
Abstract
Current research provides little evidence for the effectiveness of treatment in reducing sexual offence recidivism amongst low-risk populations. However, in real-world correctional settings, program delivery rarely occurs in a vacuum, treatment may be politically mandated and unidimensional measures of program success may preclude recognition of broader benefits. The current study investigated the effectiveness of a low-intensity treatment program, both in terms of participants’ recidivism outcomes and in terms of broader organizational/systems impacts. The results demonstrated low base rate recidivism across both program participants (n = 311) and a comparison group of men who were assessed as demonstrating similar static sexual offence recidivism risk (n = 391), and little evidence of reduced recidivism following treatment. However, program administration led to many potential participants being identified as demonstrating higher levels of dynamic risk and overridden to more intensive treatment options (n = 101). Given evidence that such options do effectively reduce recidivism in higher risk populations, these findings may suggest an overall positive net effect.
The significant personal, social and financial costs of sexual crimes are widely recognised and, over the past few decades, governments around the world have invested heavily in treatment programs that aim to reduce recidivism amongst individuals convicted of such offences. Over the past decade, a series of comprehensive meta-analyses have provided convincing evidence that when delivered in accordance with identified principles of effective correctional interventions (see Bonta & Andrews, 2017), treatment can be effective in reducing sexual offence recidivism (e.g. Hanson et al., 2009). One such principle, and a focus of current paper, is that of risk: Treatment effects are strongest when delivered to individuals with a higher actuarial risk of sexual recidivism relative to individuals with a lower risk. Notwithstanding research suggesting that offence-focussed treatment might fail to produce tangible effects for lower risk groups (Grady et al., 2017; Hanson & Yates, 2013), social and political pressures often prevail, with many jurisdictions offering (or even mandating) treatment to all individuals convicted for sexual offences.
The current study seeks to explore how practitioners and program administrators might balance socio-political pressures with ‘what works’ evidence. Underpinning this exploration, we recognise that in real-world correctional settings, program delivery rarely operates in a vacuum. As such, the impact of offering and administering a program may extend beyond those who participate in it. Therefore, we sought to examine both the extent to which a low-intensity program for men sentenced for sexual offences in New Zealand impacted recidivism outcomes, as well as its broader impact on correctional program administration. The latter included consideration of the impact of assessing and subsequently identifying men in need of more intensive treatment, where previously these men would not have been assessed.
What Works in Sexual Offence Treatment Programming?
Hanson et al’s (2009) meta-analysis of 23 studies found that programs adhering to the risk, need and responsivity principles (RNR; see Bonta & Andrews, 2017) showed the greatest reductions in sexual recidivism. Briefly, the RNR principles state that allocation of treatment resources should be made commensurate with an individual’s recidivism risk, such that individuals who demonstrate the highest level of risk, receive the highest allocation of resources/most intensive treatment programs. They also suggest that treatment programs are most effective when they actively target an individual’s criminogenic needs (factors that contribute to the likelihood of repeat criminal behaviour) and are delivered in a warm and empathic manner that match participants’ personal learning needs.
Several years after Hanson et al., Schmucker and Lösel (2015) found a small but significant overall treatment effect in their meta-analysis of 29 studies with equivalent treatment and control groups (10.1% treated vs. 13.7% untreated). Heterogeneity in treatment effects were observed across studies, including better effects for cognitive behavioural (CBT) and more individualised treatment, as well as treatment targeting individuals assessed in the medium-high risk categories for sexual reoffending. Although Schmucker and Lösel only noted these effects in community-based (as opposed to prison-based) programs, Gannon et al. (2019) recently undertook an updated meta-analysis (including 11 studies published since Schmucker and Lösel’s original meta-analysis) that found significant treatment effects in both settings (sexual recidivism: 9.5% treated vs 14.1% untreated, average follow-up 6.4 years). Further, Gannon et al.’s meta-analysis was the first such study to specifically consider staff and program variables as predictors of treatment effectiveness. They found that treatment was most effective when it was consistently facilitated by a qualified, licenced psychologist, when treatment staff were supervised by licenced psychologists, when sessions were group-based and some form of arousal reconditioning was included and when polygraph testing was absent.
As awareness of the potential benefits of sexual offence treatment programs has increased, so too has public and political pressure for them to be offered to all individuals who are convicted for sexual offences (e.g. Burdon & Gallagher, 2002; Harris & Hanson, 2004; Ward & Stewart, 2003). However, the extant literature suggests that not all such individuals are equally likely to benefit from these programs. As suggested by the RNR risk principle (see Bonta & Andrews, 2017), intensive treatment services are most likely to reduce recidivism amongst individuals who demonstrate a higher risk of recidivism as measured by actuarial instruments. Schmucker and Lösel’s (2015) meta-analysis found no significant effect of treatment for men assessed in the low-risk category based on static risk tools. In the case of the meta-analyses undertaken by Hanson et al. (2009) and Gannon et al. (2019), no conclusions could be made about the effectiveness of treatment based on actuarial risk as few of the studies they considered were coded for participant risk.
What Constitutes Low Risk?
Risk of sexual offence recidivism is generally understood as the relative likelihood that an individual who has been convicted of a sexual offence will be reconvicted of such an offence within a specified time period. It is usually assessed through use of one or more validated assessment instruments that have been developed from studies that quantitatively link specific participant behaviours and characteristics (risk factors) to re-offence rates. Risk factors may be either static (unchangeable) or dynamic (changeable; also referred to as criminogenic needs). The five-level risk and needs system developed by the Justice Centre of the Council of State Governments to standardise risk communication describes individuals assessed with the lowest risk for reoffending (Level I; very low risk) as having ‘…few, if any, identifiable criminogenic or noncriminogenic needs’ (Hanson et al., 2017a). As such, these men do not demonstrate characteristics such as general and sexual self-regulation difficulties and relational difficulties, that have been shown to increase the likelihood of sexual offending (e.g. Mann et al., 2010). Hanson et al. (2017b) argue that ‘…they are psychologically and socially similar to people without a criminal record’ and that their risk of recidivism is ‘no different from the rate of spontaneous, first-time offending for people without a criminal record…’ (p. 7). Similarly, although individuals assessed in the second lowest risk category (Level II, below average risk) may have one or two identifiable criminogenic needs, their recidivism risk remains much lower than that of men who have been convicted of sexual offences and assessed as demonstrating an average (Level III) or higher risk (Level IVa or IVb) of sexual recidivism (Hanson et al., 2017a).
In an aggregated sample of 7740 men with convictions for sexual offences, Hanson et al. (2014) found that the 15 year sexual recidivism rates of those whose static risk score was one standard deviation below the mean was 2.9%. This rate is similar to the rate of spontaneous sexual offences that Kahn et al. (2017) identified among individuals convicted for nonsexual offences over a 5-year follow-up period (1–2%). Given that the men in Hanson et al.’s study had been in the community three times as long as those considered by Kahn et al., these results suggest that there may be no greater rationale to offer sex-offence-specific treatment to men identified as being of low risk of sexual recidivism than there is to offer it to men convicted for nonsexual offences (Hanson et al., 2018). From the perspective of risk management, Hanson et al. (2018) suggested that ‘resources that may be spent on these very low risk…[clients] would be better spent on higher risk…[clients], prevention of sexual crime, and victim services’ (p. 49).
Treatment Outcomes for Men Assessed in Low-Risk Categories for Sexual Reoffending
Few studies have examined effects of psychological treatment for men assessed in low-risk categories for sexual reoffending specifically. A null treatment effect was reported by Grady et al. (2017) following their longitudinal outcome evaluation of 256 individuals who were classified as being of low static sexual offence recidivism risk and participated in the Sex Offender Accountability and Rehabilitation (SOAR) Program in the North Carolina Division of Adult Corrections and Juvenile Justice. Grady et al. (2017) found no difference in rates of recidivism for sexual or violent crimes between these men and matched controls who did not participate in the program. They did, however, find a significant reduction in nonviolent recidivism amongst men who completed the SOAR program. Similarly, in their long-term assessment of the effects of a prison-based CBT/RNR treatment program for men who had been convicted for sexual offences, Olver et al. (2020) found no differences in the sexual recidivism outcomes of low-risk participants in treatment and nontreatment groups. However, they noted significantly lower rates of violent recidivism amongst low-risk men who participated in treatment.
Other research has shown that in some circumstances, sex-offence-specific treatment of low-risk men may actually increase their recidivism risk. For example, Makarios et al. (2014) found that although increasing treatment dosage significantly reduced recidivism for men assessed as being of medium-high sexual offence recidivism risk, it had the reverse effect for those assessed in lower risk categories. Similarly, Lovins et al. (2009) found that intensive treatment of lower risk men, delivered during residential placement in a halfway house, was associated with an increased rate of sexual recidivism. They suggested that such treatment, and the context in which it was delivered, may have served to further disrupt the prosocial networks and opportunities of lower risk participants and potentially reinforced social learning of antisocial behaviour.
With minimal opportunity for treatment to influence already low recidivism base rates, together with the possibility that in some circumstances it may actually increase recidivism, it is not surprising that extant research does not support offence-specific treatment for individuals assessed with a low risk of sexual offence recidivism. However, external pressures (including social and political) often compel correctional services to offer offence-focused treatment to low-risk groups (Burdon & Gallagher, 2002; Harris & Hanson, 2004; Ward & Stewart, 2003). Moreover, it is important to acknowledge that reliance on officially recorded recidivism data underestimate true rates of sexual recidivism. Given that low base rates for sexual recidivism limit our ability to statistically detect significant changes, increasing these to reflect actual recidivism could increase the power of our analyses and the likelihood that effects would be detected. Thus, treatment programs for low-risk men might have effects that research fails to detect, but that would be detected if actual recidivism was assessed.
In addition, heterogeneity exists within groups assessed in lower risk categories, especially when risk assessments are based solely on static, unchangeable risk factors (as is often the case when allocating individuals to treatment). Indeed, although research undertaken by Hanson et al. (2017a) found that men assessed in lower static risk categories tended to demonstrate fewer criminogenic needs than those assessed in higher risk categories, approximately 25% of low-risk men were found to demonstrate one or more criminogenic needs (most commonly, sexual preoccupation). Thus, within groups of men assessed with a low static risk of sexual reoffending, some may present with ongoing criminogenic needs (dynamic risk factors) signalling potential treatment needs. Unfortunately, few other studies have considered the dynamic risk profiles of men assessed as low risk using static measures and there is little evidence in the relevant literature that dynamic risk is routinely screened in lower static risk populations. As such, men in these populations tend to be treated homogenously when it comes to decisions about treatment delivery.
Although limited research exists to inform best practices for men assessed in the below average or very low sexual recidivism risk categories, researchers tend to converge on the recommendation that planning for community reintegration is a more appropriate treatment goal than risk reduction (Hanson et al., 2009; Wakeling et al., 2012).
The Short Intervention Program (SIP) in New Zealand
In an effort to balance political pressure for treatment of all individuals convicted of sexual offences and the criminogenic needs of those individuals, in 2012 the New Zealand Department of Corrections introduced a Short Intervention Program (SIP) for men who are sentenced for sexual offences against children and assessed as low (0) or medium-low risk (1) of sexual recidivism using the Automated Sexual Recidivism Scale (ASRS) static risk assessment tool. In New Zealand, the 5 year recidivism rates for men assessed in the low risk (ASRS = 0) and medium-low risk categories (ASRS = 1 or 2) using the ASRS are 2% and 7%, respectively (Grace & Wilson, 2018). Prior to the introduction of the SIP, men with an ASRS score of 0 or 1 were not offered any sexual offence-focused interventions, and men with an ASRS score of 2 or above were assessed for high-intensity treatment. Now, all men with an ASRS score of 0 or 1 are waitlisted for the SIP 1 . As waitlisted men approach the end of their prison sentences, they are screened for denial and other factors perceived to reduce their SIP suitability (e.g. physical health problems prohibiting a prison transfer). Men considered suitable who acknowledge at least some aspects of their offending are then voluntarily transferred to a treatment unit offering the SIP where they participate in a more comprehensive assessment including dynamic risk (originally Stable-2007, now VRS-SO) before beginning the SIP. The results of the dynamic risk assessment are then used to inform clinical decision making regarding whether or not each man is placed in the SIP or diverted to more intensive treatment options.
As stated in the SIP program delivery manual (Mattson, 2012), the SIP has two primary aims: (i) for each participant to develop an ‘adequate understanding of their offence process’ and (ii) for each participant to ‘develop a safety plan that mitigates any remaining risk factors’ (p. 2). In turn, intervention content and delivery are primarily informed by the relapse prevention model. Although the SIP program delivery manual also discusses other treatment approaches including the strengths-based Good Lives Model (Ward & Stewart, 2003), the time available (<100 hours) limits the extent to which therapists can apply the GLM in practice. Similarly, while dynamic risk factors for sexual reoffending are assessed, opportunities for addressing associated criminogenic needs tend to be limited to brief exploration of offence-supportive cognitions and lifestyle factors identified in the offence chain and safety planning assignments.
Aims of the Current Research
This article grew out of a SIP evaluation commissioned by the New Zealand Department of Corrections. In planning the evaluation, it was recognised that in any program delivered by a large government agency with responsibility for managing the needs and influencing the outcomes of multiple diverse clients, the question of program success must necessarily expand beyond conventional forensic research considerations such as participant recidivism rates. Therefore, the purpose of the current research was not to evaluate the SIP program per se, but rather to evaluate its effectiveness as a means for the New Zealand Department of Corrections to balance its obligations to meeting both political (i.e. offering treatment to all clients) and client needs (offering treatment that benefits clients and communities). To this end, we considered outcomes of SIP screening and assessment, as well as SIP participation. As such, the aims of our research were: (a) To consider the impact of offering and administering the SIP on broader correctional program administration and client responsivity, including the extent to which post-waitlist assessment of potential SIP participants’ dynamic risk factors led to men being identified as needing more intensive treatment and diverted into it. (b) To assess the impact of SIP participation on participants’ recidivism outcomes.
This focus is wider than many treatment program evaluations, and necessarily so. As much as government departments (or their staff) might sometimes wish to operate in isolation from political pressures, public funding means that is not possible. Similarly, as much as researchers might want to view the treatment programs operated through those departments in isolation, that is not usually how they work. Rather, they are influenced by and influence a range of broader organisational practices and, therefore, the net effect of a program is unlikely to be limited to those who participate in it. Indeed, it is because of these influences that narrower, treatment-only focused evaluations often struggle to meet Collaborative Outcome Data Committee (Collaborative Outcome Data Committee, 2007) criteria for effective evaluation of treatment research, particularly in terms of comparison group equivalence. Certainly, the current research also struggled in this regard (Appendix A provides a review of the current study against CODC guidelines). However, rather than viewing the differences that we identified between the treated and untreated group as a limitation, we considered the influence that SIP program administration (including post-waitlist assessment of dynamic risk) had on creating them and the broader system-based effects that flowed from them.
Given the two-fold aims of this study, the research was undertaken in two stages. Stage one involved analysis of the program administration process, and stage two involved evaluation of the impact of program participation on recidivism outcomes. For ease of reading, each of these stages is discussed separately in the following sections of this article.
Method
Stage 1: Analysis of the Program Administration Process (including assessment)
Participants
For the purpose of analysing the impact of offering and administering the SIP program, we sampled all men convicted for a child sexual offence with an ASRS score of 0 (low risk) or 1 (moderate-low risk) and waitlisted for SIP groups from the inception of the program in February 2012 up to and including August 2018 (N = 823). In September 2018, the ASRS-R replaced the ASRS to waitlist men for the SIP. The ASRS-R incorporates age weights to account for the established relationship between advanced age and desistance from offending (Helmus et al., 2012). Accordingly, from September 2018, it is likely that older men who would have previously been waitlisted for more intensive treatment on the basis of their ASRS scores (which does not take advanced age into account) were instead waitlisted for the SIP. In the interests of analysing a comparable group of SIP participants (and for identifying a comparison group on the basis of ASRS scores in the evaluation of participant outcomes), men waitlisted for SIP groups from September 2018 onwards were excluded from the current evaluation.
Men waitlisted for the SIP program ranged in age from 17–89 years (M = 45.5, SD = 15.3). The recorded ethnicity for the majority of these men was New Zealand European (n = 483, 58.8%), followed by New Zealand Māori (n = 196, 23.8%), Pacific peoples (n = 109, 13.3%), Asian (n = 23, 2.8%) and other ethnic groups (n = 8, 1.0%).
Measures
Automated Sexual Recidivism Scale (ASRS): The ASRS is a measure of static risk, derived from the Static-99 (Hanson & Thornton, 1999) and scored based on information available in electronic records maintained by the New Zealand Department of Corrections. It includes seven of the 10 Static-99 items (young, index nonsexual violence – any convictions, prior nonsexual violence – any convictions, prior sex offences, prior sentencing dates, noncontact sex offences – any convictions, any male victims) and has demonstrated comparable predictive validity to the Static-99 for sexual recidivism in a New Zealand sample (Skelton et al., 2006). Validation of the ASRS was undertaken through 5-, 10- and 15-year follow-up of all men who had been convicted of sexual offences and released from New Zealand prisons during 1998, 1992 and 1987, respectively. For the 5 year cohort, the resulting ROC area under the curve figure was 0.78, for the 10-year cohort it was 0.75 and for the 15-year cohort it was 0.70 (Skelton et al., 2006). Skelton et al. (2006) noted consistency between the observed ASRS recidivism rates and those reported in the initial Static-99 validation study undertaken by Hanson and Thornton (2000). They also reported clear differences in the rates of survival to sexual reoffending for men classified in each of the ASRS risk categories: high-, medium-high-, medium-low- and low-risk.
Stable-2007: The Stable-2007 (Fernandez et al., 2014; Hanson et al., 2007) is a measure of dynamic risk factors that assesses significant social influences, intimacy deficits (capacity for relationship stability, emotional identification with children, hostility toward women, social rejection/loneliness and lack of concern for others), general self-regulation (impulsivity, poor cognitive problem solving and negative emotionality/hostility), sexual self-regulation (sex drive/preoccupation, sex as coping and deviant sexual interests) and cooperation with supervision. A recent meta-analysis found that the Stable-2007 demonstrated incremental predictive validity for sexual recidivism when used alongside the Static-99 (Brankley et al., 2021). The Stable-2007 risk categories were used to assess dynamic risk for men assessed for the SIP from its inception in 2012 until early 2016. Risk categories were favoured over total numerical scores because the former were more commonly included in the dataset provided by the Department of Corrections.
Violence Risk Scale-Sexual Offense version (VRS-SO): The VRS-SO (Wong et al., 2003-2017) replaced the Stable-2007 for men assessed for the SIP from 2016. The VRS-SO includes static and dynamic risk scales as well as structured ratings of treatment related change. The current study considered the total (prestandardised) Pretreatment Risk categories rather than the Pretreatment Dynamic Risk scores or total risk scores (Olver et al., 2018). The categories were used because these were provided for most men who commenced the SIP between February 2016 and August 2018, whereas the scores were only provided in a subset of cases. Although it would have been preferable to focus specifically on the dynamic risk scores, use of the total risk categories was accepted on the basis that all men waitlisted for the SIP had already been assessed as demonstrating low static risk using the ASRS, the VRS-SO static risk items are generally comparable to the ASRS items, and (as indicated by the overlap between ASRS and Static-99 items) the ASRS and VRS-SO static items show similar predictive accuracy (Olver et al., 2016). Therefore, any additional risk identified through VRS-SO assessment was most likely due to dynamic factors.
Procedure and Planned Analyses
The second author was provided with a list of men who were waitlisted for the SIP between its inception in February 2012 and August 2018. SIP commencement dates were provided for men accepted into the SIP; otherwise, a code corresponding with a reason for a man’s removal from the waitlist was provided. Eight reasons for removal were provided: override to higher intensity treatment program, override to individual treatment or completed approved individual treatment, override to other (e.g. adult sexual offending treatment program), completed suitable treatment program, unsuitable for a permanent reason (e.g. chronic physical health problems), out of time (generally due to client being released before commencing the SIP), denial of offence and no treatment, or deceased. Ambiguous entries were clarified with administrative staff at the relevant prison treatment unit. Risk assessment scores for men assessed for the SIP were extracted from electronic records at a Department of Corrections office.
Our analysis of the SIP program administration process involved generating frequency data for waitlist withdrawals and comparing dynamic risk assessment categories for men assessed for the SIP who commenced the SIP versus men who were overridden to more intensive treatment.
Stage 2: Evaluation of SIP Participants’ Recidivism Outcomes
Participants
ASRS Scores for SIP Completers.
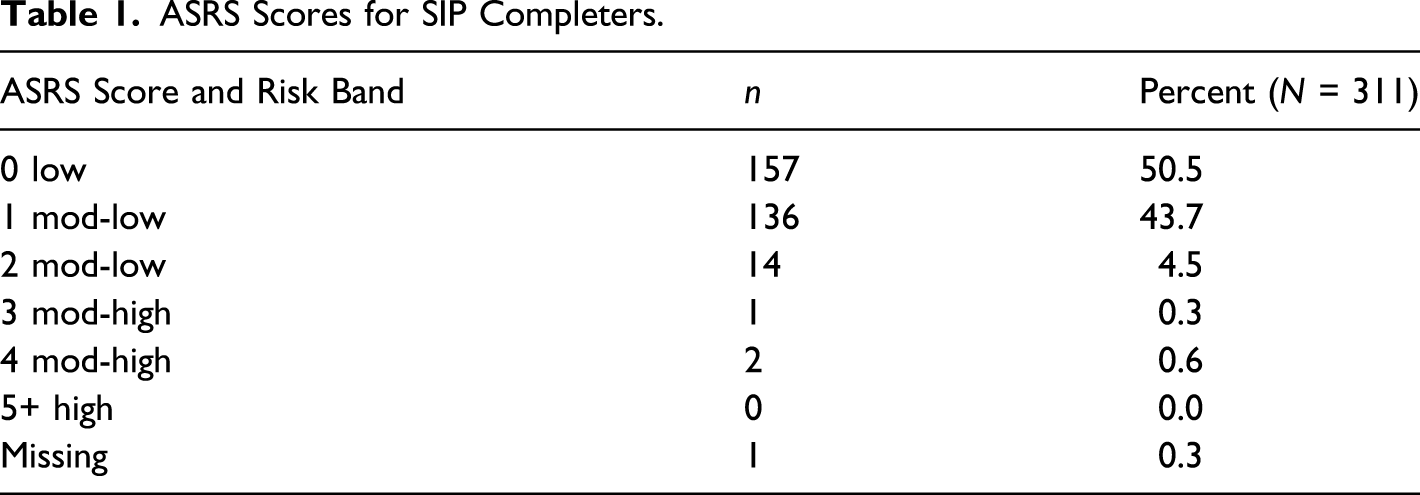
Recidivism outcomes of men who completed the SIP were compared to the recidivism outcomes of men in a comparison group. The comparison group was drawn from all men imprisoned for a child sex offence in New Zealand before the introduction of the SIP who did not complete a sexual offence treatment program and for whom ASRS scores were available 2 . Only those men with an ASRS score of 0 or 1 were included, resulting in a final comparison group sample of 391 men. Men in the comparison group ranged in age from 18 to 88 years (M = 41.51, SD = 14.74). Most identified as New Zealand European (n = 203, 51.9%), followed by New Zealand Māori (n = 95, 24.3%), Pacific peoples (n = 75, 19.2%) and other ethnic groups (n = 16, 4.09%). Ethnic identity was unspecified for two men in the comparison group (0.5%). ASRS scores for men in the comparison group were 0 (n = 199, 50.9%) or 1 (n = 192, 49.1%) (M = 0.49, SD = 0.50). Independent samples t-tests revealed no statistically significant differences between the mean age or ASRS scores of men in the SIP completers group who had been released for at least 15 months and men in the comparison group (t(692) = 1.420, p = 0.156, d = 012; t(562.986) = 1.626, p = 0.105, d = 0.11, respectively). Similarly, tested against a Bonferonni adjusted alpha level of 0.006 (0.05/8), chi square analysis revealed no significant differences between the ethnic identity of SIP completers and comparisons (Māori: χ2 (1) = 0.009, p = 0.925, v = 0.01; Pacific peoples: χ2 (1) = 6.366, p = 0.012, v = 0.24; European: χ2 (1) = 5.570, p = 0.018, v = 0.12; Other: χ2 (1) = 1.239, p = 0.266, v = 0.23).
Given that psychological assessments for men assessed in the low-risk category based on ASRS score were only introduced with the introduction of the SIP, dynamic risk categories and information pertaining to offence denial were unavailable for men in the comparison group.
Measures
Reoffenses: A list of conviction dates for sexual, nonsexual violent and general offending occurring after an individual’s actual release date were provided by the Department of Corrections. Reoffenses were coded as a dichotomous (yes/no) variable for each type of reoffending, as well as for any reoffending.
Parole breaches: A list of dates of parole breaches occurring between an individual’s actual release date and sentence end date were provided by the Department of Corrections. Breaches were recorded as a dichotomous (yes/no) variable. Some breaches occurred in the context of a reoffense and were coded both as a breach and a reoffense.
Procedure and Planned Analyses
Following our analysis of the SIP administration process, the data pertaining to SIP completers were merged with the comparison group data. Release dates and recidivism data (parole breaches and reconvictions) were provided by the Department of Corrections for both groups, and data were then anonymised. Data were analysed using SPSS (version 25).
Evaluation of SIP participant outcomes involved comparing recidivism outcomes of the men who completed the SIP and the men who comprised the comparison group. In view of the reported low rate of sexual recidivism amongst individuals classified as low risk, we first considered the absolute rate of recidivism across the SIP completers and comparison groups, including recidivism across all offence types and breaches, and recidivism within offence types (sexual, nonsexual, violent and other) and breaches. However, given substantial variation in the follow-up times between men in the SIP completers (M = 46.53 months, SD = 19.15 months) and comparison groups (M = 100.18 months, SD = 6.35 months), absolute recidivism was not used to assess the impact of the SIP on recidivism. Rather, treatment effectiveness was assessed using Cox Proportional Hazards Regression analysis to compare time between release and reoffense for men in the SIP versus comparison group.
Separate Cox Proportional Hazards Regression analyses were conducted for each recidivism outcome (sexual, nonsexual violent, other and breach) as well as any recidivism (reoffense or breach). The exponents (hazard ratio) of these analyses may be interpreted as the extent to which treatment increased or reduced the likelihood of recidivism at any given point of time following release. As such, an Exp(B) hazard ratio of 0.5 would suggest that participation in the SIP halves the rate of recidivism compared to the comparison group. Alternatively, an Exp(B) hazard ratio of 2 would suggest a recidivism rate twice that of the comparison group. This research was reviewed and approved by a University Human Ethics Committee (equivalent of a North American Institutional Review Board).
Results
Stage 1: Analysis of the Program Administration Process
Reasons for Removal from the SIP Waitlist.

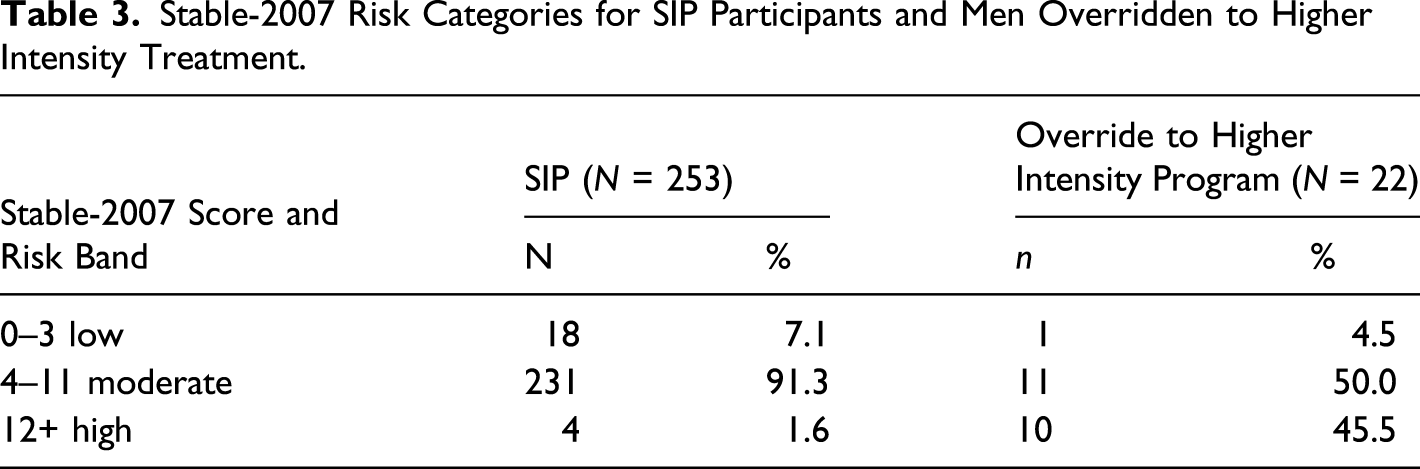
Stable-2007 Risk Categories for SIP Participants and Men Overridden to Higher Intensity Treatment.
VRS-SO Pretreatment Risk Categories for SIP Participants and Men Overridden to Higher Intensity Treatment.

As indicated in Tables 3 and 4, an increased proportion of men appear to have been overridden to higher intensity programs following the introduction of the VRS-SO. Although discussion of this finding is beyond the scope of the current article, it may be at least partly due to the greater sensitivity of the VRS-SO as a dynamic measure of sexual offence recidivism risk (Eher et al., 2015).
Stage 2: Evaluation of SIP Participants’ Recidivism Outcomes
Absolute recidivism by group
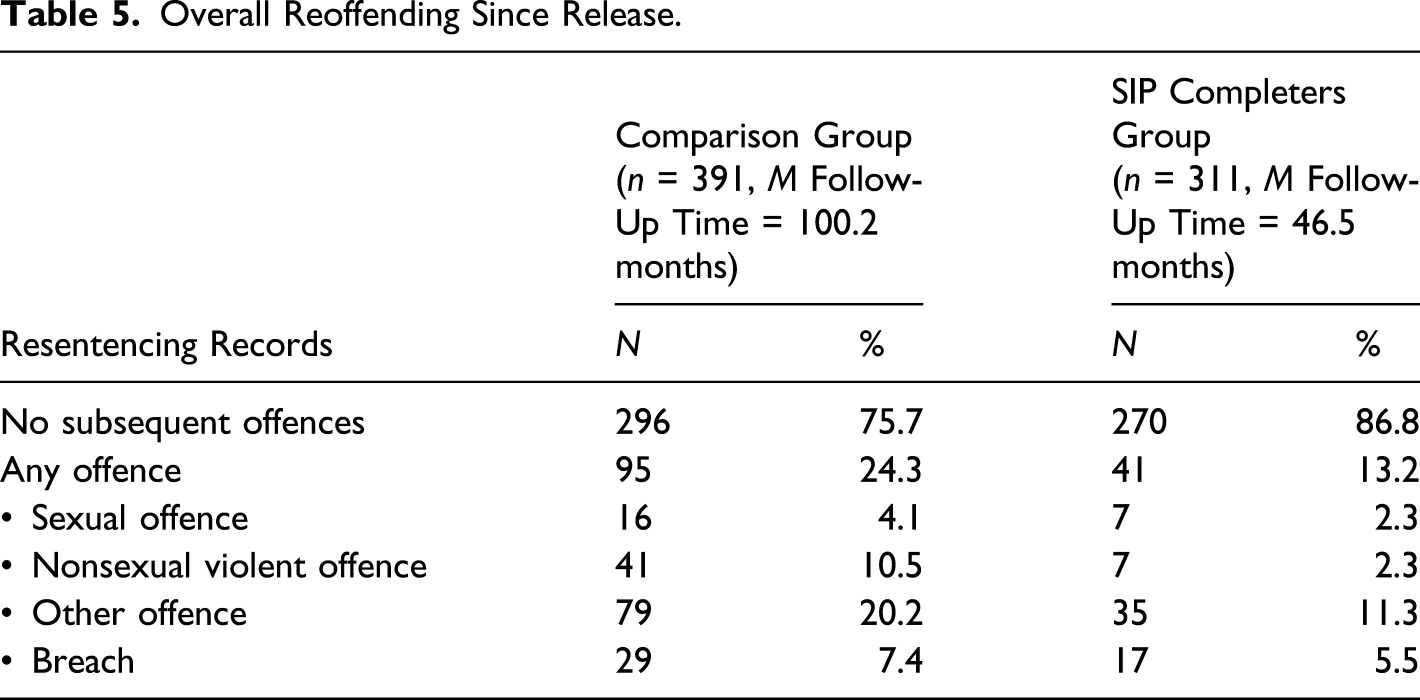
Overall Reoffending Since Release.
Relative Recidivism over Time
As shown in Figure 1, as time since release increased, SIP completers appeared slightly less likely than men in the comparison group to be reconvicted for a sexual offence. However, Cox regression analysis indicated that the size of this effect was small
4
(Exp(B) hazard ratio = 0.729) and revealed no statistically significant differences between SIP completers and comparison group member’s likelihood of sexual recidivism (95% CI [0.296, 1.799], p = 0.493). Survival function for months to sexual offence (Exp(B) hazard ratio = 0.729 (95% CI [0.296, 1.799], p = 0.493). Note. 23/702 men had committed a new sexual offence during the follow-up period.
As shown in Figure 2, our analyses did reveal a reduced likelihood of nonsexual violent offence recidivism for SIP completers (Exp(B) hazard ratio = 0.352 (95% CI [0.155, 0.800], p = 0.013). Inverting the associated hazard ratio suggests a moderate to large effect such that, at any given time during the follow-up period, men in the comparison group were 2.8 times more likely than men who completed the SIP to commit a nonsexual violent offence. Survival function for months to (nonsexual) violent offence (Exp(B) hazard ratio = 0.352 (95% CI [0.155, 0.800], p = 0.013). Note. 48/702 men had committed a new (nonsexual) violent offence during the follow-up period.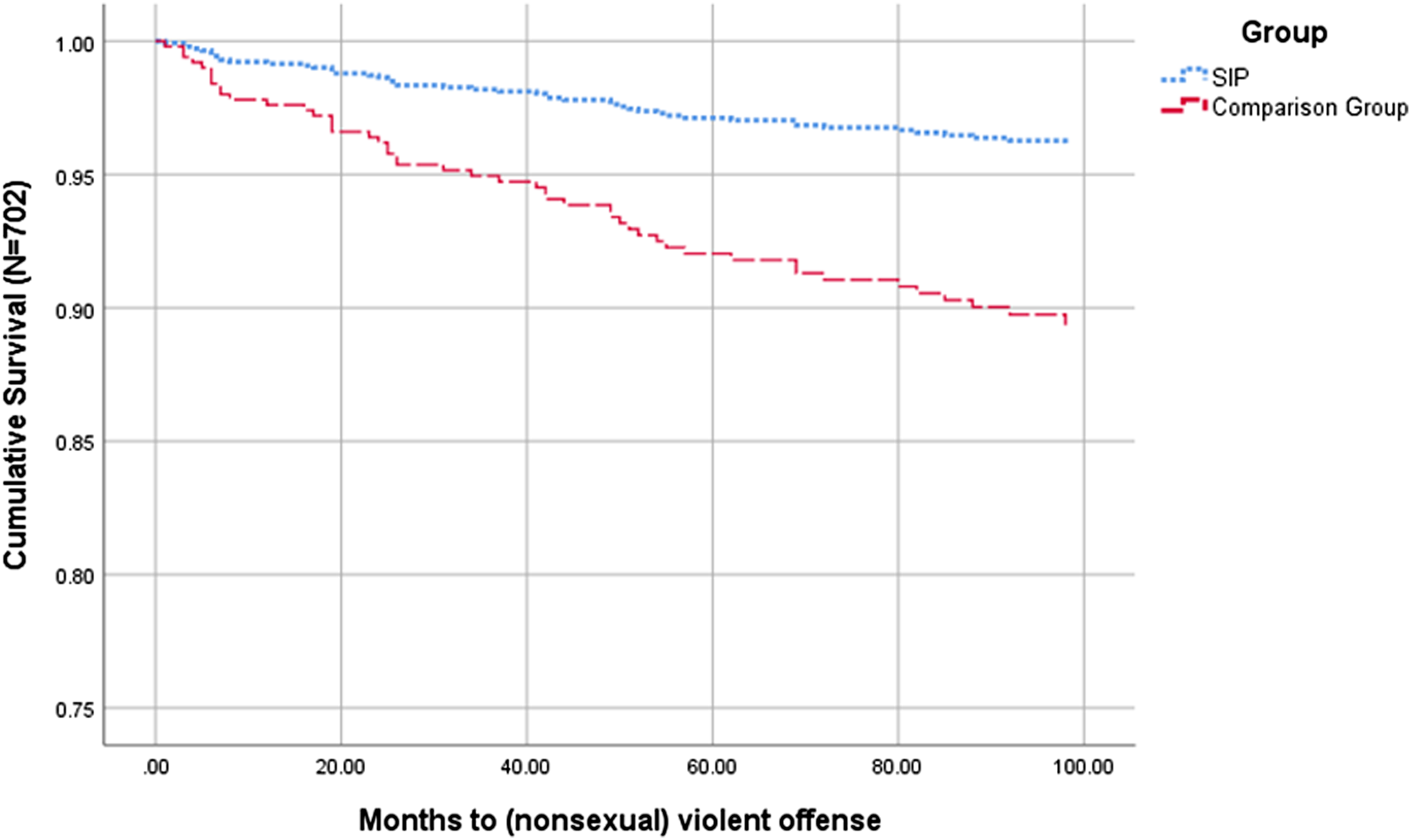
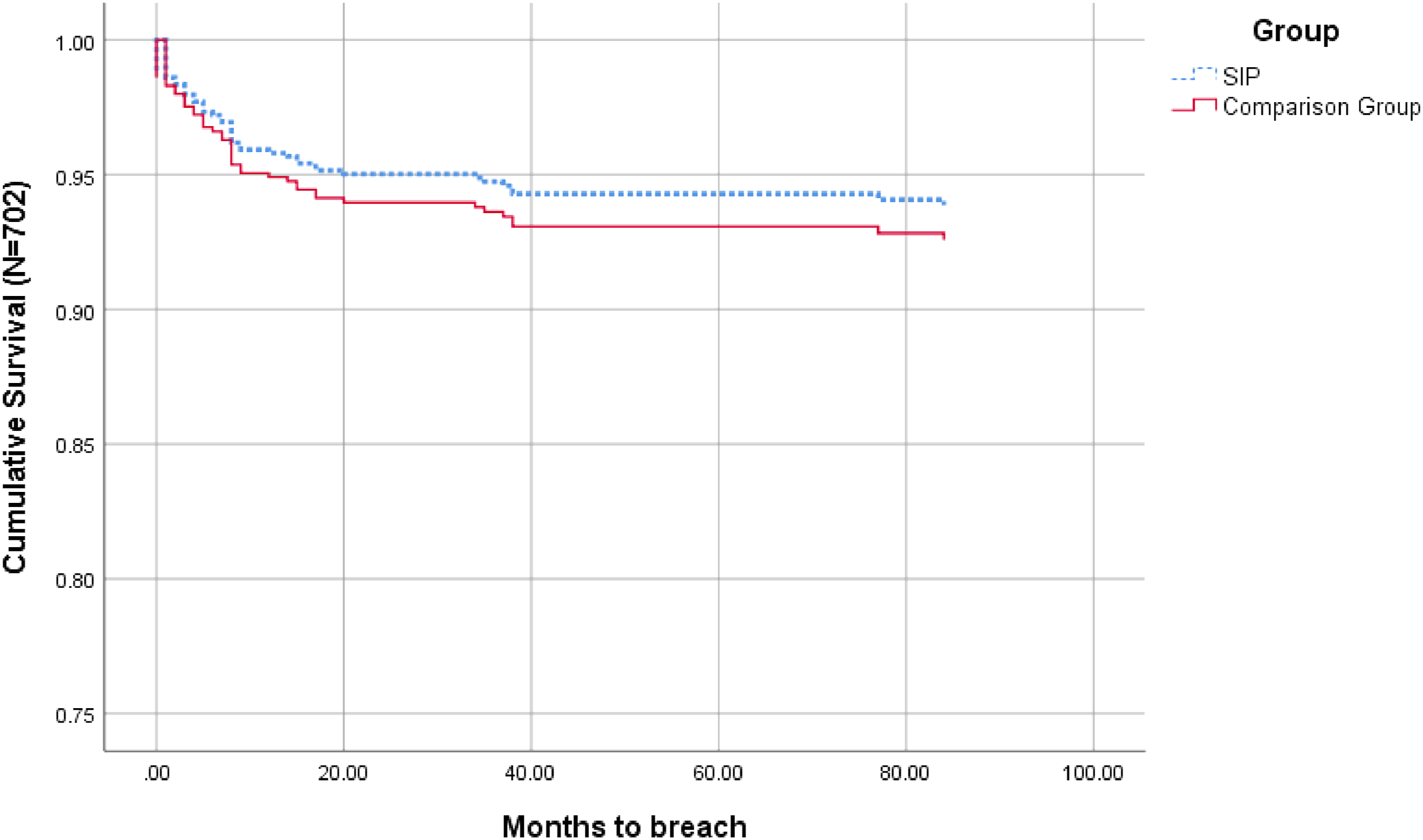
The direction of the findings from Cox Regression analyses comparing SIP completers and comparison group member’s other (nonviolent, nonsexual) recidivism outcomes (Exp(B) hazard ratio = 0.732 (95% CI [0.487, 1.101], p = 0.134), breaches (Exp(B) hazard ratio = 0.820 (95% CI [0.447, 1.506], p = 0.523) and any recidivism or breach outcomes (Exp(B) hazard ratio = 0.719 (95% CI [0.494, 1.047], p = 0.085) were also such that SIP completers appeared to demonstrate reduced likelihood of offending across time. However, these effects were small and no statistical differences were found between associated recidivism outcomes for SIP completers and men in the comparison group (Figures 3–5). Survival function for months to other offence (Exp(B) hazard ratio = 0.732 (95% CI [0.487, 1.101], p = 0.134). Note. 114/702 men had committed a new other offence during the follow-up period. Survival function for months to breach (Exp(B) hazard ratio = 0.820 (95% CI [0.447, 1.506], p = 0.523). Note. 46/702 men had committed a breach during the follow-up period. Survival function for months to any recidivism (Exp(B) hazard ratio = 0.719 (95% CI [0.494, 1.047], p = 0.085). Note. 136/702 men had committed any offence or breach during the follow-up period.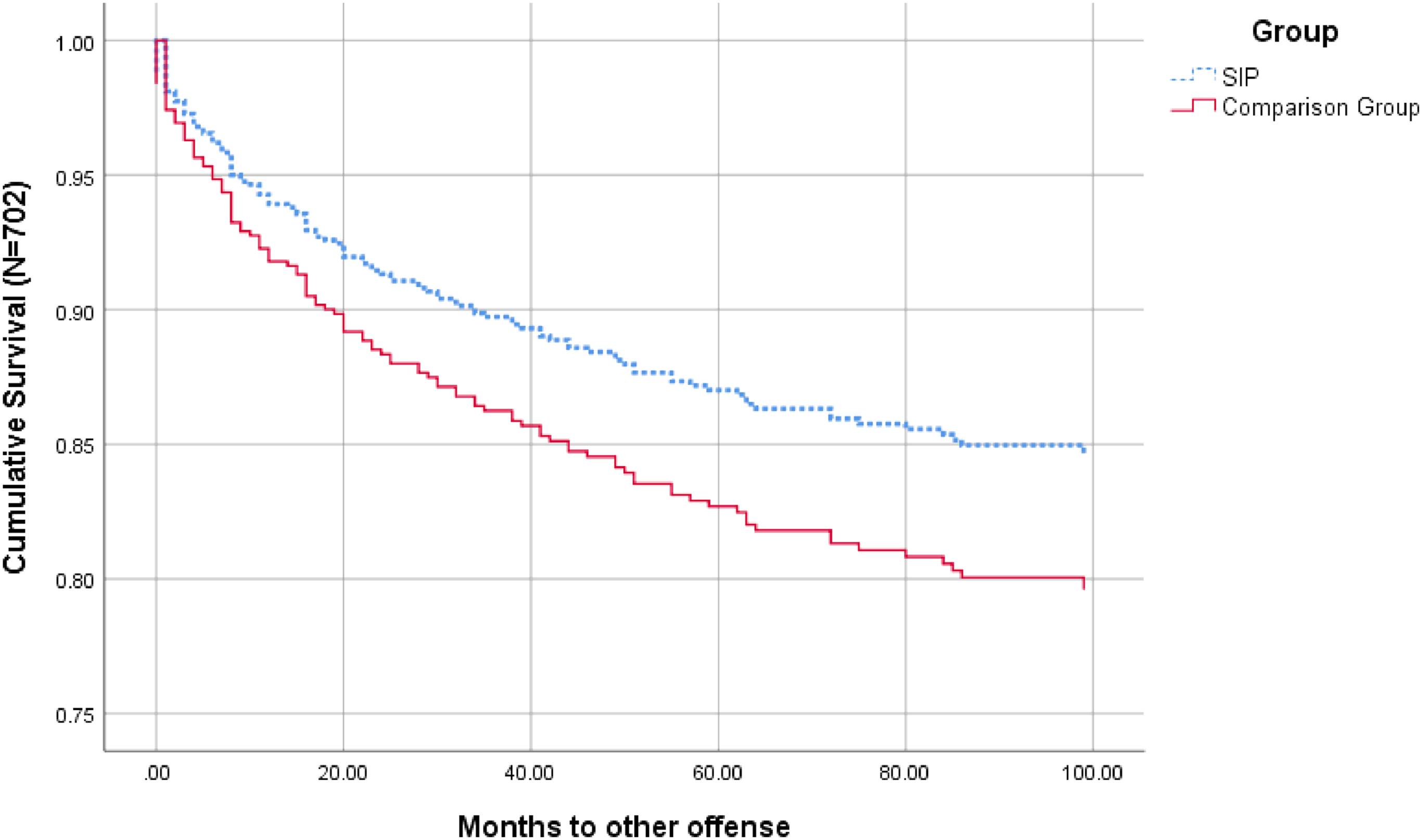

Discussion
Findings from the current research suggest that, in addition to demonstrating the New Zealand Department of Corrections responsiveness to political demands, provision of the Short Intervention Program (SIP) may also be enhancing its responsiveness to clients and contributing to increased community safety, albeit not always in ways that involve SIP completers. As a result of the assessment processes introduced as part of the SIP administration, many of the men who were initially identified as demonstrating low static risk were found to also demonstrate high dynamic risk. In turn, these men were overridden to higher intensity treatment programs. Given the evidence supporting the effectiveness of high-intensity treatment programs in reducing recidivism in higher risk populations (e.g. Gannon et al., 2019; Hanson et al., 2009; Schmucker & Lösel, 2015), this process may have contributed to reducing net recidivism across the waitlisted group and, by default, increasing public safety. Withdrawal of men who demonstrated higher dynamic risk from the SIP program may also have reduced SIP completers exposure to associated criminogenic influences; thus reducing the potential for SIP completers to be negatively affected by these influences.
Notably, these benefits were only identified because we expanded our research focus to include not only the impact of program participation on recidivism outcomes but also the impact of offering and administering the SIP on broader correctional program administration and client responsivity. This focus was broader than many treatment program evaluations and explicitly acknowledged that treatment programs offered through government agencies rarely operate in a vacuum. Rather, they are influenced by and influence a range of broader organisational practices. Although these influences have the potential to undermine comparison group equivalence and are often viewed as a limitation of treatment-only focused evaluations (e.g. Collaborative Outcome Data Committee, 2007), we considered that they may also serve to increase the effect of a program beyond its participants. Findings highlighted broader client benefits of the SIP that might not have been recognised if we had only focused on the impact of program delivery. That said, they also suggest that if all clients were routinely screened for both static and dynamic risk factors prior to being waitlisted for programs, these benefits could be as effectively realised in the absence of SIP delivery.
Results suggested that the SIP had little (if any) impact on participants’ risk of recidivist sexual offending. Further, although the data suggested a (nonsignificant) trend for SIP completers to demonstrate lower levels of postrelease sexual recidivism than men in the comparison group, this could be at least partly explained by exclusion of men who demonstrated more than moderate levels of dynamic risk and/or who denied their offences, from SIP participation. Consistent research has demonstrated that higher dynamic risk scores are associated with increased risk of sexual recidivism, above that measured by static risk alone (van den Berg et al., 2018). Further, although the relationship between denial and recidivism risk is somewhat debated (Harkins et al., 2015), there is some evidence that when interacting with low static risk, denial may increase the likelihood of recidivism (Harkins et al., 2010). While no data were available regarding the dynamic risk profiles of men in the comparison group, it is reasonable to assume that without further screening beyond static risk, at least some of them may have demonstrated more than moderate dynamic risk. Similarly, some of them may have denied their offences. In turn, these factors may have biased the comparison group to increased sexual recidivism outcomes.
Notably, recidivism amongst men in both the SIP completers and comparison group most commonly involved nonsexual offences. Further, the results suggested that completion of the SIP contributed to a significant decrease in nonsexual violent recidivism amongst participants. These findings align with those of Olver et al. (2020). They also appear to support Hanson et al.’s (2018) suggestion that men in the lowest static risk categories may not be differentiable in terms of sexual recidivism risk from individuals convicted for nonsexual offences. In line with their argument that sexual offence-focused treatment was unlikely to have any effect on men in the lowest recidivism risk groups, our results beg the question of whether the resources dedicated to this treatment program might be more effectively used. As much as the Department of Corrections is subject to external pressures to deliver treatment to men convicted of sexual offences, it is also subject to pressures to ensure that this treatment is evidence based (e.g. Department of Corrections, 2009). Within this context, Simourd and Olver (2019) argue that the question of treatment may relate less to whether and how much treatment is needed and more to the specific criminogenic needs that it is aiming to address and how these can these best be met.
As stated above, one of the benefits of SIP administration was that men with higher levels of dynamic risk were identified and overridden into more intensive treatment programs. This aligns with the RNR principles, treatment-based application of which have been reliably shown to yield the best treatment outcomes in terms of reducing sexual recidivism (Hanson et al., 2019). However, as shown by Andrews and Dowden (2006), these outcomes are only likely when treatment intensity is paired with treatment content that specifically targets the criminogenic risk factors identified through dynamic risk assessment. In line with this, Simourd and Olver (2019) argue that, for treatment to be effective, it needs to focus on assisting clients to acquire skills to address their criminogenic needs. However, as suggested by the low static and dynamic risk scores of the participants who remained in the SIP, most of them demonstrated few (if any) such needs. Further, although men who were overridden to more intensive programs demonstrated more needs, the dynamic risk scores of approximately half of them remained in the average or moderate range (and their ASRS static risk scores remained low). Relevant dosage literature suggests that clients who conform to this profile may be best served by programs that range from between 80 to 150 hours in intensity (Bourgon & Armstrong, 2005; Day et al., 2019). Therefore, it may be that these clients could actually have gained more benefit by remaining in the SIP, while those who actually remained might have benefited from an even less intensive (and more cost effective) intervention. Such an intervention could have focused less on clients developing an understanding of their sexual offence process and mitigating (likely limited) risk factors, and more on preventing risk associated with nonsexual criminogenic factors (e.g. violence) and/or planning their community reintegration. Adopting this approach would balance the evidence against providing sexual-offence-specific treatment to clients identified as having a very low risk of recidivism against political pressures to provide treatment to reduce these clients’ likelihood of returning to prison. These findings also reinforce the need to ensure that effective assessment of both static and dynamic risk, including identification of specific criminogenic needs, is undertaken prior to treatment planning and used to inform it.
Limitations
The current study was subject to several limitations. Perhaps most notably, was our inability to ensure dynamic risk and denial status equivalence between the SIP completer and comparison groups. As discussed above, it seems likely that the comparison group included men with higher dynamic risk profiles than the SIP completers group which may have contributed to or explained the trend in lower recidivism for the SIP completers versus comparison group. However, as this trend did not reach significance, its impact on our findings appears negligible. Further, although the Collaborative Outcome Data Committee (2007) standards specify group equivalence as a critical factor in ensuring quality outcome studies, they do not specify matching on the basis of dynamic risk as a key consideration in achieving equivalence. Indeed, none of the studies identified as meeting CODC ‘good’ quality standards in Hanson et al.’s (2009) review controlled for the dynamic risk profiles of participants.
The study was also limited in terms of the availability of some SIP participant and waitlist data. Recidivism was coded based on officially recorded breaches or reconvictions. The inclusion of charges that may or may not have resulted in reconviction may have increased sensitivity to detecting recidivism. However, these data are not captured by the Department of Corrections and were unavailable to the researchers. Similarly, if we had been able to specifically access the dynamic risk scores of SIP participants and overrides (as opposed to risk categories), our analyses and the conclusions we drew from them may have been strengthened. It would also have been useful to collect item level dynamic risk data to identify dynamic risk factors that were most prevalent for a lower static risk population, which is an avenue for future research.
Appendix A provides a review of the current study against CODC guidelines. In terms of CODC standards, our decision to only consider outcomes of men who completed the SIP, as opposed to including all men who commenced SIP participation in an intent-to-treat SIP group, may also be considered a limitation. However, given that only two men failed to complete the SIP and, based on available information, those men appeared to more closely resemble men overridden to intensive treatment and may ultimately have received that treatment, we perceived that this decision actually increased the strength of the study.
Finally, it must be acknowledged that the length of SIP completer follow-up was relatively short, averaging only 46.5 months (3.9 years). Although other studies have considered similar follow-up periods (e.g. Harkins et al., 2015), most specify a minimum follow-up time of 5 years (Collaborative Outcome Data Committee, 2007). We were also unable to access data regarding the community supervision provisions of SIP completers or men in the comparison group. Therefore, equivalence on this dimension could not be assessed.
Implications and Conclusions
Our findings suggest that although the SIP does not appear to reduce sexual recidivism amongst participants who demonstrate low static and low to moderate dynamic recidivism risk, its administration enables identification of men who demonstrate higher dynamic risk. In turn, these men are offered the opportunity to participate in more intensive treatment programs that may not otherwise be available to them. Given evidence that such programs can significantly reduce sexual recidivism amongst men with higher risk profiles, together with the reduced possibility of negative criminogenic influence represented by their removal, these findings suggest that the net effect of the SIP administration process may be positive. In turn, our findings highlight the diverse individual needs of men assessed as low static risk of sexual recidivism and the need for agencies responsible for their rehabilitation to ensure that all of these are accounted for before allocating them to treatment programs.
As found in previous studies, our results suggest that the postrelease offence trajectories of men assessed as being of low static sexual recidivism risk may be more aligned with men convicted of nonsexual offences than with men assessed at higher static sexual recidivism risk levels. As such, where these men do not also demonstrate moderate to high dynamic risk, they may be more likely to benefit from treatment that emphasises the development of skills to address individually specific criminogenic risks (e.g. violence) and/or reintegration planning over sexual offence risk factor mitigation. Indeed, several studies have demonstrated that comprehensive reintegration planning is associated with reductions in sexual and nonsexual violent reoffending (Dickson et al., 2013; Scoones et al., 2012; Willis & Grace, 2008, 2009). Further, although the specific nature of the reintegration content would need to be tailored to each participant, a focus on reintegration planning also aligns with contemporary strengths-based approaches to rehabilitation and desistance from offending (see Laws & Ward, 2011). Given a focus on reintegration planning does not require any offence process work, such programs could also be offered to men who deny their offences and demonstrate low static and dynamic risk. Thus, a focus on reintegration planning offers an evidence-based (and potentially more cost effective) approach to balancing political and criminogenic needs in the management of individuals assessed with a very low risk of sexual recidivism.
Footnotes
Acknowledgments
This research was supported by a Rutherford Discovery Fellowship awarded to Gwenda M. Willis. The authors acknowledge the New Zealand Department of Corrections, who supplied the data used in our analyses. Neither the funders nor the Department of Corrections had any involvement in the research and/or preparation of the manuscript. The authors take responsibility for the integrity of the data and the accuracy of the data analyses and have made every effort to avoid inflating statistically significant results. The opinions are those of the authors and not necessarily those of the New Zealand Department of Corrections.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.