
Abstract
ADHDs occur in 3% to 7% of all youth (American Psychiatric Association [APA], 2000), and are among the most common mental health disorders in pediatric and psychiatric clinic settings (Cantwell, 1996). Youth and young adults with ADHD have significant long-term functional impairment and morbidity (Cantwell, 1996; Mannuzza & Klein, 2000), frequent comorbidity with depressive disorders (Daviss, 2008), and a nearly threefold increased risk of completed suicide relative to the general population (James, Lai, & Dahl, 2004). ADHD was the most common non-mood-related disorder in youth who committed suicide in one study (Brent et al., 1988), and in youth who were offspring of parents with affective disorders and went on to have suicidal attempts or behaviors (SBs) themselves in a second study (Melhem et al., 2007). Although few youth with SB go on to commit suicide, prior SB is the single strongest risk factor for completed suicide (Brent, Baugher, Bridge, Chen, & Chiappetta, 1999; Shaffer et al., 1996). As such, identifying variables most closely linked to SB could help direct services to youth with ADHD at highest risk.
Although there has been little research on SB specifically in youth with ADHD, other risk factors of SB in general pediatric populations have been widely reported (Bridge, Goldstein, & Brent, 2006). SB especially increases not only with depressive or bipolar mood disorders, but also with conduct, oppositional defiant, and substance use disorders (Beautrais, Joyce, & Mulder, 1998; Borowsky, Ireland, & Resnick, 2001; Fergusson & Lynskey, 1995a, 1995b; Gould et al., 1998; Lewinsohn, Rohde, & Seeley, 1994; Weissman et al., 1999). Anxiety disorders are also associated with SB (Gould et al., 1998; Pilowsky, Wu, & Anthony, 1999), but their associations attenuate after controlling for the other comorbidities mentioned (Shaffer et al., 1996). SB rates increase from childhood to adolescence (Bridge et al., 2006). SB also increases with female sex (Fergusson, Woodward, & Horwood, 2000; Grunbaum et al., 2004), but rates of completed suicide are higher in boys because they tend to use more lethal means (Bridge et al., 2006). Other risk factors of SB include conflicted relationships with family (Deault, 2010; Lifford, Harold, & Thapar, 2009; Rey Gex, Narring, Ferron, & Michaud, 1998), and difficulties with peer relationships and social skills (Hawton & Catalan, 1987; Kienhorst, De Wilde, Diekstra, & Wolters, 1995). SB also increases with academic and school attendance problems (Beautrais, Joyce, & Mulder, 1996; Eggert, Thompson, Herting, & Nicholas, 1995), and decreases with academic achievement (Borowsky, Resnick, Ireland, & Blum, 1999; Resnick et al., 1997). Finally, the risk of SB increases with exposure to traumatic events, especially those involving victimization, such as physical or sexual abuse (Fergusson, Horwood, & Lynskey, 1996; Kosky, Silburn, & Zubrick, 1990; Resnick et al., 1997).
Considering these general risk factors for pediatric SB, there are several possible explanations for the increased risk seen in youth with ADHD. First, suicidality may be the direct result of certain ADHD symptoms, given the reported link in general samples between impulsive aggression and SB (Beautrais, Joyce, & Mulder, 1999; Kashden, Fremouw, Callahan, & Franzen, 1993; Kingsbury, Hawton, Steinhardt, & James, 1999; McGirr et al., 2008). If true, then ADHD patients with more hyperactive/impulsive symptoms, or the combined or hyperactive as opposed to the inattentive subtype of ADHD would be more likely to have SB. Second, suicidality in ADHD may be an indirect effect of the long-term impairment associated with ADHD in academic and social domains of function (Mannuzza & Klein, 2000). Third, adverse environmental factors like conflicted parent–child relationships (Deault, 2010; Lifford et al., 2009; Rey Gex et al., 1998) and victimization trauma (Ford et al., 2000) are common in youth with ADHD, and may increase their risk of SB. Finally, ADHD often occurs with comorbid depressive, externalizing, and substance use disorders (Angold, Costello, & Erkanli, 1999; Pliszka, 1998; Spencer, Biederman, & Wilens, 1999), and these comorbid disorders could also account for the increased risk of SB in youth with ADHD.
Few studies, however, have specifically examined potential correlates of suicidality in youth with ADHD. One longitudinal study of adolescent and young adult females reported that the combination of major depressive disorder (MDD) and ADHD carried a significantly increased risk of subsequent suicide attempts compared with either disorder alone (Biederman et al., 2008). A prospective study of youth with ADHD reported that early hyperactive and impulsive symptoms, conduct disorder symptoms, and maternal depression along with female sex were all predictive of eventual SB in adolescence (Chronis-Tuscano et al., 2010). No study to date has simultaneously examined clinical factors like ADHD severity, comorbidity, and impairment, along with environmental factors like parent–child conflict and trauma exposure, as potential correlates of SB in an ADHD sample. Determining such associations could help us to develop causative models for SB in youth and frame targets for therapeutic interventions.
The present study is a cross-sectional, case-control analysis of potential clinical and environmental correlates of lifetime SB in a previously described adolescent sample with ADHD (Daviss, Diler, & Birmaher, 2009). We hypothesized that lifetime SB would be independently associated with clinical factors related to the ADHD severity, especially hyperactive-impulsive symptoms, and impairment in academic and social function, as well as with environmental factors like trauma exposure and parent–child conflict, after controlling for depressive and other comorbidities.
Method
Participants
Participants were youth 11 to 18 years old, enrolled in a study regarding risk factors for depressive disorders in youth with ADHD. The present study examined interview and other clinical data from the first of these participants’ two-study assessments. None in the group without lifetime SB developed it by the time of the second assessment 8 months later.
All participants met criteria for a diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev; DSM-IV-TR; APA, 2000), regarding their symptoms and levels of impairment. Youth whose onsets of ADHD symptoms were up to 9 years of age were allowed, based on the argument for a broadened age of onset criterion for the diagnosis of ADHD (Barkley & Biederman, 1997). Youth with mental retardation or pervasive developmental disorders were excluded. Participants and parents were recruited from an outpatient mental health clinic and research center and from advertisements in a medical center newspaper and were offered a small monetary compensation for their time participating. All were given an explanation of the risks and benefits of the study, and those wishing to participate were asked to sign a consent form approved by the authors’ institutional review board.
The current sample is a subset of a previously reported sample of 104 (Daviss et al., 2009). Among 110 consecutive adolescents who completed initial study interviews, 6 were excluded because they either reported an onset of ADHD symptoms beyond 10 years of age (n = 5) or did not meet full symptom criteria for any subtype of ADHD (n = 1). An additional 3 were excluded from the current sample because their classifications regarding lifetime suicidal thoughts and SB were equivocal due to inadequate documentation. The final sample contained 101 youth.
Diagnostic Evaluations
All participants and their parents underwent separate, semistructured interviews using the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL; Kaufman et al., 1997). Interviews were conducted by one of four masters- or doctorate-level research clinicians under the supervision of the first author. All interviewers underwent extensive training, to achieve acceptable interrater reliability for diagnoses relevant to the present study, as previously reported (Daviss et al., 2009). Participants were classified into subgroups with and without lifetime histories of various comorbidities. Subgroups with lifetime comorbidities included 37 with a lifetime history of MDD, 53 with any externalizing disorder (conduct or oppositional defiant disorder), 6 with any drug or alcohol use disorder, and 32 with any anxiety disorder (social and specific phobias, posttraumatic and acute stress disorders, or separation anxiety, panic, obsessive compulsive, and generalized anxiety disorders).
Lifetime Suicidal Ideations and Behaviors
Youth and parents often give discrepant reports of suicidal ideations and behaviors, and while the general consensus is that youth tend to be better informants of such information than their parents (American Academy of Child and Adolescent Psychiatry [AACAP], 2001), at least one study has suggested that youth with ADHD may be less reliable reporters of depressive symptoms than their parents (Daviss et al., 2006). In the present study, suicidal ideations and behaviors were determined primarily using data gathered in the K-SADS-PL’s depressive screening module. We followed the general guidelines recommended by a consensus panel of experts for assessing suicidality, using separate interviews of the child and parent to assess for a lifetime history of suicidal ideations, suicide gestures, suicide attempts, and self-injurious behaviors (AACAP, 2001). SBs were defined as suicidal gestures, suicide attempts, or self-injurious behaviors carried out in presence of suicidal ideations. In categorizing such behaviors, interviewers were asked to consider all available information and to resolve any differences in accounts between informants when possible. When not possible, interviewers were asked to assign final ratings regarding these symptoms, favoring the report of whichever informant was judged more reliable in each participant’s case.
Potential Correlates of Lifetime SBs
Information about the various measures in the present study and their reliability has been previously reported (Daviss et al., 2009) but is briefly summarized here.
Socioeconomic status
Data about educational levels and occupations of each parent were obtained from the parent, using the Hollingshead 4-factor index (Hollingshead, 1975) to estimate a 5-point rating of socioeconomic status, with scores ranging from 1 (highest) to 5 (lowest).
Severity of ADHD symptoms and signs
The numbers of inattentive and hyperactive/impulsive symptoms at onset of ADHD reaching threshold levels were determined with the K-SADS-PL. Current ADHD symptom severity was rated by the parent, and at least one teacher if possible, using the 18-item ADHD Rating Scale (ARS; DuPaul, Power, Anastopoulos, & Reid, 1998). We followed a recommended method for combining ratings of the same construct from different informants (Piacentini, Cohen, & Cohen, 1992), using all available ARS data from parents and teachers to derive composite scores of inattentive and hyperactive-impulsive symptoms. Baseline parent ARS scores were first standardized for the final sample, determining Z scores for inattentive and hyperactive-impulsive domains. For youth having multiple teacher ratings at enrollment, teachers’ scores for each youth were averaged, and these averaged scores were then standardized. Z scores of −1, 0, and 1 indicated respective levels of ADHD severity that were 1 standard deviation below, at, or 1 standard deviation above the sample’s mean for that informant. A composite score was then calculated, averaging each participant’s parent and teacher Z scores to give equal weight to both informants. In four youth enrolled over the summer without teacher ratings, only standardized scores from the parent were used as their composite score. Last, signs of ADHD severity were measured using the Conners’ Continuous Performance Test–II (CPT-II), a 14-min computerized test in which a series of letters is presented at varying frequencies, and the participant is told to hit the space bar when shown any letter except for the letter “X.” Errors of commission (hitting the space bar when shown an X) and a faster mean reaction time (RT) were used as signs of hyperactivity/impulsivity, whereas errors of omission (failing to hit the space bar when shown another letter than X) were used as a sign of inattention (Conners, 2000).
Impairment
Adolescents rated current social, academic, and other impairment using the 23-item Social Adjustment Scale–Self-Report (SAS-SR; Weissman, Sholomskas, & John, 1981). Parents rated their children’s general impairment with the 13-item Parent Version of the Columbia Impairment Scale (CIS-P; Bird et al., 1993). Like the preceding parent and teacher ARS scores, separate, standardized scores of impairment from the SAS-SR and CIS-P were averaged to derive a final composite score of impairment, with a composite score of 1 indicating a Level 1 standard deviation above the overall sample’s mean. Such composite scores were calculated for overall impairment, and for impairment in academic function, peer relationships, family relationships, and general activities and interests, using relevant items from the SAS-SR and CIS-P.
Current parent–child conflict
The participant and accompanying parent (the mother when both parents were present) completed their respective versions of the 20-item Conflict Behavior Questionnaire (CBQ) to assess current levels of parent–child conflict within the past 2 weeks (Robin & Weiss, 1980). Once again, to derive a composite measure of parent–child conflict, we determined standardized scores of separate child and parent ratings on the CBQ for each participant, then took the average of both standardized scores to derive a final composite score, with higher scores suggesting greater conflict.
Lifetime trauma exposure
The child completed the Trauma Events Screening Inventory-Child Revised Version (TESI-CR). This 14-item questionnaire is adapted from a child interview (Ford et al., 1999) that screens for lifetime exposure to various specific types of traumatic events meeting Criterion A of the DSM-IV-TR for posttraumatic stress disorder (i.e., involving a potential threat to oneself or another’s bodily integrity). Echoing a previous study with the original version of this measure (Ford et al., 1999), we counted all types of traumatic events reported to have occurred, along with types of victimization events (e.g., physical abuse or threats, sexual molestation, mugging, being kidnapped, witnessing community violence, or witnessing family violence or threats; range = 0-9) and nonvictimization events (e.g., serious accidents, disaster, illness of self or others; range = 0-5).
Lifetime hospitalizations and pharmacotherapy
Data about participants’ prior inpatient psychiatric hospitalizations, pharmacotherapy for depression, and lifetime or current pharmacotherapy for ADHD were obtained from the initial treatment section of the K-SADS-PL interview. Stimulants, alpha agonists, and atomoxetine were counted as pharmacotherapy for ADHD, whereas bupropion and tricyclic antidepressants were counted as pharmacotherapy for ADHD and depression. Results were verified by reviewing patient medical records, when available.
Statistical Analysis
Analyses were completed using SPSS-PC Version 18.0 (SPSS Inc., Chicago, IL). An initial univariate analysis (UVA) compared groups with and without lifetime SB in the overall sample and then stratified by sex, using t tests and chi-square tests for continuous and categorical variables, respectively. A series of multivariate analyses (MVAs) with logistic regressions was then used to predict lifetime SB, with each analysis containing one significant correlate of lifetime SB from the UVA of the overall sample, along with demographic and comorbidity covariates. Last, to find the most parsimonious predictive model for lifetime SB, a forward stepwise regression was used, which allowed significant variables from UVA of the overall sample to potentially enter the final model. Given the exploratory nature of the analyses, all p values <.05 were considered significant.
Results
The final sample (N = 101) included 37 girls and 64 boys, with 20 of non-White race. In all, 28 reported lifetime SB from among 39 who reported lifetime suicidal ideations.
UVAs
Table 1 shows results from UVA of the overall sample comparing youth with and without lifetime SB. The lifetime SB group was older, more likely to be female and to have had a lifetime major depressive, externalizing, or substance use disorder. The lifetime SB group also had higher levels of impairment in each of the various functional domains and in parent–child conflict. They also had higher trauma exposure based on total events and victimization events but not nonvictimization events. Youth with lifetime SB were more likely to have experienced domestic violence, physical abuse, or being kidnapped by the noncustodial parent. The lifetime SB group was more likely to have had a psychiatric hospitalization or antidepressant treatment. There were no significant differences in UVA of the overall sample regarding variables related to the severity of ADHD, including current and early symptoms at the time of onset, signs of impulsivity and inattention on CPT-II, and any history of pharmacotherapy for ADHD.
Predictors of Lifetime SB: UVA.

Note: SB = suicidal behavior; UVA = univariate analysis; MDD = major depressive disorder; CPT-II = Conners’ Continuous Performance Test–II. Columns show means ± standard deviations, unless noted as frequencies (percentages).
UVA was repeated for girls and boys separately to see if any predictors of lifetime SB were specific to one sex. Generally, parallel associations across sexes were observed between lifetime SB and various potential predictors when girls and boys were examined separately, but findings for many variables were no longer significant due to smaller sample sizes. However, three variables related to severity of hyperactive/impulsive symptoms, which had no associations to lifetime SB in the overall sample had significant such associations in girls only. First, the combined subtype of ADHD was significantly higher for girls with versus girls without lifetime SB (56.3% vs. 23.8%, p = .044), but not for boys (75.0% vs. 65.4%, p = .523). Second, CPT-II errors of commission were higher for girls with versus girls without lifetime SB (53.2 + 9.5 vs. 45.2 ± 12.6, p = .051), but not for boys (49.6 ± 12.3 vs. 48.4 ± 10.8, p = .760). Finally, faster RTs on the CPT-II were noted for girls with versus girls without lifetime SB (43.2 ± 11.0 vs. 53.2 ± 11.5, p = .015), but not for boys (51.0 ± 13.3 vs. 49.0 ± 12.3, p = .616).
MVAs Controlling for Demographic and Comorbidity Covariates
Table 2 shows odds ratios (ORs), 95% confidence intervals (CIs), and p values from MVA for each significant variable from UVA of the overall sample, now reexamined in the overall sample while controlling for the effects of age, female sex, and lifetime diagnoses of MDD, externalizing disorders, and substance use disorders. In each model, lifetime MDD was highly significant and the strongest correlate of lifetime SB (p < .005). Other significant environmental correlates (p < .05) of lifetime SB included parent–child conflict and counts of victimization events. For quantitative composite variables like parent–child conflict, which were derived from standardized ratings, an OR of 4.3 indicates that each 1 standard deviation increment above the sample’s mean was associated with a 4.3-fold increased likelihood of lifetime SB. For other quantitative variables like victimization events, an OR of 1.5 indicates that each new victimization event type was associated with a 1.5-fold increased likelihood of lifetime SB. Among specific victimization events, exposure to family violence and being kidnapped remained significant independent correlates of lifetime SB, whereas physical abuse did not. With the exception of academic impairment, all other subtypes of impairment remained significant independent correlates of lifetime SB in these MVA models.
Predictors of Lifetime SB: MVA. a
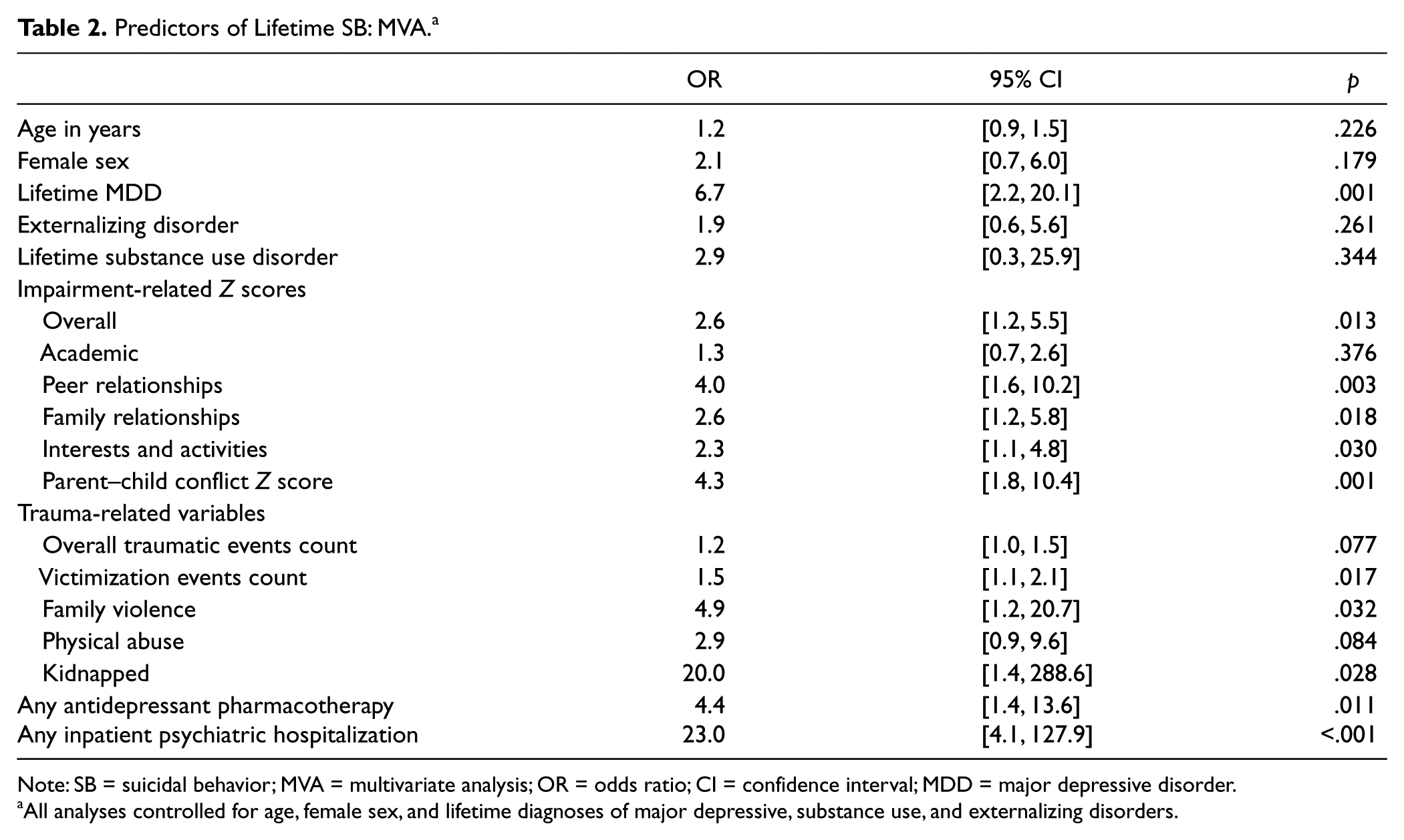
Note: SB = suicidal behavior; MVA = multivariate analysis; OR = odds ratio; CI = confidence interval; MDD = major depressive disorder.
All analyses controlled for age, female sex, and lifetime diagnoses of major depressive, substance use, and externalizing disorders.
Stepwise Regression Analysis
Table 3 summarizes the final MVA, which allowed various significant correlates of lifetime SB from UVA to enter a forward stepwise regression, to find the most parsimonious predictive model of lifetime SB in the overall sample. The final model contained lifetime MDD, along with parent–child conflict and counts of victimization trauma. This model was highly significant, χ2(3) = 44.8, p < .001, and correctly classified 81.2% of the sample regarding whether they had had lifetime SB.
Stepwise Regression Model Predicting Lifetime SB.
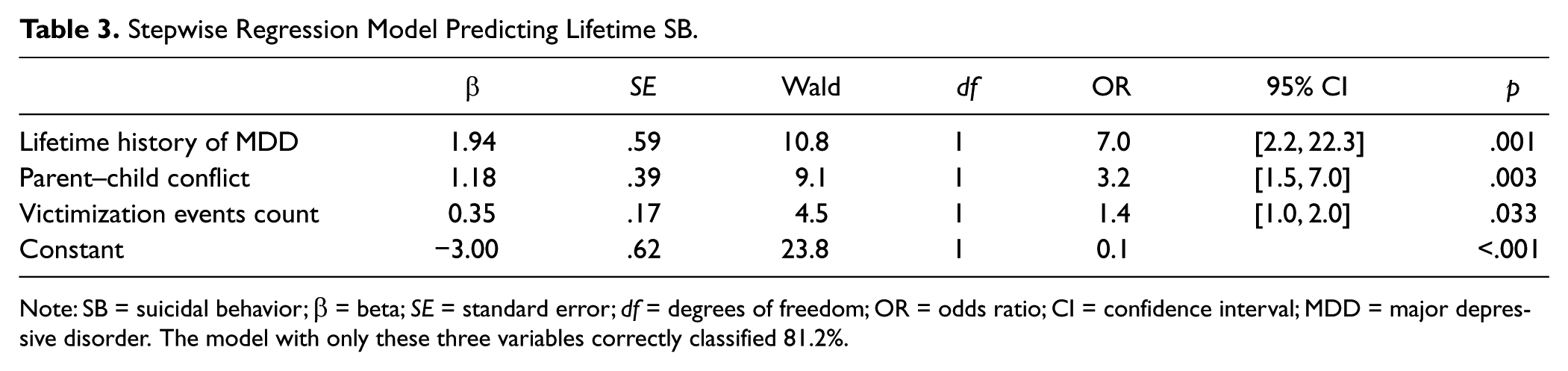
Note: SB = suicidal behavior; β = beta; SE = standard error; df = degrees of freedom; OR = odds ratio; CI = confidence interval; MDD = major depressive disorder. The model with only these three variables correctly classified 81.2%.
Discussion
The present study is the first to examine environmental factors like trauma exposure and parent–child conflict, along with variables related to ADHD severity, impairment, and comorbidity as correlates of SB in a sample of youth with ADHD. Contrary to our hypothesis, we found limited evidence that the severity of the ADHD symptoms is associated with lifetime SB in only girls. However, as hypothesized, SB was strongly associated with a lifetime major depressive, externalizing, and substance use disorders. Only lifetime MDD, however, remained a significant correlate of SB independent of these other comorbidities, age, and female sex. As hypothesized, levels of parent–child conflict, and of trauma exposure, especially victimization trauma, were also strong correlates of lifetime SB, independent of the same comorbidity and demographic covariates, as was impairment in most functional domains other than academic function. A stepwise regression model with only lifetime MDD, parent–child conflict, and counts of victimization trauma types correctly classified more than four fifths of the overall sample regarding lifetime SB. These findings suggest that adverse environmental factors at home and impaired social relationships with family and peers are also potentially important predictors of lifetime SB in youth with ADHD.
Based on findings from multiple previous studies regarding general risk factors for pediatric suicide (Bridge et al., 2006), and because SB is a symptom of depression, the fact that lifetime MDD was the single strongest correlate of lifetime SB is no surprise. Apart from MDD, however, parent–child conflict and victimization trauma were also particularly strong correlates of lifetime SB, independent of lifetime MDD and other comorbidities, and stronger correlates than other comorbid psychopathology. Our findings in this ADHD sample are consistent with other studies in general samples that have linked youth SB to parent–child conflict (Deault, 2010; Lifford et al., 2009; Rey Gex et al., 1998) and victimization trauma (Fergusson et al., 1996; Kosky et al., 1990; Resnick et al., 1997). Our study’s design, however, does not allow us to say whether such variables were a cause or an effect of lifetime SB. These variables may also simply be a marker of parental psychopathology, which has been linked to pediatric SB by other studies (Fergusson & Lynskey, 1995a; Gould, Fisher, Parides, Flory, & Shaffer, 1996). Although most individual types of victimization trauma did not occur frequently enough to be significant correlates of lifetime SB in MVA, exposure to domestic violence, kidnapping, and a wider array of victimization events were each strong independent correlates of lifetime SB. These results underscore the importance of assessing the home environment, especially for parent–child conflict and victimization trauma, when weighing the potential likelihood of lifetime SB in ADHD youth.
Based on a recent prospective study that linked early hyperactive/impulsive symptoms or the combined subtype of ADHD at a preschool age to adolescent SB (Chronis-Tuscano et al., 2010), we also hypothesized that ADHD severity regarding hyperactive-impulsive symptoms would predict lifetime SB in our sample. Although we observed significant associations in girls between lifetime SB and certain measures of hyperactive/impulsive symptoms, including errors of commission and fast RTs on the continuous performance test, as well as having the combined subtype of ADHD, we did not observe such associations in boys (who were 64% of the sample) or when examining the overall sample. Our study hints that any association between hyperactive/impulsive symptoms and lifetime SB may differ across sexes. In contrast, the study by Chronis-Tuscano and colleagues (2010) was even more predominantly male, with only 18 of the final ADHD sample of 125 (15%) being girls. This study prospectively examined ADHD severity measured during the preschool years as a predictor of subsequent SB, and did not do separate analyses by sex of such ADHD-related predictors. Such difference in these studies’ samples and designs may account for the differences in findings. As such, future studies will ideally examine the associations of hyperactive/impulsive symptoms of ADHD with subsequent SB and look for possible differences across the sexes in such associations.
Although lifetime SB was significantly associated with a limited number of measures of ADHD severity only in girls, lifetime SB was significantly associated with most areas of functional impairment in the overall sample, even after controlling for demographic and comorbidity covariates. The associations observed between SB and social impairment are consistent with studies in general samples linking SB with impaired peer relationships or social skills (Hawton & Catalan, 1987; Kienhorst et al., 1995) and impaired family relationships (Brent et al., 1994; Fergusson & Lynskey, 1995b; Gould et al., 1996; Rey Gex et al., 1998). Our findings suggest that impairment in social areas of function and general interests may be especially useful as correlates of lifetime SB in adolescents with ADHD. However, lack of association between SB and academic function contrasts with several other studies (Beautrais et al., 1996; Borowsky et al., 1999; Eggert et al., 1995; Resnick et al., 1997). Once again, differences in the sample characteristics may account for these discrepant findings regarding associations of SB with academic impairment.
The present study also examined various treatment history variables as potential correlates of lifetime SB. Although two recent studies have suggested the potential benefit of early pharmacological treatment of ADHD in reducing the long-term risk of comorbid depression (Biederman, Monuteaux, Spencer, Wilens, & Faraone, 2009; Daviss, Birmaher, Diler, & Mintz, 2008), we found no relationship between age of first ADHD treatment or exposure to any ADHD treatment and lifetime SB. However, lifetime SB was significantly associated with having had antidepressant treatment or an inpatient psychiatric hospitalization. Although black box warnings by the Food and Drug Administration have reported an increased short-term risk of suicidal ideations and SB in youth receiving antidepressants (Hammad, Laughren, & Racoosin, 2006), the associations of lifetime SB with these treatment variables are more likely explained by youth with lifetime SB being more likely to be referred for treatment with antidepressants or inpatient hospitalization (Simon, Savarino, Operskalski, & Wang, 2006). Once again, however, a cross-sectional study precludes us from determining the directional nature of such associations.
Our findings should be considered cautiously in light of several study limitations. First, we relied on retrospective reports of suicidality, prior psychiatric diagnoses, and trauma exposure, which would be more prone to rater biases and less reliable than reports obtained prospectively. Suicidal ideations and SB were determined with semistructured interviews of general psychopathology done with youth and parents, consistent with general recommendations for such assessments present at the time of the study. However, newer and more specific measures of past and present SBs have been developed with growing evidence for their validity and reliability (e.g., see Posner et al., 2011; Posner, Oquendo, Gould, Stanley, & Davies, 2007), and would have been preferable for assessing such behaviors in the current sample. Second, the lack of a prospective design prevented us from being able to establish causal relationships between SB and other variables, many of which were highly intercorrelated themselves (Daviss et al., 2009). Third, because we lacked a non-ADHD control group, we could only examine the associations of lifetime SB with ADHD severity but not with ADHD diagnosis. Fourth, having an immediate family member with a history of psychopathology (Fergusson & Lynskey, 1995a; Gould et al., 1996) or of SB (Borowsky et al., 2001; Brent & Mann, 2005) increases the risk of pediatric-aged SB, but these familial risk factors were not assessed in the present study. Fifth, we were not sufficiently powered with only 28 participants having lifetime SB to show independent associations with correlates like substance use disorders and sexual abuse, which were uncommon in our mostly male and younger adolescent-aged sample, or to test for interactive effects, which were suggested by discrepant findings across sexes regarding hyperactive-impulsive behaviors. Finally, our study’s results may not generalize to youth with ADHD in community settings, especially because we actively recruited youth with comorbid depressive disorders and excluded youth with bipolar disorders. Although we are encouraged by the results of another recent study, which suggest that correlates of morbidity among ADHD youth are consistent in clinical and community samples (Bauermeister et al., 2007), findings from the present study will need replication in other ADHD samples followed prospectively.
Even so, the present study underscores that, along with comorbid depression, factors like parent–child conflict, victimization trauma, and social impairment may be especially useful for identifying youth with ADHD likely to experience SB. Should prospective studies link such variables to subsequent SB in youth with ADHD, they could all represent modifiable risk factors of SB that could be targeted with psychosocial or pharmacological interventions in such youth.
Footnotes
Acknowledgements
In addition to our funding sources noted elsewhere, we gratefully acknowledge the help of Dr. David Brent and Dr. Boris Birmaher who served as advisors to this project, and Dr. Brent for his editorial suggestions during our preparation of this manuscript. We also thank Diane Holland and Renee’ Weinman for their help coordinating the project, Aaron Jennings and Kim Dever for their help as interviewers, and Deena Battista, Giovanna Porta, Rebecca Munnell, Ellie Kanal, and Travis Brewer for their help with data entry. We also thank our participants, and their parents and teachers for their time and contributions of data to this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In the past 2 years, Dr. Daviss has served as a consultant for Ava Cat Inc, Next Wave Pharmaceuticals, and Lexicor, and has received research support from Lexicor. Dr. Diler has had no potential conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Young Investigator’s Award from the National Alliance for Research on Schizophrenia and Depression (PI: Dr. Daviss) and by grants from the National Institute of Mental Health, including K23 MH 065375 (PI: Dr. Daviss) and P30 MH066371 (PI: Dr. Brent).