
Abstract
The available literature provides few studies on the effectiveness of methylphenidate in improving quality of life in individuals with ADHD.
Keywords
Introduction
ADHD is one of the most common mental disorders in adulthood, affecting up to 4.5% of North American individuals (Kessler et al., 2006). ADHD symptoms are associated with a wide range of impairments over life course (Knouse et al., 2008) and individuals presenting more symptoms present worse indicators of global functioning and greater functional impairment. Adults with ADHD have lower levels of quality of life (QoL; Able, Johnston, Adler, & Swindle, 2007). However, generic QoL scales—such as SF-36—may not correlate to symptoms of a specific disorder such as ADHD, indicating the need for specific QoL instruments (Adler et al., 2006). Brod, Johnston, Able, and Swindle (2006) validated the Adult ADHD Quality of Life Scale (AAQoL), a Likert-type scale consisting of 29 items distributed in the following four subscales: Productivity (11 items), Psychological Health (6 items), Life Perspectives (7 items), and Relationships (5 items). This questionnaire has been translated to Portuguese and validated for use in Brazil by Mattos, Coutinho et al. (2011) and Mattos et al., (2011). Brod et al. demonstrated that individuals with ADHD had worse QoL scores when compared with controls and subthreshold groups (below Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV; American Psychiatric Association, 1994]–suggested cutoff points). There was a negative correlation between Adult-Self Report Scale (ASRS) scores and QoL, with more severe symptoms of ADHD associated with lower levels of QoL.
Some studies have demonstrated that psychopharmacological treatments may improve QoL of ADHD individuals (Adler et al., 2006; Goodman, Ginsberg, Weisler, Cutler, & Hodgkins, 2005), but those findings need to be replicated in other sociocultural and socioeconomic contexts, like Brazil. Methylphenidate (MPH) is the most commonly prescribed stimulant drug for ADHD in Brazil. Treatment with stimulants, such as MPH, has shown to improve symptoms of ADHD in children and in adults (Mattos, Palmini, et al., 2006). A recent longitudinal study showed that individuals with ADHD treated since childhood had better measures of QoL and social and psychological functioning in adulthood, suggesting that treatment with stimulants may improve QoL (Goksoyr & Nottestad, 2008).
Our objective was to assess the effectiveness of long-acting MPH through the impact on QoL in adults with ADHD in a 12-week follow-up study. Based on previous findings, we hypothesized that treatment with long-acting MPH (OROS MPH) would improve QoL scores of individuals with ADHD.
Method
This was a Phase IV, multicenter, open-label, 12-week, follow-up study conducted in Brazil. We included individuals of both genders with a clinical diagnosis of ADHD based on DSM-IV criteria, aged 18 to 65 years old.
No participant had been treated with psychostimulants during the 4 weeks prior to the first visit. After having been diagnosed and considered eligible, the individuals were informed about the trial and signed an informed consent form. All individuals were interviewed with an adapted version of Schedule for Affective Disorders and Schizophrenia for School Aged Children, Present and Lifetime (K-SADS-PL; Grevet et al., 2005) to investigate present and past ADHD symptomatology. The onset of at least some of the symptoms must have been before the age of 7. Individuals with comorbid mood disorders, autism or Asperger’s syndrome, Tourrette’s syndrome, mental retardation, substance abuse, clinical unstable disorders, or Hamilton’s Depression Rating Scale (HAM-D) suicide item higher than 2 were excluded from the study. Assessments included Adult Self-Report Scale (Mattos, Segenreich, et al., 2006) of ADHD symptoms (ASRS) to evaluate ADHD symptoms, AAQoL, Clinical Global Impression–Severity (CGI-S), Clinical Global Impression–Improvement (CGI-I); State and Trait Anxiety Inventory (STAI), and HAM-D. Participants started with 18 mg of long-acting formulation of MPH (OROS MPH) once a day (in the morning). After 8 days, the dose was increased, and participants were maintained on 36 mg for the following 20 days. If necessary, and depending on therapeutic response, the dose could be increased to 54 mg (Day 28) and to a maximum dose of 72 mg (2 capsules of 36 mg) on Day 56 to reach the optimum dose for each participant. Sample size was calculated using two-sided paired t test (with baseline and final visit measures being considered the dependent samples), based on the effect size of MPH on ADHD symptoms (Faraone, Spencer, Aleardi, Pagano, & Biederman, 2004), considering an alpha of 5% and a beta of 20%. The study sample consisted of 60 patients [sample intention to treat (ITT) ITTs]. All patients who received OROS MPH in at least one occasion and provided ≥ 1 measure post baseline of efficacy were included in the efficacy data analysis (ITTe). The efficacy was evaluated through the mean change from the baseline on ADHD Self-Report Scale and on AAQoL.
The overall severity and change in severity of ADHD were assessed with CGI, which includes scales for Global Severity (1 = not ill to 7 = extremely ill) and Global Improvement (1 = very much improved to 7 = very much worse).
The changes in comorbid anxiety or depressive symptoms were measured as mean change from baseline on STAI and HAM-D scores.
The analysis of variance technique was applied to longitudinal data using a mixed linear model with week of treatment as a fixed effect and the presence of significant effect of factor differences between weeks were located by contrasts. Statistical tests for differences between the outcome (last visit) and the baseline were interpreted at a level of significance of 5%.
The study was approved by Ethics and Research Committees of all sites involved.
Results
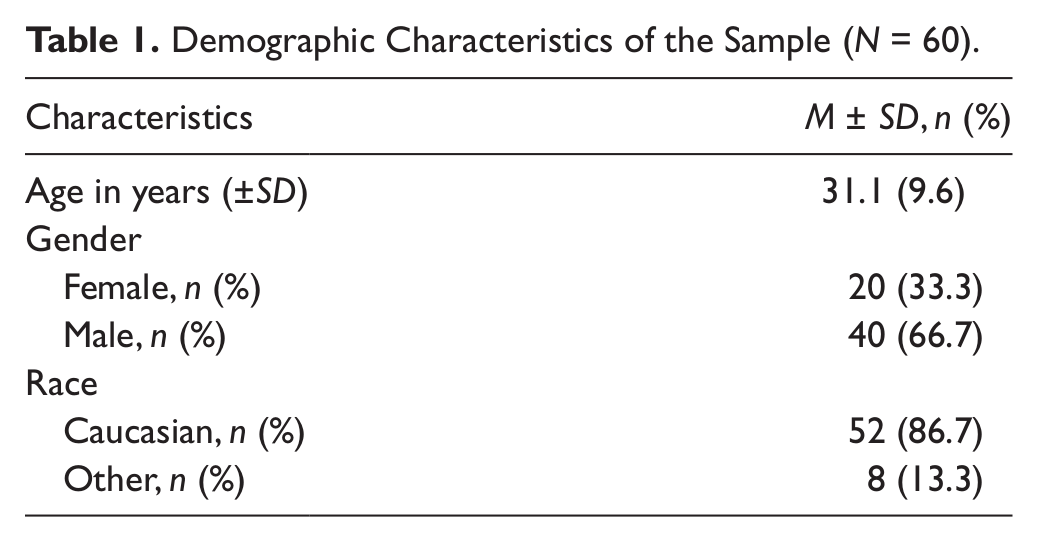
Our sample initially comprised 62 ADHD-diagnosed individuals according to strict DSM-IV criteria. Two individuals were excluded from the analysis due to lack of adherence. Our final sample comprised 60 individuals. The profile of the final sample is described in
Demographic Characteristics of the Sample (N = 60).
The sample for safety analysis comprised 60 patients who received the study drug for at least one dose and provided at least one measure post baseline of safety. Three patients withdrew before the end of the study due to the occurrence of adverse events including diarrhea, abdominal pain, dry mouth, and insomnia (1 patient); loss of appetite, dry mouth, and insomnia (1 patient); anxiety (1 patient). No severe adverse events were reported in any of the site throughout the study. Most adverse events were reported unevenly during the 12 weeks, often present in one visit but not in the others. The most common adverse events considered by the physician as probable or very probable related to the drug reported on Week 12 were decreased appetite (25%), dry mouth (16.7%), headache (11.7%), irritability (5%), and insomnia (5%).
ADHD symptom severity improved with the ASRS scores (total, inattention, and hyperactivity) significantly reduced from baseline at the consecutive evaluations at Weeks 4, 8, and 12 (
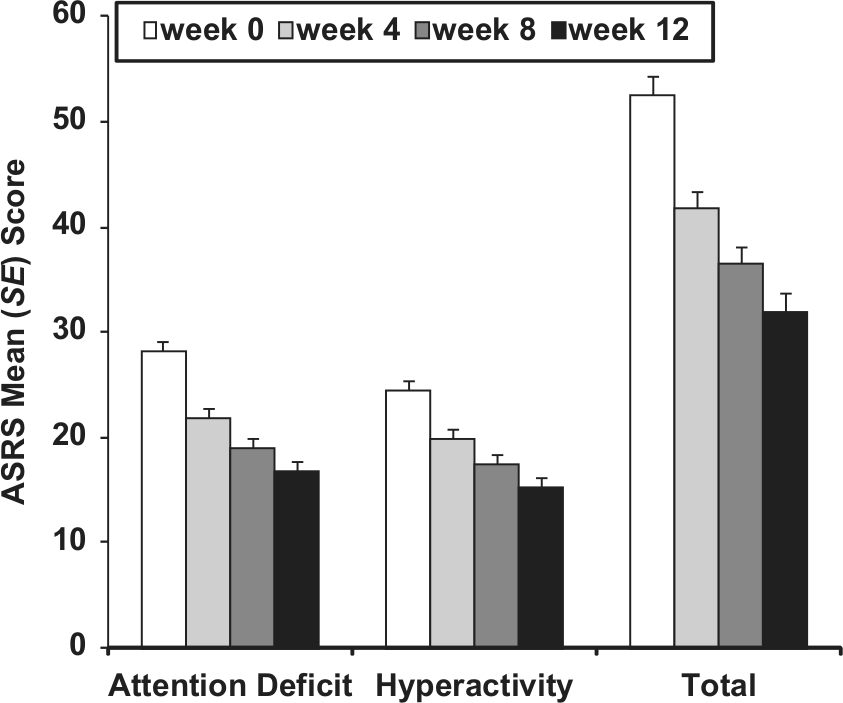
Changes in ASRS scores along the weeks.
We also found significant improvements from baseline in AAQoL both on total score as well as on each subscale (p < .0001 for all comparisons; see

Mean change of AAQoL scores along the weeks.
Scores of CGI also improved across weeks (
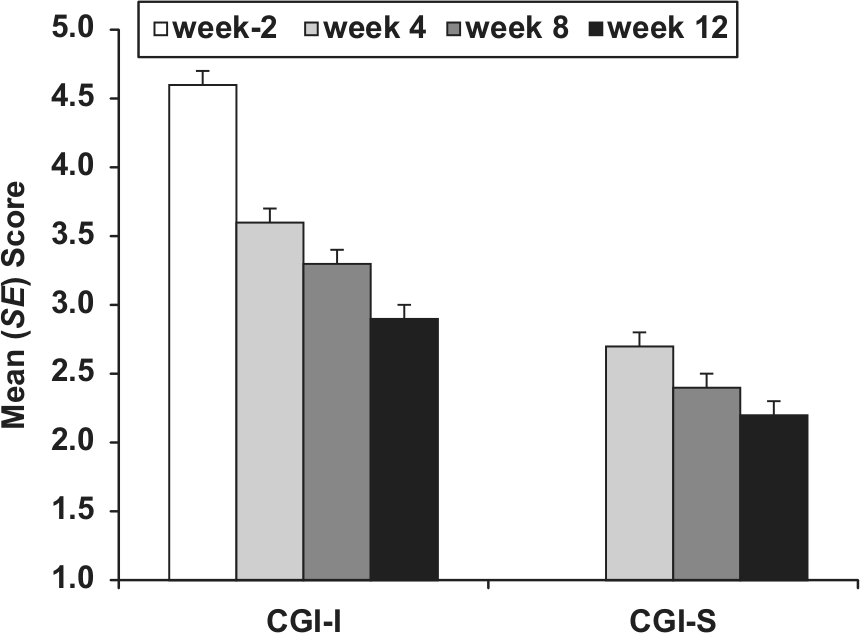
Mean change of CGI along the weeks.

Mean change of HAM-D along the weeks.
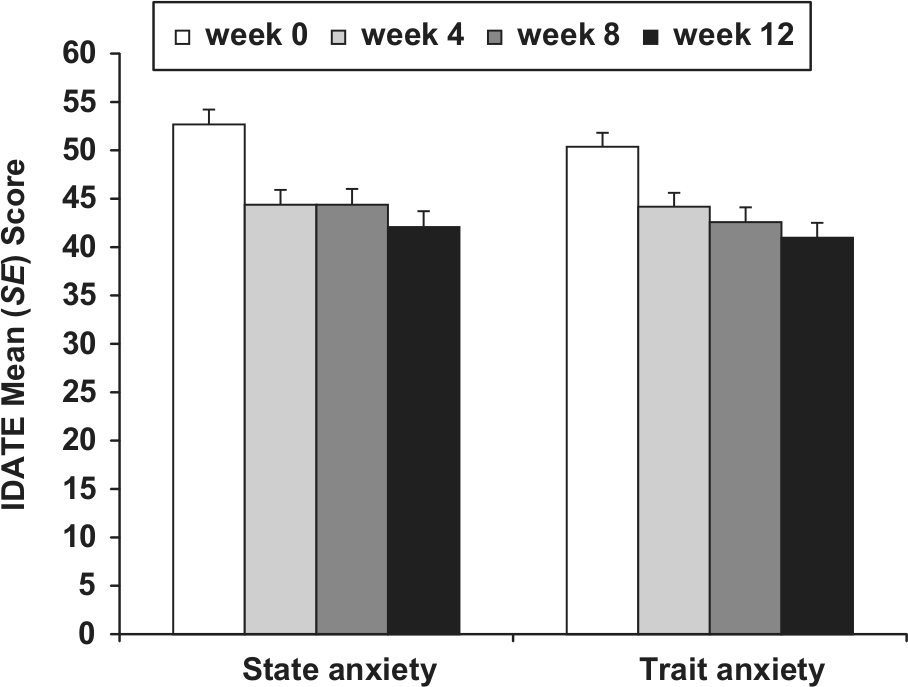
Mean change of STAI along the weeks.
Discussion
This is the first Brazilian study in adults with ADHD assessing the effectiveness of a psychostimulant on QoL variables. AAQoL is the only instrument available in our country to specifically assess QoL of individuals with ADHD. Only one study addressed the effectiveness of long-acting MPH in Brazil, but this study comprised a sample of adolescents with substance use disorder and did not investigate measures of QoL (Szobot et al., 2008). Given the evidence of lower levels of QoL among adults with ADHD when compared to non-ADHD controls (Able et al., 2007), it is important to evaluate how individuals might benefit from stimulant treatment considering the burden in various aspects of the everyday life. The assessment of QoL indicators provides a better understanding of the outcome of many different psychiatric disorders, where correlation between severity of symptoms and the impact on patient’s life is uncertain, like ADHD (Gathje, Lewandowski, & Gordon, 2008). Findings of sociological studies have demonstrated that many objective factors (education, income, etc.) may be only marginally related to the perception of the quality of the individual’s own life (Gill & Feinstein, 1994).
All QoL indexes measured by the AAQoL in our study improved with stimulant treatment: productivity, psychological health, relationships, and life perspectives. Symptoms of ADHD (total, inattention, and hyperactivity) evaluated by the ASRS, improved with the 12-week use of long-acting MPH as well as CGI scores. All but one individual who started the study completed all visits, which reinforces the advantages of long-acting MPH treatment in terms of adherence.
Although anxiety and depression are possible side effects related to the use of MPH, symptoms of anxiety and depression (STAI and HAM-D, respectively) also improved with the treatment with long-acting MPH. It seems reasonable to hypothesize that the decrease of ADHD symptoms, lower levels of functional impairments, and better QoL were responsible for the diminishing anxious and depressive symptomatology. It must be noted that no participant presented major depressive disorder or dysthymia during the study.
Our findings are in accordance with the findings of other studies that revealed that treatment with stimulants improved QoL of adults with ADHD (Able et al., 2007; Goksoyr & Nottestad, 2008). It must be noted that in the aforementioned studies, the improvement of QoL was associated with a decrease of ADHD symptoms due to the effect of the drug treatment. Again, study’s results corroborate the findings above.
Conclusions
This study provides the first evidence of QoL improvement in a Brazilian clinical sample of adults with ADHD treated with long-acting MPH (OROS MPH).
Limitations
We did not study individuals with comorbid substance use or abuse, a common comorbid condition. Also, our design was not double blind, and we did not use a placebo arm. An open-label study without a comparison group cannot determine how much of the change observed is a spontaneous variability of the disorder, how much the placebo effect is, and how much it is attributable to treatment with the active drug. Titration was performed at physician’s discretion and had no connection with prespecified quantified decrease in symptoms; greater improvements might have been seen with a clearer titration schedule.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Paulo Mattos is either an independent consultant, belongs to the advisory board or has received institutional research grant from Janssen-Cilag, Lilly, Novartis and Shire.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Janssen-Cilag Brazil.