
Abstract
Introduction
The efficacy of stimulant medications such as methylphenidate (MPH) and amphetamine for the treatment of ADHD has been established since the 1970s, and various formulations have since been developed (Kratochvil et al., 2009). Extensive efficacy and safety data are available for MPH (Wolraich & Doffing, 2004), largely relating to immediate-release (IR), short-acting formulations. The past decade has seen the development of several modified-release (MR) MPH formulations that provide symptom control over 8 to 12 hr (Brams, Moon, Pucci, & Lopez, 2010; Hosenbocus & Chahal, 2009). Compared with MR stimulants, IR stimulants are lower in cost and have greater dosing flexibility (Banaschewski et al., 2006); however, MR formulations may have the potential to reduce the stigma associated with taking ADHD medication while at school/work, improve compliance owing to fewer daily doses, and reduce the risk of drug misuse (Buitelaar & Medori, 2010). Meta-analyses have demonstrated similar effect sizes for IR MPH (0.76-0.92) and MR MPH (0.85-0.96) in children and adolescents (Faraone, 2009); nevertheless, because of cost reasons and dosing flexibility, MR formulations should not entirely replace the use of IR stimulant medications, and individual clinical choice should be allowed (Banaschewski et al., 2006).
The effects of stimulant medication on behavior throughout the day has been documented under highly controlled conditions in clinical trials (Döpfner et al., 2004; Swanson et al., 2004; Wigal, Kollins, Childress, & Squires, 2009), and these findings have been confirmed in a naturalistic setting (Döpfner, Görtz-Dorten, Breuer, & Rothenberger, 2011; Rothenberger, Becker, Breuer, & Döpfner, 2011). Head-to-head studies of MR MPH formulations have shown that superior symptom control is achieved by the formulation with the highest predicted plasma MPH concentration at a given point in time (Döpfner, Ose, Fischer, Ammer, & Scherag, 2011; Swanson et al., 2004).
In pharmacotherapy, dosing is often decided based on a combination of clinical trial data, clinical experience, and the individual needs of the patient, with the aim of combining optimal efficacy with minimal adverse events. Response to drug therapy, however, can vary considerably among patients; this creates a major challenge in pharmacotherapy, increasing the importance of individualized treatment regimens (Lin, 2007).
As with other drugs, ADHD medications are affected by interindividual variability (Froehlich et al., 2011; Stein & McGough, 2008); not all patients respond to stimulants equally. The observation of variable responses to MPH therapy in children with ADHD has led to the assumption that the overall population may be heterogeneous and comprise subpopulations with distinct symptom profiles after treatment. Subpopulations can be defined based on observed variables (e.g., age or symptom severity), and it has been shown, for example, that adolescents with ADHD need lower weight-adjusted MPH doses than children (Newcorn, Stein, & Cooper, 2010); it might be useful, therefore, to define age subgroups to partially explain the different effects of MPH. However, the determinants of response and nonresponse to MPH are not very well understood, and one alternative approach is to infer subpopulations with differential responses from the data (Lubke & Muthén, 2005; Nagin & Odgers, 2010). In this case, subpopulations are not defined in advance based on observed variables and, therefore, are called “latent”; once they are identified, observed variables (e.g., age or weight) can be used to describe them and to work out their similarities and differences.
To date, only a few studies have investigated latent subgroups in children with ADHD treated with stimulants. These studies have generally been conducted over relatively long observational periods (months or years) and with long intervals between assessment points (Frazier et al., 2010; Swanson et al., 2007), so that no information can be obtained about the immediate effects of treatment during the day. To our knowledge, only one work has evaluated the profiles of ADHD symptoms throughout the day (Sonuga-Barke et al., 2008), reanalyzing data from the Comparison of Methylphenidates in the Analog Classroom Setting (COMACS) study (Swanson et al., 2004). In this analysis, three severity classes with different mean symptom levels (low, intermediate, high) were detected during the placebo phase of the study. When treated with medication, the low-severity group showed only modest improvements compared with placebo, while treatment effects were larger in the two other subgroups, particularly in the high-severity group. For these two subgroups, symptom reduction was most pronounced 1.5 hr after medication intake and then lessened, so that 12 hr post-dose, symptom levels were slightly higher than at intake.
Observation of Safety and Effectiveness of Equasym XL in Routine care (OBSEER) was a 3-month, prospective, noncontrolled, noninterventional study involving children and adolescents with ADHD in Germany (Döpfner, Görtz-Dorten et al., 2011). The study was conducted under routine care conditions to gain insights into the effectiveness and safety of the MR MPH formulation Equasym XL (Shire Pharmaceuticals Ireland Limited, 2011), which contains 30% IR MPH and 70% extended-release MPH (MR MPH 30:70). Over the course of the study, a statistically significant decrease was observed in symptoms of ADHD, oppositional defiant disorder (ODD), and associated functional impairment as rated by parents, teachers, and clinicians (Döpfner, Görtz-Dorten, et al., 2011). Subgroups with differential treatment response could be identified over the OBSEER study period: two groups had severe symptoms at study start and showed a substantial treatment response, while two other groups (one with severe symptoms at study start and the other with less severe symptoms) showed no or comparatively little response (Hautmann, Rothenberger, & Döpfner, 2013). However, assessment points were weeks apart in this analysis, providing no information about the immediate response to medication throughout the day.
In OBSEER, the Day Profile of ADHD Symptoms (DAYAS) rating scale (Breuer, Görtz-Dorten, Rothenberger, & Döpfner, 2011) was used to assess the daily profile of ADHD symptoms and other externalizing behaviors. A statistically significant improvement in parent- and teacher-rated ADHD and ODD symptoms was observed from baseline for all periods of the day, in particular, the late morning and early afternoon until 4:00 p.m.
Treatment response and nonresponse to MPH medication throughout the day is currently insufficiently understood, and the identification of subgroups inferred from the OBSEER data seems to be a viable new way to gain insight into varying circadian medication effects. The aim of the present study was to identify and describe latent classes of patients with different symptom profiles on the DAYAS scale. In contrast to the only previous study evaluating latent subgroups for ADHD symptom profiles throughout the day that we are aware of (Sonuga-Barke et al., 2008), OBSEER was undertaken under routine care conditions, and this analysis was therefore a test of whether previous results could be replicated in a different setting. Furthermore, the sample size was much larger in OBSEER than in the previous trial (637 vs. 184 patients), increasing the likelihood of detecting smaller subgroups with more atypical symptom profiles.
Method
Participants and Study Design
The OBSEER study design has been described in detail previously (Döpfner, Görtz-Dorten, et al., 2011). Briefly, OBSEER was a postmarketing observational study of MR MPH 30:70 conducted in 169 centers in Germany. It included children aged 6 to 17 years with a confirmed diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders 4th ed., text rev. (DSM-IV-TR; American Psychiatric Association, 2000) or of hyperkinetic disorder (HKD) according to the International Classification of Diseases, Version 10 (ICD-10; World Health Organization, 1992) for whom therapy with this MR MPH formulation was already intended by the treating physician.
The planned observation period for each patient was 6 to 12 weeks after the first use of MR MPH and included three visits: prior to the start of treatment (Visit 1), 1 to 3 weeks after the first use (Visit 2), and 6 to 12 weeks after the first use (Visit 3), in accordance with standard practice. MR MPH was prescribed at Visit 1, and the dose was adjusted, when necessary, at Visits 2 and 3.
Written informed consent was obtained from parents, and the study was conducted under the responsibility of the attending physicians in accordance with local regulations. As this was an open-label observational study under routine care conditions, institutional review board approval was not required according to German and European regulations (Federal Institute for Drugs and Medical Devices & Paul-Ehrlich-Institute, 2010; European Parliament & Council of the European Union, 2001).
Assessments
ADHD symptoms and conduct problems across the day after the intake of MR MPH were evaluated at each visit using the DAYAS questionnaire (Breuer et al., 2011). Ratings were conducted by parents and teachers at the end of the school week and evaluated the behavior of children during different periods of the day, from early morning until bedtime. Correlation coefficients between daily and weekly ratings are sufficiently high to justify reliance on weekly ratings, to increase convenience for the participants (Breuer et al., 2011). Parents rated four daily periods (early morning before school, early afternoon, late afternoon and evening) and teachers two (first half and second half of the school morning). For this analysis, five items describing externalizing behavior were used: (a) hyperactivity, (b) inattention, (c) impulsivity, (d) oppositional behavior, and (e) aggressive behavior. For each period, parents and teachers rated each item on a 4-point scale using values from 0 (not at all) to 3 (very much). The DAYAS total score was calculated as the sum of the five individual item scores divided by the number of items. For this analysis, only ratings obtained at the last assessment point (Visit 3) were considered.
To detect the distinctive features of patient subgroups with different symptom profiles, the following covariates were evaluated as predictors for latent classes: sex, age, daily MR MPH dosage at Visit 3, and internalizing emotional symptoms; these were rated by parents at Visit 1 using the emotional symptoms scale (scale range = 0-10, with higher scores indicating more severe symptoms) of the Strengths and Difficulties Questionnaire (Goodman, 1997).
Statistical Analyses
To detect subgroups with different symptom profiles, a latent class cluster analysis was performed (Vermunt & Magidson, 2002) using repeated measures data from parent and teacher DAYAS ratings. Latent class cluster models assume that several latent classes exist and each person belongs to only one particular latent class; the number and size of classes are not known a priori. For the analyses, no restrictions were imposed on the variance–covariance matrices; all variances and covariances were estimated, and variance–covariance matrices were not held equal across classes (class-dependent unrestricted variance–covariance matrices). All models were computed using the Latent GOLD programme, Version 4.5 (Vermunt & Magidson, 2011).
To detect the distinctive features of the subgroups, the selected covariates (sex, age, daily MR MPH dosage at Visit 3, and parent-rated internalizing symptoms at Visit 1) were included in the model as predictors. Continuous covariates were z-transformed before being entered into the analysis; sex was coded as 0 for girls and 1 for boys. Regression of a categorical latent variable on several covariates corresponds to a multinomial logistic regression analysis.
The analysis strategy was to find a baseline model without covariates first. As a second step, covariates were introduced into the model of choice. Model selection was based on a formal statistical criterion (Bayesian information criterion [BIC]) as well as clinical considerations.
Cases with missing data on the covariates were excluded from the analysis. Cases with missing data on the DAYAS outcome measures remained in the analysis, and for parameter estimation, all available information was used (Vermunt & Magidson, 2005).
Results
Study Population
The OBSEER intent-to-treat population comprised a total of 822 patients (Döpfner, Görtz-Dorten, et al., 2011); after excluding patients with missing data on the covariates, 637 were eligible for this analysis.
The mean age (standard deviation [SD]) of children included in the analysis was 10.05 (2.51) years and 81.3% were male. Approximately half (56.0%; 338/604) had a disturbance of activity and attention (ICD-10 code F90.0, similar to ADHD combined type according to DSM-IV-TR); 35.4% (214/604) had hyperkinetic conduct disorder (F90.1) and 8.6% (52/604) had other HKDs (F90.8). About one quarter of patients (26.4%; 168/637) were treatment naïve, 45.7% (291/637) had received IR MPH, 23.2% (148/637) had been prescribed MR MPH formulations, and only 4.7% (30/637) had received medications other than MPH (e.g., atomoxetine or amphetamine) or unspecified medications. Among those previously receiving treatment, the main reasons for switching medication were insufficient overall effectiveness and/or a short duration of effect.
The symptom profile of children at Visit 3 (DAYAS, n = 637) is reported in Figure 1. A strong decrease in symptoms could be observed between the early morning, when the medication was taken, and the first and second half of the school morning. This reduction lasted until the early afternoon and was subsequently followed by a gradual increase toward the end of the day. Symptoms were higher in the evening compared with the morning. The average symptom profile corresponded to the expected average plasma level of MR MPH 30:70 over time (Wigal, Sanchez, DeCory, D’Imperio, & Swanson, 2003). In parent ratings, up to 13.2% (84/637) of data were missing; in teacher ratings, this value was up to 37.4% (238/637).
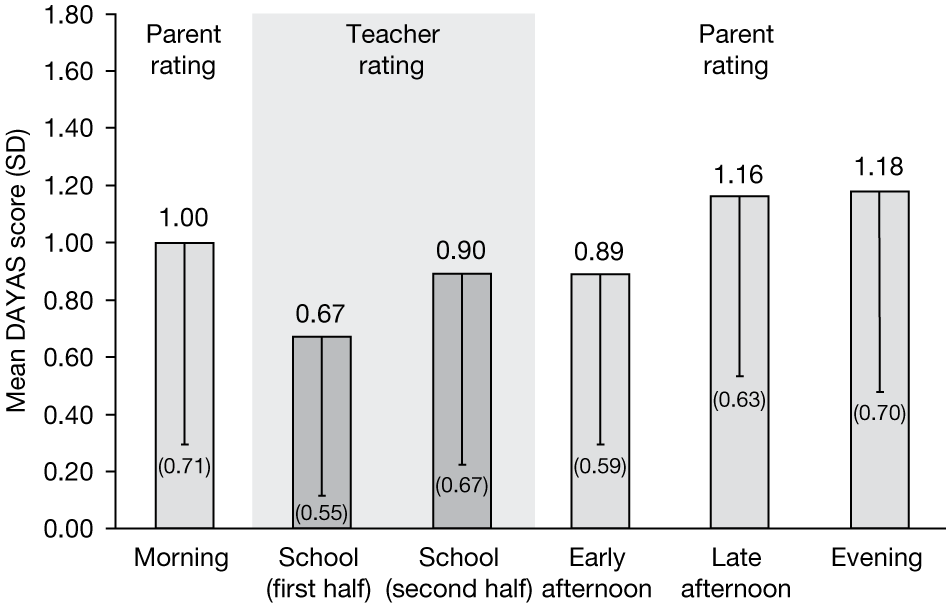
Symptom profile in parent and teacher ratings assessed using the DAYAS questionnaire in the total sample at Visit 3 (n = 637).
Latent Class Cluster Analysis
Latent class cluster models with repeated measures data from parent and teacher DAYAS ratings were analyzed. In the first step of the analysis, models with up to five classes were estimated (see Table 1) without including covariates to predict latent class membership. Based on the BIC score and clinical considerations, the two-class model was chosen (Model A2).
Results of the Latent Class Cluster Analysis.
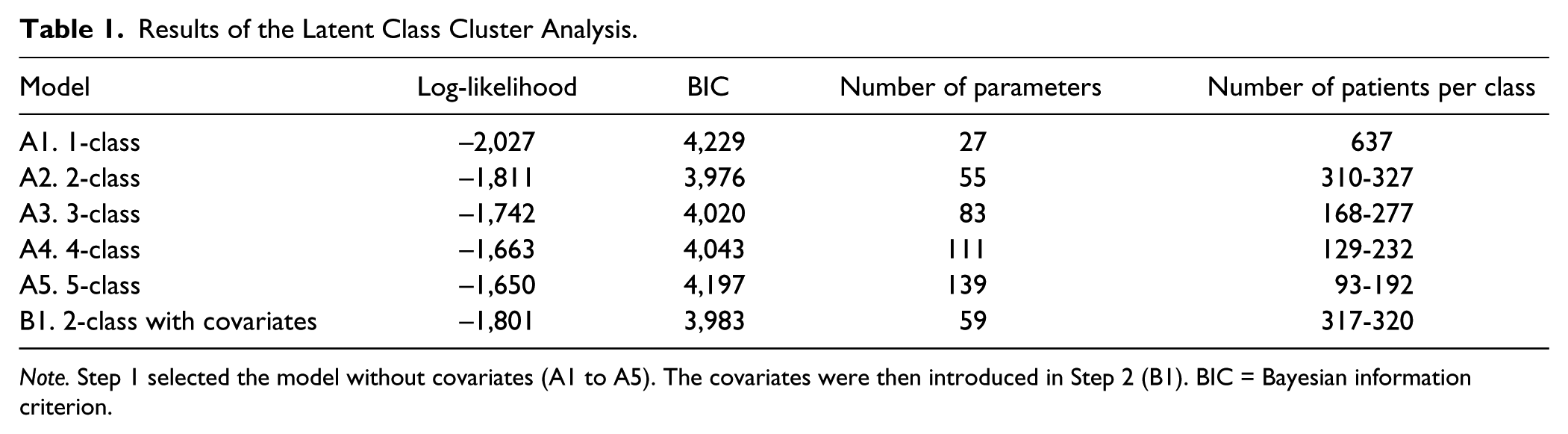
Note. Step 1 selected the model without covariates (A1 to A5). The covariates were then introduced in Step 2 (B1). BIC = Bayesian information criterion.
In the second step of the analysis, the selected covariates to predict latent classes were entered into the two-class model (Model B1). This extension only slightly influenced the results on latent classes, and their interpretation generally remained the same.
In the two-class solution with covariates, high-severity (49.8%) and low-severity (50.2%) symptom classes were identified (see Figure 2). The high-severity class showed severe symptoms in the early morning in parent ratings and a strong symptom reduction in teacher ratings during the first half of the school morning. Symptoms increased during the second half of the school morning and for the rest of the day, with high symptom levels being observed also in the evening. The low-severity class showed low symptoms in the early morning, which also decreased during the first half of the school day and then increased slowly toward the evening. For descriptive purposes, means and SDs for the covariates in the high- and low-severity classes are shown in Table 2. Patients in the high-severity class had a higher proportion of boys, were younger, and were titrated to a higher MPH dose during the study.
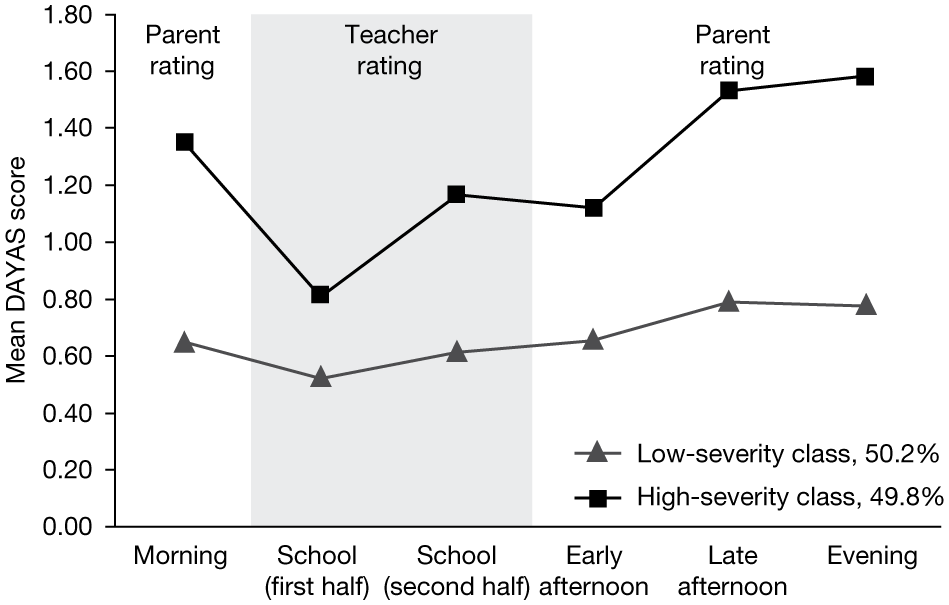
Symptom profiles of the high- and low-severity classes assessed by parents and teachers using the DAYAS questionnaire at Visit 3.
Means and SDs of Covariate Values in the Total Sample and in the Subgroups of the Two-Class Solution With Covariates.

Note. Estimates for latent classes are based on the most likely class membership. MPH = methylphenidate; MPHVisit 3 = daily dose of MR MPH 30:70 prescribed at Visit 3.
Emotional symptoms scale of the Strengths and Difficulties Questionnaire as rated by parents at Visit 1.
The results of a multinomial logistic regression analysis with latent class as a criterion and the covariates as predictors are reported in Table 3. With the exception of emotional symptoms, all covariates were useful for latent class membership prediction. Younger children, boys, and children with a more intense MPH treatment were more likely to fall into the high-severity class.
Multinomial Logistic Regression Analysis With Latent Class as a Criterion.

Note. The reference class is the high-severity class; all covariates except sex were z transformed; sex was coded 0 for girls and 1 for boys. ß= regression coefficient; OR = odds ratio; MPH = methylphenidate; MPHVisit 3 = daily dose of MR MPH 30:70 prescribed at Visit 3.
Emotional symptoms scale of the Strengths and Difficulties Questionnaire as rated by parents at Visit 1.
Discussion
Children with ADHD do not benefit equally from treatment with MPH, and there is heterogeneity in treatment response. This analysis was conducted to identify children with different daily profiles of externalizing symptoms after intake of a MR MPH formulation in the morning. Data for analysis stem from a noninterventional observational trial. This type of study can provide valuable information about the effectiveness of a drug under real-life conditions, yet the validity of the conclusions that can be drawn is more restricted than in randomized trials. Consequently, the following interpretations of the findings have to be considered with caution.
Two symptom severity classes were detected. Children in the high-severity class were generally more symptomatic, but showed a strong symptom reduction in the morning that lessened in the afternoon and evening. Children in the low-severity class were less symptomatic, and showed minor symptom reduction in the morning followed by a small increase. In both subgroups, symptom levels in the evening were slightly higher than in the morning.
The clearly observable symptom reduction in the high-severity class is an indication that medication effects are maintained or become even more apparent when children exhibit more symptoms and there is more room for symptom improvement. As medication effects lessened throughout the day, symptoms reoccurred; this might be because MPH treatment is only symptomatic and not causal, therefore ongoing medication is needed to retain low symptom levels.
In contrast, in the low-severity class, only minor improvements in symptoms were observed. This cluster of patients followed a more stable course and did not experience the ups and downs of the high-severity class. As these children were in general much less symptomatic, this group might be regarded as being well stabilized on MPH. Furthermore, it has to be considered that this analysis only included data from the final assessment point, when the children had already received MR MPH for several weeks; during this time, the average symptom level might have decreased. However, in the absence of any control group, no firm conclusions can be drawn and it might be that these children were generally less symptomatic, irrespective of any treatment.
In addition to the identified subgroups, it is also important to consider which types of subgroups could not be observed and what conclusions might be drawn from this. We did not identify a subgroup with severe symptoms that did not respond to treatment at all, or a cluster of patients where a worsening in symptoms was detected. While this can be considered indicative of the general efficacy and safety of MPH, it does not necessarily mean that all patients follow their subgroup trend, as there might still be patients within a subgroup who do not benefit from MPH. The observed profiles reflect an average trend, and within each group, there is interindividual variation. What this analysis suggests is that, if there are patients with an atypical profile, they should not be regarded as a separate subgroup but as extreme cases of the observed clusters.
In both identified subgroups, symptom levels in the evening were slightly higher than in the morning, which is likely to be due to confounding factors. First, there is a lessening of medication effects across the day; medication intake was in the morning, and MR MPH 30:70 is considered to be effective up to 7.5 hr post-dose (Anderson & Keating, 2006). Second, as shown by the placebo condition in clinical trials, children with ADHD often experience a natural increase in symptoms throughout the day, and the symptom course can be described as an inverted U-shape, with higher symptoms in the evening than in the morning (Swanson et al., 2004; Wigal et al., 2009).
Older children were more likely to be members of the low-severity class; this result might be explained by the developmental changes observed in ADHD. Although ADHD is associated with several negative outcomes reaching into adulthood (Biederman et al., 2006), longitudinal studies show that, as children get older, symptoms of inattention, hyperactivity, and impulsivity often decrease (Gau et al., 2010; Langberg et al., 2008). Therefore, it is plausible that the low-severity class comprises children at a later stage of their development. Furthermore, results from a laboratory school setting (Wigal, Kollins, Childress, & Adeyi, 2010) have shown that, irrespective of differences in the average symptom level, children of different age groups respond equally to stimulant medication when symptoms are observed throughout the day.
Boys were more likely to be in the high-severity class. As in the case of age, boys with ADHD generally present more severe symptoms than girls (Abikoff et al., 2002; Thorell & Rydell, 2008). There is evidence that treatment effects across the day are similar for boys and girls (Wigal et al., 2010), but findings are sometimes inconsistent across studies (Sonuga-Barke et al., 2007). Therefore, there are indications that male sex is predictive of higher average symptom levels, but not of better treatment response.
The high-severity class included children with higher MPH dosages, showing that patients with more severe symptoms are treated more intensely. As the effect of MPH is dose dependent (Castells et al., 2011), this finding is consistent with expectations and also might be interpreted that symptom severity in this subgroup cannot simply be regarded as a sign of undermedication. However, it may be possible that children in this subgroup were not receiving the optimal MPH dosage, as an increase in symptoms was already observed during school hours, in the morning. This subgroup may benefit from an additional dose of IR MPH in the afternoon or a medication with a longer duration of action.
Emotional symptoms were not useful for latent class subgroup discrimination. In studies observing longer periods of time than symptom change across the day, children with ADHD and comorbid anxiety seem to benefit equally from MPH as their counterparts without comorbid symptoms (MTA Cooperative Group, 1999; Owens et al., 2003). As in our analysis, both subgroups showed a treatment effect, although in different ways, and our results would be in line with this.
The interpretation of subgroup differences and specifically of the interaction between time and group is complicated by at least two factors. First, moderators of treatment response are generally investigated over longer periods of time (e.g., weeks; Hinshaw, 2007) and results from such studies cannot be easily extrapolated to explain changes over the course of the day. Second, this was not strictly a moderator analysis, in which differences in treatment outcomes are investigated in relation to third variables. The aim of this analysis was to describe latent subgroups, which is a different approach, and little research has been done on this topic to date.
This analysis confirms some important findings of Sonuga-Barke et al. (2008), who also investigated symptom profiles across the day in latent subgroups. We could replicate the finding that children with more severe symptoms show a stronger treatment response, and in both studies, the low-severity class comprised older children. However, some results were conflicting with the previous study, which identified a third group of patients with only moderate symptoms. Several factors might account for this discrepancy. As in our analysis, the number of patients was three times higher than in the COMACS study, so it is unlikely that an insufficient sample size prevented the detection of an additional subgroup. However, Sonuga-Barke et al. (2008) identified the subgroups during the placebo phase, while we analyzed the data after children had received their medication for several weeks. As a consequence of treatment, certain subgroups may have vanished, and the composition of subgroups might have changed. In addition, methodological differences such as the use of different statistical models and their specification may have affected the results and the number of obtained classes (Bauer & Curran, 2004).
The OBSEER study has several limitations, which have previously been discussed in detail (Döpfner, Görtz-Dorten, et al., 2011). As an observational study, parents were not blinded to the study treatment, which may have affected their rating of ADHD symptoms. Teachers were not formally informed about treatment and were mostly unaware, but could have been told by parents or children. As this was not a randomized controlled trial, the interpretation of the findings is complicated and the validity of the conclusions can be questioned. A control condition would have allowed both a more detailed investigation of medication effects and the disentangling of actual treatment effects from the natural course of the symptoms across the day. With respect to this analysis, there was a substantial proportion of missing data for teacher ratings of ADHD symptoms. A modern missing-data handling strategy was used, taking into account all available data. This approach was chosen because it is considered preferable to ad hoc methods (e.g., casewise or listwise deletion), even when the underlying assumptions are not met (Collins, 2006).
The identification and characterization of treatment response heterogeneity is an important area of research that is particularly relevant to clinical practice, as it provides information about the distinctive features of patient subgroups that can help the physician to optimize treatment for the individual patient. Further investigation is needed to confirm our findings and the clinical applicability of the identified subgroups, and future trials should also consider genetic information for subgroup description. In fact, interindividual variability in drug response arises from a range of factors, including psychological and environmental aspects, but genetic polymorphism is considered to be the most important contributor (Ermer, Adeyi, & Pucci, 2010; Lin, 2007). Extending this type of analysis to include biological information would therefore be useful to improve our understanding and prediction of patient subgroups with differential treatment response.
In summary, the response to MPH treatment is highly variable and currently not fully understood. This analysis aimed to identify different types of patients who vary in their symptom profiles by using a data-driven methodology. Two severity groups were detected, and no subgroup showing paradoxical treatment effects or a chronic high level of symptoms was identified, underscoring the general efficacy of MPH. Despite some differences, most findings were in line with previous results from the COMACS study (Sonuga-Barke et al., 2008) and, therefore, some subgroup characteristics appear to be robust and reliable across different settings. In our study, girls, older children, and less intensively treated children were more likely to be members of the low-severity class, in line with existing knowledge.
Footnotes
Acknowledgements
The authors would like to thank Professor Herbert Hoijtink from Utrecht University for advice regarding the statistical analyses.
Authors’ Note
Under the direction of the authors, Alyson Bexfield, PhD (Caudex Medical, UK, funded by Shire AG, Switzerland), drafted the introduction, and Monica Guidi, PhD (Caudex Medical, UK, funded by Shire AG, Switzerland), language edited the manuscript and collated and incorporated author comments. Editorial assistance in formatting, proofreading, and copy editing was also provided by Caudex Medical, UK, funded by Shire AG, Switzerland. The content of this manuscript, the ultimate interpretation, and the decision to submit it for publication in the Journal of Attention Disorders was made by the authors independently.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christopher Hautmann has received travel grants from Shire Pharmaceuticals Ltd. Aribert Rothenberger has acted as a consultant on advisory boards and/or as a speaker for Lilly, Shire Pharmaceuticals Ltd, Medice, Novartis, and UCB Pharma. He has received research support from Shire Pharmaceuticals Ltd, the German Research Foundation, and Schwaabe, and travel and educational grants from Shire Pharmaceuticals Ltd. Manfred Döpfner has received research grants and/or acted as a consultant on advisory boards for the German Research Foundation, Lilly, UCB Pharma, Shire Pharmaceuticals Ltd, Medice, and Vifor.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was funded by Shire AG, Switzerland.