
Abstract
Keywords
Constructs representing self-views (e.g., self-concept and self-esteem) have garnered an enormous and increasing amount of attention from theorists, philosophers, clinicians, researchers, educators, policy makers, and laypeople for well over the past century. Early psychologists associated the way in which individuals view themselves with psychological well-being and characterized adequate self-concept as essential for optimal human development and functioning (Shaw-Zirt, Popali-Lehane, Chaplin, & Bergman, 2005). These views led to further speculation that problems with self-concept may be the root of most individual and societal ills and the promotion of the improvement of self-concept as a panacea for wide-ranging societal problems (Baumeister, Campbell, Krueger, & Vohs, 2003). At times, perspectives on the importance of self-concept have clearly moved beyond a level of interpretation consistent with empirical findings.
The empirical examination of self-concept is complex, and thus, empirical findings have not always been clear. Results appear to vary based on the manner in which the structure of self-concept is conceptualized (e.g., global or multidimensional) and on the outcomes by which self-concept is evaluated (i.e., whether the outcomes are global or bundled [e.g., psychological well-being] or more specific [e.g., math performance]), among other factors. Although multidimensional models of self-concept have gained in popularity and garnered increasing empirical support, multidimensional and global views are not mutually exclusive and both are perceived to have merit (Marsh, 2008; Rosenberg, Schooler, Schoenbach, & Rosenberg, 1995). Domain-specific areas of multidimensional self-concept (e.g., academic and physical) have been highly associated with specific outcomes (e.g., academic grades and athletic performance) but not more global outcomes (see Marsh, 2008, for a review of this literature). Likewise, although global self-views are usually not significantly correlated with specific outcomes, they are significantly associated with more global outcomes (Swann, Chang-Schneider, & McClarty, 2007). For example, recent empirical findings have indicated that global self-views are linked to various global outcomes such as mental and physical health (Donnellan, Trzesniewski, Robins, Moffitt, & Caspi, 2005; Orth, Robins, Trzesniewski, Maes, & Schmitt, 2009; Trzesniewski et al., 2006).
Because of the challenges they experience in a variety of life domains, adults with ADHD are a particular group who may be at risk for problems with general self-concept. Within the social domain, adults with ADHD, relative to adults without ADHD, have more interpersonal difficulties (Barkley, Murphy, & Kwasnik, 1996; Blase et al., 2009; Norvilitis, Ingersoll, Zhang, & Jia, 2008) and marital difficulties (Biederman et al., 1993). Educationally, adults with ADHD are less likely than those without ADHD to attend college (Lambert, 1988), and when they do attend college, they are more likely to experience academic problems and attain lower grade point averages (Blase et al., 2009) and less likely to complete college (Weiss, Hechtman, Milroy, & Perlman, 1985). When adults with ADHD enter the workforce, they have shorter durations of employment (Barkley et al., 1996) and lower occupational attainment (Norvilitis et al., 2008) than do adults without ADHD. Problems with self-concept might reasonably be expected for individuals experiencing such difficulties across these important domains of life.
Mixed results have been found from the few studies conducted on the self-concept of adults with ADHD. Although some researchers have found adults with ADHD to report lower self-concept than do adults without ADHD (Dooling-Liftin & Rosen, 1997; Rucklidge, Brown, Crawford, & Kaplan, 2007; Shaw-Zirt et al., 2005), others have found no difference in self-concept between the two groups (Wilmhurst, Peele, & Wilmhurst, 2011). In addition, although not indicative of general self-concept, per se, some research has suggested that adults with ADHD tend to have higher self-evaluations of their specific abilities than might be expected based on actual competence (Knouse, Bagwell, Barkley, & Murphy, 2005; Rapport, Friedman, Tzelepis, & Van Voorhis, 2002). Such findings highlight the inconclusive nature of the knowledge base on the self-concept of individuals with ADHD, particularly adults with ADHD, and the need for further investigation with additional approaches.
Multi-informant assessment is one approach to more thoroughly understand the self-concept of adults with ADHD that has yet to be used. Obtaining self- and other-reports of psychological phenomena has been promoted as best practice in psychological assessment, in general (Achenbach, Krukowski, Dumenci, & Ivanova, 2005; Kraemer et al., 2003; Myer et al., 2001) and for adults with ADHD, in particular (Barkley, Fischer, Smallish, & Fletcher, 2002; Murphy & Gordon, 2006). Although cross-informant agreement for ratings of psychological phenomena tend to be moderate at best, use of self-report alone will often lead to an incomplete and biased understanding of the individual (Myer et al., 2001). Rather than being perceived as problematic, imperfect agreement among informants provides evidence of the value of obtaining multiple perspectives because each informant will likely provide unique information, resulting in a more complete clinical picture. Self- and other-reports have been found to be independently predictive of psychological functioning (Klein, 2003). Examining the self-concept of adults with ADHD via self- and parent-reports may be particularly beneficial because of the complex nature of self-concept and the limitations of self-knowledge. As discussed by Wilson and Dunn (2004), “People are not an open book to themselves” (p. 494), and others may be able through observation of behaviors to identify dimensions of self-concept that may not be within the conscious awareness of the individual.
College students with ADHD are a subgroup of adults with ADHD who, until recently, have received very little research attention but who likely possess unique characteristics relative to the general adult population with ADHD (DuPaul, Weyandt, O’Dell, & Varejao, 2009). These individuals are perhaps more likely than adults with ADHD who do not attend college to possess higher ability levels, to have experienced more school success throughout their lives, and to use more advanced compensatory strategies (Frazier, Youngstrom, Glutting, & Watkins, 2007). College students with ADHD are also likely to be a resilient subgroup within the larger adult population with ADHD because they have reached high levels of achievement despite the significant obstacles posed by the disorder (Wilmhurst et al., 2011). Given these potentially unique characteristics, issues related to self-concept may differ for college students with ADHD relative to the larger general population of adults with ADHD. Only two studies have been conducted in which self-concept was examined among college students with ADHD, with one indicating lower self-concept for college students with ADHD relative to their non-ADHD peers (Shaw-Zirt et al., 2005) and the other resulting in no difference in self-concept between these groups (Wilmhurst et al., 2011). Self-concept was measured by self-report alone in both studies.
The purpose of the current study was to examine the self-concept of college students formally diagnosed with ADHD using self- and parent-reports. Four research questions were pursued, including the following:
Research Question 1: How do college students with ADHD rate their self-concept and how do these ratings compare with those of young adults without ADHD?
Research Question 2: How do parents of college students with ADHD rate their children’s self-concept and how do these ratings compare with those of others’ ratings of young adults without ADHD?
Research Question 3: What are the roles of gender, ADHD subtype, level of educational attainment, and comorbidity in relation to the self- and parent-reported self-concepts of college students with ADHD? and
Research Question 4: How do self-reports of self-concept of college students with ADHD compare with parent-reports of their self-concept?
Method
Participants
Participants were 95 individuals who sought comprehensive psychological evaluations at a university-based clinic staffed by licensed psychologists with self-identified specialties in the assessment of learning disorders. They attended 1 of 14 small- to large-sized colleges or universities in the southeastern United States but were all evaluated at the same above-mentioned clinic. The convenience sample used in the current study consisted of all individuals assessed at the clinic between January 2005 and July 2011 who met the study inclusion criteria discussed below.
Four inclusion criteria were used to select the participants. First, participants had to be diagnosed with inattentive type ADHD or combined type ADHD using Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000; procedures for making these diagnoses are discussed below) criteria. Individuals with hyperactive-impulsive type ADHD were excluded because very few were diagnosed with this subtype, and therefore, the sample size of this group was insufficient for comparison with other subtypes. Second, participants had to be of typical college age, defined as 18 to 24 years old. Third, all participants had to be attending a 4-year college. Those attending technical schools or graduate school were excluded. Fourth, participants were required to have completed a self-report self-concept rating scale and one of their parents was required to complete the other-report version of this scale.
Participants were diagnosed with ADHD via a comprehensive psychological evaluation by a licensed psychologist with assistance from master’s-level clinicians. A multimethod, multi-informant approach was used for each evaluation, and included a clinical interview, psychological testing, academic achievement testing, behavioral observations, and self- and parent-report rating scales. Evaluations were completed over 2 days and, on average, included 10 hr of assessment. Interviews were developed by the clinical staff and included assessment of each participant’s presenting concerns, background information (e.g., developmental history and medical history), and symptoms of psychopathology. The content of the clinical interviews was similar across psychologists; however, the specific manner in which the interviews were administered varied based on the approach of each psychologist. Information derived from the clinical interview allowed each psychologist to tailor the evaluation to the referral concerns of each client. Differential diagnosis was emphasized to rule out other explanations for ADHD symptoms. For example, to rule out possible medical explanations, participants were asked about their medical history and current medical issues during the interview.
For the assessment of ADHD in particular, participants described their symptoms during the clinical interview. In addition, they and one of their parents (or both of their parents together) completed the Conners’ Adult ADHD Rating Scales–Self-Report: Long Version (CAARS-S:L; Conners, Erhardt, & Sparrow, 1999b) and CAARS–Observer: Long Version (CAARS-O:L; Conners, Erhardt, & Sparrow, 1999a), respectively. Parents also completed an informal checklist in which they rated childhood symptoms of ADHD. Further assessment of symptoms was conducted by determining the generalizability of symptoms across settings as well as the degree of functional impairment resulting from the symptoms. Although neuropsychological testing (e.g., continuous performance tests and working memory tests) was also used, in accordance with the DSM-IV-TR, participants were not required to demonstrate deficits on these tests in order for an ADHD diagnosis to be made. Rather than relying on one source of evidence or specific cutoff scores on rating scales to determine the presence of ADHD, psychologists used clinical judgment to weigh the data from each informant and each method to determine whether DSM-IV-TR criteria for ADHD and/or other diagnoses were met.
Table 1 displays the sample’s mean age, IQ scores, and T-scores from the CAARS-S:L ADHD symptom scales. As expected, relative to the inattentive type ADHD group, the combined type ADHD group reported more symptoms of hyperactivity-impulsivity, F(1, 92) = 18.69, p < .01, and total symptoms of ADHD, F(1, 92) = 7.94, p = .006, but not more inattentive symptoms, F(1, 92) = .218, p =.64. Gender of the total sample was 52.6% female and 47.4% male. Ethnicity included 87.4% White, 3.2% African American, 4.2% Hispanic, 1.1% Asian American, 1.1% American Indian, 1.1% multiracial, 1.1% Other, and 1.1% missing data. The participants were mostly underclassmen (i.e., freshmen and sophomores; 81.1%). Regarding subtype of ADHD, 43.2% were inattentive type ADHD and 56.8% were combined type ADHD. Of the total sample, 47.4% were diagnosed with comorbid conditions, including learning disabilities (n = 30), anxiety disorders (n = 13), mood disorders (n = 6), adjustment disorders (n = 1), and communication disorders (n = 4). Individuals with what some may consider more severe psychopathology (e.g., Asperger’s disorder and personality disorders) were excluded from participation.
Descriptive Characteristics
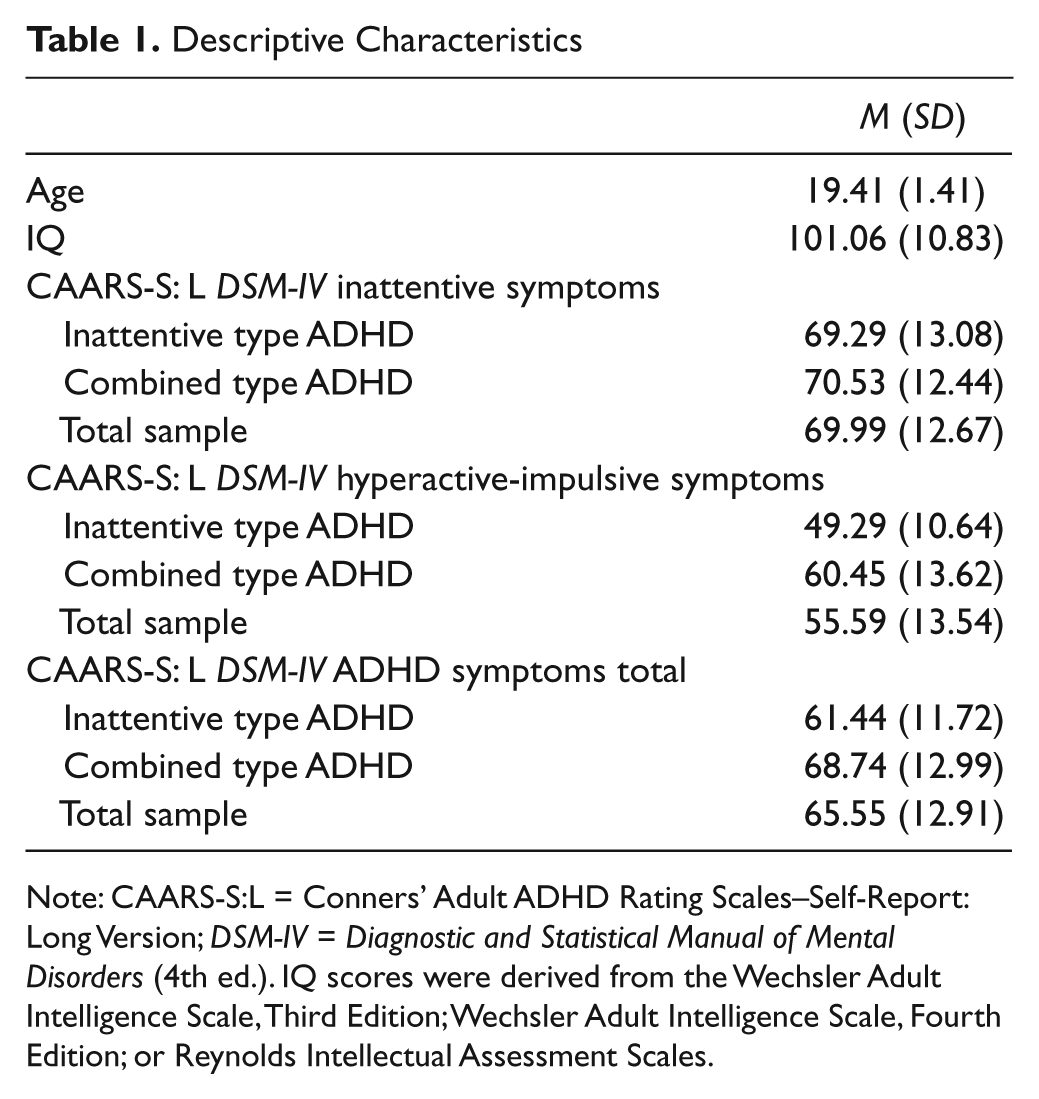
Note: CAARS-S:L = Conners’ Adult ADHD Rating Scales–Self-Report: Long Version; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.). IQ scores were derived from the Wechsler Adult Intelligence Scale, Third Edition; Wechsler Adult Intelligence Scale, Fourth Edition; or Reynolds Intellectual Assessment Scales.
Instruments
The dependent variables were measured with the Problems With Self-Concept subscales of the CAARS-S:L and CAARS-O:L. The Problems With Self-Concept subscales are made up of 6 items embedded within the larger 66-item CAARS. Rated on a 4-point Likert-type scale indicating the frequency of problems with self-concept, each item is identical in content across the two forms of the CAARS except for different pronouns and slightly different wording to account for the perspective of the informant. The content of the items relates to the frequency in which individuals are unsure of themselves, get down on themselves, and lack belief in their abilities. Both Problems With Self-Concept subscales have a mean of 50 and a standard deviation of 10.
Evidence supportive of reliability and validity for both forms of the CAARS Problems With Self-Concept subscale was provided in the technical manual (Conners, Erhardt, & Sparrow, 1999c). Reliability evidence was disaggregated by gender and indicated internal reliability coefficients of .88 for males and .87 for females in the 18- to 29-year-old age range for the Problems With Self-Concept subscale of the CAARS-S:L. A 1-month test–retest reliability coefficient of .91 for this subscale was found across the total normative sample. Similar results were found for the CAARS-O:L Problems With Self-Concept subscale, with internal reliability coefficients of .90 for males and .88 for females and a 2-week test–retest reliability coefficient of .87. For both CAARS forms, the test authors also provided validity evidence from confirmatory factor analyses indicating that the Problems With Self-Concept subscales fit well as separate factors within their larger models inclusive of ADHD symptomatology.
Procedure
Participants and one of their parents completed the instruments as part of a comprehensive evaluation at the clinic. Self-report rating scales were completed at the clinic. Parents who accompanied their children to the evaluation completed the observer-report rating scale while at the clinic. Those who did not accompany their children were telephoned and asked to complete the rating scale. Participants gave informed consent to participate in the study, and an Internal Review Board approval was attained prior to conducting the study.
Results
Self-Reported Problems With Self-Concept
As indicated in Table 2, participants self-reported few problems with self-concept. The simple t test computer program (Watkins, 2002) was used to compare the participants’ reports of problems with self-concept with those of the 18- to 29-year-old cohort (n = 261) from the normative sample of the CAARS-S:L. Results indicated no difference in reports of problems with self-concept between the two groups, t(354) = .30, p = .77.
Means and Standard Deviations on Self-Concept Measures

Note: CAARS-S:L = Conners’ Adult ADHD Rating Scales–Self-Report: Long Version; CAARS-O:L = Conners’ Adult ADHD Rating Scales–Observer-Report: Long Version. CAARS-S:L and CAARS-O:L Problems With Self-Concept subscales have a mean of 50 and standard deviation of 10.
Parent-Reported Problems With Self-Concept
Parent-reports of problems with self-concept of the participants resulted in a mean of 59.65 and standard deviation of 10.64. Compared with those completing the CAARS-O:L from the 18- to 29-year-old cohort (n = 267) of the normative sample, parents reported significantly more problems with self-concept, t(360) = 7.94, p < .001. The effect size for this difference was large (d = .95).
Role of Gender, ADHD Subtype, Level of Educational Attainment, and Comorbidity
Table 2 displays the means and standard deviations disaggregated by gender, ADHD subtype, level of educational attainment, and comorbidity. No differences in self-reported problems with self-concept were found based on gender, F(1, 93) = .14, p = .71; ADHD subtype, F(1, 93) = 1.14, p = .29; level of educational attainment, F(1, 93) = 2.41, p = .12; and comorbidity, F(1, 93) = 1.70, p = .20. Likewise, no differences were found for parent-reports of problems with self-concept based on gender, F(1, 93) = .20, p = .65; ADHD subtype, F(1, 93) = 1.41, p = .24; level of educational attainment, F(1, 93) = .001, p = .98; and comorbidity, F(1, 93) = .10, p = .75.
Comparison of Self- and Parent-Reports
The correlation between self- and parent-reports of problems with self-concept was statistically significant, r = .36, p < .001. Parents reported significantly more problems with self-concept for the participants than the participants reported for themselves, t(94) = 7.20, p < .001. The effect size for this difference was large (d = .84). The distribution of difference scores for self- and parent-ratings was examined to further understand interrater differences. Skewness (.23) and kurtosis (−.38) statistics indicated a normal distribution. Difference scores ranged from −16 to 38, with a mean, median, and mode of 9.28, 8.5, and 8, respectively.
Discussion
Results of the self-report of self-concept analysis indicated that college students with ADHD reported problems with self-concept no more than did the average young adult from the standardization sample of the CAARS. This result is similar to Wilmhurst et al.’s (2011) finding that college students with ADHD at a small private university did not report significantly different general self-concepts than did college students without ADHD. In contrast, Shaw-Zirt et al. (2005) found that college students at a large Catholic university reported greater problems with self-esteem than did college students without ADHD. It should be emphasized that, although similar to these studies, the current study is not directly comparable because a control sample of college students without ADHD was not included. In addition, mixed results between studies such as these may occur because of differences regarding how self-concept is defined and measured. In all three studies, a different instrument was used to measure self-views. Furthermore, self-esteem rather than self-concept was examined in the Shaw-Zirt et al. study. Although the terms self-esteem and self-concept are often used interchangeably, they are at times used to describe slightly different constructs. Some have argued that self-concept represents a cognitive evaluation of oneself, whereas self-esteem is more affective or emotional in nature (for a discussion of this issue see Swann et al., 2007). In addition, self-concept is sometimes conceptualized as representing a broad description of the self, whereas self-esteem is at times described as a more specific construct representing the evaluative judgment of the self (Elbaum & Vaughn, 2001). These nuances in construct meaning might partially explain the different findings between the studies.
Although college students with ADHD did not report problems with self-concept for themselves, their parents reported perceiving such problems for them. The difference between self- and parent-reports was statistically significant and large in magnitude (d = .84), and the relationship between self- and parent-reports of self-concept, although statistically significant, was moderate in magnitude (r = .36). Similar levels of modest interinformant agreement have been found when adult self-reports and observer-reports of internalizing and externalizing psychopathology have been compared (Achenbach et al., 2005). Such discordance between informants easily leads to hypotheses as to which, if any, of the reports is more valid, with subsequent clinical implications regarding the interpretive weight afforded to each report.
Many hypotheses could be logically developed to explain the low interinformant agreement between college students with ADHD and their parents when rating self-concept. Two general hypotheses that are perhaps most intuitive include (a) self-reports as more valid than parent-reports and (b) parent-reports as more valid than self-reports. Regarding the first of these hypotheses, the main assumption is that the individual whose self-concept is being assessed has the most intimate knowledge of oneself, including knowledge to which others are unlikely privy. Because of this open access to discreet information, individuals themselves can be viewed as the only informants who can fully express self-perceptions, whereas others’ perceptions are limited because they are derived only from observable behaviors. In the case of the self-concept of college students with ADHD specifically, it might be that the various challenges posed by the disorder and subsequent personal failures experienced as a result of these challenges are countered by the ultimate overcoming of odds as manifested by their admittance to college and pursuit of a college degree. College students with ADHD are a minority subgroup within the general adult population with ADHD; the vast majority of young adults with ADHD do not attend college (Wagner, Newman, Cameto, Garza, & Levine, 2005). Therefore, they may be a particularly resilient group (Wilmhurst et al., 2011) with well-developed compensatory skills (Frazier et al., 2007), permitting the maintenance of positive general self-concept, an attribute that in turn may further foster success. Despite these adaptive personal characteristics, the disorder and its associated challenges remain, however, making it more difficult for college students with ADHD to succeed than it is for most college students without ADHD. Parents of college students with ADHD may observe the continued struggles associated with the disorder and assume, albeit reasonably, that these challenges negatively affect their children’s self-concept even if they do not. Parents’ perceptions may be susceptible to a “halo effect” or the inaccurate perception of an additional problem in the presence of an established problem (Biederman, Mick, & Faraone, 1998).
A starkly contrasting hypothesis for the discordance between informants is the possibility that due to problems with metacognitive awareness, the self-reports of college students with ADHD may be compromised, whereas parent-reports may be more consistent with objective reality. Within this hypothesis, a positive illusory bias is thought to limit the self-appraisals of individuals with ADHD. Although overly positive self-appraisals are normative and conducive to adaptive psychological functioning for the general adult population (Taylor & Brown, 1988), the positive illusory bias of individuals with ADHD is thought to be atypical. Damage to the frontal lobes has been hypothesized as an etiological factor for problems with self-appraisal and self-awareness among individuals with ADHD (Barkley et al., 2002; Knouse et al., 2005) because of the empirically supported association between ADHD and atypical functioning in the prefrontal cortex (for a review see Barkley, 2006) and the role of the prefrontal cortex in executive functioning and metacognition (Fuster, 1997). Appraising oneself is, in part, a metacognitive task in that the individual must evaluate various sources of information, monitor incoming information, compare and contrast incoming information with previous information, and so on. Recruiting others to share their perceptions lessens some of the problems inherent in relying on the self-reports of those with metacognitive difficulties. Although the current study is the first to investigate self- and other-reports of self-concept for adults with ADHD, other studies have examined self- and parent-ratings of ADHD symptomatology and their relationship with various aspects of functioning. For example, relative to self-reports of ADHD symptoms for young adults, parent-reported symptoms have been found to be more predictive of impairment in educational, occupational, and social functioning (Barkley et al., 2002), suggesting greater validity of parent-reports.
Within each of the above-mentioned general hypotheses, numerous reasonable arguments could be made for supporting one type of report and minimizing another. It should be highlighted that, although the hypotheses were derived from the extant theoretical and empirical literature, they have not been tested empirically. As a gold standard by which multiple informant reports could be evaluated has not been established, quite different pictures of the self-concept of the young adult with ADHD will likely form depending on the informant report that is relied on the most. Future research testing these and additional hypotheses will need to be conducted to provide guidance in interpreting interinformant discordance.
Limitations
Several limitations should be kept in mind when interpreting the results of the current study. First, because a control group of college students without ADHD was not used, comparison of individuals in similar environments could not be made. It should be highlighted that the control group used in the current study was the nearest-aged subsample from the normative sample of the self-concept instrument. Adults from the normative sample and typical college students likely differ on a variety of characteristics and experiences that might directly or indirectly impact self-concept. Therefore, it is important to avoid interpreting these findings as suggesting no differences in the self-reports of self-concept between college students with and without ADHD. Second, investigating the perceptions of parents of college students without ADHD would have helped determine how unique the discrepancy between self- and parent-reports of self-concept in the current study was to college students with ADHD and their parents. Third, the instruments used to measure self-concept in the current study consisted of only six items each. Although psychometric evidence was available in support of score reliability and validity of the instruments, it could be argued that the number of items was insufficient for adequately and thoroughly measuring the construct under investigation. Fourth, generalizability of results may be negatively affected by the inclusion of a select group of students from only one region of the United States and who were generally ethnically homogeneous. The participants were individuals who sought comprehensive psychological evaluations, often to determine their eligibility for academic accommodations. These individuals may differ from college students with ADHD who do not participate in such services. Finally, because interrater agreement procedures for ADHD diagnoses were not used, there may be some concerns regarding the veracity of these diagnoses. The use of an extensive evaluation to determine diagnoses may lessen some of the concerns; however, diagnostic agreement between two independent evaluators would have likely eliminated these concerns.
Implications for Research and Practice
Several directions for future research can be drawn from the results and limitations of the current and similar previous studies. First, future research in which self-concept is conceptualized and measured from multidimensional and global perspectives would lead to a more thorough understanding of the self-concept of college students with ADHD. Second, inclusion of samples of college students without ADHD and similarly aged adults with ADHD who do not attend college for comparison with college students with ADHD would aid in determining the potentially unique characteristics of the latter group. Comparing the self-concept of college students with ADHD and young adults with ADHD who do not attend college would be particularly informative, especially if other variables (e.g., general cognitive ability, specific cognitive abilities, and important demographic factors) were included in these analyses. Such research could lead to a better understanding of the reasons that some young adults with ADHD attend college, whereas most do not. Third, including measures of important life outcomes along with self- and other-reports of self-concept would be informative because regression analyses to determine how well these reports predict the former would aid in determining the validity of self- versus other-reports.
Regarding implications for practice, the current study’s results underscore the importance of multi-informant assessment for college students with ADHD. Including self- and other-reports in the assessment of college students with ADHD is likely to result in unique information from each source, thus providing a more complete clinical picture. As information from multiple informants is unlikely redundant, low cross-informant agreement will often result, leading to the need for clinical judgment to determine the interpretive weight that should be afforded the information provided by each informant source. At times self-reports may carry more interpretive weight than do other-reports and vice versa. Interpretive decisions such as these should be made on a case-by-case basis, and a priori assumptions that one source is more valid than another should be avoided. Instead, the clinician must carefully consider the personal characteristics and environmental circumstances that contribute to the perceptions of multiple informants when determining possible problems with self-concept among college students with ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.