
Abstract
Several longitudinal follow-up studies of childhood ADHD samples suggest that 50% to 80% of children diagnosed with ADHD continue to meet diagnostic criteria for ADHD as adolescents (Barkley, 2006; Biederman, Petty, Evans, Small, & Faraone, 2010; Sibley et al., 2012). Psychostimulant medication is a routine part of the treatment regimen for children and adolescents diagnosed with ADHD, and hundreds of studies establish the efficacy of stimulant medications in children (Greenhill & Ford, 2002). However, the effects of stimulant medication on adolescents with ADHD remains understudied (American Academy of Pediatrics [AAP], 2011). A handful of studies suggest that these medications also improve the behavior and academic performance of adolescents with ADHD (Berek et al., 2011; Evans et al., 2001; Findling et al., 2011; Smith et al., 1998; Spencer et al., 2006). However, less is known about the way in which adolescents perceive medication effects and the resulting impact of stimulant medication on their cognitive/motivational states.
Children with ADHD show difficulties perceiving the physiological effects of stimulant medication. For example, in an early double-blind study, children were unable to differentiate administered stimulant medication from placebo (Dalby, Kapellus, Swanson, Kinsbourne, & Roberts, 1978). In a more recent investigation, children accurately guessed that they had received a placebo pill only 49% of the time, and reported that they thought they received placebo on approximately one third of the days they received active medication (Pelham, unpublished data). Some argue that because the cognition of adolescents is better developed (Keating, 2004), older youth may perceive medication effects with greater accuracy than children. Martin, Guenthner, Bingcang, Rayens, and Kelly (2007) offer some evidence that adolescents with ADHD can reliably recognize when they have taken active stimulant medication versus placebo. However, these adolescents were unable to detect the effects of medication versus placebo (e.g., the ability to concentrate, activity level, mood changes). Thus, adolescents with ADHD may be aware of some physiological properties of medication (e.g., side effects), but not others.
Beyond accurate detection of medication status, there are also questions about whether adolescents with ADHD possess medication expectancies that lead to stable attributions about the effect of medication on their performance. Children with ADHD do not appear to make such attributions. For example, in a series of balanced-placebo design studies, Pelham and colleagues demonstrated that children’s behavior and task performance do not vary as a function of medication expectancy (i.e., whether they believe they received medication or placebo) but as a function of active medication status (Pelham, Hoza, Kipp, Gnagy, & Trane, 1997; Pelham et al., 2002; Pelham, Waschbusch, Hoza, Pillow, & Gnagy, 2001). Pelham and colleagues (Pelham et al., 2002; Pelham, Murphy, et al., 1992) also found that regardless of the medication condition, boys selected their own efforts, not medication, as the explanation for their behavior on good days in a summer treatment program. On their bad days, boys blamed external factors such as task difficulty for their behavior (Pelham et al., 2002; Pelham, Murphy, et al., 1992). Finally, a series of laboratory studies using a learned-helplessness paradigm (Carlson, Pelham, Milich, & Hoza, 1993; Milich, Carlson, Pelham, & Licht, 1991) showed that medication-produced success may actually lead children to develop the expectancy that they are capable of good performance.
Although children with ADHD do not display significant attributions about the impact of medication on their performance, adolescents may do so. First, it is possible that developing cognitive capabilities might allow adolescents to connect their medication status with their task performance. Furthermore, over time, sustained stimulant medication use might lead individuals to learn that their performance outcomes are relatively dependent on medication status (e.g., Whalen & Henker, 1976). Adolescents tend to have more years of experience with stimulant medication than children, so medication-related performance attributions should be more pronounced.
One study suggested that, like children, adolescents with ADHD do not directly attribute performance to medication status (Ohan & Johnston, 1999). In an analogue task, adolescents with ADHD were instructed to imagine themselves in four scenarios (medication status crossed with good vs. bad behavior) and rate attributions for performance in these scenarios. Adolescents with ADHD were much more likely to attribute their performance to stable traits and self-control rather than medication status. However, adolescents perceived more self-control in medication scenarios. Therefore, it is possible that although adolescents do not make direct attributions about the pill, they still possess expectancies about its therapeutic effects. These findings warrant further investigation in a non-analogue study.
The current study seeks to better understand how adolescents with ADHD perceive the effects of stimulant medication. First, we examined whether adolescents could accurately detect whether they had taken active medication versus placebo. We hypothesized that adolescents would be able to accurately detect when they were medicated, particularly at higher doses. Second, we examined whether daily performance and medication status during an intensive Summer Treatment Program for adolescents (STP-A) predicted category of performance attribution (e.g., I had a good day because of . . . the pill, being treated fairly, effort). As in the Ohan study, we also hypothesized that adolescents would not directly attribute performance to medication, but would be more likely to attribute performance to effort on medication days.
Method
Participants
Participants were 46 adolescents between the ages of 12 and 17, who participated in the STP-A at a large university research center and clinic during three separate consecutive summers. In all, 41 subjects were male and five were female. A total of 85% of the participants were Caucasian. The median family income was $38,500 (range $8,300-$500,000). All participants had a diagnosis of ADHD, based on a structured parent interview consisting of the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; American Psychiatric Association [APA], 1994) symptom descriptors, and on parent and teacher ratings including the Disruptive Behavior Disorders Rating Scale (DBD; Pelham, Gnagy, Greenslade, & Milich, 1992). In addition, 50% received a diagnosis of oppositional/defiant disorder and another 17% received a diagnosis of conduct disorder. Seven of the participants (15%) had not previously received stimulant medication for treatment of ADHD; the remaining 85% had been taking stimulant medication for periods ranging from 1 to 8 years. Table 1 shows the means and standard deviations of subject characteristics.
Subject Information.

Note. ODD = oppositional/defiant disorder; CD = conduct disorder.
Wechsler Intelligence Scale for Children—Revised (Wechsler, 1974).
Goyette, Conners, and Ulrich (1978), possible scores range from 0 to 30.
Pelham, Gnagy, Greenslade, and Milich (1992), possible scores range from 0 to 3.
Procedure
All procedures were approved by the university’s Institutional Review Board. Parent consent and youth assent were obtained prior to participation in the research study.
STP-A overview
Adolescents attended the STP-A from 7:45 a.m. to 5:00 p.m., Monday through Friday, and participated in modules that were designed to approximate a secondary school setting (for full program description, see Sibley et al., 2011; that is, recreational activities, two academic learning centers, a study hall, interpersonal skills training, a business meeting, and job activities). One graduate student lead counselor and three or four undergraduate counselors supervised 9 to 12 adolescents grouped by age. A behavioral contract system was in effect throughout the day, in which adolescents earned different levels of privileges and monetary rewards for appropriate behavior and job performance. Each behavioral contract was individualized to the adolescent’s unique treatment goals. There were three different levels, with behavioral and performance requirements, and associated privileges for meeting each level were set forth in individual contracts. For an example of an individual behavior contract, see Sibley and colleagues (2011). Staff members gave immediate verbal feedback on positive and negative behaviors throughout the day, and gave detailed feedback in individual sessions following each activity. The first two weeks of the program served as a period of baseline observation and adaptation for the adolescents and staff members, and medication assessments and questionnaire procedures were conducted during the last 6 weeks of the program.
Medication procedure
Each adolescent underwent a within-subject, placebo-controlled medication assessment of methylphenidate (MPH) with 10 mg MPH, 20 mg MPH, and 30 mg MPH, administered 3 times daily. The third dose of medication was always half of the first two doses (e.g., if the first two doses were 30 mg, the third dose was 15 mg). Each adolescent received each of the four conditions on Monday to Thursday during a 6-week clinical medication assessment, with administration order randomized daily within each week. Active medication and placebo were disguised in opaque gelatin capsules and were dispensed in daily pill reminders by the university’s research pharmacy. Medication was administered at 7:45 a.m., 11:45 a.m., and 3:45 p.m.
Daily contract reports
At the end of each day, adolescents received feedback regarding the level of the contract system that they earned for that day. Behavioral criteria for meeting given levels included standardized criteria (e.g., no instances of aggression toward peers), job performance (e.g., received a score of “4” or higher from a supervisor on a standardized performance rubric), and individualized target behaviors as necessitated by an adolescent’s behavior (e.g., made at least three contributions to group discussion during the business meeting). Daily reports were reviewed with parents at the end of the day, and parents provided consequences at home when adolescents met the criteria for a given level. In most cases, the level was determined by the percentage of contract goals met (Level 1 = 90%, Level 2 = 67%, Level 3 < 67%). However, automatic demotions to the lowest privilege level occurred if any instance of the following behaviors was observed: repeated noncompliance with adult requests, leaving the activity area without permission, intentional physical aggression toward a peer or staff member, or intentional destruction of property. After receiving feedback regarding their levels, subjects made attributions for their daily performance in meeting the terms of their contracts. A “good day” was defined as being on Level 1 or improving a level from the previous day. A “bad day” was defined as being on Level 3 or decreasing a level from the previous day. For adolescents who remained on Level 2 two consecutive days, research assistants asked the adolescent to classify the day as good or bad.
Questionnaire procedures
Questionnaires were administered by research assistants who did not interact clinically with the adolescents and were uninformed of medication conditions (Pelham et al., 2002). The research assistant read the following instructions: “I am going to ask you some questions about your day. This is not a test, so there are no right or wrong answers. I just want to know how you felt about your day.” After ensuring that the adolescent understood the format of the questionnaire and the instructions, and ensuring confidentiality of responses, the research assistant administered the questionnaire.
First, participants rated on a 10-point Likert-type scale each of seven attribution categories: their ability, task difficulty, their effort, the degree to which the pill helped them, how fairly they were treated by teachers or counselors, the degree to which their having ADHD influenced their performance, and their luck. These questions asked the adolescent to rate the degree to which each of the attribution categories was responsible for his or her success or failure. The scale for these questions ranged from 1 (really true) to 10 (not true at all).
After the adolescent completed the Likert-type scale ratings, the research assistant displayed seven 4″ × 6″ cards, upon which were written explanations for the adolescent’s daily performance (e.g., “tried hard”). The subjects were asked to rank, from best reason to worst reason, each attributional dimension. The research assistant displayed the cards in random order and removed each card from the display after the adolescent chose that card.
Finally, for adolescents who attended during Years 2 and 3 (N = 36), two questions were asked that assessed the degree to which the adolescents were able to discriminate their medication status. Adolescents were asked (a) whether they thought they had received medication or placebo that day, and (b) if medication, whether they thought they had received a little medication, a medium-sized amount of medication, or a lot of medication.
Dependent Measures
Perception of medication status
For each adolescent, sensitivity and specificity of his or her perception of medication status were computed and served as dependent measures. Sensitivity is the “true-positive” rate, or the proportion of time that adolescents correctly guessed they were medicated. Specificity is the “true negative” rate, or the proportion of time that adolescents accurately guessed that they received placebo. Adolescents’ perceptions were also examined as a function of success or failure in meeting daily goals.
Attributions for performance
The questionnaires were administered a maximum of 23 days, distributed across outcome (good or bad day) conditions. The dependent measures were adolescent ratings for each of the seven attribution categories, averaged over days within each outcome condition.
Results
Medication Sensitivity and Specificity
To assess whether adolescents can accurately detect medication status, rates of sensitivity and specificity for whether or not the adolescent believed he or she received active medication were computed for each adolescent. Lambda coefficients were calculated to correct sensitivity and specificity rates for chance (Coughlin & Pickle, 1992). Sensitivity was computed overall and separately for each of the three drug conditions (i.e., 10 mg, 20 mg, 30 mg). For each adolescent, overall sensitivity (correctly guessed medication) ranged between 0 and 1 with a mean of 0.63 (SD = 0.25,λ = .38). Specificity (correctly guessed placebo) rates ranged between 0 and 1 with a mean of 0.59 (SD = 0.27,λ = .54). The mean sensitivity at the 10-mg dose was 0.54 (SD = 0.27, λ = .23), at 20 mg was 0.64 (SD = 0.30,λ = .40), and at 30 mg averaged 0.71 (SD = 0.32, λ = .52). Therefore, after correcting for chance, adolescents displayed even poorer accuracy at detecting stimulant medication status. Adolescents were more accurate at guessing medication status when they had taken a higher dose of medication, χ2(9) = 59.91, p < .001.
Sensitivity and specificity rates also differed as a function of daily performance. Table 2 shows these rates. On good days, adolescents guessed that they received medication on 43% of the placebo days, whereas on bad days, adolescents guessed that they had received placebo on 44% of the medication days. Overall, they guessed medication on 60% of good days and on 46% of bad days.
Sensitivity and Specificity Rates as a Function of Outcome.
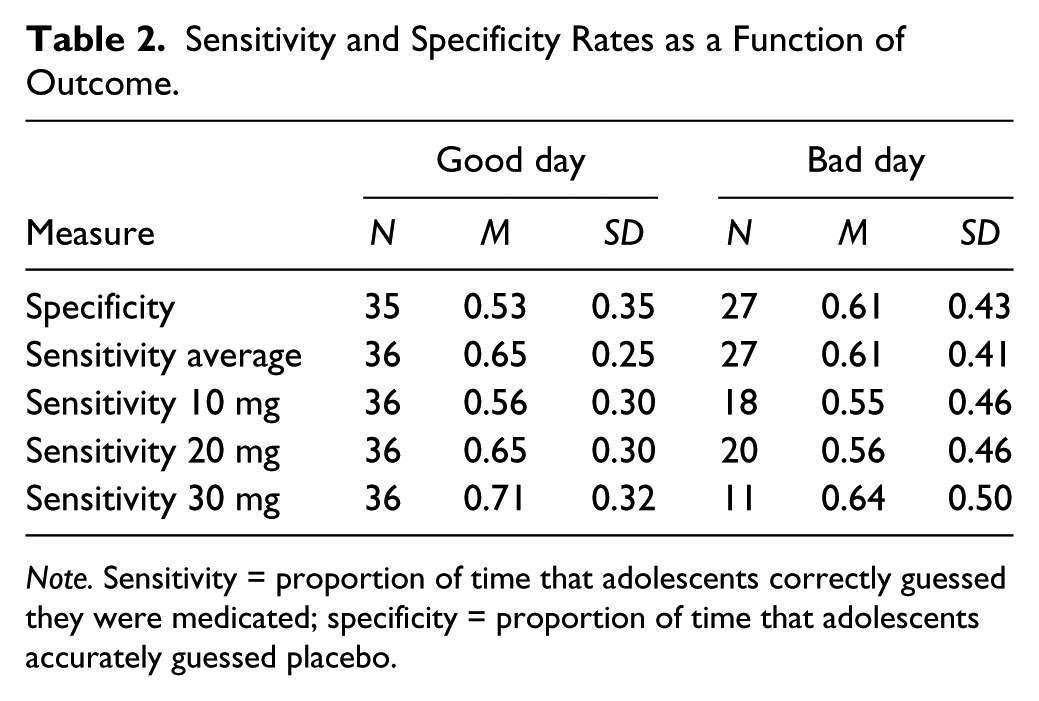
Note. Sensitivity = proportion of time that adolescents correctly guessed they were medicated; specificity = proportion of time that adolescents accurately guessed placebo.
Medication Attributions
Prior to the examination of medication attributions as a function of performance (good day vs. bad day) and medication dose (placebo, 10 mg, 20 mg, 30 mg), the relationship between these two variables was examined. Although there was a trend for participants to experience more good days on higher doses of medication (placebo = 57.1%, 10 mg = 60.3%, 20 mg = 61.0%, 30 mg = 72.1%), this effect was not statistically significant, χ2(3) = 3.83, p = .28.
Attributions for good days and bad days
To allow participants with missing data points to remain in the analyses, Linear Mixed Models were used to analyze data. Performance (good day vs. bad day) was specified as a within-subjects factor, and each of the seven attribution categories was examined as a separate dependent measure. Univariate effects suggested that on good days (see Figure 1), adolescents were more likely than on bad days to attribute performance ease of task, F(1, 81.66) = 10.12, p = .002; ability, F(1, 72.33) = 28.16, p <.001; effort, F(1, 60.99) = 187.74, p = .002; fair treatment, F(1,78.68) = 10.42, p = .002; and luck, F(1,81.66) = 10.12, p = .002. On good days, particularly strong attributions were made for effort and ability (see Figure 1). On bad days, no strong performance attributions were made in any category. On both good days and bad days, adolescents failed to attribute performance to the pill and having ADHD.

Adolescent attributions for daily success and failure during the STP-A.
Adolescents’ attributional rankings were also examined descriptively. For both good days and bad days, we examined the frequency with which each attribution category was ranked as the primary reason for one’s success. On good days, adolescents most frequently nominated effort (67.5%) as the primary reason for their success, followed by ease of the task (12%), ability (7%), luck (6%), and fairness (6%). On good days, ADHD and pill were ranked first less than 1% of the time each. On bad days, unfair treatment (36%) was chosen as the primary reason for performance. Lack of effort (17.5%), task difficulty (14%), luck (14%), and the pill (10%) were chosen less frequently. The adolescents rarely chose lack of ability (3.5%) or ADHD (5%) as reasons for their poor performance.
Attributions as a function of medication status
To allow participants with missing data points to remain in the analyses, Linear Mixed Models were used to analyze data. Medication status (placebo, 10 mg, 20 mg, 30 mg) was specified as a within-subjects factor, and each of the seven attribution categories was examined as a separate dependent measure. There were no significant univariate effects for any attribution category (p > .55), suggesting that stimulant medication did not influence adolescent performance attributions.
Discussion
The present study investigated (a) the ability of adolescents with ADHD to discern placebo from active MPH and (b) whether adolescents with ADHD possessed medication expectancies that influenced performance attributions on good and bad days. Results demonstrated that adolescents with ADHD displayed the same attributional patterns as children with ADHD (Pelham et al., 2002; Pelham, Murphy, et al., 1992). Specifically, adolescents (a) inaccurately distinguished medication from placebo on approximately 40% of days and (b) rarely attributed their good or bad days to medication status. Contrary to previous conjecture (Ohan & Johnston, 1999), our study revealed no evidence that these attributions are stronger in adolescents than in children. Each finding is discussed below.
Overall, adolescents guessed that they were medicated 58% of the time and guessed that they were unmedicated 42% of the time. Considering that they were actually medicated on 75% of the days and received placebo only 25% of the time, these rates indicate that they did not reliably detect medication status. Sensitivity rates were particularly poor after correcting for chance agreement (λ = .23-.52). Although accuracy improved at higher doses, even at the highest dose, the adolescents continued to guess placebo on 29% of their medicated days. These results suggest that adolescents possessed poor physiological awareness of the medication, especially at the lower doses. These data are consistent with previous work in children (Pelham et al., 2002; Pelham, Murphy, et al., 1992) and adolescents (Martin et al., 2007).
The adolescents in this study displayed an attributional pattern that was similar to that of younger children in the same setting (Pelham et al., 2002; Pelham, Murphy, et al., 1992). Namely, they were most likely to attribute performance to effort and ability on good days. On bad days, attributions were much weaker and less consistent; however, performance rankings suggested that adolescents were most likely to blame external factors, such as unfair treatment, for poor performance. This attributional pattern is consistent with a self-serving bias that is widely reported in the general population (e.g., Miller & Ross, 1975). However, these internal attributions may be accurate, as it is likely that occasions of increased adolescent effort ultimately led to good days. With regard to medication, adolescents were unlikely to cite the pill as a reason for their daily performance during the STP-A. This finding was slightly surprising, as one would expect that cognitive maturation and a longer lifetime history of medication use (up to 8 years) could strengthen medication attributions. These results suggest that adolescents with ADHD do not believe that their medication significantly affects their performance. This finding is striking because the same sample of adolescents showed a strong response to medication on behavioral and academic measures (Evans et al., 2001; Smith et al., 1998).
Although this sample of adolescents did not make direct causal medication attributions (e.g., “I did well because I took the pill today”), it appears that some adolescents still possessed medication expectancies. For example, on good days, adolescents said they were medicated on 43% of the placebo days, and on bad days, they said that they received placebo on 44% of the medicated days. Thus, adolescents were slightly more likely to guess that they were medicated on good days, regardless of whether they actually received medication or placebo. In addition, on bad days, the pill was chosen as the primary reason for performance on 10% of occasions. Thus, some adolescents appeared to believe that failing to take active medication led to poor performance. Contrary to the findings of Ohan and Johnston (1999), however, medication status had no effect on the strength of attributions. Thus, adolescents did not appear to experience a greater sense of control over their behavior on medication days.
Our finding that adolescents do not believe medication impacts their performance is consistent with data on medication desistence in adolescents. It is widely known that adolescents discontinue stimulant medication use at high rates, such that by age 18, less than 10% of youth who were prescribed stimulant medication continue to take it (McCarthy et al., 2009; Molina et al., 2009). Probing the reasons for desistance, Kuriyan et al. (2013) found that the primary reasons teens cited for stimulant discontinuation were, “I got better and didn’t need it” (76.2%), “I didn’t want to take it” (62.0%), and “My medication didn’t help me with my problems” (58.9%). Therefore, the attributional pattern found in adolescents with ADHD may relate to their unwillingness to take stimulant medication.
It may also be the case that poor self-insight prevented adolescents from perceiving their impairments and the subsequent effect of medication on their functioning. Like children with ADHD, adolescents tend to under-report their symptoms and impairment (Fischer, Barkley, Fletcher, & Smallish, 1993; Sibley et al., 2012). Some argue that inaccurate self-report by individuals with ADHD stems from a characteristic self-perception bias (Hoza, Pelham, Dobbs, Owens, & Pillow, 2002). This hypothesis is consistent with the adolescents’ tendency to blame external factors for their failure and internal factors for success (see Figure 1). This study suggests that medication-related self-perception deficits are also present in adolescence.
This study should be considered in the context of its limitations. First, our sample primarily was composed of White, middle-class males with a history of stimulant medication use, and our study was conducted in a treatment setting. Thus, some findings may not generalize to other populations or settings. This sample was also primarily composed of young adolescents (age M = 12.5), and results may be different for older adolescents. It should also be noted that the adolescents had very few failure days. As a function of the ongoing behavioral treatment program, the group average was approximately 17 good days and only 6 bad days during the 23-day assessment. Five subjects never experienced failure on their daily contracts, and 50% of the adolescents had fewer than 5 negative days. The results of the attributions for failure are therefore based on few data points, and further research may be needed to clarify adolescents’ attributions for failure. Given the small number of subjects in this study, we were unable to investigate individual differences. For example, factors such as gender, attributional style, response to medication, ADHD symptom profile, or diagnostic comorbidity could influence subjects’ attributions. In addition, some participants had no prior exposure to stimulants for treatment of ADHD, limiting their ability to develop medication expectancies from personal experience. Unfortunately, we were unable to look at the relationship between medication attributions and duration of stimulant treatment because we did not collect lifetime history of stimulant medication use from participants. Further research is needed to investigate individual factors that may affect the attributions of adolescents and adults with ADHD, and to compare them with individuals without ADHD.
This study possesses important research and clinical implications. First, the inability of adolescents to reliably discern active medication from placebo validates that adolescents are typically blind to their medication status in placebo-controlled studies. Second, the inaccurate medication expectancies identified in this study provide further support for the hypothesis that some adolescents may refuse to take effective medication because they incorrectly perceive it as unhelpful. Given the poor outcomes experienced by adolescents with ADHD and the limited long-term benefit of childhood stimulant medication, continued treatment during the teen years is essential (Molina et al., 2009). Further work is needed to investigate the relationship between medication expectancies and desistance. If medication expectancies are implicated in desistance, an intervention designed to improve the accuracy of self-perception with respect to medication response could be one way to improve the adherence and outcomes of adolescents with ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Institute of Mental Health (MH45576). Dr. Pelham has also been supported by grants from NIMH (MH47390, MH48157, MH50467, MH53554, MH62946, MH069614), NIAAA (AA06267, AA11873), NIDA (DA05605, DA12414), and the Institute of Education Sciences (LO3000665A, R324B060045).