
Abstract
Background and Need for Additional Treatments (Tx)
ADHD is a chronic, impairing brain-based neurodevelopmental disorder that costs billions annually in special education needs, underachievement, lost productivity, traffic accidents, and delinquency (Arnold, 2004). It predisposes to other psychiatric disorders and substance abuse, disrupts relationships and occupational functioning, and reduces the quality of life (Spetie & Arnold, 2007). Currently the best documented, most successful, and most widely used treatment (Tx) for ADHD is Food and Drug Administration (FDA)-approved medication (e.g., Arnold, 2004). However, even when administered in a careful algorithm with another established Tx for ADHD, behavior modification, 32% of children do not fully benefit from this presumed optimal combination Tx (Swanson et al., 2001). Furthermore, even for those with good initial response, no one has been able to document persisting benefit of medication beyond 2 years (e.g., Jensen et al., 2007; Molina et al., 2009). In addition, an unknown percentage of families refuse even to try medications because of fears about side effects and/or possible addiction. The 8-year follow-up of the Multimodal Tx Study of ADHD (MTA; Molina et al., 2009) noted the disappointing long-term results of current Tx and the need for new treatments.
Our recent reviews of complementary and alternative Tx for ADHD (Hurt, Lofthouse, & Arnold, 2011) identified neurofeedback (NF; also called electroencephalogram [EEG] biofeedback or neurotherapy) as one of the most promising. NF uses operant conditioning principles based on real-time measurement and processing of electrical activity measured from scalp electrodes to alter neural activation patterns. There has been an explosion of nondrug neuromodulation interventions over the last decade, driven in part by the discovery of brain plasticity. They are particularly relevant to ADHD because of the evidence from brain imaging for deviance in size and symmetry of brain structures in ADHD. They include EEG-NF, functional magnetic resonance imaging-neurofeedback (fMRI-NF), cognitive brain training, transcranial magnetic stimulation (TMS), transcranial direct current stimulation (tDCS), transcranial alternating current stimulation (tACS), deep-brain stimulation (DBS), and neuro-entrainment devices. EEG-NF is the oldest and best established of these interventions for ADHD. Figure 1 further illustrates the increased research interest in NF, with an exponential growth of publications over the last 5 to 8 years.
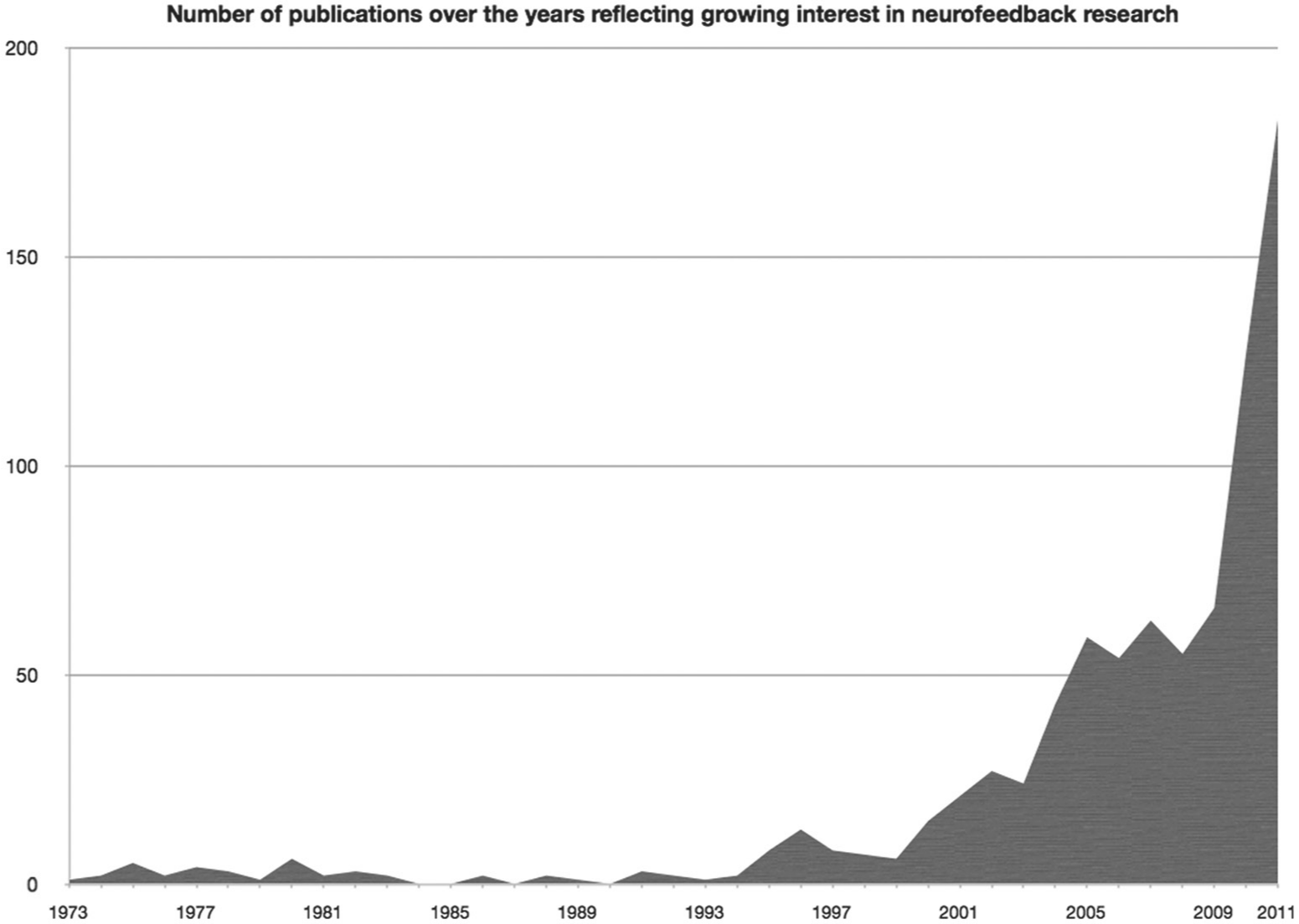
This figure demonstrates the growing interest expressed by the number of publications covering the term “Neurofeedback” or “EEG Biofeedback.”
Rationale of NF for ADHD
The theoretical and evidential foundation of NF for the Tx of ADHD is based on (a) the idea that the brain’s electrical activity can be conditioned and (b) research on the physiological basis of ADHD and EEG dysfunctions and their relationship to underlying thalamocortical mechanisms.
Classical conditioning of the EEG was shown as early as 1935 (Durup & Fessard, 1935). Jasper and Shagass (1941a) demonstrated that conditioning of the alpha-blocking response demonstrated all of the Pavlovian types of conditioned responses. They subsequently demonstrated voluntary control of the alpha-blocking response based on classical conditioning principles (Jasper & Shagass, 1941b), which laid the foundation for techniques currently known as NF. Thus, established studies demonstrate that classical conditioning can be applied to EEG parameters. More recent studies have demonstrated conditioning of not only cortical EEG (reviewed in Sherlin et al., 2011) but also more focal neuronal activity, such as in monkey frontal eye fields (Schafer & Moore, 2011), marmoset intracortical sensorimotor rhythm (SMR; Philippens & Vanwersch, 2010), human medial temporal cortex (Cerf et al., 2010), and early visual processing areas such as V1 and V2 (Shibata, Watanabe, Sasaki, & Kawato, 2011). The clinical applications of these techniques were not discovered until the beginning of the 1960s by Kamiya and Sterman (for review, see Kamiya, 2011; Sterman, LoPresti, & Fairchild, 2010) with the first clinical application for ADHD in 1976 (Lubar & Shouse, 1976).
Neuroimaging studies have indicated that ADHD is associated with smaller frontal lobes and other brain regions responsible for sustained attention, behavioral planning, and motor control (e.g., Swanson & Castellanos, 2002). PET and SPECT research has indicated reduced blood flow and metabolism suggesting electrophysiologic underarousal at frontal and central midline cortical regions in approximately 80% to 90% of patients with ADHD (Clarke, Barry, McCarthy, & Selikowitz, 2001). The most consistent EEG finding reported in the ADHD literature is increased absolute power in the slow-wave theta band (3.5-8 Hz: Bresnahan, Anderson, & Barry, 1999; Chabot & Serfontein, 1996; Clarke, Barry, McCarthy, & Selikowitz, 1998; Clarke et al., 2001; DeFrance, Smith, Schweitzer, Ginsberg, & Sands, 1996; Janzen, Graap, Stephanson, Marshall, & Fitzsimmons, 1995; Lazzaro et al., 1998; Lazzaro et al., 1999; Mann, Lubar, Zimmerman, Miller, & Muenchen, 1992; Matsuura et al., 1993), especially in central and frontal regions, probably reflecting underarousal of the central nervous system (Barry, Johnstone, & Clarke, 2003). Some studies have also reported decreased power in the beta band (12-21 Hz: Callaway, Halliday, & Naylor, 1983; Mann et al., 1992; Matsuura et al., 1993) and deviant sensory and cognitive processing for early and late stages of the event-related potential (ERP; Barry et al., 2003). Two meta-analyses of theta-beta ratio (TBR) have demonstrated that it differentiates children with ADHD from control groups (Boutros, Fraenkel, & Feingold, 2005; Snyder & Hall, 2006). However, a meta-analysis by Arns, Conners & Kraemer (2013) in this same issue reviews conflicting data and methodological limitations of studies supporting TBR in ADHD, although this measure still remains a core finding in a substantial subgroup of ADHD patients. Conceptually, this measure is in line with the EEG vigilance model originally developed by Bente (1964) and recently further developed by Hegerl, Himmerich, Engmann, and Hensch (2010), hypothesized to explain the ADHD symptoms and subtypes where decreased vigilance levels (excess frontal theta and also excess frontal alpha) explain the impairments in sustained attention and a vigilance autostabilization syndrome explains the hyperactive and impulsive behavior as a means to increase vigilance (Hegerl et al., 2010; Sander, Arns, Olbrich, & Hegerl, 2010).
In addition to these frequently reported findings, three other neurophysiological subgroups within ADHD have also been reported: (a) those with excess beta or beta spindling, which is more prevalent in males and responds well to stimulant medication (Arns, Gunkelman, Breteler, Spronk, 2008; Chabot & Serfontein, 1996; Chabot, Orgill, Crawford, Harris, & Serfontein, 1999; Clarke et al., 1998, 2001; Clarke et al., 2003; Hermens, Cooper, Kohn, Clarke, & Gordon, 2005); (b) those with paroxysmal or epileptiform EEG activity hypothesized to respond well to anticonvulsant Tx (for overview, see Arns, 2012); and (c) those with a slowed individual alpha peak frequency (iAPF), in general considered nonresponders to stimulants (Arns, 2012; Arns et al., 2008) but also nonresponders to other Tx such as repetitive TMS (Arns, de Ridder, Strehl, Breteler, & Coenen, 2009; Arns, Drinkenburg, & Kenemans, 2012) and antidepressants (Ulrich, Renfordt, Zeller, & Frick, 1984).
Previous Randomized Clinical Trials (RCTs) of NF for ADHD
Consistent with the previous findings, most studies investigating NF Tx of ADHD have used theta/beta NF (TBNF), with 9/15 studies included in a 2009 meta-analysis using TBNF at fronto-central locations (Arns et al., 2009). To date, 11 published studies have used a RCT controlled design (Arnold et al., 2012, this special section; Bakhsheyesh, Hänsch, Wyschkon, Rezaj, & Esser, 2011; deBeus & Kaiser, 2010 [a chapter]; Gevensleben et al., 2009, 2010; Holtmann et al., 2009; Lansbergen, van Dongen-Boomsma, Buitelaar, & Slaats-Willemse, 2010; Leins et al., 2007; Levesque, Beauregard, & Mensour, 2006; Linden, Habib, & Radojevic, 1996; Perreau-Linck, Lessard, Levesque, & Beauregard, 2010; Steiner, Sheldrick, Gotthelf, & Perrin, 2011). Most studies reported significant reductions in ADHD symptoms compared with a control condition. The 2009 meta-analysis by Arns of 6 peer-reviewed published randomized trials of NF for ADHD (Bakhsheyesh et al., 2011; Gevensleben et al., 2009; Holtmann et al., 2009; Leins et al., 2007; Levesque et al., 2006; Strehl et al., 2006) found a large effect (between-group effect size [ES]: d = 0.80) for inattention and medium effect for hyperactivity (d = 0.40) and impulsivity (d = 0.69). In a more recent review of 9 controlled RCTs that reported ESs (Lofthouse, Arnold, Hersch, Hurt, & deBeus, 2012), there was a medium between-groups mean ES of d = 0.54 for overall ADHD symptoms (0.54 and 0.55 for inattention and hyperactivity/impulsivity, respectively). In addition to these clinical improvements, normalization of ERPs after NF (Arns, 2012; Heinrich, Gevensleben, Freisleder, Moll, & Rothenberger, 2004; Kropotov et al., 2005; Kropotov et al., 2007; Wangler et al., 2011), normalization of EEG power post-Tx (Doehnert, Brandeis, Straub, Steinhausen, & Drechsler, 2008; Gevensleben et al., 2010), and effects on neural substrates of selective attention imaged with fMRI (Levesque et al., 2006) have been demonstrated. One of the larger studies reported stability of pre–post NF changes and superiority over the control condition on parent ratings at follow-up 6 months post-Tx (Gevensleben et al., 2010). In addition, uncontrolled follow-ups of 4 studies also found persistence and a trend for further improvement 3 to 6 months post-Tx (Heinrich et al., 2004; Leins et al., 2007; Strehl et al., 2006) and 2 years post-Tx (Gani, Birbaumer, & Strehl, 2008), although each study is limited in some manner casting doubt on their findings (Lofthouse, Arnold, & Hurt, 2010).
In addition, Gevensleben et al. (2009) found higher pre-Tx theta predicted larger clinical improvements after TBNF, explaining 20% of the variance, suggesting that preselection of participants, based on TBR, might enhance the clinical effects of TBNF, and thus act as a possible biomarker of Tx responsiveness. Similarly, in a nonrandomized study of TBNF of participants preselected for a deviating TBR, Monastra, Monastra, and George (2002) reported the largest within-participant ES to date for a NF study (Hedges’ d = 1.81) and recently a similar approach (where NF protocols were personalized) found a similar ES of 1.78 (Arns, Drinkenburg, & Kenemans, 2012). These three studies provide further support for the notion of personalizing treatments based on EEG biomarker.
These results are promising but not conclusive. Only 3 of the 10 peer-reviewed controlled RCTs used blinding and sham NF designs essential for controlling nonspecific Tx effects to measure specific effects of NF (Arnold et al., 2012; Lansbergen et al., 2010; Perreau-Linck et al., 2010). None of these studies showed superiority of NF over sham, but they were small studies having 8, 14, and 39 participants, respectively, and had several methodological issues that make interpretation difficult. Most importantly, none of these studies demonstrated that EEG learning (e.g., learning curves) had actually taken place; thus, we cannot assume that active NF was actually compared to sham.
Questions About Sham Double-Blinding
There has been a question whether NF should be evaluated as an unblindable psychological treatment (using the APA guidelines, for example: Arns et al., 2009; Sherlin, Arns, Lubar, & Sokhadze, 2010a, 2010b) or as a blindable treatment requiring a double-blind placebo-controlled study (e.g., Lofthouse et al., 2010, 2012). Sham Tx in NF research has been questioned on both ethical and practical levels. La Vaque and Rossiter (2001) argued against using a sham NF on the basis of the Declaration of Helsinki (World Medical Association, 1997). Those principles “prohibit designs that would withhold ‘the best proven diagnostic and therapeutic’ procedures from any participant” (p. 23). LaVeque and Rossiter instead suggested an active-control condition with known clinical efficacy. However, others have argued against this recommendation for several reasons (see Lofthouse et al., 2010, for review), including problems with defining and identifying “best-proven” Tx, the Declaration of Helsinki being aspirational, not mandatory; the difficulty of interpreting a result with no significant difference between two active treatments; the clinical and scientific necessity of a placebo study when there is minimal risk, valid informed consent, and protection of participants by other relevant ethical guidelines accompanied by need of important research for future clinical care; and the probability that placebo controls may require fewer participants than active controls and reduce exposure to risks of nonresponse and adverse effects. On such rationales, the FDA routinely requires placebo-controlled studies for new drugs.
The practical question about sham Tx in NF research involves three issues. First, researchers in the NF field have questioned whether a sham Tx condition can be developed that is truly inert and does not lead to learning via unintentional feedback. Such could occur by chance alone as there will be an unknown number of occasions in the long course of Tx when the child’s brainwaves will fall in the desired EEG Tx target range as random reinforcement is given. Unintended therapy could also occur via random feedback cuing the participant to engage in an activity (e.g., pay attention) and move into the desired EEG Tx target range. None of the three RCTs that used a sham Tx (Arnold et al., 2012; Lansbergen et al., 2010; Perreau-Linck et al., 2010) investigated the possibility of unintended feedback by examining EEGs of individual sessions. However, at the International Society for Neurofeedback and Research (ISNR) conference in Phoenix in 2011, Hill and Zaidel reported a study that used a sham NF versus real NF (albeit with a non-ADHD adult sample) and time-marked participants’ EEGs with rewards provided by the sham feedback; they found no unintended feedback associated with the sham (Hill & Zaidel, 2011).
Given the fact that NF is based on operant conditioning principles, the active treatment should be in line with principles of learning theory and conditioning principles for any learning to take place (reviewed in Sherlin et al., 2011) and a double-blind design may demand a deviation from such principles. Previous attempts at double-blinding have suffered from the use of auto-thresholding, which prevents “shaping” (making the learning target a “moving target”). Noncontingent feedback in some non-NF studies has been demonstrated to result in “superstitious behavior” in pigeon (Skinner, 1948) and man (Koichi, 1987). A sham condition must consider, prevent, and/or monitor such unintended learning.
A second practical issue is whether a sham Tx that is truly inert in accordance with learning theory principles can be validly blinded to participants, informants, and experimenters. As none of the three RCTs tested the inertness of their sham Tx, there are no data on this issue specific to ADHD. However, Hill and Zaidel (2011), using technology similar to that in the study proposed here, reported participants were unable to guess their assignment better than chance, and by the 4th Tx the two randomly assigned groups diverged significantly in EEG parameters. This suggests that the active Tx but not the sham was having an effect on the EEG and the participants could not tell the difference. One of the participants worked elsewhere as a NF technician, but had not herself received any EEG Tx before this experiment. During Tx, she was convinced she was receiving “real” NF even though actually assigned to sham. In addition, Arnold et al. (2012) examined blinding validity for participants and parent informants and found their guesses about the Tx assignment were no better than chance, suggesting that blinding a sham NF Tx is possible.
The final practical concern is whether a sample can be recruited and retained through assessments and 40 Tx sessions when using a truly inert sham Tx that is validly blind to all. Some NF investigators thought that families would not consent to a study with a sham condition. Unfortunately, the three sham-controlled RCTs did not systematically examine the inertness of their sham Tx and then test blinding. However, Arnold et al. (2012) were able to successfully recruit 39 participants in 2 school years with 87% retention for 40 Tx, with excellent blinding of children and parents, and the sham group (as well as active group) showed no obvious EEG changes in a simple pre–post measure of TBR.
The proposed design in this manuscript will, for the first time in the field, incorporate time stamping of sham-condition reinforcement events on the sham subject’s real EEG, making it possible to determine post hoc if there may be inadvertent contingencies generated by the sham condition. Trainer/technician blindness will also be insured by a carefully crafted technology described below and demonstrated by Hill and Zaidel (2011) and will be checked by trainer guesses at treatment end.
Pilot Work
The NIMH-funded Ohio State University (OSU) pilot feasibility study (Arnold et al., 2012) indicates that a well-blinded large RCT of NF utilizing a sham control of equal intensity and duration is feasible. It showed that participants can be recruited and retained for 40 Tx knowing they might be assigned to the control condition. The retention rate was 87% for 40 Tx, 92% for 20 Tx even though participants had to give up medication to be in the study and three of the five dropouts quit specifically to obtain medication. Guesses about Tx assignment by parents and children were no better than chance. The discouraging exploratory comparison of active Tx to placebo (no significant difference in benefit) makes a large double-blind randomized trial all the more necessary in view of the multiple positive studies in the literature with control groups that were not blinded. The pilot results suggest the following: three Tx per week as the most feasible, efficient, and palatable; use of a large sample, selectively recruited with a high TBR; age > 7 years, including children on stimulant medications as well as unmedicated (for sample representativeness and to prevent attrition); and using quantitative EEG (QEEG) and tracking of the noncontingent random reinforcement to check the inertness of the sham NF.
The Collaborative NF Project
Following presentation of the NIMH/OSU pilot study results at the 2010 ChADD annual meeting, a group of ADHD investigators and NF experts began talking about collaborating on a large, multisite, double-blinded RCT of NF for ADHD. For over a year since then, this group had weekly teleconferences to plan this study and develop a grant application. The cross-site investigational team was selected not only for balance between NF and mainstream ADHD investigators but also for expertise in Tx strategy, assessment, design, biostatistics, data management, and multisite RCT execution. Initially, this group included the full spectrum of views commonly expressed in the fields of NF and ADHD, including a passionate advocacy of NF for ADHD and an equally passionate skepticism. Despite initial disagreements requiring intense discussion and revisiting of available data, a high level of collegiality developed, based on examination of data and recognition of a shared primary interest to rigorously examine NF with a design producing results (whatever they are) acceptable to all. The objective is to see whether there is a specific effect worth supporting, by third party payers as well as the community.
There will be four sites, two university-based (OSU [with Drs. Nicholas Lofthouse and L. Eugene Arnold, co-PIs] and University California San Francisco [UCSF; Dr. Keith McBurnett]) and two based at NF clinics (a private clinic associated with University of North Carolina [UNC; Dr. Roger deBeus, PI], and The Neurodevelopmental Center, RI [Dr. Laurence Hirshberg, PI]), each of which will recruit 45 participants. In addition to these site investigators, the study will include a consultation team of experts in the fields of NF (Drs. Joel Lubar, Vincent Monastra, Cynthia Kerson, and Martijn Arns), ADHD RCTs (Drs. Keith Conners, Helena Kraemer, and Arnold), statistics (Drs. Kraemer and Jeff Pan), and data management (Dr. Robert Rice). The proposed protocol received plenary critique at the 2011 meeting of the ISNR and was revised in that light.
Proposed Study Primary Goals, Specific Questions, and Hypotheses
The major aims are to test whether NF has specific benefit for ADHD, whether benefit persists for 2 years beyond Tx end, and whether the putative biomarker for responsiveness and mechanism of action, TBR, is valid. Current literature about NF’s specific benefit in ADHD is inconclusive. The proposed double-blind RCT will build on the recently completed NIMH-funded pilot feasibility trial to clarify the evidence base of a promising Tx that has the potential for filling a critical gap in the ADHD Tx armamentarium, especially for Tx with enduring effect.
Question 1: Does NF Have a Specific Benefit Beyond Placebo Response? (Primary Question)
Hypothesis 1: Children randomly assigned to NF will, when assessed in an unmedicated state, show significantly greater reduction of inattentive ADHD symptoms rated by parents and teachers than those assigned to double-blind placebo sham Tx of equal duration, intensity, involvement, and appearance (primary outcome).
Additional analyses
In elucidation of the primary outcome, other outcomes, such as parent- and teacher-rated hyperactive-impulsive symptoms, other psychiatric symptoms, impairment, clinical global impression (CGI), and neuropsychological test scores should also improve more with NF than with placebo sham.
Question 2: Does NF Benefit Persist After Termination of Training?
Hypothesis 2: At 6-month, 1-year, and 2-year follow-ups, children who received NF will have equal or better levels of inattentive symptoms than at completion of training. When assessed in an unmedicated state, their inattentive symptoms will be significantly less severe than those who did not receive NF.
Additional analyses
In elucidation of this outcome, the NF group should have more medication discontinuers, fewer medication starters, and lower average medication dose than in the placebo group.
Question 3: Are There Subgrouping or Other Variables That Moderate NF Tx Response?
Hypothesis 3: Initial TBR will moderate Tx effect: Those with higher baseline TBR will show significantly greater advantage of NF over sham placebo than those with a lower ratio.
Additional analyses
Exploratory (hypothesis-generating) analyses will include other EEG variables and demographic and clinical variables to investigate other possible moderators and nonspecific predictors of NF outcome, and to develop an optimal moderator paradigm combining multiple individual moderators.
Question 4: Is NF Benefit Mediated by the Hypothesized EEG Power Changes?
Hypothesis 4: Decrease in EEG TBR will significantly mediate therapeutic effect of NF, especially at follow-ups.
Additional analyses
Improvement in ERP and a measure of within-session EEG change will also be examined as possible mediators of NF therapeutic effect.
Question 5: Does Selection for High TBR Select a “Diagnostic” Subgroup (Biomarker) That is Uniformly Responsive to Tx Regardless of ADHD Subtype?
Exploratory analysis
Variability in response on the primary outcome should be significantly less (variance of the change score will be lower) than for published medication trials, which do not select for a biomarker.
Question 6: What Deeper Brain Structures Have Their Function Affected by NF?
Exploratory analyses
Low-resolution electromagnetic tomography (LORETA) of ERP is an EEG-based form of brain imaging inexpensive enough to allow application to all participants. LORETA will be applied at baseline and endpoint QEEG and at ERPs in neuropsychological testing. The localized deep brain changes identified will be explored as outcomes and mediators.
Question 7: What Proportion of Well-Diagnosed ADHD Has Excess Eyes-Open TBR?
Although the literature substantiates a significant difference in TBR between normal controls and ADHD, the exact distribution of theta-beta power in ADHD is unclear because of varying conditions and definitions across studies and a possible secular trend in normal children. This study will standardize screening conditions in a large current sample (expect ~300, possibly more, to screen).
Exploratory descriptive analysis: We expect that about 50% to 85% of 7- to 10-year-old children with rigorously diagnosed ADHD will have eyes-open specifically defined theta-beta EEG power ratios ≥5.0.
Study Design
The design will be a multisite, parallel-group, double-blind randomized comparison of active NF (n = 108) to sham NF (n = 72) for up to 38 treatments in a 13-week period, with 6-, 13-, and 25-month follow-ups, in 180 children aged 7 to 10 years with Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) ADHD diagnosis.
Randomization ratio
As Woods et al. (1998) recommended a less than 1:1 proportion of placebo assignment when the main interest is in comparing issues of active Tx, we decided to randomize participants at each site to active versus sham in a 3:2 ratio, in blocks of five, balanced on current ADHD medication. With Dr. Kraemer’s consultation, we decided on 40% of the sample with sham as statistically adequate and ethically desirable (as well as useful for recruitment) to minimize the sham exposure, in view of the fact that the sham participants will be considerably inconvenienced. A 3:2 randomization ratio requires only negligible increase of the number. The slightly unbalanced randomization has been considered in the power analysis below. Randomization will be supervised by the study biostatistician and data management center (DMC) staff who will not have any contact with participants or assessments, and will be implemented by an unblinded consultant who has no contact with participants.
Participants
Inclusion criteria
Participants will be 180 boys and girls aged 7 through 10 years with IQ ≥ 80 and rigorously diagnosed DSM-IV-TR (4th ed., text rev.; APA, 2000)ADHD inattentive type or combined type (structured interview and doctoral-level clinician using DSM criteria). To insure clinically meaningful severity, all participants will have an item mean ≥1.5 SD above norms on a 0-3 metric on parent ratings of either DSM inattentive symptoms or all 18 ADHD symptoms and on teacher ratings of either inattentive symptoms or all 18 ADHD symptoms (while off medication for purposes of assessment). They also must have an eyes-open QEEG with theta-beta power ratio ≥5.0, well above the normal mean for age based on norms by Monastra et al. (1999) and Snyder and Hall (2006). If participants are taking stimulants for their ADHD, they can continue taking them during the study but must discontinue temporarily a week before major study assessments (baseline, Tx 20, Tx 40, and follow-ups) to prevent biasing the results.
Exclusion criteria
Participants will be excluded if they have a comorbid disorder requiring psychoactive medication other than FDA-approved ADHD medication, a medical disorder requiring systemic chronic medication with confounding psychoactive effects, sleep apnea, restless legs syndrome, IQ < 80, plans to move requiring school change during the next 3 months, plans to start other ADHD Tx in the next 3 months, antipsychotic agent in the 6 months prior to baseline assessment, fluoxetine in the 4 weeks prior to baseline, other psychiatric medication in the 2 weeks prior to baseline, or previous NF of >5 Txs. (Stable stimulant medicine is allowed but must be stopped for a week prior to major assessments.) Based on unpublished data of one of the consultants, vitamin D deficiency will be a temporary exclusion; after repletion, candidates who still meet diagnostic categorical and severity criteria may enter.
General Plan and Procedures
The study will run for 5 years; the first 3 years will involve participant recruitment and NF Tx (either active or sham) and the remaining 2 years will involve completion of 6-, 13-, and 25-month follow-ups for the later-recruited participants, completing the data cleaning, running statistical analyses, and publishing study findings. To capture teacher data each year, recruitment will begin at the start of the school year and continue until 3.5 months before the end of the school year, similar to what was done in the OSU pilot study, which successfully recruited 39 participants in 2 school years. All participants will undergo a comprehensive psychiatric, medical, and QEEG screen, with parent-, teacher-, and clinician-based assessment to determine study eligibility.
Medical problems that could mimic ADHD will be ruled out by medical review and physical exam, with any indicated laboratory work before participants are randomized. Vitamin D will be tested in all participants because one of the planning group members has prepublication data showing a high rate of D deficiency in ADHD, with many symptoms responsive to repletion. Those who are deficient will have appropriate supplementation before being reevaluated for entry.
After clinical eligibility criteria are met (DSM-IV-TR diagnosis and 1.5 SD above norms on teacher and parent ADHD symptom ratings) a one-channel EEG recording will be obtained at Cz. If the TBR is 5:1 or more, the participant will have a 19-channel QEEG to determine which site to train (F3, Fz, Cz) based on the most deviant of the three sites by inspecting their power spectral displays. In addition, determining the peak amplitudes within them will establish the frequency ranges for training, using up to 4-Hz bins within 3-9 Hz for theta and 13-21 Hz for beta.
Parent and teacher ratings (composited for primary outcome) of inattentive symptoms will be obtained at baseline, every 10 sessions during Tx, at post-Tx (after the 38th Tx) and at 6-, 13-, and 25-month follow-ups. Neuropsychological measures will be conducted at baseline, mid- (at the 20th session), and post-Tx (at Session 40), and at follow-ups. Clinician ratings will be obtained at baseline, Session 20, post-Tx, and follow-ups. QEEG and ERP data will be collected at baseline, post-Tx, and 13-month follow-up. IQ and academic functioning will be tested at baseline, 1-year, and 2-year follow-up. Information about adverse effects and the NF Observer Rating System will be collected every Tx session. Changes in concomitant Txs will be monitored every session and at follow-ups. Finally, child and parent satisfaction and child, parent, and trainer blinding will be examined at the post-Tx assessment. Study staff administering the assessments will also receive this blinding question at the post-assessments.
Tx strategy and number
The intended Tx is downtraining of theta power and uptraining of beta power for 38 Txs of active NF versus 38 Txs of sham NF using stored EEGs to preserve the blind. It has been conventional in clinical and research NF to administer between 20 and 40 Tx. The OSU pilot feasibility study suggests asymptote of improvement by Tx 24, but that result is questionable because no EEG learning curve was demonstrated. The Arns et al. (2009) meta-analysis shows the best ES to be in studies that used 35 Txs or more. In this study, we are planning 40 sessions; however, Sessions 20 and 40 will be used for major assessments, leaving 38 sessions of actual Tx, which the NF experts on the team assure should be sufficient for optimal benefit.
As part of the protocol, without breaking the blind, all participants will have clinical progress (parent and teacher ratings of ADHD symptoms) evaluated at Session 20 (after Tx 19), and those who have not shown a beginning of response (at least 10% decrease in symptom score averaged across raters) will for ethical and cost reasons exit double-blind study Tx (but not the study) and have conventional clinical follow-up with some assistance to reimburse Tx costs such as prescription copays or behavior therapy. Analysis of data from two different studies shows that those who do not show at least 10% improvement by Tx midpoint do not respond to the full Tx, whether active NF or control condition (Arns, Drinkenburg, & Kenemans, 2012). Every Tx has nonresponders (up to 20%-30% for FDA-approved drugs), so it should not be surprising that we anticipate some nonresponders in this trial. Because of the patient and family time and effort burden and the cost to the study of wasted Tx, it is desirable not to continue a Tx that we can tell with confidence is not working. Active NF and placebo participants will be treated alike in this regard, without breaking the blind. All participants will be included in follow-up assessments at 6 months, 1 year, and 2 years, and in intention-to-treat (ITT) analyses, all Tx received will be tracked for subgroup and covariate analyses.
Tx fidelity
An important issue will be quality assurance of optimal and reliable NF. All trainers/technicians will receive initial reliability training from Drs. Lubar and Monastra, acknowledged leaders in the field. Then Drs. Lubar and Monastra will monitor and promote Tx fidelity by reviewing videotapes of Tx sessions five times during Tx for each participant, by visiting each site yearly to observe, and by phone consultations as needed.
Follow-up times
The 1-year follow-up will actually be done at 13 months from baseline, making it 10 months from completion of the 3-month NF Tx, the same time lapse as the MTA (the “gold-standard” of Tx outcome studies in ADHD) 24-month assessment was from the end of the 14-month MTA Tx. Similarly, the 2-year follow-up will be 25 months from baseline, 22 months from Tx end, the same time lapse from Tx end as the MTA 36-month assessment. Thus, considering the elapsed time from study Tx end to examine persistence of effects, our 1-year assessment will match the MTA 24-month assessment and our 2-year assessment will match the MTA 36-month assessment. The importance of this is that the MTA medication advantage had attenuated by 24 months and was lost by the 36-month assessment. Therefore, if the NF advantage persists to 2 years, it will suggest more staying power than medication after cessation of study Tx, an important public health and cost consideration, and would warrant more direct comparisons in future studies.
Blinding strategy
To facilitate the double-blind sham-controlled method this study will use, participants assigned to sham and their trainers will be fed EEG data from prerecorded files rather than from the participant’s live signal. All other actions and controls are the same as using live data. To prevent unblinding of experienced NF trainers/technicians, the stored sham signal is responsive to any artifact activity that arises in the simultaneously recorded (and saved) real-time EEG (by blending the artifactual signals from electromyographic (EMG) and electrooculogram (EOG) into the prerecorded EEG) so that the provider controlling the feedback cannot differentiate between live and simulated data. The saving of the real EEG, which is time marked with the rewards provided by the sham feedback, will allow for investigation of the possibility of any unanticipated real reinforcement. To insure blindness of the NF trainer, the prerecorded EEG data will be a series of 38 consecutive EEGs from the same age-matched clinical case so that the EEGs of the sham group will also show “training progress” over successive sessions the same as real NF should.
Even the Tx fidelity monitors (Drs. Lubar and Monastra) will maintain the blind. Although they will be reviewing actual EEG summary data for all participants and making sure that the training parameters were reset for all participants in accordance with the protocol used for this study, this will not unblind them. They will implement the same process for all participants without knowing whether the participant received “real” or “sham” feedback; they do not need to see the actual EEGs to make sure that the time per task increases after the 10th, 20th, and 30th sessions. They only need to inspect the computer data that indicates time per task and review the patient–therapist interactions (videotaped or on-site visit) to confirm that coaching is optimal.
NF Tx equipment EEGer will be the NF software, which has been widely used for 10 years. For hardware, the Thought Technology and Brainmaster hardware will be used. The hardware and software have been used by thousands of NF providers in research and clinical settings. Although the software allows for considerable customization, the basic training screens allow for provision and removal of rewards for three bands of EEG activity, one to be used to remove reward when theta amplitudes exceed the threshold set, one used to provide reward when beta amplitudes exceed the threshold set, and one used to remove reward when EMG activity increases, as indicated by increases in amplitudes of activity above 65 Hz. Thus, a range of formats is available for visual and auditory feedback. All contingencies and all threshold changes are time stamped on the EEG record, which is stored for later analysis. At baseline, end of Tx, and 1-year follow-up, a 19-channel EEG will be recorded with Mitsar 202 amplifiers and the WinEEG software (Mitsar, St. Petersburg, Russia). EOG correction based on Gratton, Coles, and Donchin (1983) will be applied to the 19-channel recording and these data will be further de-artifacted (such as muscle artifact and residual EOG) using NeuroGuide Deluxe (NeuroGuide, St Petersburg, Florida). The Mitsar system will be used for QEEG and ERP neuropsychological testing.
Outcome Measures
The standardized psychiatric diagnostic interview at screening and follow-ups will be the Children’s Interview for Psychiatric Syndromes–Child (ChIPS) and Parent (P-ChIPS) versions (Weller, Weller, Fristad, & Rooney, 1999a, 1999b; Table 1). Parent-rated scales will include the Conners–Third Edition: Long Version (C-3:P; Conners, 2008), Impairment Rating Scale (IRS; Fabiano et al., 2006), and the Children’s Sleep Habits Questionnaire (CSHQ; Owens, Spirito, McGuinn, & Nobile, 2000).
Multi-Informant Schedule of Measures.
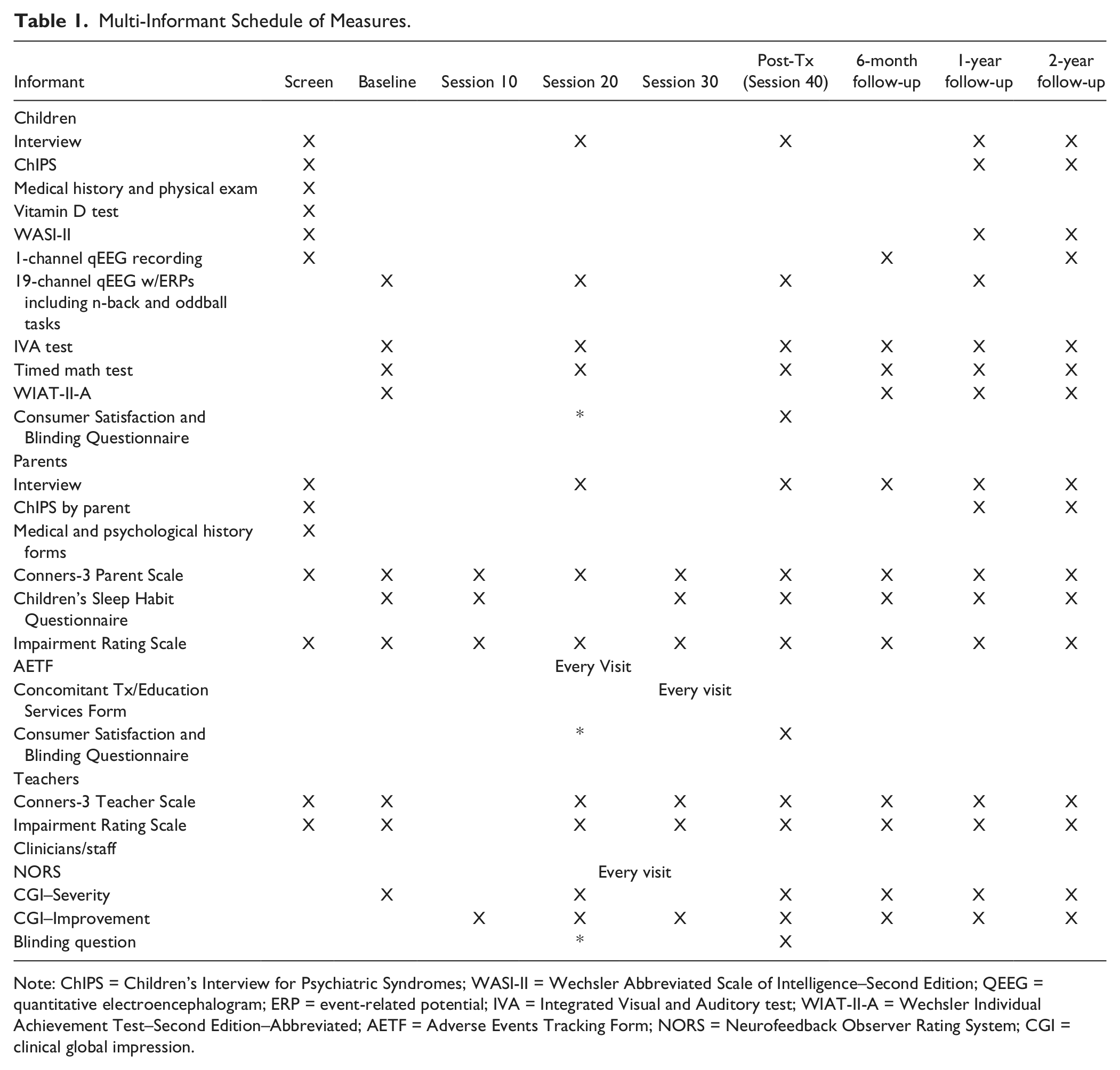
Note: ChIPS = Children’s Interview for Psychiatric Syndromes; WASI-II = Wechsler Abbreviated Scale of Intelligence–Second Edition; QEEG = quantitative electroencephalogram; ERP = event-related potential; IVA = Integrated Visual and Auditory test; WIAT-II-A = Wechsler Individual Achievement Test–Second Edition–Abbreviated; AETF = Adverse Events Tracking Form; NORS = Neurofeedback Observer Rating System; CGI = clinical global impression.
Teacher-rated scales will include teacher versions of the C-3 and IRS. The 18 DSM ADHD symptoms from the parent and teacher C-3 will be used for the severity inclusion criterion. Clinician and staff ratings will be the CGI (Guy, 1976) and the Neurofeedback Observer Rating Scale, used in the NIMH-OSU pilot feasibility study. Intellectual and academic functioning will be measured by the Wechsler Abbreviated Scale of Intelligence–Second Edition (WASI-II; Wechsler, 2011), Wechsler Individual Achievement Test–Second Edition–Abbreviated (WIAT-II-A; Wechsler, 2001). Neuropsychological testing will include the Human Brain Institute (HBI; St. Petersberg, Russia) oddball and n-back tasks for ERPs (further discussed below), the Integrated Visual and Auditory test (IVA; BrainTrain, Richmond, VA, USA), continuous performance test, and a timed arithmetic test found to be a sensitive measure of Tx effect in drug studies (e.g., Arnold et al., 2004). Adverse effects and changes in concomitant Tx will be monitored by the Adverse Events Tracking Form (AETF) and Concomitant Tx/Education Services Form (CTESF) used in the NIMH-OSU pilot feasibility study of NF.
Blinding checks
The Consumer Satisfaction and Blinding Questionnaire (CSQ; Parent and Child) successfully used in the OSU pilot study will also be used to measure parent and child satisfaction with NF Tx and blinding to assigned Tx condition. The same “blinding” question from the latter questionnaire will be administered to the clinicians and study staff conducting assessments.
EEG data will mainly track changes in the TBR, which is the primary training target. Resting EEG will also be examined by a region of interest (ROI) analysis to identify functional changes in predefined prefrontal cortical areas (dorsolateral prefrontal, orbitofrontal, ventrolateral prefrontal, and dorsal anterior cingulate). Cortical response during attentional or cognitive processing will be measured through analysis of ERPs. ERPs show time-locked responses to either external or internal stimuli, which are extracted from the EEG while the participant is performing a neuropsychological task, in this case n-back and oddball tasks. The responses are averaged over many trials and reflect early attentional processing and higher cognitive processes, such as memory and expectation. ERPs have been studied in ADHD and have been demonstrated to normalize after NF Tx. The n-back and oddball ERP tasks will be used to investigate whether normalization of ERPs occur by (a) comparing the pre- to post-Tx ERPs and (b) comparing both of these to the sham control group, with a specific focus on the late-cognitive parts of the ERP (e.g., P300). Furthermore, these ERPs will be submitted to source localization using LORETA to investigate which deeper functional areas are implicated.
Functional brain imaging strategy
LORETA uses an inverse solution equation to locate activation in deeper grey matter structures based on EEG signals detected on the cortical surface. This measure has been reported to accurately map activity from several cortical regions. In a recent review and meta-analysis on the rostral anterior cingulate and its role in predicting Tx response to antidepressants, Pizzagalli (2011) found that studies using LORETA-based EEGs exhibited similar ES as fMRI and SPECT scans, demonstrating LORETA’s utility as a robust, reliable alternative to fMRI, with higher temporal resolution and considerably less expense.
Data management
Data will be centrally managed by the OSU DMC under the direction of Dr. Robert Rice, who has worked closely on other multisite trials. Using Teleform (Cardiff Software, Vista, CA, USA), the DMC will use fax technology to convert completed forms to TIFF images that will be emailed and processed through Teleform into a SQL server database. The DMC will invoke 25 procedures and programs to scrub and clean the data. The DMC will provide sites with monthly productivity reports that will include missing forms, missing data, late visits, and accrual information.
Statistical considerations
Participants will be centrally randomized to the two groups, Tx (T) and control (C), stratified by site, with probability of 60% into T. Sample sizes at each site will be approximately equal. The primary outcome measure (and most of the secondary outcome measures) will be obtained (blinded to Tx group) at baseline and periodically throughout Tx.
Analytic strategy
After blinded data cleaning, demographic and recruitment information will be summarized by randomly assigned Tx groups. Outcome measurements will be plotted and summarized over time by Tx group. Visual displays of each measurement will be generated. Missing data patterns will be summarized and reported.
The conclusion comparing T versus C will be based on the primary outcome variable (average of z scores of parent and teacher ratings of inattentive symptoms). The primary hypothesis will be tested at significance of 0.05. Holm’s procedure will be used for the testing of multiple secondary outcomes. Exploratory (hypothesis-generating) analyses will be done to generate hypotheses for future studies and to detect possible moderators of Tx on the various outcomes (baseline variables that identify patients on whom the effects of T vs. C differ). Such moderators are important scientifically, suggesting etiologies of the disorder, but also important clinically, in that they help target the Tx to those most likely to have positive response. Besides these, the ES (with its 95% confidence interval) for all outcome measures will be summarized after 19 and 38 Tx sessions and at follow-ups.
The primary analysis of Tx effect of 38 sessions will be based on a linear mixed model with repeated measurement, assuming a linear response on ln(t + 1), where t is time from randomization, to fit the curvilinear response trajectory typically seen in RCTs. The focus is to show that the trajectories, here determined by the individual slopes of the response on ln(t + 1), in the T-group are clinically preferable to those in the C-group. Analyses of the effect at follow-up will be based on the corresponding contrast of mixed models for repeated measurement with unstructured covariance matrix over time. The analyses will include a Tx effect, a site effect, and a Tx × Site interaction.
In multisite RCTs, although all sites adhere to the same research protocols, there are often major site differences. With the planned monitoring for fidelity to research protocols, we would not expect a Tx-by-site interaction (indicating differences in ES from site to site), but it would not be surprising to find a site effect (indicating different populations from which participants are drawn and different research staffs).
Analysis will be done by ITT, that is, every patient randomized will be taken into account. Although every effort will be made to avoid missing data or dropouts, mixed models are particularly useful in dealing with missing data problems. In addition, sensitivity analyses will be carried out using data imputation techniques based on propensity score or linear regression models.
Power and sample size
The critical ES has been set at d* = .5 (standardized mean difference between T and C, corresponding to a number needed to treat = 3.6), generally considered a moderate ES. For a two-tailed test of the primary outcome, in this four-site design, 140 participants are required (T:C ratio of 3:2) to provide at least 80% power to detect an ES of d* = .5 or larger, at significance level of 0.05. To allow for the 10% to 15% attrition found in the pilot feasibility study, and to provide additional degrees of freedom for the moderator and mediator analyses, we plan to randomize 180, to make 45 per site, with 27 randomized to T and 18 to C at each site.
Rationale for This Design: Issues and Alternatives Considered
In the 16 months of teleconference and email discussions leading to the proposed design, we considered many alternatives. Chief among these was the choice of control group. Considerable and evolving sentiment supported using a clinically practical comparator such as optimal medication, EMG biofeedback, or a computer-based (perhaps even Internet based) training of attention and cognitive skills. Although these were attractive possibilities, we agreed, after considerable debate, that the most pressing issue was to establish whether NF has a specific effect beyond placebo; and those other comparisons would best await resolution of that primary issue. Thus, comparison to a double-blinded sham seemed necessary, while adhering to conditioning principles and remaining close to how the Tx is applied in practice.
The sham itself and the related blinding strategy entailed considerable discussion. The blinding strategy and technology used in the NIMH-OSU pilot feasibility study (Arnold et al., 2012) did not seem appropriate for this one. It used the CyberLearning Technology with “fuzzy logic,” which continually shifted the threshold; and it used a videogame to provide reinforcement rather than a coach dispensing rewards for meeting a fixed threshold that could be manually adjusted. The NF experts in the planning group did not consider this optimal nor is it the way the majority of NF is done clinically.
To give NF its best chance to demonstrate a specific benefit, we needed to use the most widely established and optimal Tx method, using manually set thresholds and active coaching. How to blind this then became the challenge. One possibility might be to train posterior alpha as the control Tx. However, circulation of this idea to the broader NF community elicited feedback pointing out flaws, including that posterior alpha training would probably be beneficial to a substantial minority. The most preferred optimal method for double-blinding became the use of a stored EEG on which the participant’s eye movement and other artifacts are overwritten with the NF trainer dispensing rewards based on the stored EEG rather than the participant’s actual EEG. This strategy was fortuitously and successfully “field-tested” in a different type of study presented at a recent ISNR annual conference (Hill & Zaidel, 2011). We will, of course, check on the adequacy of blinding by an end-of-study questionnaire, and will examine the participants’ actual EEGs with reinforcements time marked, to check that the sham was indeed inert and not accidentally reinforcing.
Once we decided that the active training would involve TBR, the NF experts on the team struggled with the decision of what would be the best TBR threshold algorithm for standardizing conditions of measurement, and what theoretical underpinnings would validate this decision. All NF studies that included TBR as a main feature reported it differently. The group had to consider where, under what task, and what TBR standards should apply. Some studies reported eyes-closed (EC) TBR, whereas others used eyes-open (EO), whereas others reported an average of different conditions, including tasks such as reading or drawing. The minimal amount of time of the artifacted record was an important issue. For example, if data are artifacted and used from later in the recording rather than the first 2 min, there could be a spuriously high theta power. After review of all relevant literature, we decided that 2 min of clean data during EO at Cz, Fz, and F3 would determine inclusion and training parameters and that the best cutoff ratio for inclusion would be TBR ≥ 5.0.
The actual handling and artifacting of the screening EEG assessment required discussion as this information would further determine Tx parameters and statistical decisions. Recognizing the lack of standards in this area of neurophysiological evaluation, we decided that an artifacting strategy involving spectral power analysis and EOG correction would be optimal.
Another area entailing considerable discussion was whether to allow stimulant medication during the study. There were good arguments on both sides. It was complicated by the observations of the NF experts in the planning group that effective NF sometimes reduces the optimal medication dose, requiring dose adjustment to relieve side effects. The NIMH-OSU pilot feasibility study excluded ADHD medication because we were attempting to develop response curves with very frequent parent and teacher ratings. This became problematic, as 3 of the 5 dropouts (of 39 randomized) dropped out to resume or obtain medication. Thus, although having drug-free participants would be “cleaner,” it could increase attrition. Furthermore, excluding medication would make the sample unrepresentative of ADHD because a substantial proportion of those taking medication might not be willing to give it up for 3 months. Therefore, we decided that the best solution is to allow established stimulant medication to continue through the trial but have it wash out for a week before each major assessment, and to educate parents about the need to monitor for medication side effects and consider dosage reduction (study physicians will be available to advise the prescriber as needed).
As with most studies, there was a tension between the desires for optimal, comprehensive assessment and the practicalities of participant burden and cost. At one time, we had six neuropsychological tests, which we reduced to four to shorten the assessment. Similarly, we reluctantly discarded several scales that were not essential. We retained the most commonly used sleep measure, the CSHQ (Owens et al., 2000), because one of the planning group members has some unpublished data suggesting that a mechanism of NF benefit is via sleep improvement mediated by sleep-spindle (Arns & Kenemans, 2012), and it seems important to have some data for an exploratory analysis in that regard. Originally, we had planned a comprehensive screening battery of blood tests, which was reduced because of cost to a test for vitamin D and anything else the medical history and physical exam raise suspicion about. Relatedly, the neurophysiological assessments were discussed at great length. Ultimately, the Integrated Auditory and Visual Continuous Attention Test (IVA) and HBI ERP tasks were chosen to have a CPT-like task for repeated assessment (IVA) and a CPT task during an EEG recording enabling us to also investigate the neurophysiological changes associated with this task via ERPs. Many other options were considered and some were initially included but jettisoned due to time and funding constraints.
In clinical practice, NF trainers often respond to within-session EEG changes by adding training of areas not related to the initial QEEG interpretation. However, the need to provide a standardized protocol thwarted this common personalized NF approach. It limited the study to doing NF at one of three sites (Fz, CZ, or F3) only and allowed only changes responding to frequency shifts at the same site throughout the 38 training sessions.
It would also have been desirable to include functional MRI or similar high-resolution brain imaging for exploratory detection of possible moderators or biomarkers. Cost containment foreclosed that option. Therefore, we decided on LORETA as a way of visualizing electrophysiologic changes in deeper brain structures during rest and ERP task.
The age range was an important topic. The experience in the OSU pilot encouraged us to raise the lower end of the age range to 7. At first, we planned to go up to age 14. However, reports of TBR showed a sharp change at about age 11 to 12 years in normal TBR. We were concerned about including too much maturational heterogeneity, the need for two different norms for sample selection, and the practical difficulty of deciding the correct norms for the transitional age of 11 to 12 years. Therefore, we settled on the 7 through 10 age band. This age also has a secondary advantage of being roughly comparable with the age of the MTA sample for cross-study comparisons.
At first, we had hoped to have doctoral-level licensed clinicians to optimize the Tx. However, this was reconsidered because of expense. The NF experts in the planning group thought that master’s level technicians or postdocs trained and monitored by Drs. Lubar and Monastra would be a reasonable solution.
An important decision with implications for public health application was whether to take all who met the ADHD categorical and dimensional criteria or restrict the sample based on QEEG finding of elevated TBR. On one hand, it would be good to be able to generalize the findings to all moderate-to-severe ADHD. One the other hand, taking those without the EEG abnormality targeted by the treatment would risk diluting the signal from the appropriate participants with the noise from those who had no chance to improve because they did not have the problem targeted. Ultimately, we realized that even if the required elevation of TBR selected only a third of those with ADHD, that would still have public health importance, representing 2% to 3% of all children at the current estimates of child population incidence.
A related decision was whether to have only one protocol for all and personalize by selecting the participants (with high TBR) who matched the treatment or have treatment options and personalize by taking everyone and matching the Tx to the participant. The latter was tempting because there is some evidence that those without high TBR might benefit from other strategies, such as uptraining SMR (12-15 Hz) or training slow cortical potential. However, we felt that in this first large-scale attempt to demonstrate a specific effect, we should focus on the approach with the most encouraging evidence to date, namely, downtraining TBR in those with a high TBR.
Conclusion—Study Innovations and Implications
The proposed RCT is innovative on several fronts.
First, this will be the first sham-controlled RCT of NF with a large enough sample to detect a medium specific effect. There have been previous sham-controlled trials with too small a sample to rule out a Type II error, and there have been large studies showing a significant effect but not sham-controlled so that we cannot be sure the effect is specific rather than placebo response. This study for the first time addresses both shortcomings.
Second, the investigative team is unique for the NF field. Previous literature and conference presentations reveal considerable tension between mainstream ADHD experts and NF experts. In contrast, the planning and execution of this RCT involve mainstream ADHD scientists and RCT experts (to insure credible scientific rigor) and NF experts (to insure credible and rigorous Tx). It is important that all stakeholders have input so that the results, whatever they are, will be credible to all.
Third, a new blinding technology will be used that has been demonstrated by Andrew Hill in a non-ADHD study: Feedback for sham participants will be based on a prerecorded EEG on which the participant’s eye, muscle, and other artifacts will be overlaid so that the trainer/technician (as well as the patient) cannot discern that it is not the participant’s own EEG.
Fourth, for the first time, the sham condition will be checked for unwitting reinforcement by time marking the reinforcements on the participant’s real EEG for later inspection. This will provide a check on the inertness of the sham.
Fifth, in accordance with the emphasis on Research Domain Criteria (RDoC), the data and analyses will be included to examine TBR as a possible biomarker for Tx response that cuts across ADHD diagnostic subtypes.
Sixth, the cost-effective neuroimaging strategy, LORETA, will be used to explore effects of NF on deeper brain structures known to be involved in ADHD.
Clinical and Public Health Implications
Testing of this promising Tx in a way that is rigorous in clinical method and research design is greatly needed to see whether NF is an effective alternative Tx option for the many youth who do not respond to or refuse current evidence-based Txs and to see whether NF holds additional promise as a complimentary Tx option. If this trial demonstrates that NF has a specific effect beyond the placebo response, especially if this effect persists over time, then this evidence will significantly inform decisions about inclusion of NF in comprehensive care. If the results are negative, then consumers, insurers, practitioners, and investigators may choose to redirect their resources to other new treatments for ADHD. Although NF is initially expensive and time-consuming, it would, if proven specifically effective, have several clinical and public health advantages over widely used treatments, including behavior therapy and cognitive-behavioral therapy, which cannot clearly differentiate specific from nonspecific effects. In comparison with concerns about difficulty in measuring the fidelity of most psychosocial treatments, NF has the potential to be standardized and quantified to a high degree, leading to increased consistency in delivery. In addition, NF would have some advantage over medication if safety and enduring effects after Tx cessation are demonstrated. A positive outcome would also likely lead to increased acceptance of this intervention by professional training programs, resulting in improved and more rigorous training of NF providers.
Potential refinements
We are currently seeking funding for this RCT and welcome any suggestions to improve the scientific yield and public health value of the proposed study.
Footnotes
Author’s Note
The Collaborative Neurofeedback (NF) Group consists of the following ADHD and NF investigators and clinical trials experts (listed alphabetically): L. Eugene Arnold, MD, MEd, Ohio State University, Columbus, OH; Martijn Arns, PhD, Utrecht University and Research Institute Brainclinics, the Netherlands; Keith Conners, PhD, Duke University, Durham, NC; Roger deBeus, PhD, Skyland Behavioral Health Associates, Ashville, NC; Laurence Hirshberg, PhD, Brown University, Providence, RI; Cynthia Kerson, PhD, ISNR Research Foundation, San Rafeal, CA; Helena Kraemer, PhD, Stanford University, Palo Alto, CA; Nicholas Lofthouse, PhD, Ohio State University, Columbus, OH; Joel Lubar, PhD, University Tennessee, Knoxville, TN; Keith McBurnett, PhD, University California San Francisco, San Francisco, CA; and Vince Monastra, PhD, FPI Attention Disorders Clinic, Endicott, NY.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Arnold has had research funding from NIMH, Autism Speaks, CureMark, Forest, Lilly, and Shire; advisory board honoraria from AstraZeneca, Biomarin, Noven, Roche, Shire, and Seaside Therapeutics; and consulting honorarium from Tris Pharma, and travel support from Noven. Dr. Conners receives royalties from MHS for the Conners Scales used in the proposed study. The remaining authors have no disclosures.