
Abstract
Keywords
Introduction
ADHD in childhood has been shown to confer significantly increased risk for alcohol and other drug (AOD) use disorders in adolescence and young adulthood (Baker, Prevatt, & Proctor, 2012; Biederman et al., 2006; Biederman et al., 2010; Wilens et al., 2011; Wilens & Morrison, 2011). A recent meta-analysis showed that children with ADHD are 2.5 times more likely than children without ADHD to develop AOD use disorders (Lee, Humphreys, Flory, Liu, & Glass, 2011). Moreover, despite evidence to the contrary (Biederman et al., 2008; Biederman, Wilens, Mick, Spencer, & Faraone, 1999; Wilens, Faraone, Biederman, & Gunawardene, 2003; Winters et al., 2011), concerns remain that stimulant class medications for ADHD may further elevate this risk (Volkow & Swanson, 2008).
These theoretical concerns are derived from preclinical studies suggesting that exposure to stimulants during adolescence increases their reinforcing effects via a rise in dopamine concentration in the nucleus accumbens (Volkow & Swanson, 2008). Likewise, epidemiological data suggest that early exposure to substances with abuse potential may increase the risk of drug abuse and dependence in adulthood (Volkow & Swanson, 2008). Although the available clinical literature suggests that treatment with therapeutic oral doses of stimulants for ADHD does not increase the risk for addictive disorders (Biederman et al., 1999; Biederman et al., 2008; Mannuzza et al., 2008; Tamm et al., 2013; Wilens et al., 2003; Winters et al., 2011), these studies have largely been retrospective in nature, and almost exclusively focused on the development of full clinical abuse or dependence. Considering that the first step in the development of AOD use disorders is initiation of use, more work is needed to assess whether stimulants mitigate drug and alcohol use.
To the best of our knowledge, there has been only one small, prospective study by Donovan and Levin (2011) that examined the impact of the stimulant lisdexamfetamine (LDX) on alcohol and drug use in a small sample of ADHD youth (n = 13, M age = 14 years) at high risk for addictive disorders by having an older sibling with a substance use disorder (SUD). During a period of 6 months of open LDX treatment, 3/13 participants became intermittent users of alcohol or marijuana.
Given the detrimental impact of drug and alcohol addiction on a teen’s health and functioning, as well as the profound impact on his or her lifetime morbidity and mortality (Centers for Disease Control and Prevention, 2012; Department of Health and Human Services Publication, 1999), efforts at preventing the development of addictive disorder are of very high clinical and scientific importance and a top public health priority in this country (Healthy People 2020 Objectives, 2012; National Institute on Drug Abuse [NIDA], 2012b). Prevention of addictive disorders is particularly relevant in the context of stimulant treatment for ADHD, considering the high prevalence of ADHD, and the fact that ADHD significantly increases the risks for addictive disorders. Efforts at mitigating the development of ADHD-associated addictive disorders are highly consistent with the aims set forth by the NIDA to intervene early and to target risk factors (NIDA, 2012a; Volkow & Swanson, 2008).
Therefore, the main aim of the present study was to prospectively assess the effects of systematically deployed and monitored long-term stimulant treatment on AOD use disorders in adolescents with ADHD. This report is a secondary analysis, using data from a prospective open-label 24-month treatment study of osmotic-release methylphenidate (OROS MPH) in a large sample of adolescents with Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) ADHD, ascertained for a study on the prevention of smoking. Given lack of placebo control, for comparison purposes, we used a sample of similar age and sex youth with and without ADHD derived from ongoing studies in our program with available information on alcohol and drug use. We hypothesized that treatment with OROS MPH would mitigate the use of alcohol and drugs in youth with ADHD. To the best of our knowledge, this is the largest systematic prospective evaluation of stimulant treatment on alcohol and drug use in youth with ADHD.
Method
Participants
Clinical trial participants
The clinical trial was approved by local Institutional Review Board, and registered with ClinicalTrials.gov (NCT00181714). Informed consent was ascertained from parent(s) or guardian(s) and assent from each adolescent. Participants were compensated for study visits completed. Participants were active from 2004 to 2011.
Clinical trial participants were 12 to 17 years old, with ADHD according to DSM-IV by clinical interview with a study child psychiatrist with expertise in ADHD. Participants with any clinically significant or unstable medical or psychiatric condition by psychiatric interview were excluded, including active non-nicotine substance use disorders. Medication (OROS MPH) was prescribed under open-label conditions at weekly office visits for 6 weeks and at monthly office visits thereafter for up to 24 months. OROS MPH was clinically adjusted according to tolerability and efficacy (maximum 1.5 mg/kg/day, 126 mg/day) based on physician interview of the participant and his or her parent/guardian. Medication compliance was systematically monitored by pill count at every study visit.
Of 203 participants who signed consent, 22 participants were found to be ineligible due to insufficient criteria for ADHD, prior methylphenidate nonresponse, or current psychiatric/medical comorbidities, including 7 participants with active substance use (primarily marijuana). An additional 27 participants withdrew consent or were lost to follow up. Of 154 participants who began study medication, 39 participants did not have the outcome measure of interest (Drug Use Screening Inventory [DUSI]) at and after Week 10 (i.e., first monthly assessment), due to loss of interest/compliance (n = 19), adverse effects (n = 18), and lack of response (n = 2). Data for this analysis were derived from the remaining (n = 115) study participants.
Mean OROS-MPH exposure for the sample (n = 115) was 13 months (endpoint), and the mean OROS-MPH dose at endpoint was 64.6 ± 25.4 mg/day (1.02 ± 0.33 mg/kg/day). Clinician rated ADHD–Rating Scale (ADHD-RS) score at baseline (27.2 &0x002B; 10.0) significantly decreased to a mean score of 9.3 ± 7.8 at endpoint, t(114) = 17.76, p < .001. There were no serious adverse effects related to the study medication, including in participants who discontinued early due to adverse effects. Adverse effects for study participants were consistent with the well-documented adverse effects profile of OROS MPH (e.g., low appetite, headache, insomnia); detailed information on adverse effects is available on request.
Comparator participants
Comparator participants were derived from opportunistic samples of youth of similar age and sex with and without ADHD for our research program who completed the same assessment instrument (DUSI, see below) examining alcohol and drug use. Comparators were derived from naturalistic study, and therefore they were not subject to screening criteria as occurs in a clinical trial (i.e., to screen out active substance use disorder or significant medical condition to enter a clinical trial). Given this, we controlled for potential confounders such as psychiatric comorbidities using multivariate logistic regression. ADHD comparators were stratified based on whether they were currently on medication (n = 18) or not (n = 26).
Alcohol and Substance Use Assessments
Alcohol and illicit drug use was based on youth self-report using modified versions of the DUSI–Revised (DUSI-R; Tarter, Kirisci, & Mezzich, 1996), given to participants at every study visit. The DUSI-R is a multidimensional self-report instrument, developed to quantify drugs and alcohol use and commonly associated health, psychiatric, and psychosocial problems (Kirisci, Mezzich, & Tarter, 1995). Rates of alcohol and substance use were derived from the question: “How many times have you used x in the last month?” Participants were asked about use of alcohol as well as illicit drugs, including cocaine, marijuana, stimulants, hallucinogenics, benzodiazepines, opiates, and inhalants. We also conducted urine toxicology screens at every study visit for clinical participants only, using a multidrug test for Cocaine, Amphetamine, Methamphetamine, Marijuana (THC), Methadone, Morphine, Phencyclidine, Barbiturate, Benzodiazepine, and Tricyclics (MultiDrugTests.Com Rapid Detect, Inc., Poteau, Oklahoma).
Data Analysis and Statistics
Our primary hypothesis was that OROS-MPH treatment would be associated with a low rate of alcohol and illicit drug use in clinical trial participants as compared with untreated ADHD comparators. Clinical trial participants included in this analysis are those with DUSI-R completed at Week 10 (i.e., first monthly assessment) and after (n = 115), with the last observation carried forward (LOCF) for participants who did not complete the full study schedule of 24 months. The prevalence of alcohol and substance use in the past year was compared between the clinical trial sample and the historical comparison samples of youth with and without ADHD using Pearson’s chi-square test. While Pearson’s chi-square is calculated with frequencies, percentages are presented as a standardized way to compare groups and as estimates of the larger populations. We controlled for potential confounders such as psychiatric comorbidities using multivariate exact logistic regression (e.g., a binary outcome marijuana use predicted by group status and bipolar disorder). Exact logistic regression was used because zero cells precluded the use of standard logistic regression.
In addition, McNemar’s chi-square test was used to compare alcohol and substance use at the 10-week assessment and endpoint for clinical trial participants (n = 112). While a clinical assessment and a negative urine toxicology screen at study entry were indicative of no active substance use disorder, participants could have a positive finding at the 10-week assessment (per DUSI-R, per urine toxicology).
Results
Characteristics of the Sample
As shown in Table 1, the majority of clinical trial and comparator participants were male, in midadolescence. Mean age, gender frequency, and IQ did not meaningfully differ between the groups (Table 1) nor did race or socioeconomic status (SES; all ps > .10). Rates of oppositional defiant disorder (ODD) were significantly higher in all ADHD groups compared with the non-ADHD comparators (p < .001). In addition, the two comparison ADHD groups had significantly more bipolar disorder than the clinical trial ADHD participants (p = .03), yet absolute numbers of bipolar disorder cases were limited. There were no other statistically significant differences in psychiatric comorbidities, including conduct disorder, major depressive disorder, and multiple anxiety disorders.
Characteristics: Clinical Trial Participants and Historical Comparators.
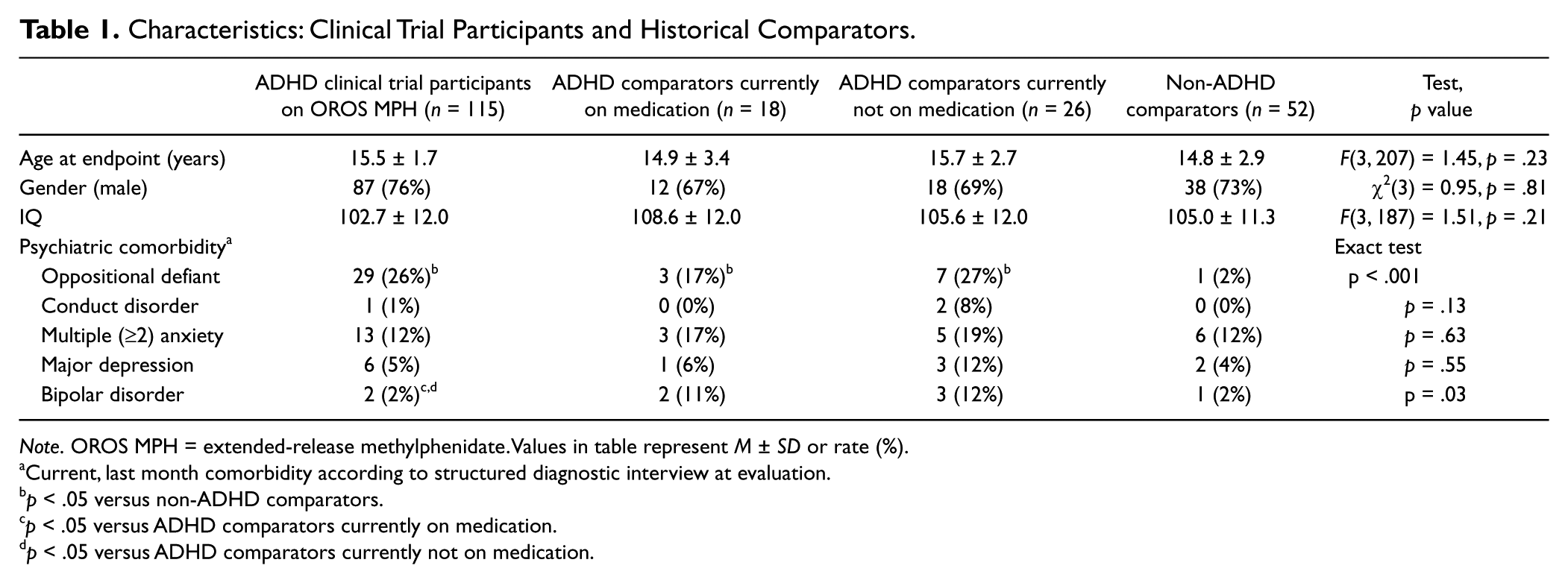
Note. OROS MPH = extended-release methylphenidate. Values in table represent M ± SD or rate (%).
Current, last month comorbidity according to structured diagnostic interview at evaluation.
p < .05 versus non-ADHD comparators.
p < .05 versus ADHD comparators currently on medication.
p < .05 versus ADHD comparators currently not on medication.
Alcohol and Substance Use Outcomes: Clinical Trial Participants Versus Comparators
As can be seen in Figures 1 to 3, results of Pearson’s chi-square tests showed that rates of alcohol, marijuana, and other drug use in the past year (per the DUSI-R) were significantly lower in the clinical trial OROS-MPH group as compared with the two ADHD comparator groups. There were no statistically significant differences in alcohol, marijuana, and other drug use between the OROS-MPH group and the non-ADHD comparators. All findings remained statistically significant after controlling for bipolar disorder using exact logistic regression (alcohol: p = .02 for OROS-MPH vs. ADHD current meds and p = .004 for OROS-MPH vs. ADHD not current meds, marijuana: p < .001 for OROS-MPH vs. ADHD current meds and p = .002 for OROS-MPH vs. ADHD not current meds, and other drugs: p = .03 for OROS-MPH vs. ADHD current meds and p < .001 for OROS-MPH vs. ADHD not current meds).
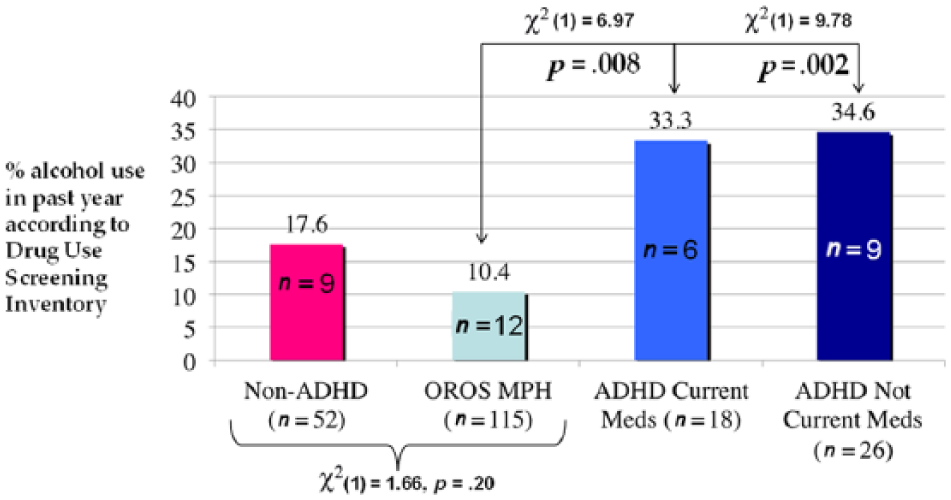
Rates of alcohol use in past year.
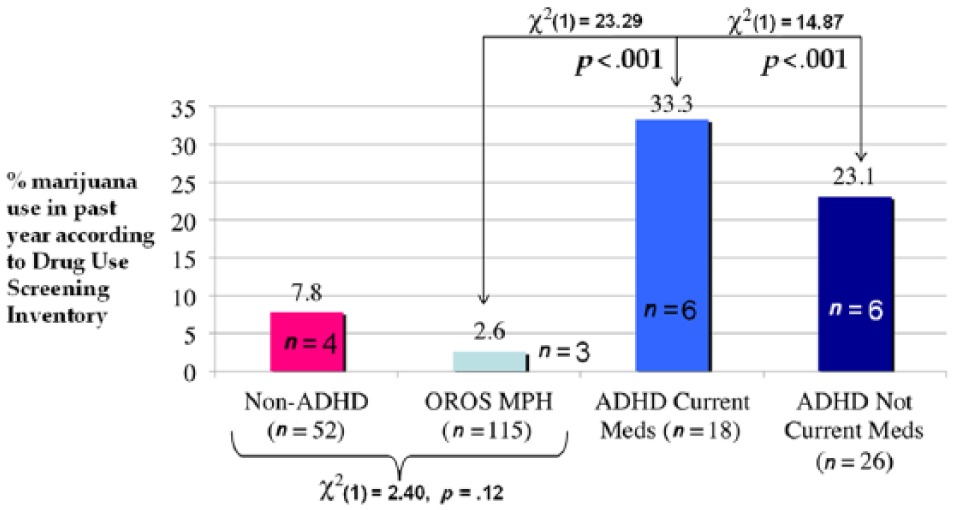
Rates of marijuana use in past year.
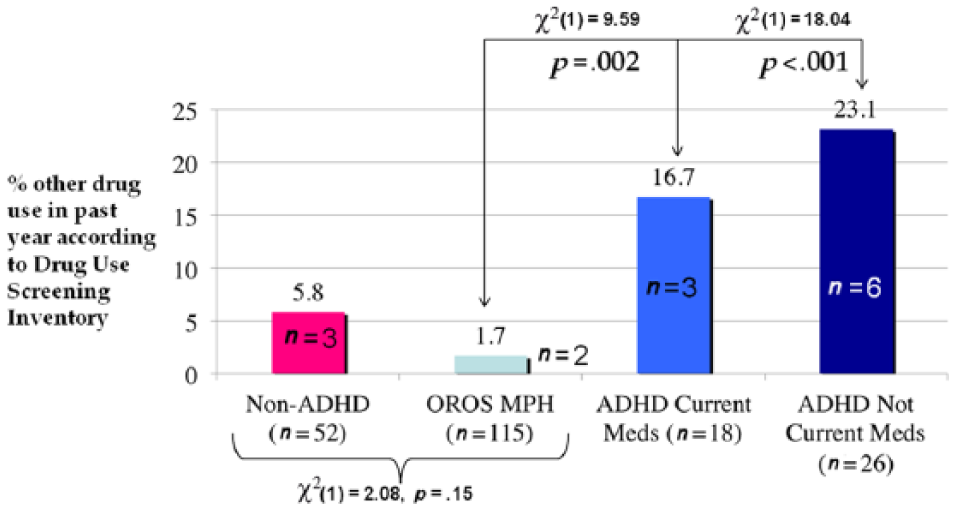
Rates of other drug use in past year.
Alcohol and Substance Use Outcomes in Clinical Trial Participants
As shown in Table 2, the rate of alcohol, marijuana, and other drug use in clinical trial participants was low at Week 10 and at study endpoint (M = 13 months OROS MPH). The difference in marijuana use reached statistical significance (p = .046). Similar low rates of substance use were observed in urine toxicology data for clinical trial participants (Table 3).
Alcohol and Drug Self-Reported Use in OROS-MPH Participants.
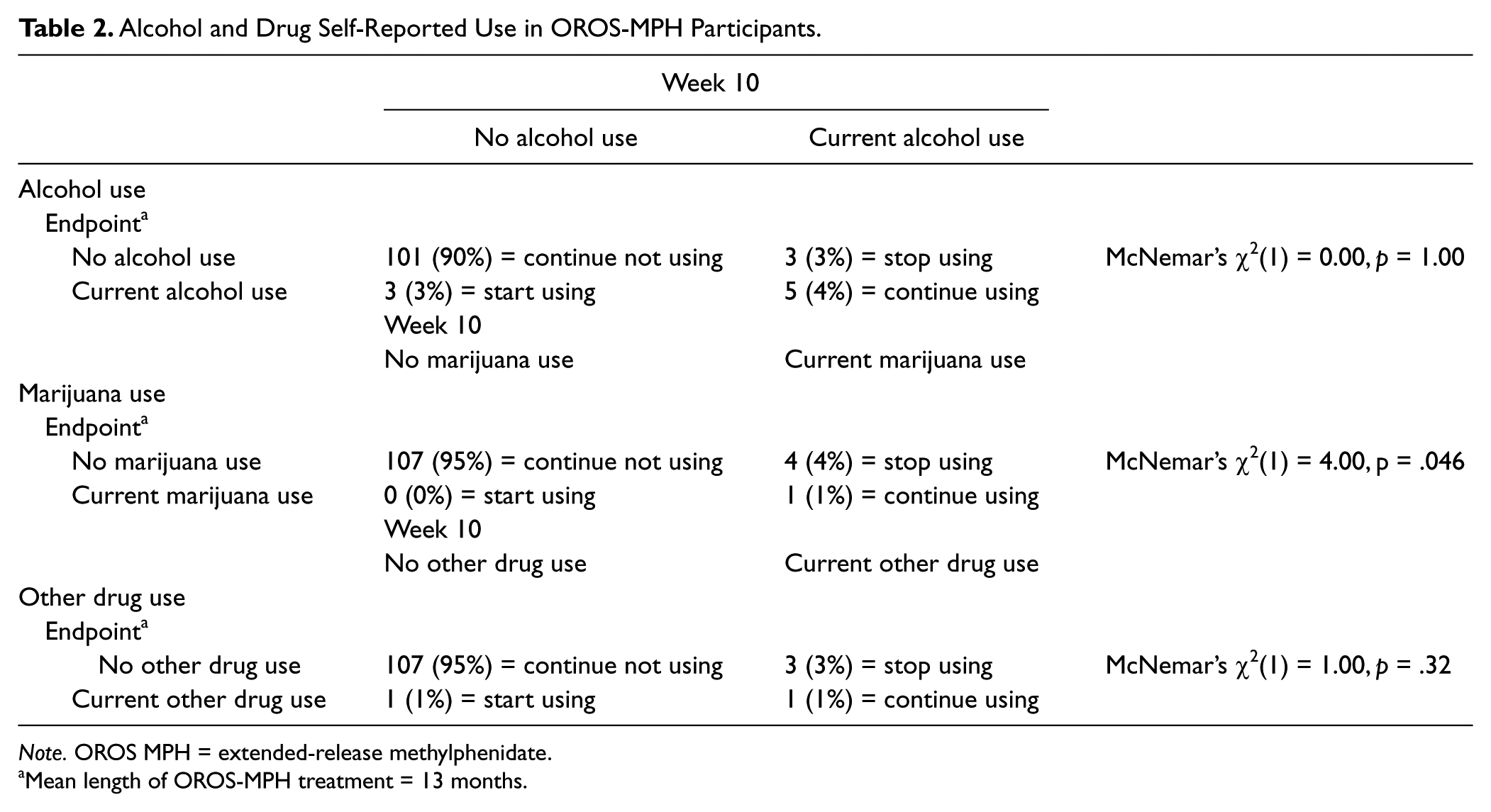
Note. OROS MPH = extended-release methylphenidate.
Mean length of OROS-MPH treatment = 13 months.
Urine Toxicology in OROS-MPH Participants.
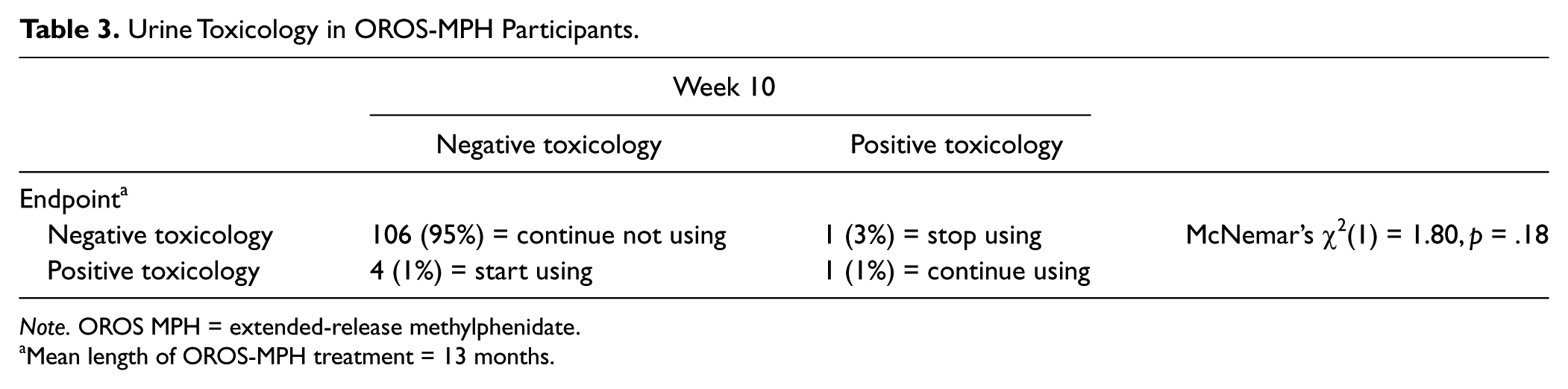
Note. OROS MPH = extended-release methylphenidate.
Mean length of OROS-MPH treatment = 13 months.
Discussion
This study assessed the effect of treatment with OROS MPH on alcohol and illicit drug use in a large sample of adolescents with ADHD. In this secondary analysis, long-term, systematically administered OROS-MPH treatment (M = 13 months) at robust dosing (M = 1.02 ± 0.33 mg/kg/day) was associated with rates of AOD use that were significantly lower than those observed in a historical sample of untreated ADHD comparators and indistinguishable from those in non-ADHD comparators. However, given methodological limitations, no definitive conclusions may be drawn.
These prospective results expand the available literature from retrospective naturalistic studies, which have shown that treatment with therapeutic oral doses of stimulants for ADHD mitigates the risk of the development of full clinical abuse or dependence of drugs and alcohol (Biederman et al., 1999; Biederman et al., 2008; Mannuzza et al., 2008; Wilens et al., 2003). These results seem to suggest that well-monitored, robust stimulant treatment, as occurred in the clinical trial, may be critical for stimulants’ protective effects on alcohol and drug use in youth with ADHD as low rates of alcohol and drug use were not similarly observed in naturalistically treated ADHD comparators. However, numerous other factors may be responsible for differences observed between these groups.
Considering that drug and alcohol use is the first step toward the development of AOD use disorders, any impact on the early stages of the path toward development of addictions in ADHD youth is of high clinical and public health significance. This is particularly so considering that ADHD confers an increased risk of initiation and experimentation with alcohol and illicit drugs, even when controlling for comorbid conduct disorder (Elkins, McGue, & Iacono, 2007; Malone, Van Eck, Flory, & Lamis, 2010). In a recent report, Malone et al. (2010) suggested that untreated ADHD results in accumulating risk of alcohol and drug use across childhood, magnifying other processes associated with onset of drug use. Lee et al.’s (2011) meta-analysis, which included the Elkins et al. (2007) study, suggested that childhood ADHD confers a significant increase in the odds of ever having used nicotine or illicit drugs, an association impervious to demographic and methodological factors.
Although the reasons why well-monitored, robust stimulant treatment in adolescents with ADHD may reduce alcohol and drug use are not entirely clear, several plausible explanations can be offered. It is possible to hypothesize that protective effects against alcohol and drug use could be due to the clinical improvement of ADHD symptoms (e.g., reduced impulsivity or novelty seeking) with attendant functional improvements (e.g., improved school engagement, quality of social relationships). It is also possible that stimulant treatment may reduce unhealthy attempts at self-medication. More work is needed to examine the mechanisms by which stimulant treatment may exert a protective effect on the early stages of drug and alcohol use in youth with ADHD, and whether these putative mechanisms vary per subtype.
Strengths of this present study include the long-term, prospective, systematic monitoring of a large cohort of adolescents with ADHD entering the clinical trial within the typical window of alcohol and drug initiation. The main limitation of this study stems from its uncontrolled, open-label design involving prescreened ADHD youth without substance use disorders. Thus, we cannot assert a causal relationship between low rates of alcohol and drug use in the screened clinical trial participants and OROS-MPH treatment. Our findings may reflect an atypical clinical trial sample at low risk of alcohol or drug use, or protective, psychosocial factors, including the knowledge that they were to be urine tested at study visits, instead of the presence of OROS MPH. Additional risk factors not assessed in this study include familial/genetic risk of substance use. Although a long-term, randomized, placebo-controlled study of stimulant monotherapy would be ideal to evaluate this issue, such an approach may be unfeasible as it would deprive adolescents with ADHD of an effective treatment during a critical developmental period. The relatively small comparator sample of naturalistically treated ADHD youth who were not screened for active substance use is a further limitation. In addition, these comparator youth were not systematically drug tested, as were the clinical trial participants.
These prospective findings add to the literature on the relationship between treatment with therapeutic stimulants and AOD use in youth with ADHD. Further prospective clinical trials building on this work should aim to minimize differences between treatment and comparison groups to allow for more definitive conclusions about the impact of stimulants on alcohol and drug use in this at-risk population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In the past 12 months, Dr. Hammerness has participated as an investigator/principal investigator, in research studies funded by the following companies: Cephalon, Forest, Johnson & Johnson, Novartis, Ortho-McNeil Janssen, Shire, Takeda Pharmaceuticals and Elminda Ltd. Dr. Hammerness has also received royalties from Greenwood Press and advance from Harlequin Press. Joseph Biederman, MD, is currently receiving research support from the following sources: ElMindA, Janssen, McNeil, and Shire. In 2012, Dr. Biederman received an honorarium from the MGH Psychiatry Academy and The Children’s Hospital of Southwest Florida/Lee Memorial Health System for tuition-funded CME courses. In 2011, Dr. Biederman gave a single unpaid talk for Juste Pharmaceutical Spain, received honoraria from the MGH Psychiatry Academy for a tuition-funded CME course, and received honoraria for presenting at international scientific conference on ADHD. He also received an honorarium from Cambridge University Press for a chapter publication. Dr. Biederman received departmental royalties from a copyrighted rating scale used for ADHD diagnoses, paid by Eli Lilly, Shire and AstraZeneca; these royalties are paid to the Department of Psychiatry at MGH. In 2010, Dr. Biederman received a speaker’s fee from a single talk given at Fundación Dr. Manuel Camelo A.C. in Monterrey Mexico. Dr. Biederman provided single consultations for Shionogi Pharma Inc. and Cipher Pharmaceuticals Inc.; the honoraria for these consultations were paid to the Department of Psychiatry at the MGH. Dr. Biederman received honoraria from the MGH Psychiatry Academy for a tuition-funded CME course. In previous years, Dr. Biederman received research support, consultation fees, or speaker’s fees for/from the following additional sources: Abbott, Alza, AstraZeneca, Boston University, Bristol Myers Squibb, Celltech, Cephalon, Eli Lilly and Co., Esai, Fundacion Areces (Spain), Forest, Glaxo, Gliatech, Hastings Center, Janssen, McNeil, Medice Pharmaceuticals (Germany), Merck, MMC Pediatric, NARSAD, NIDA, New River, NICHD, NIMH, Novartis, Noven, Neurosearch, Organon, Otsuka, Pfizer, Pharmacia, Phase V Communications, Physicians Academy, The Prechter Foundation, Quantia Communications, Reed Exhibitions, Shire, the Spanish Child Psychiatry Association, The Stanley Foundation, UCB Pharma Inc., Veritas, and Wyeth. Stephen Faraonem, PhD, receives consulting income and/or research support from Shire, Otsuka and Alcobra and research support from the National Institutes of Health (NIH). He is also on the Clinical Advisory Board for Akili Interactive Labs. In previous years, he received consulting fees or was on Advisory Boards or participated in continuing medical education programs sponsored by: Shire, McNeil, Janssen, Novartis, Pfizer and Eli Lilly. Dr. Faraone receives royalties from books published by Guilford Press: Straight Talk about Your Child’s Mental Health and Oxford University Press: Schizophrenia: The Facts.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data derived from an Investigator Initiated Trial funded by Janssen Scientific Affairs (Clinical Trial Registration Number: NCT00181714).