
Abstract
ADHD is a chronic neurodevelopmental condition characterized by the presence of inattention, impulsivity, and hyperactivity. ADHD still remains the most often diagnosed psychiatric disorder with prevalence ranging from 3% to 9% (Polanczyk et. al., 2007) The differences in prevalence seem to be the result of different sampling and diagnostic criteria applied. Follow-up studies show that from 30% to 80% of children diagnosed with ADHD still remain symptomatic in adolescence (Klein & Mannuzza, 1991; Lambert, Hartsough, Sassone, & Sandoval, 1987). The prevalence for adult ADHD in the community is 4% to 5% (Wilens et al., 2003).
Patients with ADHD also present more academic difficulties, poor social skills, low self-esteem, and emotional problems than do people without ADHD (Fisher, Barkley, & Fletcher, 1993).
There has been a lot of discussion in the literature regarding the possible association between ADHD and other psychiatric conditions especially bipolar disorder (BPD; Sachs, Baldassano, & Truman, 2000; West, McElroy, Strakowski, & McConville, 1995) and Asperger’s syndrome (AS; Goldstein & Schwebach, 2004). The reasons for the controversies can be explained by similarity of the symptoms of disorders as is the case in BPD or by the complexity of symptoms as in case of AS, which may overshadow the presence of symptoms of ADHD. Although the presence of symptoms of hyperactivity in patients with AS has been described by many authors (Fombonne, Simmons, Ford, Meltzer, & Goodman, 2001; Goodman, 1999), the present diagnostic criteria still exclude common diagnosis of ADHD and pervasive developmental disorder (PDD).
The majority of follow-up studies in ADHD focuses on the assessment of functioning, symptoms decline, identification of early predictors, or moderators of outcome. Methodological issues differ with respect to design, diagnostic criteria, participant characteristics, and assessment methods (Ingram, Hechtman, & Morgernstern, 1999). Although the initial diagnosis of ADHD is always accompanied by detailed differential diagnosis, the follow-up examination is often limited to the presence of ADHD or to identification of comorbid conditions. What is interesting is that we were unable to find a follow-up study in which patients with ADHD were diagnosed with disorders that exclude the diagnosis of ADHD such as schizophrenia or AS, at follow-up. Although the main goal of the study presented in this article was to test the functioning of patients with ADHD 6 to 8 years after the diagnosis, the decision was made to determine whether there has a been a symptoms decline, subtype change, and diagnosis migration as well.
Method
Participants
All participants were patients of the Outpatient Department of Child Psychiatry in Warsaw, Poland, diagnosed with ADHD at first assessment in 2002 (SD = 2.43, M = 10.27; Kołakowski, 2002). Out of the 291 patients diagnosed with ADHD for the purpose of another study, 180 were successfully contacted (159 males and 11 females). From this group, 101 were chosen for follow-up procedure (93 males and 8 females). Ages at follow-up ranged from 12 to 17.2 years (SD = 2.48, M = 17.3). A total of 45% of participants attended middle school, 40% attended high school, and 15% attended college. All participants were Caucasian. Of the participants, 70% had been prescribed medication at some point of the study. Follow-up period ranged from 6 to 7 years. A total of 79 participants refused to participate.
An initial diagnosis of ADHD at the beginning of the follow-up was done by psychiatrists specializing in child psychiatry. The diagnostic procedure was based on the developmental interview, rating scales, and the ADHD module of Kiddie-Schedule for Affective Disorders and Schizophrenia-Polish Version (K-SADS-PL) and information from school.
The patients above the cutoff scores in the rating scales were selected for K-SADS interview. Those above-cutoff scores in rating scales and K-SADS were coded as having ADHD. All participants met the criteria for ADHD according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). Exclusion criteria included a diagnosis of autism or PDD.
Follow-Up Measures
The following measures were collected at the time of follow-up:
Age: Age of each child at the time of follow-up was measured
Length of follow-up
Conners’ Parent Rating Scale
The presence of ADHD. The participants were diagnosed for the presence of ADHD by a trained psychologist.
Change of diagnosis. Patient records were analyzed for the change of diagnosis.
Data analysis
The article presents descriptive data regarding symptoms, subtype, and diagnosis change. The analysis of the course of ADHD was made on the basis of the percentage of confirmed ADHD cases, including subtypes, at follow-up. Length of the follow-up was calculated as the difference between ages at initial assessment and at follow-up.
Results
Out of 291 patients, 61.8% (n = 180) were contacted and 56.1% (n = 101) agreed to participate in further testing. In all, 23 participants refused to participate although they fulfilled the inclusion criteria, which included the presence of ADHD as well as comorbidities such as oppositional defiant disorder (ODD) and conduct disorder (CD) at initial assessment, and inclusion in health care systems (see Figure 1). Other patients contacted (n = 79) were not included in health care systems (n = 56) or refused to participate (n = 23). From the contacted group, 77% of patients were rediagnosed with AS, 2.2% (n = 4) received a diagnosis of BPD, 2.2% (n = 4) were diagnosed with mental retardation, 1 patient with schizophrenia, and 1 with Smith–Magenis Syndrome; 1 patient had died. Those patients who were rediagnosed as having BPD or AS were not rediagnosed for ADHD. They were also not included in the remission group.

Characteristics of the group contacted for follow-up.
The analysis of the course of ADHD was made on the basis of the percentage of confirmed ADHD cases, including subtypes, at follow-up. Summary is presented in Figures 2, 3, and 4.
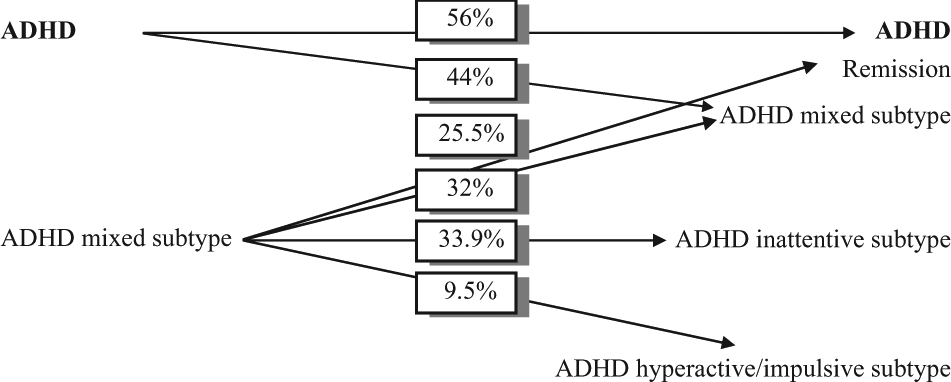
The course of ADHD and the course of ADHD mixed subtype.

The course of inattentive subtype.
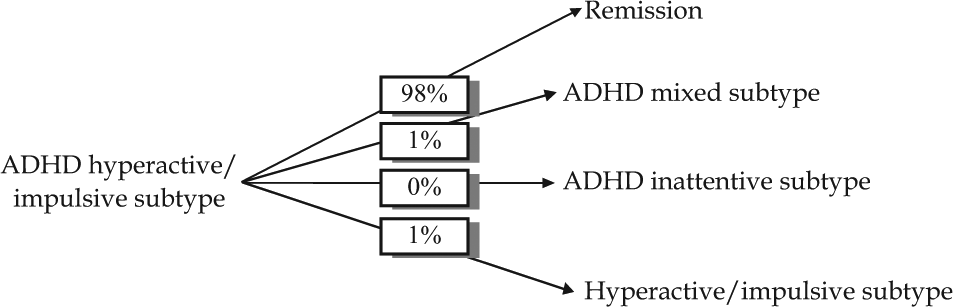
The course of hyperactive/impulsive subtype.
In total, 56% of patients with ADHD still met the criteria for the disorder. Full remission was observed in 25.5% of patients with primary mixed subtype, 32% received the same diagnosis, 32% were diagnosed with inattentive subtype, and 9.5% were diagnosed with hyperactive/impulsive subtype (see Figure 2).
Only 11% of patients with primary inattentive subtype still met the criteria for ADHD: 3% were diagnosed with mixed subtype, 5% with inattentive subtype, and 3% with hyperactive-impulsive subtype (Figure 3).
As much as 98% with primary hyperactive-impulsive subtype did not meet the criteria for ADHD at follow-up. Only one participant was rediagnosed with the same subtype and one with mixed subtype (see Figure 4).
Discussion
Limitations of the Study
The study has certain limitations that need to be taken into account when considering the study and its contributions. First of all, the prevalence and comorbidity of affective and anxiety disorders as well as AS was not well established in the group contacted for follow-up at baseline diagnosis. This was due to the fact that ADHD was still a new diagnosis in Poland 10 years ago and the main focus of psychiatrists was to determine the presence of that disorder. What is more is that, little was known about the diagnosis of AS, which could have contributed to false-positives diagnosis of ADHD and explain the change of diagnosis during the follow-up period. Another limitation is the type of pharmacological interventions applied for the treatment of ADHD. Majority of patients received tricyclic antidepressants (TPA) as a basic pharmacological intervention. This was caused by lack of registration of psychostimulant drugs and their limited availability. Criticism can also be presented when considering the prevalence of comorbid disorders such as ODD and CD in the study group, which hindered the homogeneity of the study group. In conclusion, the study contribution is limited due to the type of pharmacological interventions, the specificity of the baseline diagnosis, and group characteristics.
Subtypes and Remissions
There is a scarcity of research in the literature testing the course of ADHD and its subtypes. A 15-year follow-up study (Weiss & Hechtman, 1986) showed that 66% of patients with ADHD still had symptoms from at least one group: impulsivity, hyperactivity, or inattention. Lambert et al. (1987) found that after 3 to 4 years of diagnosis, 43% of males still met the criteria for ADHD. Neither the number of symptoms nor subtypes were described at follow-up. In a prospective 8-year follow-up study, Gittelman, Mannuzza, Shenker, and Bonagura (1985; M age = 18) observed symptomatic remission in 68.5% of participants. Barkley et al. (1990) observed full remission in 28.5% of participants in another prospective 8-year follow-up study on 123 boys aged 4 to 12 years. It is worth noticing that results of the present study are comparable with results of other researches.
The results of the study do not show the age at which the symptoms start to decrease. It is likely that the greatest decrease of symptoms takes place quite soon after the diagnosis. Taylor, Sandberg, Thorley, and Giles (1991) showed that 36.5% of boys aged 6 to 7 years did not meet the criteria for ADHD 9 months after the diagnosis. Such a result is very interesting and very often observed in clinical practice both in patients included and not included in health care systems. Such decrease may be explained by the psychological effect of diagnosis. A number of studies shows that environmental factors, such as parental attitudes, play an important role in successful response to treatment (Coleman & Karraker, 1998; Reimers, Wacker, Derby, & Cooper, 1995; Slep & O’Leary, 1998). These factors include parental style, attribution, parental beliefs, and sense of efficacy. A visit to a psychiatrist, diagnosis, and psychoeducation may modify the perception of child’s behaviors and cause change in behavioral strategies used by parents. As a result, undesirable behaviors that are listed in diagnostic criteria for ADHD tend to fade and no longer meet the “significant impairment” criterion in the eyes of caregivers and teachers. Another explanation is connected with the issue of reliability of diagnosis and concentration on symptoms rather than etiology. It is possible that
35% of patients present behaviors which are the result of inappropriate parental strategies,
35% of caregivers introduce appropriate behavioral and pharmacological interventions,
such a high number of spontaneous remissions is related with imperfect diagnostic criteria, and
children are referred to psychiatrist at the peak of the symptoms intensity which tend to decrease with age.
The dynamics of symptoms intensity in our study was heavily influenced by ADHD subtype. The highest decrease was observed in participants with primary diagnosis of mixed subtype. Such result can be explained by the different dynamics of decrease of symptoms of hyperactivity, impulsivity, and inattention (Bauermeister, Alegria, Bird, Rubio-Stipec, & Canino, 1992; Hart, Lahey, Loeber, Applegate, & Paul, 1995). In a 4-year follow-up study on boys (M age = 7), Bauermeister et al. (1992) showed that the greatest decrease in the intensity of symptoms of hyperactivity and impulsivity was observed in the 1st and 3rd year of the study. Symptoms of inattention tend to decrease between 1st and 2nd year of the follow-up and remained stable until the end of the study. The authors did not observe any relationship between age and the decrease of symptoms of inattention in Hart et al.’s study.
The number of remissions in patients with primary diagnosis of mixed subtype in the current study may be related to the decrease of symptoms of hyperactivity and impulsivity with no decrease in symptoms of inattention. Such a result is consistent with the findings of the study: 33.9% of patients with primary diagnosis of mixed subtype were diagnosed with inattentive subtype at follow-up. Analogously, 98% of participants with primary hyperactive-impulsive subtype and 89% with inattentive subtype were not diagnosed with ADHD at follow-up.
Other Diagnosis
In the present study, as much as 7.7% of patients were rediagnosed with AS between the first and the second assessment. At the time of first diagnosis, knowledge about AS was limited among Polish specialists, which might have contributed to change in diagnosis. Another reason for misdiagnosis could have been caused by diagnostic bias. Psychiatrists expected to diagnose ADHD in children whose parents reported impulsivity, inattention, or hyperactivity as chief complaints. The third explanation is related to the presence of ADHD symptoms in PDDs. Lee and Ousley (2006) were testing the frequency of ADHD in children and adolescents with autism spectrum disorders (ASD). In all, 78% of patients with ASD met the criteria for ADHD. Similar results were obtained by Lee and Ousley and by Frazier et al. (2001). Lee and Ousley also found that individuals with ASD had the same distribution of ADHD, regardless of chief complaint being symptoms of ADHD or not.
It is possible that caregivers of participants in the present study were more sensitive to symptoms of ADHD as most of them did have a chance to observe their children in social situations. Kube, Petersen, and Palmer (2002) found that the majority of patients with AS had a chief complaint of ADHD. Taking into consideration the fact that a lot of patients with ASD fulfill the criteria for ADHD, the diagnosis of ASD could have been overlooked.
BPD or mental retardation was rediagnosed in 2.2% of patients during the follow-up period. In case of BPD, such a result seems surprisingly low, taking into consideration the prevalence of ADHD among patients with BPD ranging from 98% in prepubertal manic group (Wozniak et al., 1995), around 70% in early adolescence (West et al., 1995) to 30% in late adolescence (Geller et al., 1998). The possible explanation for such low rate of BPD diagnosis during follow-up may be that patients with BPD dropped out either because they were referred to an inpatient unit or were referred to correction facilities due to behavioral problems.
The later diagnosis of mental retardation could have been the reason of inappropriate or delayed psychological evaluation at first admission and emphasizes the importance of in-depth diagnosis at referral.
Only one case of schizophrenia between follow-up is not difficult to explain, taking into account the different criteria of these disorders. Although in both disorders the major symptoms represent primary cognitive dysfunction, attentional dysfunction is the only common symptom (Golberg, Weinberger, Berman, Pliskin, & Podd, 1987).
In conclusion, the reliability of initial diagnosis was high. The study showed that the rates of all subtypes of ADHD decreased and that more measures need to be taken in terms of differential diagnoses of ADHD and AS.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financed by the Warsaw Medical University as a research grant.