
Abstract
Problems with self-regulation are often theoretically and empirically linked to sexually abusive behavior, as is also true of experiences of early childhood abuse and maltreatment. Questions remain regarding how indicators of dysregulation and self-regulatory deficits interact and are associated with prior maltreatment. In the current study, a range of variables potentially indicative of emotional, cognitive, interpersonal, and behavioral dysregulation and adverse childhood experiences (ACEs) were examined using the frame of the multimodal self-regulation theory among 156 adult men residing in secure forensic care who were receiving treatment for prior sexual offenses. Data were subjected to principal components analysis, resulting in four components that described varying aspects of dysregulated behavior and experiences: Problematic Sexual Behavior (PSB)-Impulsivity, Serious Mental Illness (SMI)-Aggression, ACEs-Suicidality, and Paraphilic Interests-Behavioral Stability. One component comprised of variables associated with maltreatment was associated with impulsivity and PSBs, as well as SMI and violence via linear regression analysis. Theoretical and clinical implications are discussed.
Keywords
Self-regulation is a process through which people manage their thoughts, emotions, and behaviors and is at the core of many conceptualizations of problematic and illegal sexual behavior. This includes considerations of negative affect, affective instability, and emotionality and emotion regulation (e.g., Grady & Shields, 2018; Howells et al., 2004; Marshall & Barbaree, 1990; Ward et al., 1995; Zaremba & Keiley, 2011); sexual self-regulation (Sigurdsson et al., 2010; Smid & Wever, 2019); inhibition and impulse control (Prentky & Knight, 1991; Turner et al., 2018); executive functioning abilities (Burton et al., 2016; Turner & Rettenberger, 2020); and the ability to self-monitor and self-manage thoughts, behaviors, and interpersonal relationships (Burk & Burkhart, 2003; Johnston & Ward, 1996; Marshall 1989, 1993; Stinson, Sales, & Becker, 2008; Ward & Hudson, 1998; Yates & Kingston, 2006)—all in relation to the development and maintenance of sexually abusive behavior. Specific models incorporating these and related aspects of self-regulatory functioning have included the integrated etiological theory of sexual offending (Marshall & Barbaree, 1990; Marshall & Marshall, 2000), the self-regulation model of sexual offending (Ward & Hudson, 1998), the pathways model (Ward & Siegert, 2002), the integrated theory of sexual offending (Ward & Beech, 2006, 2016), and the multimodal self-regulation theory (Stinson, Sales, & Becker, 2008).
Similarly, theoretical and treatment models beyond the forensic literature have examined the impact of self-regulation on a range of problem behaviors, including impaired social relationships (e.g., Koole et al., 2006; Rawn & Vohs, 2006), suicidality and self-harm behavior (Koerner, 2011; Linehan, 1993), alcohol and substance abuse (e.g., Hull & Slone, 2004; Sayette & Creswell, 2017), and disordered eating (e.g., Herman & Polivy, 2011), with models like Dialectical Behavior Therapy (DBT; Linehan, 1993), Acceptance and Commitment Therapy (ACT; Hayes et al., 1999), and mindfulness-based interventions that incorporate awareness and self-monitoring gaining prominence in both community and forensic clinical work. Increasingly, such approaches are becoming more integrated as treatment modalities for common self-regulatory problems in persons with justice-system involvement and who would benefit from treatment related to problematic sexual behavior (PSB) (Brillhart, 2017; Byrne & Ní Ghráda, 2019; Marotta, 2017; McCann et al., 2007; Quinn & Shera, 2009; Sakdalan & Gupta, 2014).
Alongside research examining PSB in the context of self-regulation is rapidly mounting evidence of the impact of adverse childhood experiences (ACEs) and maltreatment across the lifespan on the development and maintenance of these behaviors as well. Rates of developmental adversity among adults and youth who have engaged in sexually abusive behavior are consistently high and reveal multiple and repeating forms of maltreatment or early childhood disruption (e.g., Hall et al., 2018; Levenson & Socia, 2015; Levenson et al., 2014a, 2014b; Puszkiewicz & Stinson, 2019; Reavis et al., 2013; Weeks & Widom, 1998), often related to more severe and extensive engagement in sexually abusive behavior (Levenson & Grady, 2016; Yoder et al., 2018). Further, findings related to early adversity have been incorporated into attachment-based models describing the pathway from childhood maltreatment to later difficulties with managing sexual behaviors and maladaptive coping (Grady et al., 2017; Yoder, Grady, & Dillard, 2019; Zaremba & Keiley, 2011), as well as models exploring the effect of trauma on executive functioning—a cognitive process integral to self-regulation—via the development of specific traits associated with antisociality (e.g., Developmental Etiological Theory; Knight & Sims-Knight, 2004; Yoder, Grady, & Precht, 2019).
Within the current study, a primary goal is to examine differing aspects of self-regulation and associated behaviors in a sample of adult males engaged in treatment in secure forensic care related to prior acts of sexual aggression either in the community or while in institutional settings. Self-regulation is viewed here within the context of the multimodal self-regulation theory, which posits that dysregulation in cognitive, emotional, interpersonal, and behavioral domains, paired with deficits in adaptive self-regulatory coping, precipitate the development of PSBs. Additionally, this theory holds that early experiences of trauma, maltreatment, or adversity influence the development of self-regulatory functioning. Thus, we will first provide a brief description of the theoretical model and previous efforts to test tenets of the theory using a range of samples of men who have committed sexual offenses.
The multimodal self-regulation theory of sexual offending is premised on a view of self-regulation that involves one’s ability to modulate behavior, emotions, and thoughts in relation to specific goals (e.g., Baumeister & Heatherton, 1996; Karoly, 1993; Stinson, Sales, & Becker, 2008). This model assumes self-regulation to be an innate, biologically driven process impacted throughout the lifespan by experience and learning. Any emergent state of imbalance—be it emotional, physiological, cognitive, or interpersonal—results in a feeling of dysregulation or discomfort that prompts a drive to restore homeostasis. Individuals use learned mechanisms of coping in order to self-regulate, and these self-regulatory strategies may be functional or dysfunctional (i.e., they either work or they do not), and adaptive or maladaptive (i.e., they are non-harmful and healthy, or they instead cause harm to self or others). Thus, much of the multimodal self-regulation theory is concerned with the development of maladaptive, albeit functional, self-regulatory strategies in those who exhibit PSB in response to felt dysregulation. This theory additionally incorporates crucial developmental factors that influence a person’s self-regulatory ability and acquisition of behavioral patterns across the lifespan. These include a range of biological and genetic factors that influence development of self-regulatory abilities, important peer and family relationships, and other factors that impact individual development (e.g., trauma, systemic and ecological challenges). Foundational components of this model are not specific to sex offending behavior but more generally describe the development of problematic self-regulatory mechanisms that may significantly contribute to harmful sexual behaviors for some individuals, based on their life experiences, personality characteristics, and environmental contingencies reinforced over time.
First, emotional sensitivity and reactivity, increased negative emotionality, and difficulty de-escalating emotional states are early biological and temperamental contributors to difficulties with self-regulatory functioning. Ample research evidence suggests observable individual differences in infants and young children with regard to experiences of emotionality and response to changes in the environment (e.g., Chess & Thomas, 1977; Linehan, 1993; Thomas & Chess, 1977; Zentner & Bates, 2008). Those who react more readily, who react more strongly, and who have greater difficulty returning to baseline may be those for whom development of functional and adaptive self-regulatory strategies is more challenging yet necessary.
Second, how others in the person’s immediate environment respond to signs of distress or dysregulation shape that individual’s ability to appropriately and effectively self-regulate. Importantly, unhealthy relationships with family, peers, or systems in the individual’s environment (e.g., schools, criminal justice system) that may include a range of experiences like trauma, neglect, or perceptions of isolation and failure to meet others’ expectations not only exacerbate dysregulation but also compromise the development of adequate coping skills to self-regulate. Individuals characterized by such developmental disadvantages may suffer from a number of self-regulatory deficits. Specifically, they may lack the regulatory skills necessary to respond to dysregulation in an effective way, or they may develop maladaptive strategies, such as sexually abusive behavior or other impulsive and potentially harmful behaviors, to regulate their emotions, behaviors, cognitions, and interpersonal interactions (Stinson & Becker, 2012; Stinson, Becker, & Sales, 2008; Stinson, Sales, & Becker, 2008). Growing evidence suggests that early traumatic experiences may alter the structure and function of the developing brain (e.g., Creeden, 2009, 2013, 2020; Ehrlich et al., 2016), potentially impacting a range of factors associated with self-regulatory functioning.
Finally, a number of other factors, including personality, perceptions of opportunity, and reinforcement following the use of a particular regulatory strategy, further influence response to dysregulation and selection of self-regulatory strategies. Personality features like callousness, impulsivity, entitlement, low frustration tolerance, or sensation seeking may contribute to the use of strategies that may be harmful to others (e.g., Vitacco et al., 2010; Yoder et al., 2020). Early messages regarding boundaries, relationships, intimacy, and sexuality may distort perceptions of sexual opportunity and the role of sexual behavior in the context of dysregulation (e.g., Puszkiewicz & Stinson, 2019). Whether or not chosen mechanisms for self-regulation are effective—meaning that they reduce the experience of dysregulation in the moment—reinforces the likelihood of these or other similar strategies being employed in the future. Thus, maladaptive sexual behaviors and associated urges and fantasies may become part of the individual’s larger repertoire of self-regulatory practice.
Initial research examining self-regulation using the multimodal self-regulation theory as a frame focused on the role of emotional dysregulation in predicting sexually abusive and other illegal behaviors in a sample of civilly committed “Sexually Violent Persons” (Stinson, Becker, & Sales, 2008). Via path analysis, measured indicators of emotional dysregulation were significantly associated with onset, severity, and pervasiveness of sexual offending, revealing important covariance underlying the relationship between sexual offending and antisocial behavior. A subsequent study considered how different presentations of self-regulatory deficit may account for varying types of behavioral dysregulation in an inpatient forensic psychiatric sample (Stinson et al., 2011). Factor analysis of diagnostic variables produced two factors presumed to be descriptive of emotional and cognitive dysregulation, and dysregulated behavioral outcomes entered into a separate analysis produced criminal, sexual, and suicidal categories. Regression analysis revealed that emotional dysregulation significantly contributed to only criminal and suicidal behaviors, whereas cognitive dysregulation significantly contributed to all three forms of dysregulated behavior (Stinson et al., 2011).
Additional research is needed to explore conceptual relationships in diverse samples and with varying forms of measurement and to evaluate other important correlates of self-regulatory difficulties and outcomes associated with sexually abusive behavior within this conceptual frame. While there are numerous evaluations of differing facets of self-regulation and self-regulatory processes, it is important to examine these within a variety of samples and to determine how these facets are at times interrelated and also how they may function independently. Another aspect of this process that has been examined within the literature but not yet within the view of self-regulatory processes described within the multimodal self-regulation model is the proposed role of maladaptive family relationships or experiences of early childhood adversity. Within this etiological theory, the relevance of early maltreatment and familial dysfunction is twofold. First, experiences of trauma, maltreatment, or familial dysfunction may exacerbate dysregulation to the point that the individual has difficulty with adequate self-regulation. And second, environments characterized by hostility, violence, or unrelenting chaos are those that may understandably fail to teach the developing child functional or adaptive self-regulatory strategies.
In the current study, we examine a sample of adult men residing in secure forensic care with histories of violence and sexual offending. We have selected a broad range of psychiatric symptoms and behaviors, ACEs, indicators of justice-system involvement, institutional behavior samples, and measures of attitudes and behavior associated with sexual and criminal offending to assess using principal components analysis. Our hypotheses are as follows: Through principal components analysis, we will be able to identify relationships between varying indicators of emotional, cognitive, interpersonal, and behavioral dysregulation, as well as experiences of early childhood adversity. The resulting components will demonstrate ways of measuring or categorizing differing features of difficulties with self-regulation. Early childhood experiences will be significantly associated with later outcomes associated with dysregulation and self-regulatory problems, consistent with what is suggested within the multimodal self-regulation theory.
Methods
Sample
Participants were 156 adult males residing in a secure forensic psychiatric hospital in the Midwestern United States. This sample was originally drawn for a study of treatment programming research (for a more detailed description of the sample, see Stinson et al., 2017). All participants had been deemed eligible for treatment related to PSB due to either a history of sex offenses in the community or illegal sexual behaviors in the current or previous residential facilities, though participation in treatment was not required for inclusion in the present sample. All procedures were reviewed and approved by the institutional review board (IRB) associated with the first author at the time of data collection, as well as by the research council of the facility from which data were obtained. Herein, we report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study. Data were archival in nature and had been documented as part of routine treatment at the facility.
Descriptive Statistics for Demographic Characteristics and Variables Entered into the Principal Components Analysis, N = 156.
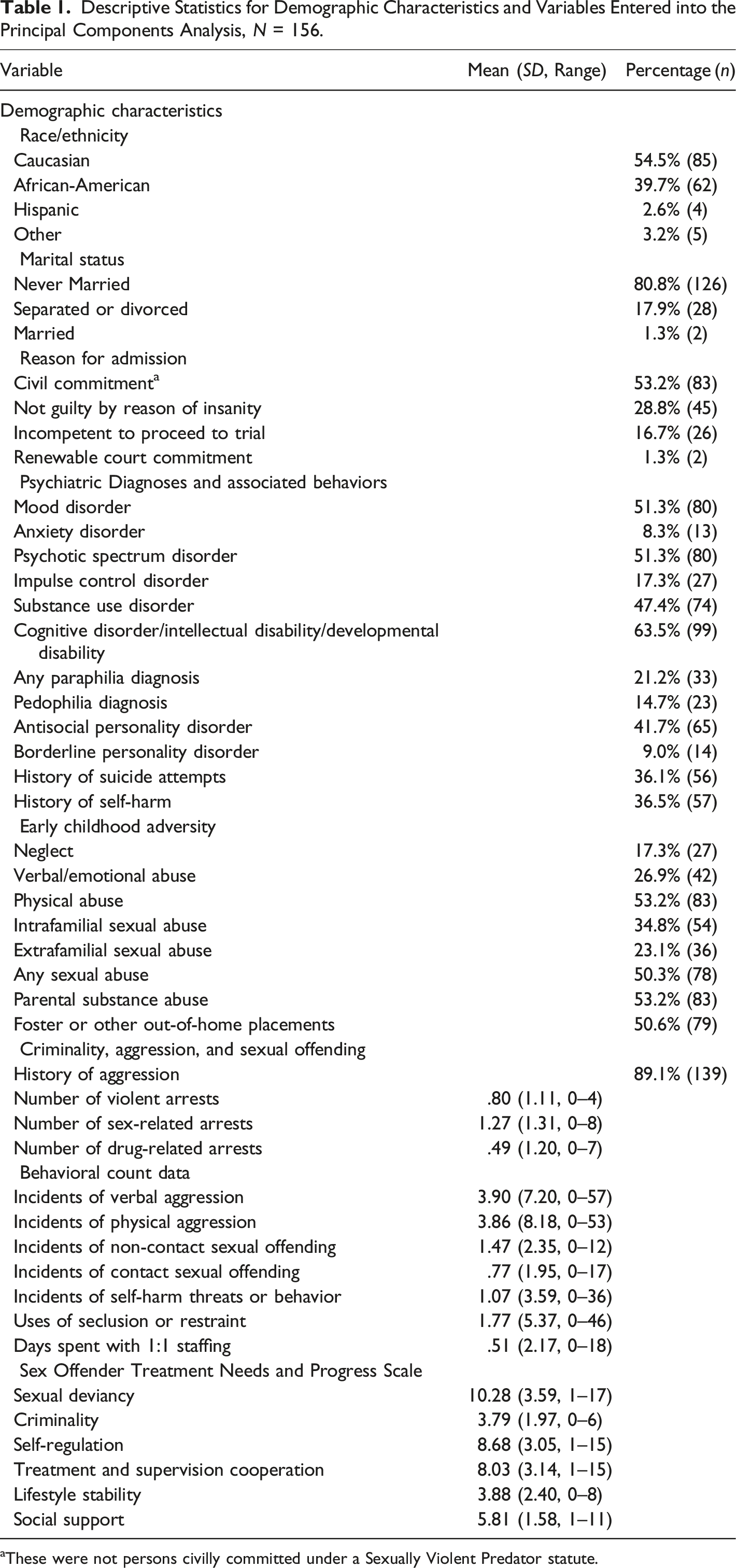
aThese were not persons civilly committed under a Sexually Violent Predator statute.
Measures
Data were obtained from archival hospital records that included social history reports, medical and psychiatric evaluations, arrest history data, psychological assessments, and sexual history reports. Diagnostic information was collapsed into major symptom categories to accommodate diagnostic variability (e.g., all forms of schizophrenia, schizoaffective disorder, disorders with psychotic symptoms, delusional disorder, schizophreniform disorder, brief psychotic disorder, and psychotic disorder not otherwise specified were all included within the category “psychotic disorder”) and coded as either present (1) or absent (0). This coding scheme additionally allowed for co-morbidity, which was common within the sample. Historical information regarding suicidality and suicide attempts, as well as count data for incidents of self-harm while in the facility, were also included as diagnostic information relevant to the current analysis. In addition to demographic and diagnostic information, specific measures included in each set of analyses are discussed further below.
For the purposes of the current study, only data that had been documented pre-treatment were used to reduce the influence of a treatment predicated on self-regulatory skills training on variables that may serve as indicators of self-regulation. All pre-treatment variables pertaining to psychiatric symptoms and diagnosis, violence and criminality, and historical maltreatment or abuse were included in the principal components analysis described further below. Variables with excessive missing data or that were solely demographic in nature were excluded.
Early Childhood Adversity
Documented instances of childhood abuse, neglect, and household dysfunction were coded as either present (1) or absent (0) according to client self-report or reports obtained from family members, caregivers, case managers, law enforcement or judicial officials, or those involved in social service agencies. Categories of documented maltreatment included physical abuse, intra- and extrafamilial sexual abuse, and neglect, while categories representative of household dysfunction included parental substance abuse and history of foster care placement.
Criminality, Aggression, and Sexual Offending
Archival participant records contained information related to reported age of onset of aggressive behavior—as described through client self-report and when possible corroborated by reports from involved family members or legal guardians—and any available records indicative of prior psychiatric treatment. Incidents of aggression that either prompted psychiatric treatment or occurred within the context of hospitalization were noted. Arrest records were available through a combination of the above-noted sources in addition to pretrial evaluations and other legal investigations. During the course of treatment and risk assessment associated with sexual offenses, participants had frequently provided information related to their onset and nature of sex offending behavior. These sources were used to determine history of aggression (dichotomously coded) and number and types of arrest.
Behavioral Count Data
Archival records describing incidents of verbal and physical aggression, sexual behavior, threats and behaviors of self-harm, use of seclusion and restraint, and days spent with 1:1 staffing were available for periods of up to 1 year pre-implementation of treatment programming and 2 years while participants were in treatment related to their sexual offenses. To exclude possible treatment effects, only pre-treatment count data in 6-month increments were used for the purpose of the current analyses. As not all participants were admitted for a full year prior to treatment implementation, data from the 6-month period immediately prior to treatment initiation were used.
Sex Offender Treatment Needs and Progress Scale (SOTIPS; McGrath & Cumming, 2003). The original version of the SOTIPS is an instrument describing important indicators of treatment progress and dynamic risk, measured in 6-month increments. Items include cognitive, behavioral, and motivational aspects of criminal and sexual behavior problems, grouped into five subscale measures. These subscales include the following: (1) sexual deviancy, describing degree of responsibility-taking for sexual offending, risk-taking, and sexual behaviors, attitudes, and interests; (2) criminality, rating criminality and rule-breaking behaviors and attitudes; (3) self-regulation, describing an individual’s substance abuse, emotional management, mental health stability, problem solving, and impulsivity; (4) treatment and supervision cooperation, describing willingness to change and cooperation with treatment and supervision; (5) lifestyle stability, indicating the degree to which the participant manages vocational, residential, and financial concerns; and 6) social support, or social and romantic relationships and involvement. For those participants diagnosed with intellectual disability, the comparable Treatment Intervention and Progress Scale for Sexual Abusers with Intellectual Disabilities (McGrath, 2005) was used. On each of these subscales, all items are scored from 0 to 3, with higher scores representing greater difficulties and needs in this area. Thus, for each subscale, participants’ total scores range from 0 to 6 on the shortest subscale (criminality) and 0–18 for the lengthiest (sexual deviancy). Ratings were established prior to treatment and throughout the treatment study period through interviews with treatment providers and review of participant treatment records. To control for the potential effects of treatment on participants’ scores, only pre-treatment SOTIPS scores were used in the current analysis.
Analytic Plan
Prior research on the multimodal self-regulation theory has used a combination of psychiatric, behavioral, and criminological variables to test the existence of factors describing proposed dysregulation, as well as relationships between emotional and cognitive dysregulation and important behavioral outcomes (Stinson, Becker, & Sales, 2008; Stinson et al., 2011). However, these studies were limited by the scant number of indicators available to describe important components of the theory with regard to varying facets of dysregulation. In the present study, we used principal components analysis (oblimin rotation with Kaiser Normalization) to understand the relationships between of a broader set of variables. Descriptive information regarding all variables initially entered into the principal components analysis is found in Table 1, and correlations between these are presented in Table S1. There were few instances of missing data, with 14 of the 37 variables evidencing missing data points ranging from .6 to 1.3% across the sample. Two participants evidenced a higher degree of missing data, missing seven data points across the 37 variables included. Little’s test indicated that these data are missing completely at random, χ 2 = 69.332, p = .632. Missing data were replaced through multiple imputation prior to the analysis.
Initial review of the resulting components involved examining the scree plot and resulting components with an Eigenvalue of 1. As is described further within the results section, subsequent analysis used an Eigenvalue of 2 and consideration of factor loadings that were .3 or above. Following this, the factor scores were submitted to linear regression analysis (Enter method) to evaluate relationships between resulting components. All analyses were conducted with SPSS version 27.
Results
Bivariate Correlations Across Variables
As is shown in Table S1, many of the selected variables evidenced significant correlations with one another. A number of these relationships were rather unsurprising, such as correlations between varying mental health diagnosis, categories of ACEs, and individual subscales of the SOTIPS. However, some interesting correlations emerged. For example, psychotic symptoms were negatively correlated with cooperation with treatment and supervision, and ACEs were unrelated to aggression and arrest. Further, institutional misconduct was not significantly correlated with indicators of community misconduct. Additional analyses will help clarify these relationships.
Principal Components Analysis
Results of the Principal Components Analysis With a Four-Factor Solution Following Removal of Variables From Previous Step, N = 156. Factor loadings of 0.300 or higher are presented in bold text.
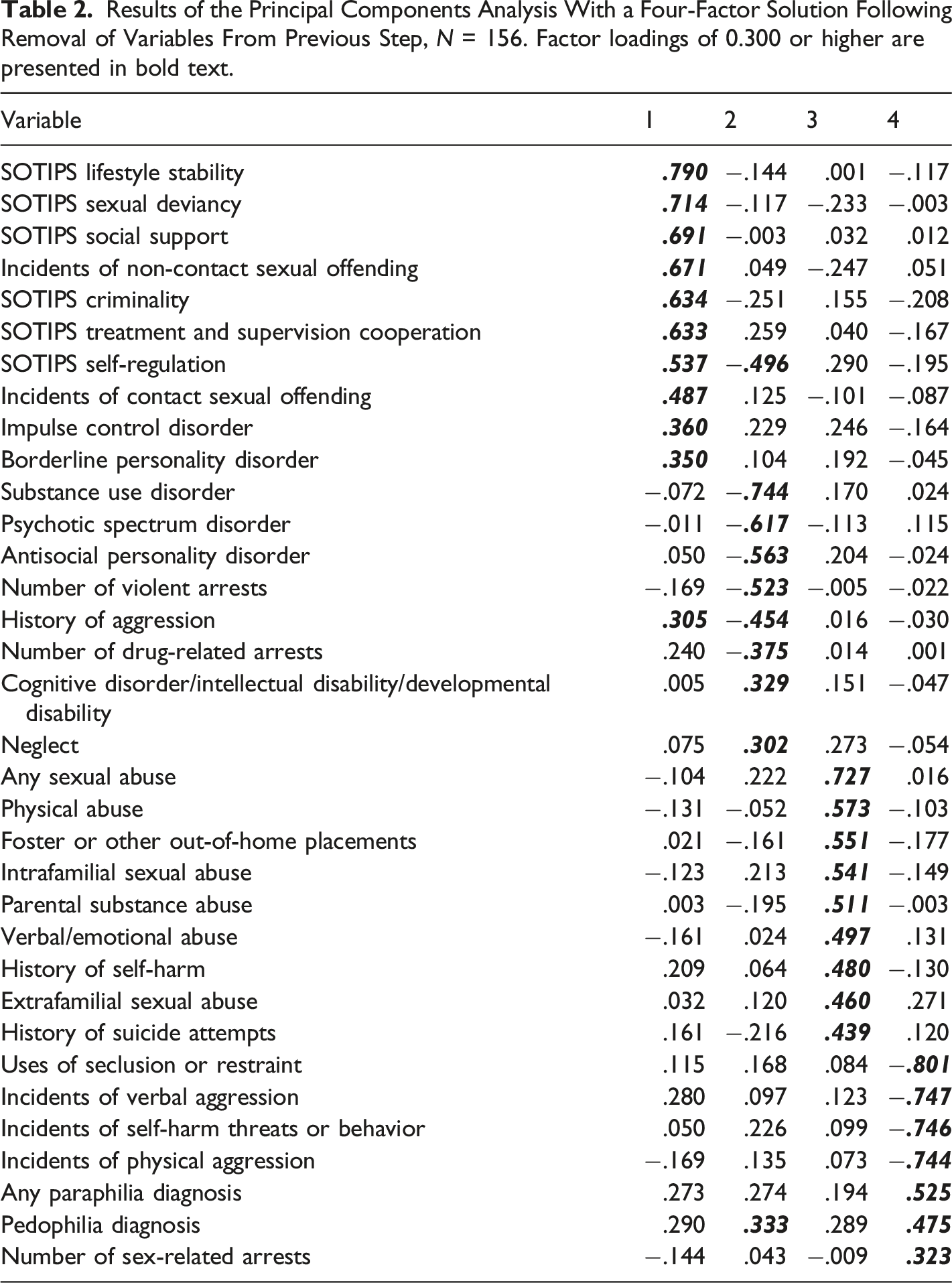
The first resulting component, PSB-Impulsivity, included impulse control disorder, borderline personality disorder, history of aggression, institutional sexual misconduct, and all six subscales of the SOTIPS. Thus, this component appears to collectively include indicators of continuing PSBs and poor performance in treatment specific to sexual offending and criminality, as well as some degree of non-sexual impulsivity. The second component, Serious Mental Illness (SMI)-Aggression, included positive factor loadings for pedophilia, neglect, and cognitive, intellectual, or developmental disability, while there were negative factor loadings for psychotic spectrum disorders, substance use, antisocial personality disorder, history of aggression, violent and drug-related arrests, and self-regulation as measured on the SOTIPS (where higher scores are equated to poorer emotional stability and self-regulatory functioning). This combination of indicators appears to capture some degree of SMI, increased violence and aggression, poorer self-regulatory functioning, and lesser degrees of neglect, cognitive impairment, or pedophilia diagnosis. The third component, ACEs-Suicidality, includes indicators of prior suicidality and self-harm, as well as a range of ACEs inclusive of abuse, parental substance abuse problems, and foster and other out-of-home placements. Finally, our fourth component, Paraphilic Interests-Behavioral Stability, was comprised of positively-loaded factors associated with paraphilic interests and increased number of sexual arrests and negatively-loaded indicators of non-sexual institutional misconduct. This reflects a combination of paraphilic sexual interests and behaviors along with some degree of behavioral stability within the institutional setting.
Cronbach’s α and Bivariate Correlation Matrix of Component Scores.
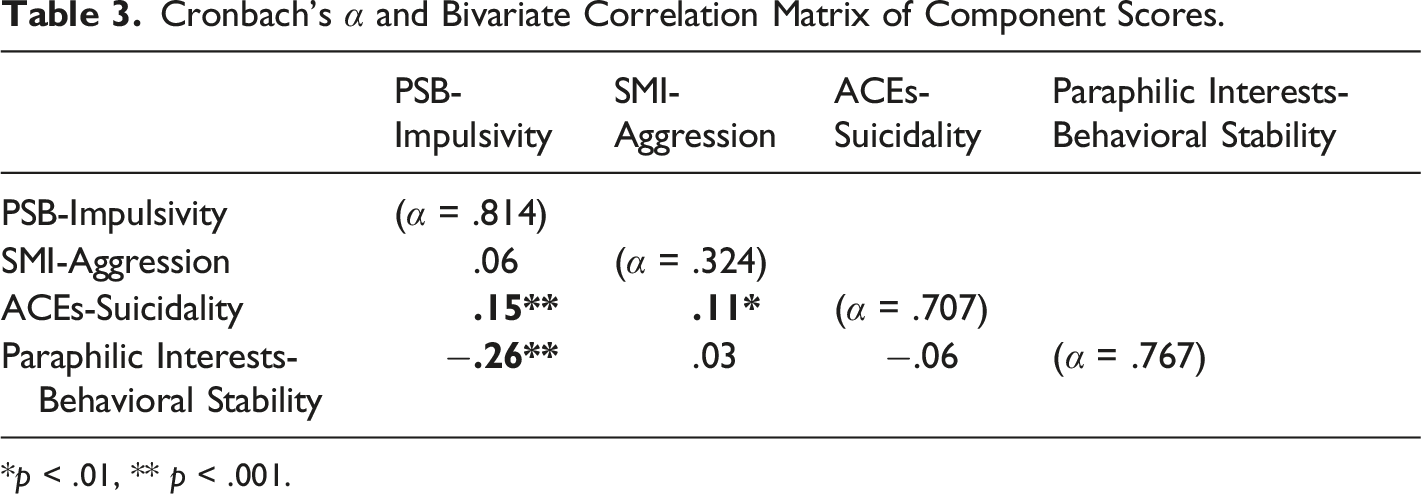
*p < .01, ** p < .001.
Linear Regression Analyses
Linear regression analysis of theorized relationship between ACEs-Suicidality and PSB-Impulsivity, SMI-Aggression, and Paraphilic Interests-Behavioral Stability.
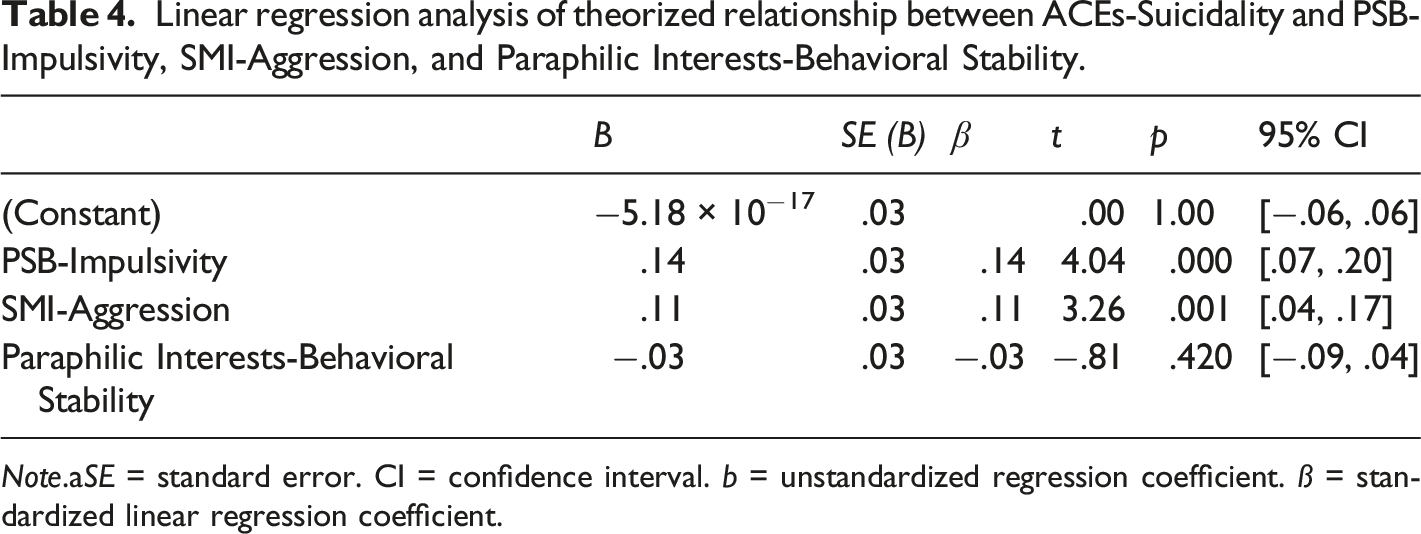
Note.aSE = standard error. CI = confidence interval. b = unstandardized regression coefficient. ß = standardized linear regression coefficient.
Discussion
Theoretical and Research Implications
Within the principal components analysis, four components were identified that reflect varying aspects of emotionality, behavioral problems, impulsivity, sexual misconduct, and early childhood adversity. In contrast with previous findings evaluating dysregulation from the frame of the multimodal self-regulation theory, resulting components were not divided into strictly behavioral, cognitive, or emotional indicators of self-regulatory problems. Instead, the components appear to capture facets of behavior, emotionality, and experiences that may categorize different needs or types of persons who exhibit signs of self-regulatory difficulty.
In PSB-Impulsivity, representative variables include indicators of continuing institutional sexual behavior problems, poor progress in treatment aimed at addressing sexual offending and criminality, and diagnostic labels associated with some degree of non-sexual impulsivity and affective lability. These variables loaded independently of others that are more traditionally associated with sexual behavior problems, including paraphilic diagnoses, pedophilic sexual interests, and severity of sexual offense history. Instead, Paraphilic Interests-Behavioral Stability included these specific variables and the relative absence of institutional non-sexual behavior problems, perhaps suggesting different typologies of participants with sex offending histories within this sample. This is consistent with other research describing typologies of persons who have committed sexual offenses that differentiate opportunistic offending and antisociality from sexual offending more associated with paraphilic interests (e.g., Beech, 1998; Ennis et al., 2016; Knight et al., 1994; Mandeville-Norden & Beech, 2009). Here, a similar pattern thus emerges in a forensic mental health sample of persons with PSB. The two components additionally differed with regard to the occurrence of institutional sexual misconduct, non-sexual misconduct, and sexual offending in the community. This supports prior findings that community and institutional forms of sexual and violent misconduct are not definitively associated with the same predictors (McDermott, Edens, Quanbeck, Busse, & Scott, 2008; Walters & Heilbrun, 2010).
SMI-Aggression appears to represent problems with behavioral self-regulation and psychotic spectrum disorder that may uniquely characterize forensic mental health populations. A large number within the sample were diagnosed with disorders containing aspects of psychosis, ranging from forms of schizophrenia and schizoaffective disorders to mood and bipolar disorders with psychotic features. That these aspects of the individuals’ cognitive functioning and regulatory ability aligned more strongly with violent and aggressive behavior, as well as problematic and illegal substance abuse, rather than with their sexual behavior, is noteworthy. In prior research (Stinson et al., 2011), psychosis and cognitive or intellectual impairments were associated with one another and interpreted as representing differing forms of cognitive dysregulation. Here, they loaded on the same component but differed with regard to valence once again. This may suggest that they share a degree of variance and could identify aspects of disordered or problematic thinking that are independent of more emotionally themed indicators of dysregulation.
Finally, ACEs-Suicidality included experiences of early abuse, maltreatment, and household dysfunction, as well as suicidality and self-harm, which are often associated with histories of trauma. Such histories were common within the sample, as fewer than 20% reported no early childhood adversity, and the prevalence of physical abuse, sexual abuse, parental substance abuse, and foster care placement each exceeded 50% within the sample. And while this measures largely historical occurrences of maltreatment and household dysfunction, findings from the regression analyses suggest that they have a continued impact on behaviors in the community and institutional settings, as ACEs-Suicidality was significantly predicted by PSB-Impulsivity and SMI-Aggression via linear regression. It was not significantly associated, however, with Paraphilic Interests-Behavioral Stability, which seemed more indicative of paraphilic interests and a greater number of sexual offenses, perhaps driven by offense-supportive sexual interests rather than sexualized coping or difficulties with self-regulation.
Clinical Implications
Our findings, as well as evidence from previous research, suggest that assessing self-regulatory ability and history of maltreatment may have implications for understanding important treatment needs and risk (e.g., Hanson & Harris, 1998; Kingston et al., 2012). Further, existing treatments for impulsive and problematic behavior have included a focus on self-regulation, including DBT (e.g., Dimeff & Koerner, 2007; Linehan, 1993) the good lives model (Ward & Brown, 2004; Ward et al., 1998, 2007), and safe offender strategies (Stinson & Becker, 2012). It is possible, then, that the concepts included in the multimodal self-regulation theory and the present analysis may improve treatment design and outcomes and help us better understand divergent presentations of dysregulation and how to target these in treatment.
As the principal component analysis differentiated three aspects of treatment need (i.e., impulsivity and continuing sexual behavior problems, indications of psychosis and violent behavior, and paraphilic sexual interests and greater non-sexual behavioral stability), this suggests opportunities for individual treatment planning and use of the Risk-Needs-Responsivity model for identifying non-criminogenic needs relevant to subpopulations of forensic mental health clients. This may additionally contribute to differing levels of risk for those who continue to exhibit aggressive and PSBs within a secure setting that could impact the form and dose of appropriate treatment. Given that SMI and continuing behavioral instability were identified within the analysis, there is a need for treatment and assessment that is designed for and evaluated in this population, rather than those that have simply been adapted from community or correctional models.
Finally, given the degree to which experiences of trauma, maltreatment, and early adversity were evident within the sample and significantly associated with many of the behaviors targeted in current treatment, there is a need for trauma-informed models of treatment and staff training in forensic mental health treatment settings. This involves a holistic understanding of the impact on trauma on development, relationships, mental health, and important behavioral outcomes, as well as treatment implementation that recognizes and appropriately addresses trauma-based responding and previously learned ways of maladaptive coping. In this way, treatment can be designed and delivered in a manner that facilitates safety and trust, fosters opportunities for choice and compassion, and builds trauma resistant and adaptive coping skills for clients (see further Levenson, 2014; Levenson et al., 2016, 2017).
Limitations and Conclusions
Despite interesting results with implications for future research, the current study faced a number of limitations. While structural equation modeling would allow for more precise assessment of the theoretical model, we were constrained by the size of the sample. Also, we were reliant on archival data and were therefore unable to directly measure ongoing signs of dysregulation in participants. Future research should include directly observable or incrementally measured indicators of dysregulation, and should include varied forms of dysregulation for maximal adherence to the theorized model. Similarly, our reliance on historical aggregate measures of abuse and maltreatment did not account for severity of abuse, long-term impacts on participants, or other qualitative features of an individual’s abuse experience that might contribute to the association with dysregulation and behavioral outcomes.
Another limitation is the applicability and generalizability of the current sample to the broader, heterogeneous population of persons involved in treatment for sexual offending. These were persons in inpatient forensic psychiatric care within a treatment program in a single US state. Though it is arguable that this subpopulation of persons who have engaged in sex offending behavior may exhibit more intense signs of dysregulation due to mental health problems and serious histories of trauma and maltreatment, they were also all receiving psychotropic medications that might have impacted their rates of aggressive and sexual behavior during the observation period 6 months pre-treatment, and they may not be as generalizable to a non-psychiatric population.
Finally, the goal of the current study was to broadly examine a range of experiences and behaviors purportedly associated with dysregulation and self-regulatory difficulties. More thorough exploration of multiple facets of dysregulation, the interaction between dysregulation and ongoing events, and environmental contingencies that may further influence self-regulation outcomes is still needed. Because not all aspects of the multimodal self-regulation theory have been empirically evaluated, it remains to be seen how each of these elements fits real-world clinical samples, and whether or not the many elements involved can be retrospectively measured and tested. Future research should seek to further define theoretical concepts, use multiple measures for differing components of the model, and incorporate prospective measurement and observation of dysregulation whenever possible.
In conclusion, the multimodal self-regulation theory attempts to explain the development of sexual behavior problems as a response to deficits in the ability to appropriately regulate experiences of dysregulation. Early evidence has supported several tenets of the theory, including that factors indicative of emotional and cognitive dysregulation can be extracted from available measures, and that they are significantly associated with sexual and aggressive behavioral outcomes. The current research project supports these findings, as we were similarly able to extract indicators of dysregulation, and these provided some predictive validity for aggressive and sexual outcomes, moderated by past childhood experiences of abuse and maltreatment. This provides encouragement for future research and use of the multimodal self-regulation theory to better understand persons with histories of PSB and their unique treatment and risk management needs.
Footnotes
Acknowledgments
The authors take responsibility for the integrity of the data, the accuracy of the data analyses, and have made every effort to avoid inflating statistically significant results. The authors wish to thank the following people for their assistance and constructive feedback on previous versions of this manuscript: Carrie LeMay, Kevin Nunes, Theresa Gannon, Mark Olver, Michael Seto, and the anonymous reviewers.
Kelcey Puszkiewicz is currently affiliated with the Psychiatry Department at University of Arkansas for Medical Sciences in Little Rock, Arkansas. Michael Lasher is currently affiliated with the Virginia Center for Behavioral Rehabilitation in Burkeville, Virginia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.