
Abstract
Introduction
A significant relationship has been found between ADHD and offending, and it is important to understand the nature of this relationship and potential treatments for this population (Young et al., 2011a). The association between ADHD symptoms and offending has been investigated by two complementary approaches. The first involves studies of clinical populations among people with ADHD (Barkley, Murphy, & Fischer, 2008) that focuses on a selective clinical group and usually consists of a more severe variant of the population that has been clinically referred to health services. The second approach takes an epidemiological perspective (Gudjonsson, Sigurdsson, Sigfusdottir, & Young, 2014) that typically focuses on large community samples and consists, by its nature, of a less severe variant of the population. Clinical and population studies have advantages and disadvantages, and both methods are important contributors to research. One of the strengths of epidemiology is that it provides the opportunity for achieving better representativeness of the general population; however, it is less able to inform about specific clinical problems and their treatments.
Longitudinal epidemiological studies suggest that hyperactivity and conduct problems in childhood contribute more to the risk of adult offending (recorded by official statistics) than family and social circumstances (Brassett-Grundy & Butler, 2004; Stevenson & Goodman, 2001). In their review of the literature, Barkley et al. (2008) argued that children with ADHD are at elevated risk of offending and substance use in adulthood, although the presence of childhood conduct disorder (CD) “greatly elevates these risks and, in some cases, accounts for them entirely” (p. 326). This proposition was investigated by Gudjonsson, Sigurdsson, Sigfusdottir, et al. (2014) in a cohort study of more than 11,000 Icelandic students in further education (age 16-24 years). They found that self-reported ratings of both non-violent and violent delinquency correlated significantly with all predictor measures (ADHD symptoms, CD, substance use, association with delinquent peers, emotional lability, anger problems, violent attitudes, and low self-esteem) with small to large effect sizes. Multiple regressions showed that after controlling for age and gender, ADHD contributed 8.2% and 8.8% to the variance in nonviolent and violent delinquency, respectively, but these effects were largely mediated by the comorbid measures, particularly substance use, association with delinquent peers, and CD. The findings suggest that it is the presence of CD and substance use that increases the risk of criminal offending in adulthood rather than ADHD acting as an independent risk factor. In particular, the regular use of heroin has been found to be significantly associated with repeated convictions for property offenses and alcohol for repeated violent offenses (Young, Wells, & Gudjonsson, 2011b).
Results from longitudinal follow-up studies are inconclusive on the relative contribution of ADHD and CD to subsequent offending. A number of studies have shown that ADHD among boys predicts adult offending independently of CD (Farrington, 1990; Sourander et al., 2006; Taylor, Chadwick, Heptinstall, & Danckaerts, 1996), especially when hyperactivity–impulsivity symptoms are sustained (Babinski, Hartsough, & Lambert, 1999). In a longitudinal follow-up study of boys with ADHD, Sibley et al. (2011) found that regardless of comorbidity, all children with ADHD are at risk of future offending, although the greatest risk was posed by those with comorbid ADHD and CD. In contrast, Satterfield et al.’s (2007) 30-year prospective study of hyperactive boys found that only those with comorbid CD were at increased risk of arrest, conviction, and imprisonment in adulthood. In a Norwegian follow-up study using official criminal records, Mordre, Groholt, Kjelsberg, Sandstad, and Myhre (2011) found no direct relationship between ADHD and later offending.
These studies have failed to account for the potential contribution of childhood emotional problems, most likely reflecting that the role of emotional problems is less researched and established than the role of ADHD and CD in later offending (Mordre et al., 2011). There is evidence that children’s early (aged 3) “undercontrolled” behavioral style (i.e., irritable, impulsive, and emotionally labile) predicts emotional problems at age 26 (Caspi et al., 2003). Emotional lability at age 16 (defined by a high “neuroticism” score on the Eysenck Personality Inventory) has been found to be predictive of later offending (Farrington, Ttofi, & Coid, 2009). Gudjonsson, Sigurdsson, Young, Newton, and Peersen (2009) found among adult prisoners that neuroticism was a better predictor of adult ADHD symptoms than antisocial personality traits. They proposed that the key link with offending may be that neuroticism exacerbates existing propensities for poor behavioral inhibition among people with ADHD. This is consistent with the theory of Retz and Rosler (2009) that differentiates between reactive–affective and proactive types of delinquent and violent behaviors in offenders with ADHD. In this model, reactive–affective violence is characterized by unplanned, spontaneous acts and driven by impulsivity and emotion. Proactive offenses, by contrast, tend to be more premeditated acts that are most associated with antisocial traits.
This study aimed to investigate the relative relationship between childhood hyperactivity, emotional, and conduct problems, and adult criminal offending by reanalyzing data that previously reported an epidemiological follow-up of boys identified in childhood with these characteristics (Taylor et al.,1996; Taylor, Sandberg, Thorley, & Giles, 1991) and examining their official criminal records 19 years later. This study contributes to the literature above and beyond the findings of Gudjonsson, Sigurdsson, Sigfusdottir, et al. (2014) in two respects; first, it is a prospective rather than a cross-sectional study, and second, criminal offending was obtained from official conviction records rather than self-report. We investigated which of the three predictors (hyperactivity, emotional, and conduct problems) best predicted general criminal offending at outcome (i.e., any conviction) and violent and nonviolent convictions. Given that CD is reported to be more directly related to offending than hyperactivity (Fergusson, Horwood, & Lynsky, 1993; Lynam, 1996), our first hypothesis was that childhood conduct problems would be the best overall predictor of general criminal offending with hyperactivity having little independent effect. Consistent with the theoretical framework of Retz and Rosler (2010) and the empirical findings of Gudjonsson et al. (2009), the second hypothesis was that emotional problems would contribute relatively more to violent than nonviolent criminal offending due to its association with poor behavioral control.
Method
This study involves a secondary analysis of data previously collected to investigate the long-term risk of childhood hyperactivity and conduct problems (Taylor et al., 1991, 1996). In the original study, the cases were stratified into five groups (hyperactivity and conduct problems co-occurring, pure hyperactivity, pure conduct problems, inattentive without hyperactivity, and controls) and the participants in these five groups were followed up 19 years later. For the purpose of the present article, the five groups from the original study were combined into one large group to maximize power and the analysis relied on the continuous scores from the Rutter A(2) parent questionnaire and the Rutter B(2) teacher questionnaire. The original survey and current follow-up are outlined below.
The Original Survey
Participants
The original survey, from which all the subjects were taken, has been previously described (Taylor et al., 1991). As a brief summary, the participants included all 6- and 7-year-old boys (3,215 boys), on the registers of mainstream schools in the London Borough of Newham, with the schools for severely learning disabled children excluded.
Measures
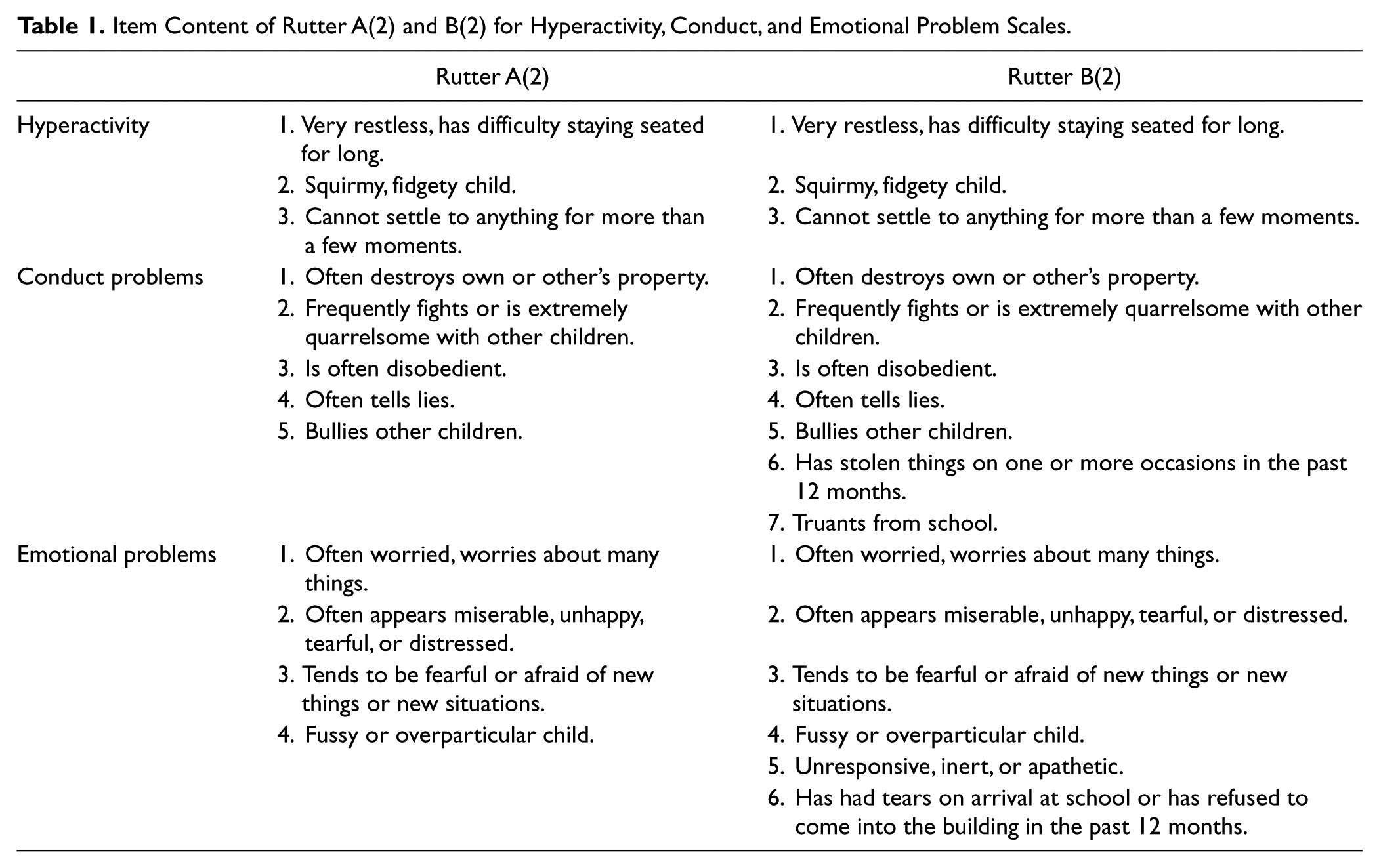
The Rutter A(2) parent questionnaire and the Rutter B(2) teacher questionnaire assess hyperactivity, conduct, and emotional problems, each item on a 3-point scale (doesn’t apply, applies somewhat, and certainly applied) rated 0, 1, or 2, respectively (see Table 1). These subscales have been validated against standardized interview measures and psychiatric diagnosis in previous surveys and on the Isle of Wight studies (see Rutter, Tizard, Yule, Graham, & Whitmore, 1976; Schachar, Rutter, & Smith, 1981). Furthermore, they have been found to identify different subgroups with good predictive and discriminative validity (Schachar et al., 1981). In the present study, for the Parent scale, the Cronbach’s alpha was .81 for hyperactivity, .73 for conduct problems, and .62 for emotional problems. For the Teacher scale, the Cronbach’s alpha was .81 for hyperactivity, .81 for conduct problems, and .65 for emotional problems.
Item Content of Rutter A(2) and B(2) for Hyperactivity, Conduct, and Emotional Problem Scales.
Procedure
The Rutter A(2) questionnaire was completed for 80% (n = 2,572) of the children by their parents and the B(2) questionnaire for 99% (n = 3,183) by their class teachers. In total, 2,462 children had both screening questionnaires completed.
In the original design of the study, which followed the then understanding of ADHD, the groups selected for detailed study were those with scores above cutoff for CD who also met criteria for pervasive hyperactivity (mixed, constituting 5.3% of the study population), those who met criteria for pervasive hyperactivity but not for conduct problems (hyperactive, amounting to 3.7%), those who met criteria for conduct problems but not for pervasive hyperactivity (conduct problem, amounting to 14%), those who showed inattentiveness but no hyperactivity (inattentive, amounting to 1.3%), and those not meeting criteria for either condition (control). Because the original study investigated the long-term risk of childhood hyperactivity and conduct problems (Taylor et al., 1991, 1996), participants were excluded at this stage if they had scores of 5 or greater on the Emotional Disorder subscale of either the Parent or Teacher scale as it was intended to obtain “purer” measures of childhood hyperactivity and conduct problems that were not contaminated by severe emotional problems.
The cases were stratified by behavioral group and then randomly sampled from the resulting groups, to give approximately equal numbers in each group for detailed study. The selected boys were traced through the schools and, after giving consent, 194 participated in the second-stage measures (parental interview, test, and observational measures) administered 9 months after the initial screening (Taylor et al., 1987). At this time, consent was also given for future follow-up of Ministry of Justice records for 182 participants.
The measures used in the current (follow-up) study for association with the Rutter A(2) and B(2) criminal records were the Continuous Hyperactivity, Emotional Problem, and Conduct Problem scales (rather than the Categorical Stratification). Data from the Parent and Teacher scales were aggregated on each of the three domains.
The Follow-Up Study
Participants
All 182 second-stage participants who consented to future follow-up of Ministry of Justice records were selected.
Procedure
The follow-up for the present study was made 19 years later (i.e., participants were 25-27 years old) when official records of conviction data were requested from the Ministry of Justice who were able to provide 173 records (95%). No reason was given for the 9 records that could not be located.
Outcome measure
The Ministry of Justice Offenders Index provided official records on conviction history (i.e., the number, type, and date of convictions) after reaching the age of criminal responsibility (i.e., age 10 years or older). For analysis, we classified conviction history into three categories: (a) any conviction (i.e., total of violent and nonviolent convictions), (b) violent convictions (e.g., violence against a person, sexual offenses), and (c) nonviolent convictions (e.g., theft, burglary, robbery, receiving stolen goods, criminal damage).
Statistical analysis
For the purpose of the present study, parent and teacher ratings were aggregated for each of the three Rutter scales. Multivariate Analysis of Variance (MANOVA) was used to measure overall group differences on the three dependent measures (i.e., conduct problems, hyperactivity, and emotional problems). Its advantage is that it takes account of the correlations between the dependent variables and provides information on how much the three variables combined differentiate between the participants with and without conviction at follow-up. Those with conviction at follow-up versus those without a conviction were used as a “fixed” (categorical) factor. The MANOVAs were followed up with univariate (t tests) analyses, and group effect sizes were determined using Cohen’s (1992) recommendations for t tests between groups (Cohen’s d: 30 = low, .50 = medium, .80 = large). A discriminant function analysis (stepwise) was conducted for the conviction outcome measures to find the linear combinations of the dependent variables that best discriminated between the criminal offense groups.
Results
Out of the 173 boys, 43 (25%) had one or more criminal convictions (M = 1.84, SD = 5.8, range = 0-44) with 31 (18%) having more than one conviction. Out of the 43 participants with a conviction, 20 (47%, 11.5% of the total sample) had a conviction for an act of violence, 16 of whom (37%, 9% of the total sample) also had a conviction for at least one other violent criminal offense. For those boys with a conviction, the mean age at the time of first conviction was 17.5 years (SD = 2.3, range = 13-23 years).
MANOVA showed a main effect of group differences for total convictions—Pillai’s Trace: F(1, 171) = 3.1, p < .05, η2 = 0.052—and violent convictions—Pillai’s Trace: F(1, 171) = 6.0, p < .001, η2 = 0.096. There was no main effect for nonviolent convictions, Pillai’s Trace: F(1, 171) = 0.91, ns.
In view of the nonsignificant MANOVA for nonviolent convictions, univariate analyses (t tests) were conducted for total convictions (n = 43 vs. 130) and violent convictions (n = 20 vs. 153) only. The data are presented in Table 2. With regard to total convictions, only conduct problems significantly discriminated between the two groups, with a small effect size. For violent convictions, all three predictors significantly discriminated between the two groups (one-tailed tests); the effect sizes were moderate for emotional problems and low for conduct problems and hyperactivity.
Mean Scores, t-Value, and Effect Size on the Three Rating Scales for Those With Conviction and No Conviction, Grouped Into Total Convictions and Violent Convictions.

p < .05. **p < .001.
A discriminant function analysis showed that for total convictions, only conduct problems significantly discriminated between the two groups (Wilks’s Lambda = 0.969, χ2 [1] = 5.3, p < .05) with 76.3% of the grouped cases being correctly classified.
For violent convictions, only emotional and conduct problems discriminated significantly between the two groups (Wilks’s Lambda = 0.908, χ2 [2] = 16.4, p < .001) with 90.1% of the grouped cases being correctly classified. The respective statistics were emotional problems, Wilks’s Lambda = 0.937, F(1, 170) = 11.4, p < .001, Standardized Canonical Discriminant Function Coefficient = 0.90, and conduct problems, Wilks’s Lambda = 0.908, F(1, 169) = 8.8, p < .001, Standardized Canonical Discriminant Function Coefficient = 0.59.
Spearman’s rho correlation showed no significant relationship between the three predictors and age at first conviction.
Discussion
The purpose of the present study was to investigate the relative contribution of childhood hyperactivity, conduct, and emotional problems in predicting convictions obtained from the Ministry of Justice official records. The official statistics showed that one quarter of the sample had a criminal conviction at follow-up 19 years later, many of whom were repeatedly offending. This is generally consistent with official statistics showing 28% of 21- to 45-year-old males have at least one conviction (Budd, Sharp, & Mayhew, 2005).
Significant main effects were found for total and violent convictions, the strongest being for violent convictions. As hypothesized, conduct problems significantly predicted a criminal conviction (irrespective of type of criminal offense). By contrast, emotional problems, followed by conduct problems, predicted violent convictions. Hyperactivity was not a significant predictor in the models. Univariate analysis showed that emotional problems have a medium effect size on violent convictions, whereas the effect size for conduct problems was small.
The results indicate that the risk of children with hyperactivity for developing criminal convictions is predicted by their associated conduct and emotional problems rather than by their level of hyperactivity, which is consistent with the findings of the longitudinal studies of Satterfield et al. (2007) and Mordre et al. (2011). Early conduct problems are clearly a salient predictor of a future conviction either independently or in conjunction with hyperactivity. The most likely mechanism is through the development of antisocial personality disorder (Lynam, 1996; Retz & Rosler, 2009), substance misuse (Young et al., 2011b; Young, Misch, Collins, & Gudjonsson, 2011c), and associations with delinquent peers (Farrington et al., 2009; Gudjonsson, Sigurdsson, Sigfusdottir, et al., 2014). However, we acknowledge that we had no direct measure of antisocial personality disorder in the current study.
There was a marked difference among the predictors between a conviction for violence and conviction for any criminal offense. It was hypothesized that emotional problems would more strongly relate to violent criminal offending than general offending, and this was supported. This is consistent with the findings of Gudjonsson, Sigurdsson, Adalssteinsson and Young (2013) who showed that mood instability was a stronger incremental predictor of self-reported “reactive” offending in adolescents beyond antisocial personality traits and ADHD symptoms. By comparison, antisocial personality traits were the single most powerful predictor of self-reported general offending. In the Gudjonsson, Sigurdsson, Adalssteinsson, et al. (2013) study, entering mood instability into the regression had no significant incremental effect, whereas entering antisocial personality traits mediated almost half of the effect of ADHD symptoms on general offending.
What had not been anticipated was that the effects of emotional problems were considerably stronger than those of conduct and hyperactivity. The finding is striking given that participants with serious emotional problems had been excluded from the baseline survey suggesting that the influential factor may be an emotional vulnerability to environmental adversity, such as stress, rather than clinical symptoms of anxiety and depression. The findings suggest that early childhood emotional problems, even when below threshold for emotional disorder, may be a risk for mood instability in adolescence and young adulthood perhaps due to a reactive and explosive temperament. Neuroticism, which is conceptually linked to emotional problems (Eysenck & Eysenck, 1975), has been shown to develop into a stable personality trait into adulthood (Caspi et al., 2003), informs on person–context interactions in everyday life in terms of negative affect and sensitivity to stress (Jacobs et al., 2011). This may present as poor behavioral control in violent criminal offenders, and future studies need to investigate how emotional problems in early childhood moderate feelings of anger, violent cognitions, and poor behavioral control. Indeed, the development of violent cognitions is particularly pertinent to violent behavior (Unnever, Cullen, & Pratt, 2003).
It is noteworthy that in the current study, 80% of those with a conviction for violence also had a conviction for a nonviolent criminal offense. This group of criminal offenders is therefore likely to be the more serious and persistent offenders, which is reflected in the relatively larger amount of variance in violent versus nonviolent convictions explained by the three predictor variables than by conviction of any type (i.e., offending vs. nonoffending). Those with poor behavioral control may be predisposed to engaging in unplanned, opportunistic criminal activity (Young et al., 2011a), institutional aggression (Young et al., 2011c; 2009), substance misuse (Gudjonsson et al., 2012b; Young et al., 2011b; 2011c), and motivation to engage in offending when feeling provoked (Gudjonsson, Wells, & Young, 2011). In addition, poor behavioral control is also likely to affect their capacity to engage effectively with the criminal justice process, including police interrogation (Gudjonsson, Sigurdsson, Einarsson, Bragason, & Newton, 2008; Gudjonsson, Sigurdsson, Sigfusdottir, & Young, 2012a; Gudjonsson, Young, & Bramham, 2007) and the trial process (Gudjonsson & Young, 2006).
Data on treatment history during the intervening years were not available from the records of offending. At that time in England, conditions such as ADHD were seldom recognized as such, and in particular, stimulant drugs such as methylphenidate were very rarely used. Indeed, a self-report study on a subset of the participants indicated that none had received medication for ADHD (Moyá, Stringaris, Asherson, Sandberg, & Taylor, 2014). From this perspective, therefore, our results contribute to the natural history of the problem. It is possible that effective treatment could have improved the outcome—although there is evidence that pharmacological treatment for ADHD does not necessarily reduce the risk of future antisocial behavior and offending (Langley et al., 2010). If, however, the young people in this study had been treated effectively for ADHD, then this could have explained the lack of prediction from hyperactive behaviors. It is not likely that such an explanation applies.
More intensive and multimodal treatments for childhood ADHD, including psychological interventions, are needed; stimulants alone are probably insufficient to reduce offending. Indeed, combined treatment approaches may be a more effective intervention as treatment effect sizes have been shown to be greater when both pharmacological and cognitive behavioral treatments are provided (Emilsson et al., 2011).
The current study’s main strength is that it was a prospective epidemiological study. The participants were assessed in early childhood and followed up 19 years later using official criminal records obtained from the Ministry of Justice. The results are not influenced by medication for ADHD. The limitations are as follows: First, that the study is not based on an ADHD diagnosis but on behaviors determined by rating scales. Second, children with serious emotional problems were excluded from the original survey, which may have reduced the power of the current findings, and the current results should not be generalized to children with clinical anxiety or depression. Third, the children were not identified by rigorous or objective measures of inattention in childhood (i.e., the focus was primarily on ratings of behavior). Fourth, the sample followed up for criminal record check was small (n = 173), and the number of people with a conviction was small (n = 43). Hence, the further breakdown by conviction type, which was necessary to meet the aims of the article, reduced power and may have resulted in some nonsignificant results. Fifth, the records did not include data regarding possible mediating influences on the participants in the intervening years such as their substance use or personality disorder, which means we were unable to examine the potential influence of these factors at outcome. In spite of these limitations, the findings further our knowledge about the developmental mechanisms that mediate criminal behavior by showing that symptoms of emotional problems in early childhood contribute to the risk of violent criminal offending independent of conduct problems and hyperactivity. This is a novel finding that requires further research.
Footnotes
Acknowledgements
This research was supported by the Medical Research Council (Reference G9900839), initially as a project grant and later as part of the work of its Child Psychiatry Unit and Centre for Genetic, Social and Developmental Psychiatry. We are grateful to colleagues involved in the initial survey—Professor M. Rutter, Dr. S. Sandberg, Dr. G. Thorley, and Ms. S. Giles. Thanks also to participants and their families, and the schools and Education Department in Newham.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Susan Young has received speaker fees and travel honoraria from Janssen, Eli-Lilly, Shire, Novatis, and Flynn-Pharma, and received research grants from Janssen, Eli-Lilly, and Shire. Gisli Gudjonsson has received speakers fees and travel honoraria from Janssen, Eli-Lilly, and Shire. Eric Taylor has none.
Author Biographies
![]() ).
).