale Scores.
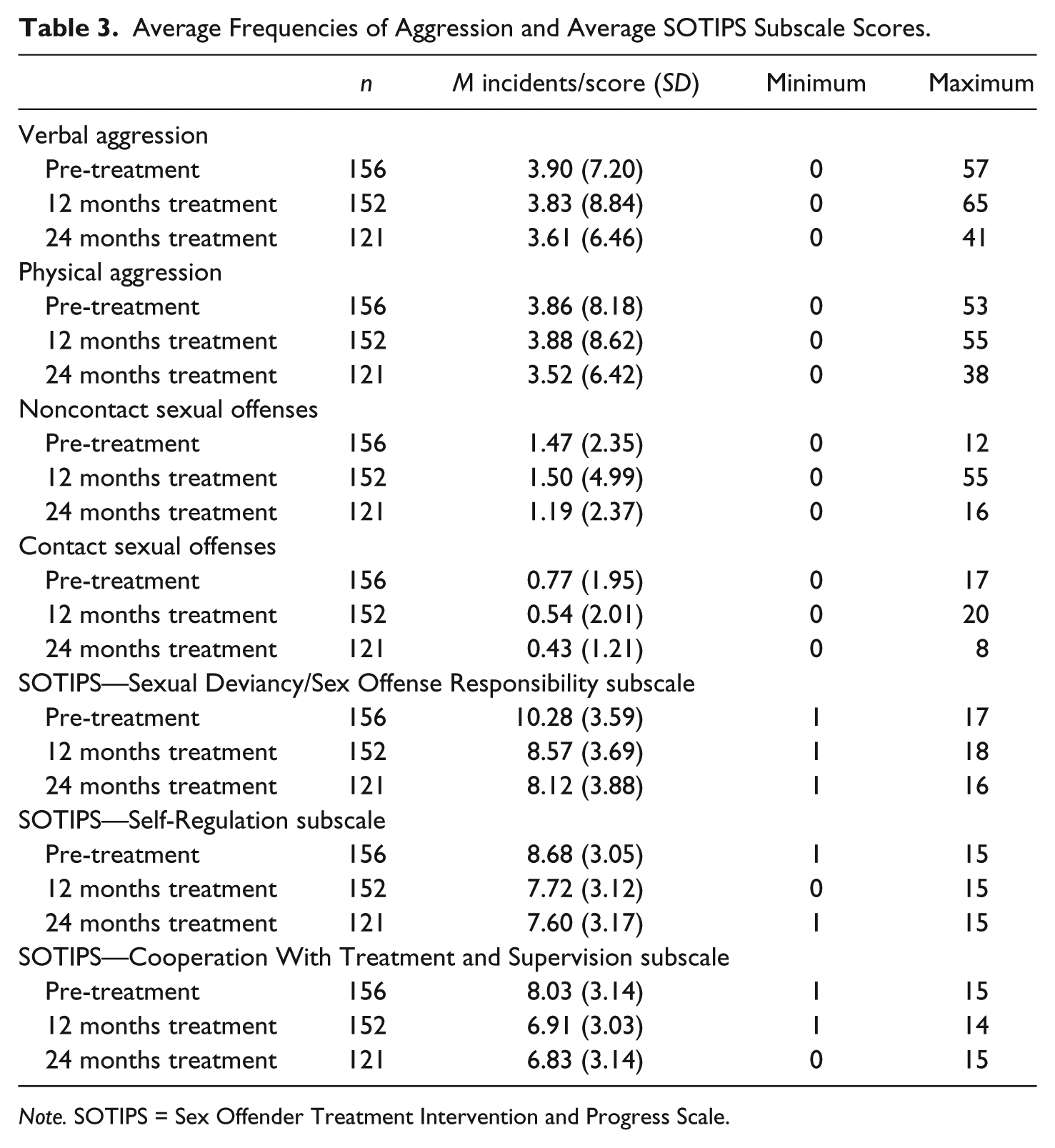
Note. SOTIPS = Sex Offender Treatment Intervention and Progress Scale.
Paired-Samples t Tests by Group Over 2 Years (n = 121).
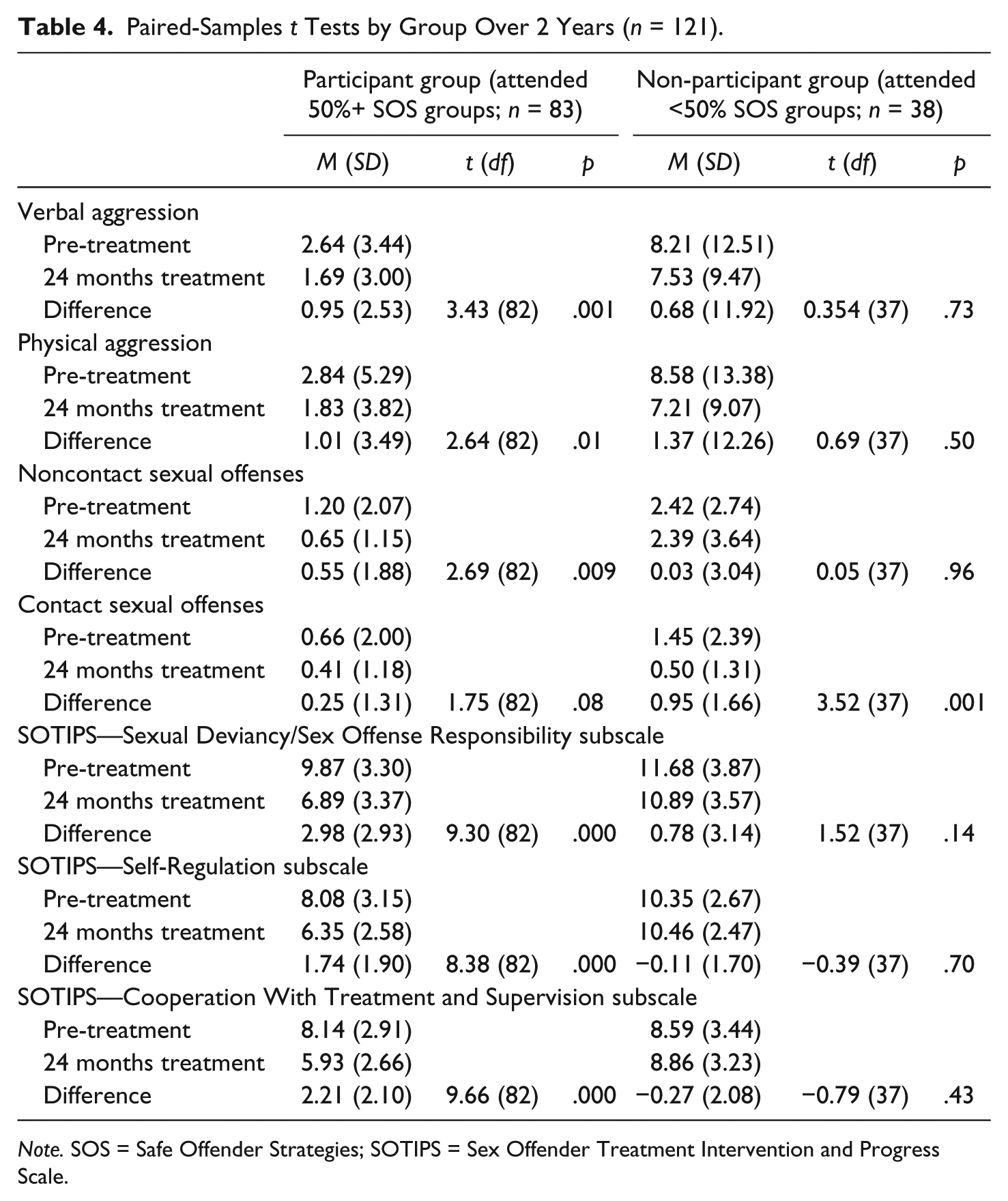
Note. SOS = Safe Offender Strategies; SOTIPS = Sex Offender Treatment Intervention and Progress Scale.
However, we must also examine the impact of group attendance, time, and risk on treatment outcomes. Thus, to demonstrate this effect with greater precision, 6-month incremental data were analyzed using stepwise multiple regression to determine the impact of time, percentage of groups, and predicted risk on target behaviors and treatment progress scores. A significant treatment dose effect (i.e., percentage of groups attended over time) was demonstrated for verbal aggression at 18 months, R2 = .59, F(2, 133) = 94.32, p < .001, and 24 months, R2 = .36, F(2, 118) = 33.20, p < .001. This effect was also seen for physical aggression at 18 months, R2 = .57, F(2, 133) = 89.70, p < .001, and 24 months, R2 = .37, F(2, 118) = 34.80, p < .001. Similar findings were demonstrated for noncontact sexual aggression at 18 months, R2 = .26, F(2, 134) = 23.20, p < .001, and 24 months, R2 = .30, F(2, 118) = 25.57, p < .001. With regard to contact sexual offending, treatment participation was a significant predictor of a reduction in contact sexual offenses at 18 months, R2 = .71, F(2, 134) = 109.34, p < .001, but not for the smaller 24-month sample, where the only significant predictor of end-point contact sexual aggression was pre-treatment contact sexual aggression, R2 = .58, F(1, 119) = 165.31 p < .001. These data are described further in Table 5. In sum, those participants who attended a greater percentage of SOS groups during those first 2 years of treatment evidenced a significant reduction in the number of incidents of verbal and physical aggression, as well as noncontact sexual aggression following 18 and 24 months of treatment, and that a highly significant number benefitted from treatment at 18 months for their contact sexual offending, but that this was not necessarily true at 24 months for this sample.
Effects of Percentage SOS Groups Attended on Behavioral Outcome at 18 and 24 Months.
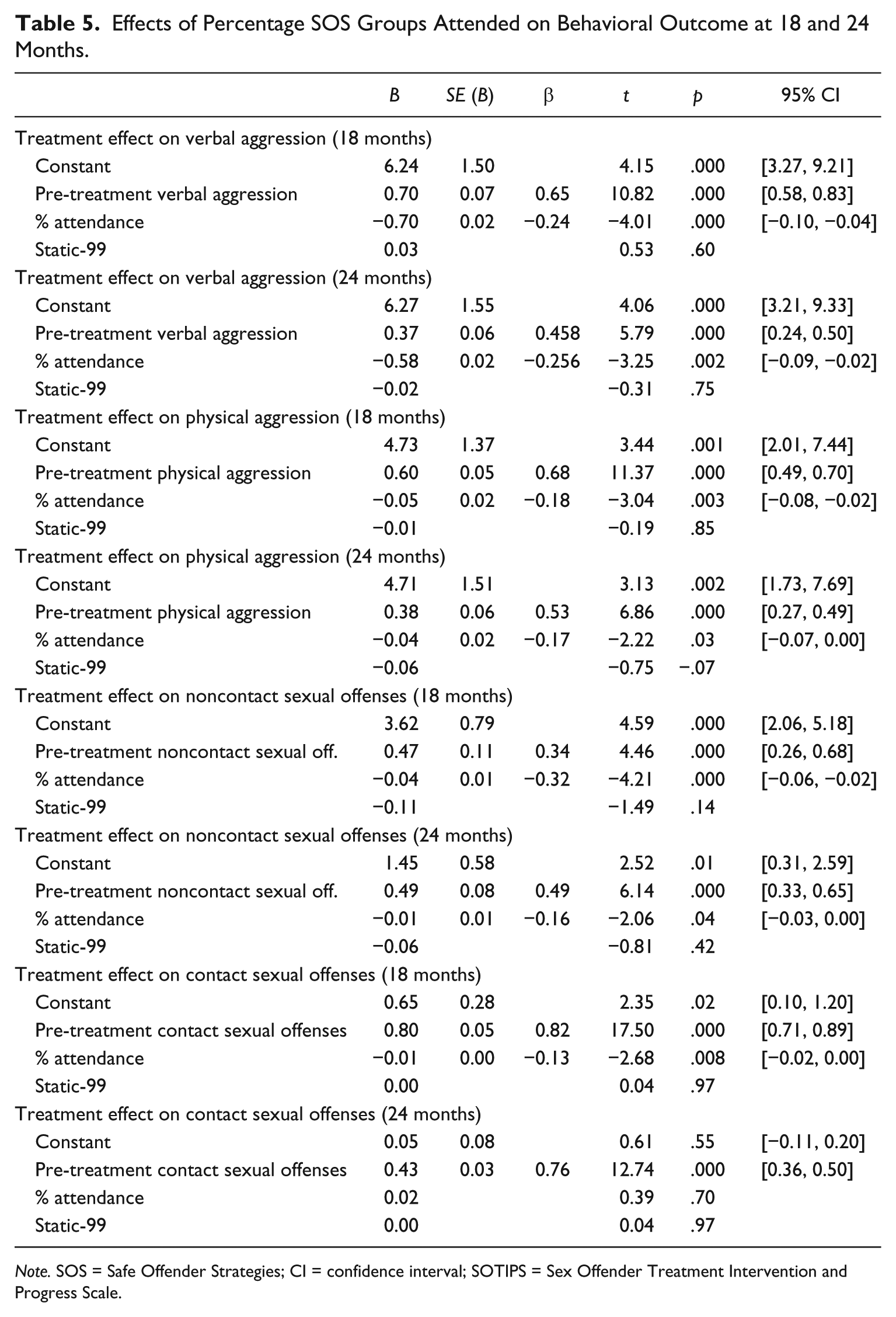
Note. SOS = Safe Offender Strategies; CI = confidence interval; SOTIPS = Sex Offender Treatment Intervention and Progress Scale.
Similar findings were obtained through multilevel modeling procedures. We focused these analyses primarily on sexual offenses that occurred during the 2-year treatment period, as the regression procedures described above would be most affected by the low base rates of such behaviors and loss of “successful” (i.e., nonsex offending) participants. Here, multilevel modeling rendered a significant effect of SOS group attendance over time on noncontact (β = −0.01, ratio of estimate to standard error [Est/SE] = −2.73, root mean square error of approximation [RMSEA] = 0.17, Akaike information criterion[AIC] = 13,249.10, Bayesian information criterion [BIC] = 13,276.58) and contact sexual offending (β = −0.10, Est/SE = −2.83, RMSEA = 0.05, AIC = 12,173.33, BIC = 12,200.81). Static-99R risk scores were not significant predictors in either of these models (noncontact sexual offending: β = −0.06, Est/SE = −0.71; contact sexual offending: β = −0.02, Est/SE = −0.54).
On the SOTIPS measure of treatment progress, multiple regression revealed a significant treatment effect for improvement on all three subscales of interest: Sexual Deviancy/Sex Offender Responsibility at 18 months, R2 = .58, F(2, 135) = 91.47, p < .001, and 24 months, R2 = .53, F(2, 118) = 65.37, p < .001; Self-Regulation at 18 months, R2 = .65, F(2, 135) = 125.55, p < .001, and 24 months, R2 = .70, F(2, 118) = 139.17, p < .001; and Cooperation With Treatment and Supervision at 18 months, R2 = .55, F(2, 135) = 82.17, p < .001, and 24 months, R2 = .57, F(2, 118) = 77.39, p < .001. These findings are described further in Table 6. As was the case with the behavioral progress indicators, improvements in sexual attitudes and responsibility, observable self-regulatory ability, and cooperation with treatment and supervision as the result of treatment attendance over time were evident following 18 and 24 months of SOS treatment. Treatment effects were also observed for these variables through use of multilevel modeling. Significant changes in sexual deviance/sex offender responsibility scores, RMSEA = 0.23, AIC = 12960.13, BIC = 12987.63, were predicted by time in SOS, β = −0.47, Est/SE = −6.38; percentage of SOS groups attended, β = −0.01, Est/SE = −4.62; and Static-99R risk score, β = −0.28, Est/SE = −2.17. Self-regulation scores were significantly predicted (RMSEA = 0.26, AIC = 12519.90, BIC = 12547.40) by both time in SOS, β = −0.20, Est/SE = −4.07; and percentage of SOS groups attended, β = −0.01, Est/SE = −5.08; but not estimated risk, β = −0.04, Est/SE = −0.34. Finally, significant predictors of cooperation with treatment and supervision (RMSEA = 0.12, AIC = 12681.58, BIC = 12709.08) included both time, β = −0.25, Est/SE = −4.09; and percentage of groups attended, β = −0.01, Est/SE = −5.31; but not risk, β = −0.046, Est/SE = −0.44.
Effects of Percentage SOS Groups Attended on SOTIPS Treatment Progress Indicators at 18 and 24 Months.
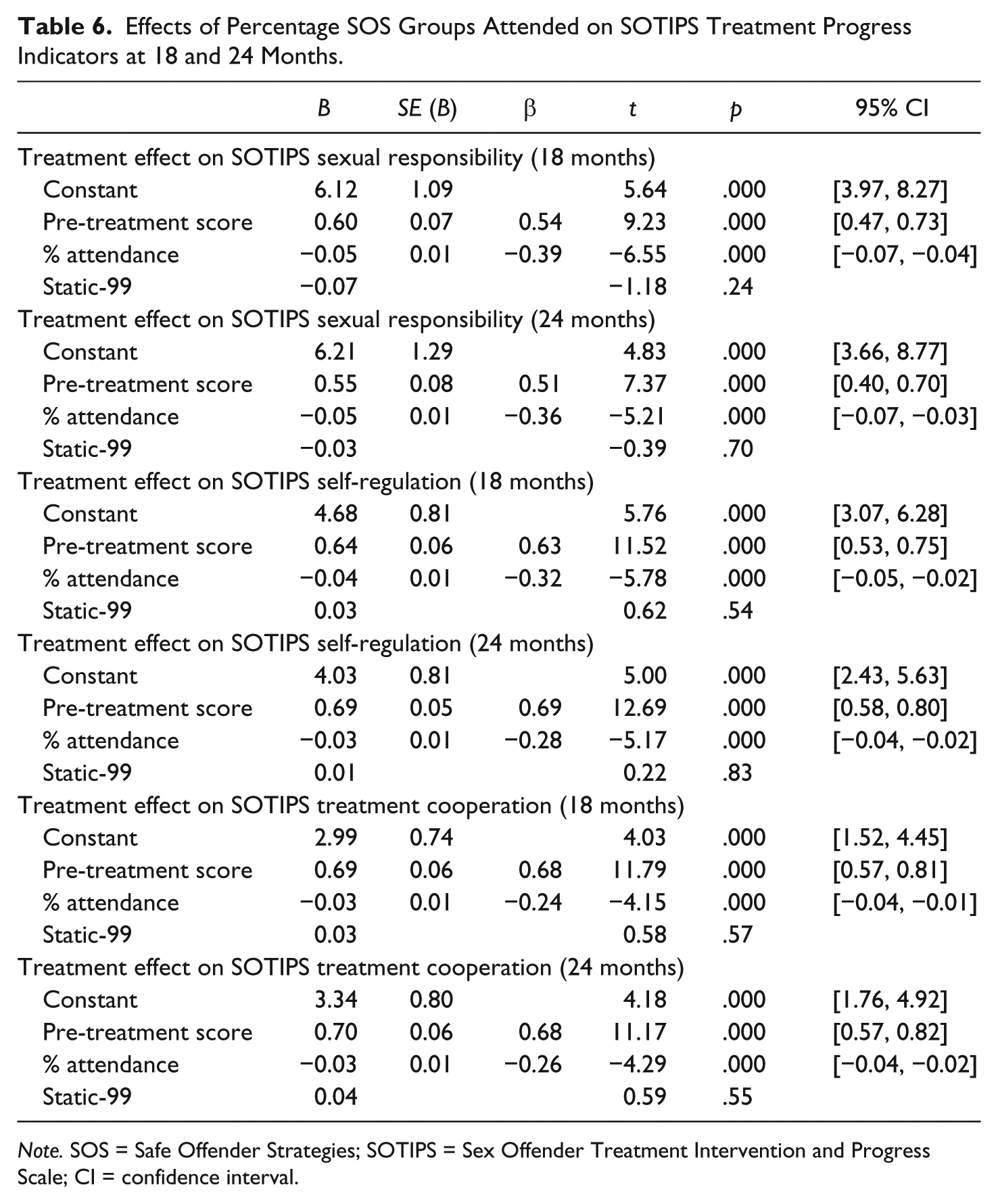
Note. SOS = Safe Offender Strategies; SOTIPS = Sex Offender Treatment Intervention and Progress Scale; CI = confidence interval.
Discussion
In this study, a sample of 156 inpatient sex offenders in a forensic psychiatric hospital receiving SOS over a period of 2 years were examined for significant changes in their rates of sexual and other aggression, as well as treatment engagement, self-regulatory ability, and demonstrated learning related to sexual responsibility and behavior. With regard to our proposed hypotheses, results suggest significant decreases in sexual and other aggression (Hypothesis 1), improvements in treatment engagement and compliance with supervision (Hypothesis 2), and self-regulatory abilities and prosocial views inconsistent with sexual offending (Hypothesis 3) for those clients who attended 50% or more of SOS groups, and those who attended a greater number of SOS groups over time. These findings are comparable with earlier research suggestive of the effectiveness of sex offender treatment modalities utilizing a Risk-Needs-Responsivity perspective (Hanson et al., 2009a, 2009b), as well as one other study describing SOS as an effective treatment in comparison with a relapse prevention protocol (Stinson, McVay, & Becker, in press).
Although only 33% of the current sample presented as moderate-high or high risk on the Static-99R, it is of note that the participants demonstrated significant need in terms of psychiatric, interpersonal, and criminogenic needs as evidenced by the SOTIPS. In addition, mean incidents of verbal, physical, and sexual aggression among participants both before and during treatment demonstrated a degree of continuing behavioral risk among this group, as few had not engaged in these behaviors at some point during the pre-treatment or treatment periods.
Implications
These treatment effects are evident for those participants who actively attended treatment over a course of 2 years, at the end of which most clients had only reached Module 4 of 10 of the SOS treatment manual (Stinson & Becker, 2012). Thus, an important implication of these findings is that clients can begin to make significant changes in their behavior, thoughts, and self-regulatory and self-management abilities during the early stages of treatment, and that such changes may be evident in even a sex offender population with complex and multifaceted needs. Another important implication is one often discussed within the sex offender treatment and general psychotherapy literature—motivation and commitment to treatment are key elements that shape the course of treatment and its eventual outcome (e.g., Prescott, 2009; Tierney & McCabe, 2002). The results of the current study suggest that those who merely attended more groups over a greater period of time—perhaps regardless of finite differences in their levels of participation or the initial complexity of their treatment issues—showed behaviorally noticeable and statistically significant changes as treatment progressed, in comparison with their pre-treatment baseline.
Within the findings reported here, it is clear that some differences were evident between those who participated in treatment and those who did not. Although all participants engaged in problematic behavior in the period observed prior to the initiation of SOS, those who did not attend treatment had overall higher rates of problematic behavior than those who did. We attempted to control for this in our regression analyses in that pre-treatment level of behavioral instability was included as an independent variable. A treatment effect for SOS was still evident following this step. Furthermore, contrary to what might be expected, those who were less engaged in treatment were persons with offenses against adults rather than children, a lesser degree of cognitive impairment, and more prominent psychotic and borderline personality-disordered symptoms. Thus, rather than an effect of impulsivity or sexual deviance, it is possible that the groups differed in treatment motivation and engagement due to psychiatric or other factors.
Implications for further treatment with this population and risk management include a continued focus on self-management and self-regulatory skills. As evidenced by findings from the SOTIPS as well as demonstrable behavior changes, SOS was effective in increasing clients’ self-regulatory abilities and control over their behaviors. Presumably, they were able to develop adaptive self-regulatory strategies through this skills-based approach and apply them in the moment, often generalized beyond just sexual behavior and to other problematic behaviors as well. As was evidenced by the SOTIPS, participants presented with a range of treatment needs, including significant psychiatric symptoms, impulsivity, offense-supportive beliefs and attitudes, continuing behavior problems, and difficulties complying with treatment and facility supervision guidelines. These areas of treatment emphasis and necessary skills development could also be incorporated into a client’s risk management plan, to further the effectiveness of treatment even beyond the immediate intervention.
Although this treatment was initially piloted on an inpatient sex offender population, there is reason to believe that it will also be effective for clients with serious psychiatric disorders or intellectual/developmental disabilities who are receiving sex offender treatment in the community. SOS emphasizes the role of self-regulation and self-regulatory deficits, so that a variety of client issues can be conceptualized in a common frame and individualized to fit a particular client’s needs. Thus, although we have demonstrated some early empirical support for treatment effectiveness with a complex client population in one setting, it is possible that this may also generalize to those with psychiatric symptoms or cognitive limitations in other treatment settings.
Of note are findings about risk in the current analyses. Idealistically, if treatment followed the fundamental Risk-Needs-Responsivity principles, clients would be matched to programming appropriate for their level of risk. Because of statutory requirements and facility policy for this particular sample, we were not able to substantially vary the dose or length of treatment offered to participants based on their risk. Thus, all participants received SOS in the same manner, despite different offenses, offense severity, and the presence or absence of continued offending behavior. Yet, risk scores on the Static-99R were unrelated to all outcome variables of interest with one exception, and that was the Sexual Deviance/Sex Offense Responsibility scale on the SOTIPS. This scale is likely more sensitive to risk, as it includes indices of other risk-relevant variables, such as offense-supportive sexual interests and insights into continued risk. That the other outcomes were not significantly affected by participants’ predicted risk though is an important point, and this may reflect idiosyncrasies within a complex psychiatric population. Thus, decisions regarding treatment need and potential outcome may need to be made in concert with other individualized considerations.
A final implication relates to the length of treatment. Here, we have indicated improvements over a 2-year course of treatment—measurable at 18- and 24-month endpoints—at which point, a number of clients were transferred to less restrictive alternative placements in which they continued to receive care, and the remaining clients continued to receive SOS as usual. It is our belief that with such a complex client group, including persons with sexual and other behavioral problems, long histories of trauma and maltreatment, prominent psychiatric symptomology, and significant intellectual, cognitive, and developmental deficits, comprehensive and long-term treatment is needed. How “long-term” is often dependent on the individual case, but SOS was designed for those who perhaps needed more than a 6- to 12-month course of treatment emphasizing one area of particular need (i.e., sex offending). Thus, another implication of these findings is that although those who attended treatment showed significant improvement, these improvements were still not sufficient to justify unsupervised and unsupported release to the community. It is expected that meaningful and lasting change takes time, and that clients will need to continue learning and practicing adaptive regulatory skills in treatment before they are fully ready to use them with minimal support, and before they have fully replaced maladaptive skills with newly learned ones.
Study Limitations
A crucial limitation of the current study is that it represents only a time-limited sample of the effectiveness of SOS. As noted already within this discussion, participants had only received 2 years of a longer form of treatment, and that they had most often completed only 4 modules of a 10-module curriculum at the time of data collection. For some, this was sufficient for facility administration to feel confident in transferring them to less restrictive placements. However, for others, it led to continued treatment within the same facility. At this point, we do not know whether further treatment offers continued benefit, or whether clients would reach a maximum point of benefit at some time prior to the end of a 10-module treatment cycle. Similarly, treatment was not administered as frequently as what would be ideal, given the complex needs of the sample. As noted previously, clients who attended 100% of available groups in Years 1 and 2 were provided, on average, 33 and 30 sessions, respectively. Gaps in treatment might have led to increased attrition or failure to retain treatment concepts, thus limiting the overall impact of SOS on behavior.
A second limitation is the generalizability of the current sample population. This sample was comprised of a group of psychiatric inpatients residing in a therapeutic milieu, who were receiving other forms of psychosocial intervention and psychotropic medications at the time of the study. They demonstrated significant treatment need on measures such as the SOTIPS, and presented with significant history of psychiatric symptoms and long-term hospitalization. Thus, the impact of SOS on these clients’ behaviors, treatment attitudes, and self-regulatory improvement may not generalize to those receiving treatment in other settings, or for other types of problems, or who may present with fewer indicators of complex risk. Yet, as we were most interested in improvements from individual participant baselines, we were able to decrease the impact of setting on the results, as well as combine participants at different levels of security and with different diagnoses to mitigate the effect of the severity and complexity of their presenting problems.
Third, it should be emphasized that participants in SOS treatment during this period were involved in other structured, empirically based forms of psychosocial intervention to address other treatment needs, including mental health symptoms, skills deficits, and violent behavior. Thus, although SOS did demonstrate an impact on participants’ aggressive and sexual behaviors over time, other forms of intervention and involvement with treatment providers likely contributed to their overall success in achieving treatment milestones. It is also possible that some of the changes observed over time were attributable to the effects of these varied interventions. Future research would benefit from appreciably measuring the impact of other forms of treatment intervention for this complex population. It is also important to note that the clients began SOS at different time points within their current period of admission, in that some began their participation after a lengthy period of hospitalization and alternative treatment, whereas others began more immediately on their admission. Thus, future study and analysis should consider the impact of longer- versus shorter-term exposure to other treatments in the same therapeutic milieu.
Fourth, the current sample is relatively small, given the number of outcome variables in the analysis. This is compounded by the fact that some cases were dropped from the multivariate analysis for lacking a complete (i.e., 3 years with six data points) data set. Many of the actual decreases in problematic behavior were small, either due to low base rates and aggregation of such decreases, or small though statistically measurable changes in behavior. Results are therefore modest, and we would hope that a larger and more complete data set would allow for a greater understanding of the impact of treatment. Relatedly, although results were statistically significant, the practical significance of a decrease in less than one incident of aggression or sexual offending during a given year is limited. A larger sample with a longer allowable treatment time period would perhaps demonstrate stronger and more observable changes in participants’ outcome behaviors.
A fifth limitation reflects our inability to strictly adhere to and evaluate the effectiveness of the treatment in relation to the principles of Risk-Need-Responsivity. As noted previously, we were unable to assign clients to group conditions on the basis of risk, as all clients in the facility were required to attend sex offender treatment for statutory and administrative reasons. However, although two thirds of the sample presented as low or low-moderate risk on the Static-99R, it is also notable that they presented with greater degrees of impulsivity, psychiatric complexity, and continuing behavior problems, which may in fact speak to other measurable indicators of risk. It is notable that the higher-needs participants (e.g., those who evidenced a greater degree of behavioral instability and aggression prior to treatment) were less likely to engage in treatment. Future study should examine the impact of first module of treatment in addressing motivational issues, as well as specific difficulty in motivating and engaging high-needs and high-risk offenders.
We were better able to assess criminogenic and noncriminogenic treatment needs through the SOTIPS, although this instrument has been primarily normed on correctional and community samples of offenders, rather than a psychiatric or seriously mentally ill population (McGrath et al., 2005; McGrath et al., 2012). Responsivity factors were primarily assessed through treatment attendance and improvement over time, although future studies should incorporate a measure of participant perception of treatment, or observable interactions between participants and treatment providers.
In addition, this study utilized a design that evaluated dose-treatment effects, meaning that participant changes were compared with their own baseline. Treatment effects were seen as a function of percentage of groups attended and time in treatment. The study did not utilize comparison groups, nor did it compare SOS with another available treatment (such a comparison with relapse prevention can be viewed in Stinson, McVay, & Becker, 2016). A stronger treatment design would have utilized randomized controls or a treatment waitlist, although this was not ethically feasible for the current study. Clients in the facility could not be denied treatment, nor were they cognitively able to understand alternative treatment materials, as was made clear by facility administration. Thus, this early attempt to evaluate the effectiveness of SOS based on available baseline data produced modest results suggestive of a dose response effect.
Conclusions and Future Directions
From these findings, we can conclude that SOS did have a positive impact on treatment engagement, behavioral stability, and prosocial beliefs and behaviors among a sample of inpatient psychiatric sex offenders with serious mental illness and intellectual/developmental disabilities, as a function of group attendance over a 2-year period at the initiation of treatment. This treatment targeted self-regulatory ability in these participants, utilizing a manualized, skills-based treatment and strongly emphasizing the needs and responsivity components of the Risk-Needs-Responsivity model. Further research needs to consider the generalizability of these results to other sex offender samples and treatment environments, how these results fare in comparison with samples who have received other treatments, and what the continued effectiveness of SOS would be in this and other samples beyond the first 2 years of treatment.
Footnotes
Acknowledgements
The authors wish to gratefully acknowledge the support of Drs. Anthony Menditto and Marc Maddox in the completion of this pilot project.
Authors’ Note
This study represents a pilot investigation of the effectiveness of a treatment manual that was authored by the first two authors of this manuscript and is commercially available. Financial involvements include royalties payments from the publisher of the text.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.