
Abstract
Objective:
Asian American and Pacific Islander (AAPI) students with ADHD may face increased risk for college maladjustment due to cultural factors and a tendency to delay treatment. This is the first study to examine ADHD prevalence, ADHD-related impairments and comorbidities, and ADHD treatment utilization in AAPI college students.
Method:
AAPI, White, Hispanic, and Black undergraduates (n = 258,005) from the American College Health Association—National College Health Assessment II survey were included in the study.
Results:
AAPI students had lower ADHD prevalence rates than White and Black students, and similar prevalence to Hispanic students. AAPI students with ADHD had significantly higher risk for comorbidities and social and academic impairments, compared to White students with ADHD. Approximately half of AAPI students with ADHD did not utilize treatment despite experiencing psychiatric comorbidities and functional impairments.
Conclusion:
AAPI college students with ADHD are underutilizing treatment despite elevated psychiatric comorbidities and functional impairment.
Asian Americans and Pacific Islanders (AAPIs) are the fastest growing racial/ethnic minority group in the U.S. Over the past two decades the AAPI population has increased by 81%, reaching 18.9 million people in 2019 (Budiman & Ruiz, 2021a). Currently, AAPI students comprise 7.7% of the undergraduate population in the U.S. (U.S. Department of Education, 2021). ADHD is an increasingly prevalent condition in college students (11.6%; American College Health Association, 2020) and is associated with psychological distress, academic and social impairment, and emotional difficulties that each independently predict lower probability of college success (Green & Rabiner, 2012). While both populations are increasing, ADHD prevalence rates, associated functional impairments, and ADHD treatment utilization patterns have never been examined among AAPI college students.
Risk for College Maladjustment
Although never investigated, AAPI college students with ADHD may be at elevated risk for college maladjustment compared to other racial groups for two reasons. First, cultural risk factors such as acculturative stress, racial discrimination, and elevated expectations of scholastic success are experienced by the AAPI population and are each associated with greater depressive symptoms and psychological maladjustment among AAPIs (Cornejo et al., 2020; Garcia et al., 2019). Second, more than half of first-year college students with ADHD have co-occurring depression or anxiety, compared to only 11.2% of those without ADHD (Anastopoulos et al., 2018). Thus, the presence of ADHD may amplify the effects of cultural risk factors among AAPI students with ADHD. A variety of additional internal and external barriers, that are further explained in the next section, can reduce the likelihood of AAPI students receiving ADHD diagnoses and treatment. Thus, this population (AAPI+ADHD) seems especially important to better understand.
Shared cultural values, such as family recognition through achievement, are salient among AAPI individuals and especially emphasize academic success (B. S. K. Kim et al., 2001; Uehara et al., 2018). Not surprisingly, AAPI college students are likely to prioritize educational outcomes and face greater academic pressure and worry more about academic performance than White students (Saw et al., 2013; Uehara et al., 2018). On the other hand, college students with ADHD report significantly more academic concerns, are less confident about their academic abilities, and obtain GPAs 0.5 to 1 standard deviation lower than those without ADHD (DuPaul et al., 2021; Green & Rabiner, 2012). Thus, AAPI students with ADHD may experience significant difficulty meeting these elevated academic expectations.
This confluence of (a) greater parental educational pressure in AAPI college students and cultural risk factors such as acculturative stress and racial discrimination, and (b) the negative impact of ADHD on functioning across multiple domains may make AAPI college students with ADHD especially vulnerable to college maladjustment compared to students with ADHD of other racial/ethnic groups. At this time, however, no research has investigated this topic.
Treatment Barriers
These diatheses are particularly concerning given that AAPIs delay psychiatric treatment for as long as possible, subsequently presenting to intake with the highest levels of distress compared to other racial groups (Chen, 2005). Moreover, Asian/Asian American college students have the lowest mental health treatment utilization, with approximately 80% of psychiatric cases left untreated (Lipson et al., 2018). Compared to White college students, Asian/Asian Americans have 64% lower odds of medication use and 51% lower odds of psychotherapy for any mental health disorder (Lipson et al., 2018). Historical and contemporary racialization of Asian American communities has contributed to high mental health stigma and stereotypes such as the model minority myth, leading to negative attitudes, feelings of shame, and avoidance of professional mental health services with a Western cultural focus (Kim & Zane, 2016; Okazaki et al., 2014). Stigma and self-concealment, or the tendency to hide distressing and potentially embarrassing personal information, are both associated with lower use of mental health treatment among AAPIs (Masuda & Boone, 2011). Of note, self-concealment among AAPIs also relates to emotional control and maintenance of family or community reputation (Masuda & Boone, 2011), either of which may reduce engagement with mental health treatment. Additionally, cultural mistrust, or suspicion of mainstream White institutions and health care systems, contributes to negative help-seeking attitudes among Asians living in Western cultures (David, 2010; Soorkia et al., 2011). Cultural mistrust also mediates the detrimental relationship between racial discrimination and well-being among Asian Americans (P. Y. Kim et al., 2017). These unique cultural and systemic factors may decrease the likelihood of ADHD treatment among AAPIs and increase impairment related to untreated ADHD.
Therefore, while never investigated, AAPI college students with ADHD may be at greater risk for negative outcomes associated with untreated ADHD (Shaw et al., 2012) compared to college students of other ethnicities. This is unfortunate as evidence-based interventions (e.g., stimulant medication, cognitive behavioral therapy, and organizational skills training) exist for college students with ADHD (for a review, see Fleming & McMahon, 2012).
Aims and Hypotheses
In short, the confluence of ADHD and external pressure to succeed academically may make AAPI college students especially vulnerable to maladjustment during college, yet AAPIs with ADHD are also less likely to utilize treatment for such maladjustment due to barriers such as mental health stigma, mistrust of healthcare systems due to racial discrimination, and culturally significant values (e.g., self-concealment). Despite this apparent “perfect storm,” no research to date has examined this clinically important topic. This study aims to fill the existing gap in the college student and ADHD literatures by examining ADHD prevalence rates, associated functional impairments, and ADHD treatment utilization patterns in AAPI college students. Based upon pediatric data, AAPI college students are hypothesized to demonstrate the lowest prevalence of ADHD diagnoses among racial groups (i.e., Black, White, Hispanic; Wong & Landes, 2022) yet endorse similar levels of ADHD-associated impairment (e.g., academic and social). AAPI students are also hypothesized to be the least likely to utilize psychotherapy or pharmaceutical treatment for ADHD compared to all other racial/ethnic groups (Lipson et al., 2018). Across all racial/ethnic groups, college students with ADHD are expected to report more functional impairment than students without ADHD (Green & Rabiner, 2012).
Methods
A secondary data analysis of the American College Health Association—National College Health Assessment (ACHA-NCHA) II Fall 2015 to Spring 2019 (American College Health Association, n.d.) was conducted. Universities conducted the ACHA-NCHA II on individual campuses in accordance with their institutional policies and distributed surveys through in-person campus sampling or online. Colleges and universities randomly selected students or surveyed students in randomly selected classrooms. Each participating campus maintained participant confidentiality and obtained approval from their respective institutional review boards. Importantly, the ACHA-NCHA II is considered a valid measure for deriving prevalence estimates and for examining health behaviors, diagnoses, and group differences among college students (American College Health Association, 2013; Kerr et al., 2021). The data set has no identifying information; thus, this study is IRB-exempt.
The current study used cross-sectional survey data from 426,425 undergraduate students from U.S. schools participating in Fall 2015 (40 schools), Spring 2016 (137 schools), Fall 2016 (51 schools), Spring 2017 (92 schools), Fall 2017 (52 schools), Spring 2018 (140 schools), Fall 2018 (40 schools), and Spring 2019 (98 schools). Surveys were available continuously throughout the entire academic semester. Students between the ages of 18 and 24 years old, who identified as being of non-Hispanic White, AAPI, Hispanic, or Latino/a (hereafter shortened to “Hispanic”), or Black race or ethnicity and were enrolled on a full- or part-time status were included. As the vast majority of undergraduate college students are between the ages of 18 and 24 (National Center for Education Statistics, 2022), students outside the age group were excluded. Students without American citizenship were also excluded as international students can face additional stressors that negatively impact their mental well-being, face greater mental health stigma, and are less likely to seek mental health services compared to Asian Americans (Maeshima & Parent, 2022).
Participants
The final sample for the current analyses consisted of 258,005 students (61% of the original sample). The most common reasons that participants did not meet eligibility criteria were age older than 24 (n = 98,091), graduate students or those not seeking a degree (n = 70,356), biracial or multiracial ethnicity or ethnicity other than AAPI, White, Hispanic, or Black (n = 58,913), and international students (n = 31,755). In the final sample, most students (95.7%, n = 246,815) were enrolled in a 4-year college or university (compared to 2-year institutions). The average age of participants was 20 years (SD = 1.52) with more female (70.3%, n = 181,249) than male participants. Slightly more than half of the participants were first- or second-year students (52.9%, n = 136,550) and most were enrolled full-time (96%, n = 247,636). Racial/ethnic distribution for the current analyses was 72% White (n = 185,638), 12.3% Hispanic (n = 31,745), 11% AAPI (n = 28,260), and 4.8% Black (n = 12,362). Demographic data with a breakdown between ethnicities are included in Table 1.
Sample Demographics, by Ethnicity.
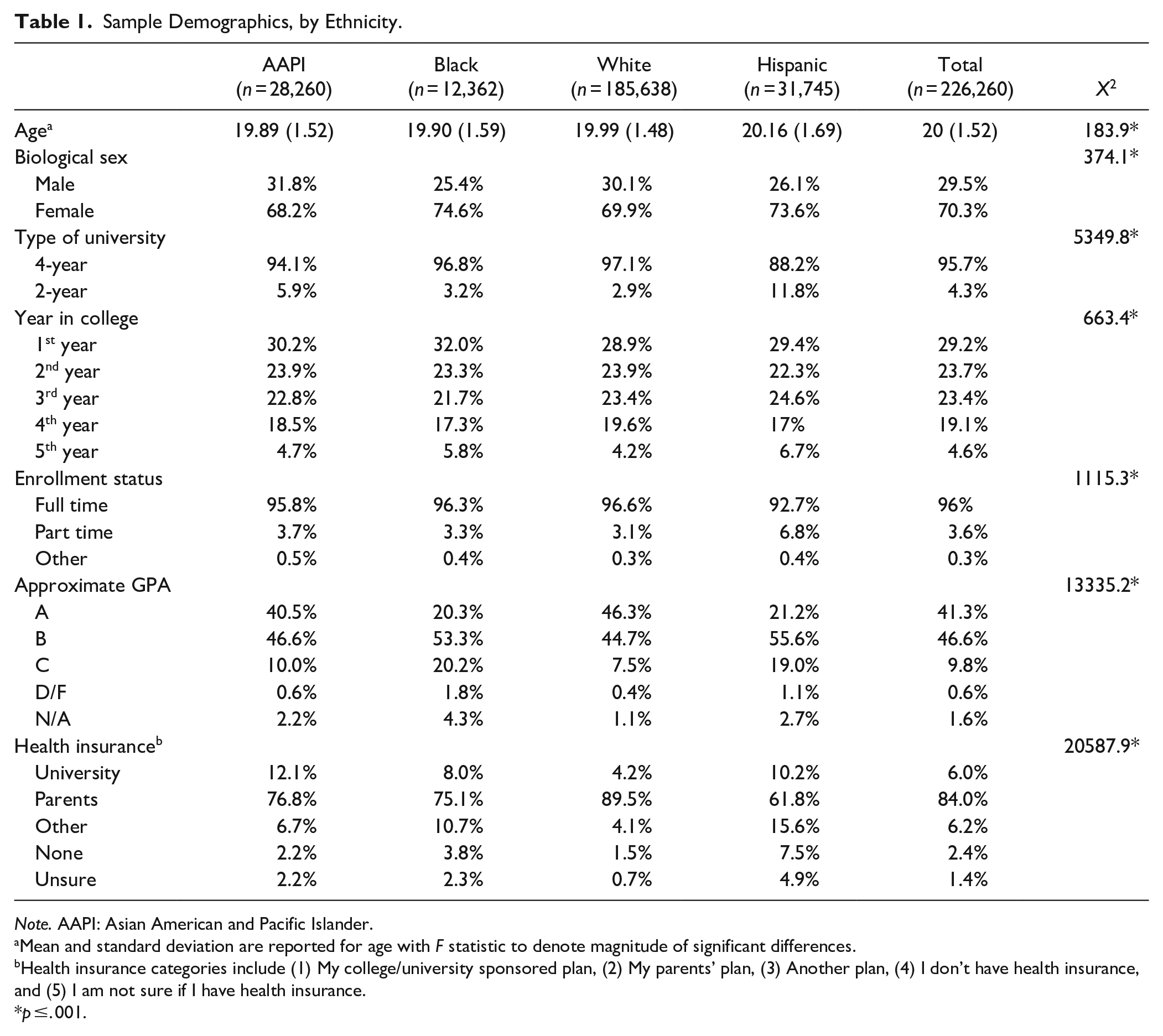
Note. AAPI: Asian American and Pacific Islander.
Mean and standard deviation are reported for age with F statistic to denote magnitude of significant differences.
Health insurance categories include (1) My college/university sponsored plan, (2) My parents’ plan, (3) Another plan, (4) I don’t have health insurance, and (5) I am not sure if I have health insurance.
p ≤. 001.
Measures
The ACHA–NCHA II consisted of 66 items related to health behaviors and outcomes. All responses were self-reported by the participants. For this study, a subset of the items was used as the three primary dependent variables, described below.
Current Prevalence of ADHD
One item asked, “Do you have any of the following?” with a list that included ADHD, chronic illness, deaf/hard of hearing, learning disability, mobility/dexterity disability, partially sighted/blind, psychiatric condition, speech or language disorder, and other disability. Response options for each condition were “yes” and “no.” Individuals who marked “yes” for ADHD were used to determine current prevalence of the disorder.
Past Year ADHD-Related Functional Impairment
Four items assessing functional impairments related to ADHD were included. The first item assessed psychiatric comorbidities with the question “Within the last 12 months, have you been diagnosed or treated by a professional for depression or anxiety?” Response options for each condition were “no,” “yes, diagnosed but not treated,” “yes, treated with medication,” “yes, treated with psychotherapy,” “yes, treated with medication and psychotherapy,” or “yes, other treatment.” Following a precedent in the literature (Oswalt et al., 2020), responses for this item were collapsed into dichotomous categories of “not diagnosed or treated within the last 12 months” or “diagnosed or treated in the last 12 months.”
The second item assessed functional impairments with the question “Within the last 12 months, have any of the following been traumatic or very difficult for you to handle. . .” with a list that included academics, intimate relationships, and other social relationships. Response options for each domain were “no” and “yes.” Intimate relationships and other social relationships were combined into an omnibus “social impairment” variable as they were highly correlated, χ2(1) = 31,177.30, Cramer’s V = 0.37, p < .001. Students who reported no impairment in intimate and other social relationships were coded as 0, students who reported at least one type of social impairment were coded as 1, and students who reported both types of social impairment were coded as 2. Thus, two variables of the presence of academic (a binary variable) and social (an ordinal variable) impairments were created from this item.
The third item assessed severity of academic impairment with the question, “Within the last 12 months, has ADHD affected your academic performance?” Respondents were asked to select the most serious outcome on 4-point Likert scale (1 = “I have experienced this issue, but my academics have not been affected,” 2 = “Received a lower grade on an exam or important project,” 3 = “Received a lower grade in the course,” and 4 = “Received an incomplete or dropped the course”). Additional response options of “not applicable” and “significant disruption to thesis, dissertation, research or practicum work” were excluded as they included those without ADHD or were not relevant to the undergraduate curriculum. This variable was treated as an ordinal variable with higher scores indicating more severe academic impairment.
The fourth item assessed stress levels by asking “Within the last 12 months, how would you rate the overall level of stress you have experienced?” Response options on a 5-point Likert scale ranged from “no stress” to “tremendous stress.” This variable was treated as an ordinal variable with higher values indicating higher reported stress levels.
Past Year ADHD Treatment Utilization
One item was used to examine treatment utilization, “Within the last 12 months, have you been diagnosed or treated by a professional for . . . ADHD?” Response options were “no,” “yes, diagnosed but not treated,” “yes, treated with medication,” “yes, treated with psychotherapy,” or “yes, treated with medication and psychotherapy.” Response options were not dichotomized for analysis.
Data Analysis
SPSS version 26 was used for all analyses. A chi-square analysis was conducted to determine if prevalence of ADHD differed between ethnic groups, stratified by biological sex. Binary logistic regressions for binary outcomes (e.g., presence of comorbidities) or ordinal logistic regressions for ordinal outcomes (e.g., three-level social impairment) were conducted to test for main effects of ethnicity and ADHD diagnoses and interaction of ethnicity with ADHD diagnosis. AAPI students served as the reference group in regression analyses. A multinomial regression was used to examine differences in type of treatment utilization for individuals with ADHD. Significance was considered at p ≤ .001 for all analyses, and effect size measures (e.g., 95% confidence intervals of odds ratio for individual variables and pseudo R2 for the entire model) were used to interpret results to reduce Type I errors (Khalilzadeh & Tasci, 2017). Missing data was excluded listwise.
Results
Current Prevalence of ADHD
AAPI college students had lower prevalence of ADHD (3.8%) compared to White (9.0%) and Black (4.5%) college students, and similar ADHD prevalence compared to Hispanic students (3.6%), χ2(2) = 538.08, Cramer’s V = 0.046, p < .001. The prevalence of ADHD among female students mimicked the same pattern across all racial groups. Female Hispanic students were least likely to be diagnosed with ADHD, followed by AAPI, Black and White women. However, among males, AAPI students were the least likely to be diagnosed with ADHD, followed by Hispanic, Black, and White students. See Table 2 for prevalence results.
Prevalence of ADHD, by Ethnicity and Biological Sex.
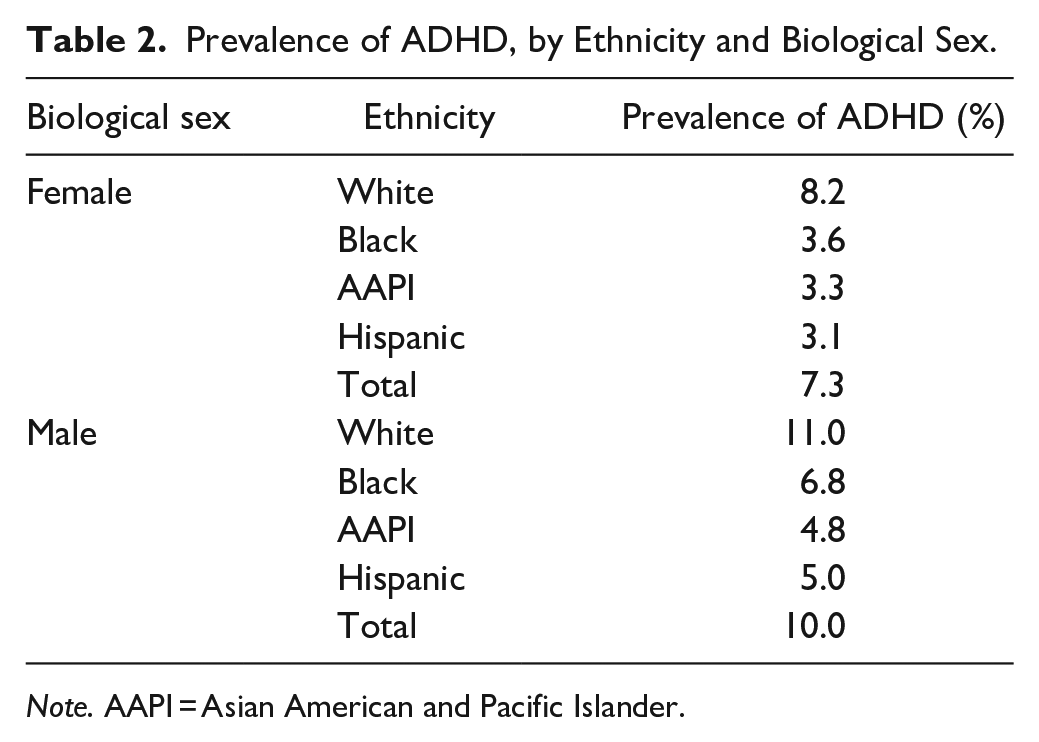
Note. AAPI = Asian American and Pacific Islander.
Functional Impairments
Comorbid Anxiety and Depression Diagnoses
As shown in Table 3, anxiety (χ2(9) = 18,461, p < .001) and depression (χ2(9) = 11,565, p < .001) diagnoses yielded similar results. Significant interactions between White students (as compared to AAPI students) and ADHD diagnosis was found for both disorders. Specifically, when students had ADHD, White students were significantly less likely (p < .001) to have comorbid anxiety (OR = 0.57, 95%CI [0.50, 0.66]) and depression (OR = 0.58, 95%CI [0.51, 0.67]) compared to AAPI students. However, there was no significant interaction between Black students and ADHD status, or Hispanic students and ADHD status emerged. This indicates that the association of ADHD diagnosis with anxiety and depression comorbidity did not differ between Black, Hispanic, and AAPI students with ADHD. Significant and positive main effects of race indicated that Hispanic and White students were more likely to be diagnosed with anxiety compared to AAPI students, regardless of ADHD diagnosis. There were no significant differences in likelihood of depression diagnoses among racial groups Finally, regardless of race, individuals with ADHD had five times higher risk of being diagnosed with anxiety (OR = 5.31, 95% CI [4.65, 6.07]) and depression (OR = 5.98, 95% CI [4.35, 5.71]), compared to those without ADHD.
Regression Results.
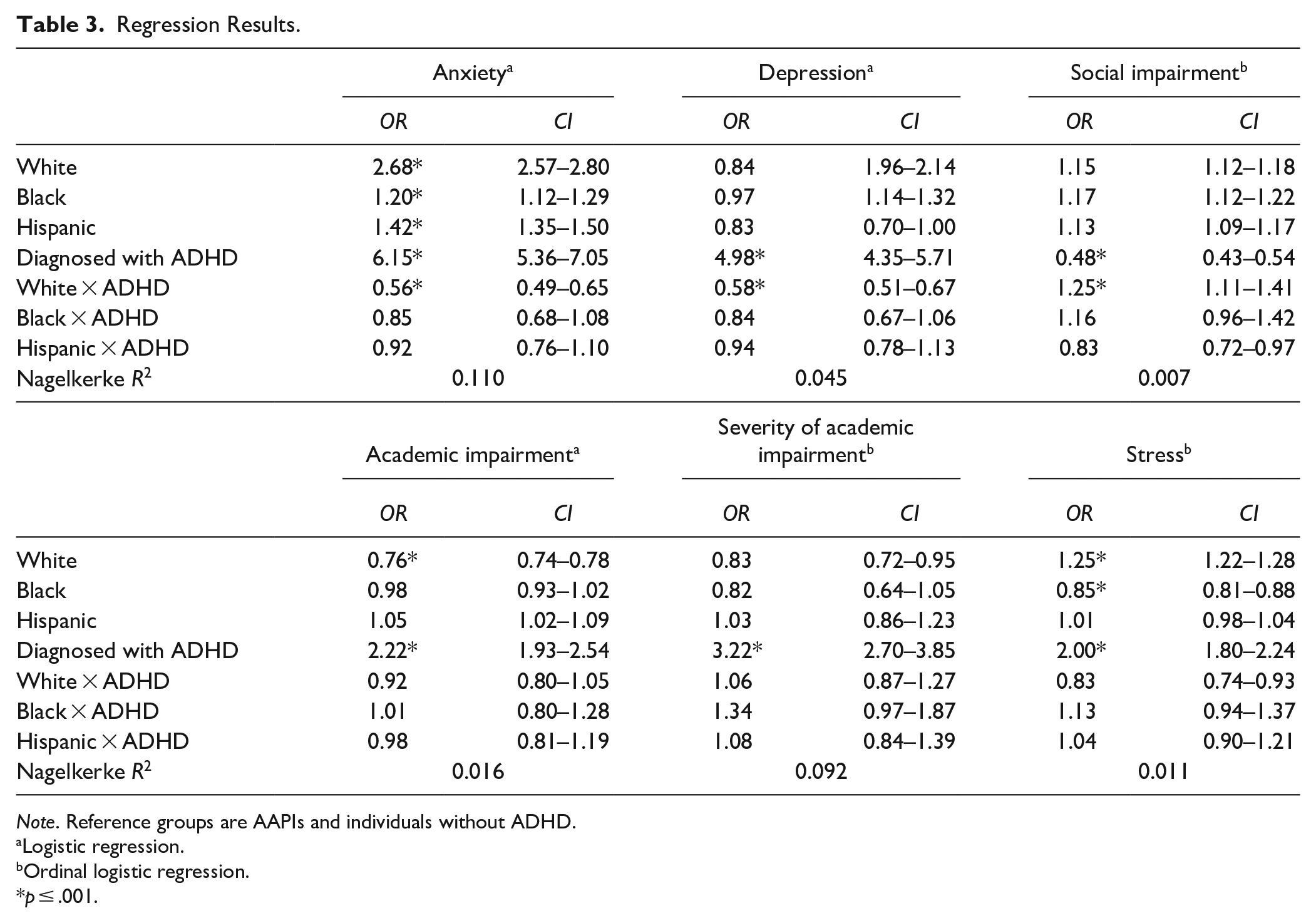
Note. Reference groups are AAPIs and individuals without ADHD.
Logistic regression.
Ordinal logistic regression.
p ≤ .001.
Academic Impairment
The overall logistic regression model was statistically significant, χ2(7) = 3,056, p < .001. Main effects of race indicated that White students were significantly less likely to report academic impairment compared to AAPI students (OR = 0.76, 95% CI [0.74, 0.78]). No differences emerged between Black and AAPI students or Black and White students. Individuals with ADHD were at greater than two-fold increased risk to report academic impairment compared to those without ADHD (OR = 2.22, 95% CI [1.93, 2.54]) and were significantly more likely to report severe academic impairment (i.e., receiving incomplete for a course; OR = 3.22, 95% CI [2.70, 3.85]). Interaction terms were nonsignificant; severity of academic impairment among individuals with ADHD did not vary as a function of race.
Social Impairment
A statistically significant ordinal logistic regression model emerged, χ2(7) = 1561, p < .001. A significant interaction demonstrated that AAPI students with ADHD were more likely to report high levels of social impairment compared to White students with ADHD. Main effects indicated that individuals with ADHD were significantly more likely to experience greater social impairment compared to those without ADHD (OR = 2.03, 95% CI [1.82, 2.27]), regardless of race. AAPI students were less likely to experience social impairment compared to all other racial groups, regardless of ADHD status.
Stress
Main effects show significant effects of ADHD status; students with ADHD reported two-fold increased risk of high stress levels compared to students without ADHD (OR = 2.00, 95% CI [1.78, 2.24]). White students had higher likelihood of reporting greater stress levels compared to AAPI students (OR = 1.25, 95% CI [1.22, 1.28]), and AAPI students were more likely to report greater stress than Black students (OR = 0.85, 95% CI [0.81, 0.88]). Results for Hispanic students were not significant. Interaction effects were not significant; stress levels among individuals with ADHD did not vary as a function of race.
Treatment Utilization
The multinomial regression was significant, χ2(28) = 71,714, p < .001. Compared to AAPI students, Black students were significantly more likely to be diagnosed, but not treated, regardless of ADHD status (OR = 1.87, 95% CI [1.36, 2.56]). Interaction effects demonstrated that White students with ADHD were significantly more likely to be treated with medication compared to AAPI students with ADHD. No other main or interaction effects were significant. Frequency analyses revealed that approximately half of AAPI and Hispanic students with ADHD did not receive any treatment. Similarly, 40% of Black students and 30% of White students with ADHD did not receive treatment for ADHD. Across all racial groups, students were most likely to opt for medication treatment, followed by a combination of psychotherapy and medication, and were least likely to opt for psychotherapy only. Finally, a reasonable number of participants (16%–21%) across ethnic groups were diagnosed with ADHD in the past year. See Table 4 for full results.
Types of Treatment Utilization in the Past 12 Months Among College Students With ADHD.

Note. AAPI = Asian American and Pacific Islander.
Discussion
This study expands on previous research regarding racial-ethnic disparities in ADHD prevalence rates and treatment utilization in children and is the first to examine ADHD in AAPI college students. The hypotheses posited that AAPI students with ADHD are not utilizing treatment despite being at risk for maladjustment during college and were supported by the results from this large, nationally representative dataset. AAPI students had lower prevalence of ADHD compared to White and Black students, and similar prevalence rates to Hispanic students. Compared to White students, AAPI students reported greater social and academic impairment and greater psychological distress. However, AAPI students with ADHD were less likely to receive treatment compared to White students with ADHD. Disparities between reported impairment and treatment received were similar for Black, Hispanic, and AAPI students. Main effects demonstrated that college students with ADHD reported more functional impairment and comorbid diagnoses than students without ADHD, regardless of race. This finding is in line with extant literature (Nelson & Liebel, 2018) and support the external validity of these data.
Our findings are also consistent with studies in children, demonstrating lower prevalence of ADHD among Asian Americans compared to White and Black samples (Wong & Landes, 2022). However, previous studies have demonstrated higher ADHD prevalence among Hispanic children compared to Asian American children (Wong & Landes, 2022); our study results are inconsistent with this literature. This difference may be due to the college sample used in the current study and because the current sample combines Asian American and Pacific Islander groups.
AAPI college students with ADHD reported higher levels of academic and social impairment and were at greater risk for a comorbid anxiety and depression diagnosis compared to White students. One possible reason for these outcomes may be that AAPIs delay psychiatric treatment for as long as possible (Chen, 2005). Alternatively, increased parental academic pressures for AAPI college students (Chao & Tseng, 2002; Uehara et al., 2018), combined with negative impacts of untreated ADHD (Green & Rabiner, 2012) may contribute to higher risk for functional impairments. Future research should consider how AAPI parental socialization factors may influence risk for negative functional outcomes in college students with ADHD.
This study’s results demonstrate that within the ethnic groups, AAPIs are most likely to opt for medication. The preference for medication treatment is consistent with overall patterns of ADHD treatment among college students in this sample and with ADHD treatment guidelines that recommend medication as the first line of treatment (De Crescenzo et al., 2017). On the other hand, lack of available culturally sensitive therapy may deter AAPI students from seeking psychotherapeutic treatment. Stigma, self-concealment, risk of loss of face, and cultural mistrust are all associated with lower use of psychotherapy among AAPIs (Masuda & Boone, 2011).
Similar disparities between need for and actual treatment received among Black, Hispanic, and AAPI students may reflect larger systemic barriers responsible for health disparities in the United States. While 42.5% of White students received medicine for ADHD, only 25% to 29% of students from other racial/ethnic groups received medication. This trend supports extant literature demonstrating undertreatment of ADHD in minoritized groups that has been linked to racial (and gender) bias in clinical care (Abdelnour et al., 2022). Such biases may also be associated with a cultural mistrust of White healthcare institutions, creating negative attitudes toward culturally incompetent care (Castro-Ramirez et al., 2021; P. Y. Kim et al., 2017).
Clinical Implications
AAPI and Hispanic college students with ADHD are at-risk for college maladjustment yet are not seeking help. Notably, approximately half of AAPI and Hispanic students who are diagnosed with ADHD did not receive any treatment and may be a prime target for interventions to increase treatment engagement. Both psychotropic and psychotherapeutic treatment modalities may be appropriate for AAPI college students with ADHD. Thus, practitioners may consider providing psychoeducation about both treatment options while highlighting psychotropic treatment for AAPI patients to increase treatment engagement. Psychoeducation about ADHD and treatment options may also be beneficial in high school to aid the transition into college (Canu et al., 2021). Similarly, Hispanic students may also benefit from psychoeducation about both treatment options, while Black students may benefit from prioritizing medications to promote treatment engagement.
For students who opt for or who may benefit from concurrent psychotherapy, addressing stigma at the outset of counseling or the screening process may increase individuals’ positive attitudes toward and willingness to seek therapeutic treatment. A brief self-affirmation intervention demonstrated increases in positive attitudes and intentions for help-seeking among student veterans and community members (Seidman et al., 2019), and may be considered for AAPI and Hispanic college students. This intervention asked participants to rank-order personal values until they found the single most important value, and then write about “why the value made them feel good about themselves, what about it is important to them, and what it enables them to do in their life in domains such as work, relationships, and hobbies.” (Seidman et al., 2019, p. 655) Furthermore, outreach programs (e.g., informative brochures that speak to AAPI cultural values and counseling) might help to prevent, reduce, or overcome barriers related to counseling.
AAPI students may also benefit from explicit discussion of academic concerns. Clinicians may consider framing treatment goals for ADHD with academic outcomes; for example, therapy for ADHD will build concentration skills and may increase the quality of academic work. Current and previous findings demonstrate that AAPI students report the highest levels of academic impairment and tend to worry more frequently about academics due to perceptions of parental expectations for academic achievement (Saw et al., 2013). Therefore, a focus at the outset of treatment on academic concerns to validate client presenting problems may increase treatment engagement and reduce attrition (Ibaraki & Hall, 2014).
Clinicians may also consider using directive, solution-based approaches which are rated more positively among AAPI college students (Pan et al., 2019). This approach is in line with values of self-concealment and emotional control, and desires to protect family harmony or save face. In addition, mindfulness and acceptance-based psychotherapies may resonate with AAPI students because of their theoretical roots in Asian philosophies (Hall et al., 2011). Examples of such therapies include Dialectical Behavior Therapy (DBT; Fleming et al., 2015) and mindfulness-based therapy (Cairncross & Miller, 2020). Similarly, college/university administrators could help improve faculty and student awareness of classroom accommodations, services at college disability resource centers and promote organizational skills training (LaCount et al., 2018). Students with ADHD may also benefit from psychoeducation to dismantle the notion that they will be perceived negatively by peers and professors for utilizing academic accommodations (Lefler et al., 2023).
Finally, integrated behavioral healthcare settings are particularly well suited to address the underutilization of mental health services among AAPIs (Huang et al., 2016). Mental health stigma is a likely contributor to negative attitudes, feelings of shame, and avoidance of professional mental health service providers (Kim & Zane, 2016). By meeting AAPI patient preferences to seek help from medical providers (Chu et al., 2011), integrated settings can encourage earlier engagement with mental health treatment (Huang et al., 2016). Furthermore, integrated healthcare settings recognize the interconnection between the mind and body, a concept culturally relevant to many AAPIs (Leung et al., 2009), and may be suited for cultural adaptation. Importantly, it is imperative for clinicians to explore individual adherence to cultural values while being careful to not assume that all AAPIs have homogenous experiences. AAPIs constitute at least 28 different ethnic groups, and despite sharing some cultural characteristics, these subgroups are distinctive with regard to conceptualizations of mental illness (Pham, 2013) and willingness to use mental health services (Lee et al., 2015).
Limitations and Future Directions
First, this study was not able to characterize the diversity of Asian-American and Pacific Islander groups represented in this sample, limiting generalization to all Asian populations and biracial or multiracial students. Examining AAPIs as an aggregate group ignores how cultural differences across AAPI groups may be associated with varying prevalence rates and views of mental illness (Chaudhry & Chen, 2019). Future research in which more detailed racial-ethnic data are collected would be useful. Moreover, the response rate for the ACHA-NCHA-II is approximately 14% and may also limit the generalizability of these findings. Second, small pseudo R2 values of regression models indicate that other variables may explain additional variance in the models. The variable examining social functional impairment did not specify “ADHD” in the prompt and thus may reflect impairment unrelated to ADHD. Similarly, it is possible that participants who formerly met criteria for ADHD were excluded from the ADHD participant group in this sample, thus reducing the magnitude of group differences in impairment. Relatedly, the phrasing of the question regarding past year diagnosis and treatment makes it difficult to determine if the relatively large number of participants (16%–21%) across ethnic groups were diagnosed with ADHD in the past year or were reporting a pre-existing diagnosis. Future research should investigate de novo diagnoses of ADHD in college students as a function of race/ethnicity.
Third, this study did not include or control for variables related to socioeconomic status (SES), which can vary widely within the AAPI population (Budiman & Ruiz, 2021b) and can affect one’s ability to seek mental health care (Castro-Ramirez et al., 2021). Future studies can incorporate indicators of SES when examining the heterogeneity in ADHD help-seeking among AAPI groups. Fourth, dependent measures in this study were largely categorical and dichotomous assessments of impairment and treatment utilization. Future research using continuous data (e.g., Likert scales) and additional variables (e.g., perceived effectiveness of treatment, number of sessions attended, GPA, family history of ADHD) will provide more nuanced comparisons and may explain more variance in the regression models. This programmatic line of research can also be enhanced by incorporating qualitative data to encourage stakeholder engagement in intervention planning, implementation, and evaluation. Finally, future research on healthcare disparities in ADHD treatment utilization should incorporate a wider systemic lens in addition to focusing on mutable individual factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kevin Antshel has received Investigator Initiated Research funding from Takeda Pharmaceutical Company and participated on an Advisory board for Arbor Pharmaceutical Company. The authors have no other sources of support to declare.
Disclaimer
The opinions, findings, and conclusions presented/reported in this article/presentation are those of the author(s) and are in no way meant to represent the corporate opinions, views, or policies of the American College Health Association (ACHA). ACHA does not warrant nor assume any liability or responsibility for the accuracy, completeness, or usefulness of any information presented in this article/presentation.