
Abstract
Introduction
ADHD is a neurodevelopmental disorder with an estimated worldwide prevalence of 5% (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007). In Sweden, the first-line recommendation for treatment is nonpharmacological interventions; the second-line treatment is medication with central stimulants. This is in keeping with guidance from the Swedish Medical Products Agency and the U.K. National Institute for Health and Care Excellence (NICE; 2018). According to the World Health Organization (WHO), pediatric overweight and obesity are important public health challenges and are well-established risk factors for future cardiovascular disease, diabetes, and cancer (Cote, Harris, Panagiotopoulos, Sandor, & Devlin, 2013; Ezzati et al., 2002). While largely preventable, childhood overweight and obesity constitute major risks for adult obesity (Gordon-Larsen, The, & Adair, 2010). In the Western world, the prevalence of overweight in children and adolescents has increased substantially over the last two decades and is estimated at 20% to 25% (Ng et al., 2014). Recent national data on Swedish 10-year-old children are in line with this (Karolinska University Hospital, 2017). Not only does this trend pose a risk to future physical health of the individual, but overweight young people are also more often bullied, present with a lower quality of life, and have lower self-esteem (Halfon, Larson, & Slusser, 2013).
Several studies have demonstrated an association between ADHD and overweight or obesity (Gungor, Celiloglu, Raif, Ozcan, & Selimoglu, 2016; Spencer, Faraone, Tarko, McDermott, & Biederman, 2014; Waring & Lapane, 2008), although the evidence is inconclusive (Byrd, Curtin, & Anderson, 2013; Erhart et al., 2012; Fliers et al., 2013; Hanc et al., 2015; Holtkamp et al., 2004; Racicka, Hanc, Giertuga, Brynska, & Wolanczyk, 2015). Nigg et al. (2016) reported an odds ratio (OR) of 1.22 (95% confidence interval [CI]: [1.11, 1.34]) for obesity among children with ADHD in a meta-analysis of 43 studies. Another meta-analysis found a similar OR of 1.20 (95% CI: [1.05, 1.37]) for obesity in children with ADHD (Cortese et al., 2016). ADHD diagnosis is more common in boys, and there are limited data on overweight/obesity in girls with ADHD (Byrd et al., 2013; Fliers et al., 2013).
Studies on methylphenidate (MPH) have shown that a single dose of MPH reduces energy intake from fat and carbohydrates in obese adolescents (Danilovich, Mastrandrea, Cataldi, & Quattrin, 2014) and reduces energy intake in obese adult males (Leddy et al., 2004). On the contrary, other studies have indicated that MPH-medicated children have lower activity levels and thus a decrease in total daily energy expenditure (Butte, Treuth, Voigt, Llorente, & Heird, 1999; Konrad, Gunther, Heinzel-Gutenbrunner, & Herpertz-Dahlmann, 2005). In clinical studies, a modest association between MPH treatment and lower weight gain has been documented (Poulton & Cowell, 2003; Powell, Frydenberg, & Thomsen, 2015; Schwartz et al., 2014; Swanson et al., 2007; Wilens et al., 2005). Wilens et al. (2005) reported a moderate reduction in short-term (4-6 months) weight gain and a minor reduction in weight for age z-score over 21 months of extended release MPH medication. In the Multimodal Treatment of ADHD (MTA) study, Swanson et al. (2007) showed a stimulant-related decrease in weight z-score until 3 years of treatment of initially stimulant-naive children (n = 88). In a large longitudinal study, Schwartz et al. (2014) studied body mass index (BMI) trajectories in medicated and unmedicated children with ADHD and found that unmedicated ADHD was associated with higher BMI as compared with children without stimulants or without ADHD. A meta-analysis by Cortese et al. (2016) found that rates of obesity were about 40% lower in individuals pharmacologically treated for ADHD compared with those who were not treated. This was, however, based on a subset of studies and the association was nonsignificant. Despite all the above associations, data on the effects of stimulant medication on already established overweight or obesity in children with ADHD are still scarce and conflicting (Dubnov-Raz, Perry, & Berger, 2011; Mattes & Gittelman, 1983; Schertz, Adesman, Alfieri, & Bienkowski, 1996).
The aim of this study was to investigate the prevalence and ORs of overweight and obesity in stimulant-naive boys and girls diagnosed with ADHD in the county of Värmland, Sweden, as compared with a reference group from the same area and to compare the change in BMI for age (i.e., the relative position in the BMI growth chart) after the initiation of MPH treatment in normal versus overweight/obese children with ADHD.
Method
Study Population
We performed a population-based retrospective study with approval from the Regional Ethics Review Board in Uppsala, Sweden. The study group consisted of children (<18 years) with normal intellectual ability, resident in the county of Värmland, Sweden, and receiving immediate or extended release MPH medication for ADHD as of August 2015. Children with diabetes mellitus, an eating disorder, or motor impairment were excluded. In the county of Värmland, 4.8% of all boys aged 10 to 17 years and 2.2% of all girls aged 10 to 17 years were prescribed ADHD medication in 2015, according to the National Board of Health and Welfare. The prescription rate was similar to that of the rest of the country. In Sweden, the prescription of stimulants for children up to 18 years of age is licensed only to specialists in child and adolescent psychiatry or pediatric neurology. This service is centralized, and medication was prescribed as a second-line intervention as part of a multimodal treatment approach. Families also received psychosocial intervention, including psychoeducation about the disorder, but no specific intervention against overweight was routinely provided. ADHD was diagnosed using Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria. The diagnosis was made at a cross-disciplinary conference after an assessment including medical and psychiatric history, physical examination, psychological evaluation, and reports from parents and preschool or school teachers. MPH doses were individually titrated based on symptoms, functional impairment, and side effects as reported by patients, guardians, and teachers.
Reference Group
All children in the county have their heights and weights measured by the school nurse at 6, 10, 13, and 16 years of age. Data are stored in the Pupil Health Database and were used to obtain an age- and sex-matched reference group from the general population when calculating ORs for overweight/obesity in the clinical study group. Six-year measurements (n = 2,321) were used as reference for the age interval 4 to 8 years in the study group, 10- and 13-year data together (n = 2,370 and n = 2,082, respectively) for the age interval 9 to 13 years, and 16-year data (n = 1,925) for the age interval 14 to 18 years.
Data Collection
Heights and body weights of children with ADHD diagnosis receiving MPH were available through electronic records. Measurements were in all cases performed by trained medical staff. Children had their heights and weights measured at the start of treatment and thereafter on a six-monthly basis while on treatment. We collected heights and weights at four different time points: at the initiation of treatment (I), 6 months into treatment (“I + ½y), between 1 and 1½ years into treatment (I + 1½y) and between 2½ and 3 years into treatment (I + 3y). In the case of more than one available measurement during any of the intervals, the last one was used for analysis to represent the longest possible follow-up.
To ensure that the baseline measurements (I) in all cases were before the start of medication, matched heights and body weights up to 6 months prior to the start of treatment were accepted for calculation of the relative position in the BMI chart (if data were not available at the exact medication starting point). For the measurements made while on treatment, a margin of plus or minus 2 months outside the desired interval was accepted. Prescriptions of MPH were reviewed, identifying the maximum daily dose during and after titration. Concomitant prescriptions of anti-psychotic, anti-depressive, or anti-epileptic medications (with metabolic effects); a diagnosis of autism spectrum disorder (ASD); and the lifetime diagnosis of major depressive disorder were recorded for adjustment purposes.
Statistics
BMI (kg/m2) was calculated and children were classified as underweight/normal weight (hereafter presented as “normal weight”), overweight, or obese according to established age-adjusted International Obesity Task Force (IOTF) BMI cutoffs (Cole, Bellizzi, Flegal, & Dietz, 2000). Overweight and obesity correspond to BMI 25 and 30, respectively, at the age of 18 years. Hereafter, the overweight category includes obese children, because already manifest obesity requires previously established overweight.
The BMI standard deviation score (BMI-SDS), that is, z-score, represents the age- and sex-specific standardized BMI (also interpreted as the relative position in a growth chart). It was calculated at the initiation (BMI-SDS(I)) of stimulant medication, and at I + ½y, I + 1½y, and I + 3y, based on the WHO growth reference for 5 to 19 year of age (de Onis et al., 2007) using AnthroPlus software (WHO, 2009). For each individual, the changes in BMI-SDS from I to I + ½y, from I to I + 1½y, and from I to I + 3y were calculated.
ORs for overweight and obesity in the ADHD group were calculated compared with the reference group. Stratification for sex, age, comorbid diagnoses (ASD and lifetime major depressive disorder), and prescription of the abovementioned psychotropic medications was made. Chi-square tests were used for cross-tabulation data. Wilcoxon signed rank tests were used for comparisons of paired data and Mann–Whitney U tests for comparisons between groups. To investigate the relationship between BMI-SDS at the initiation of MPH and changes in BMI-SDS at the different measurement points, stepwise multivariate regression models were performed with the change in BMI-SDS as the dependent variable and BMI-SDS(I), sex, age, ASD diagnosis, maximum daily dose of MPH/kg body weight, and concomitant use of psychotropic drugs as the independent variables. Modeling with the same adjustments was done with BMI-SDS(I) grouped into quartiles included in the regression models with the first quartile as the reference, as predictors of the change in BMI-SDS to I + 3y (representing the longest treatment duration). A reduction of ⩾0.5 in BMI-SDS for age was regarded as clinically highly important and hence we also assessed the proportions of children (normal vs. overweight at MPH initiation) fulfilling this criterion at I + ½y, I + 1½y and I + 3y. Statistical analyses were performed in SPSS (Version 20, IBM, New York, NY, USA).
Results
We identified 744 children eligible for inclusion. Seven children were excluded due to lack of essential study data (i.e., uncertain date of first MPH prescription or lack of height or weight measurement at initiation), eight were excluded due to a concomitant diagnosis of eating disorder and five due to diabetes mellitus. Hence, in total 724 children were included in the study. Medication with MPH was initiated between March 2006 and August 2015, 0 to 78 months after ADHD diagnosis (mean 6 months). Descriptive data on the study group are presented in Table 1. Mean (SD) doses of MPH by body weight after individual titration were lower in overweight children than in normal weight children: 0.71 (0.26) mg/kg versus 0.86 (0.29) mg/kg (p < .001).
Descriptive Data of the 724 Children in the Study Group.
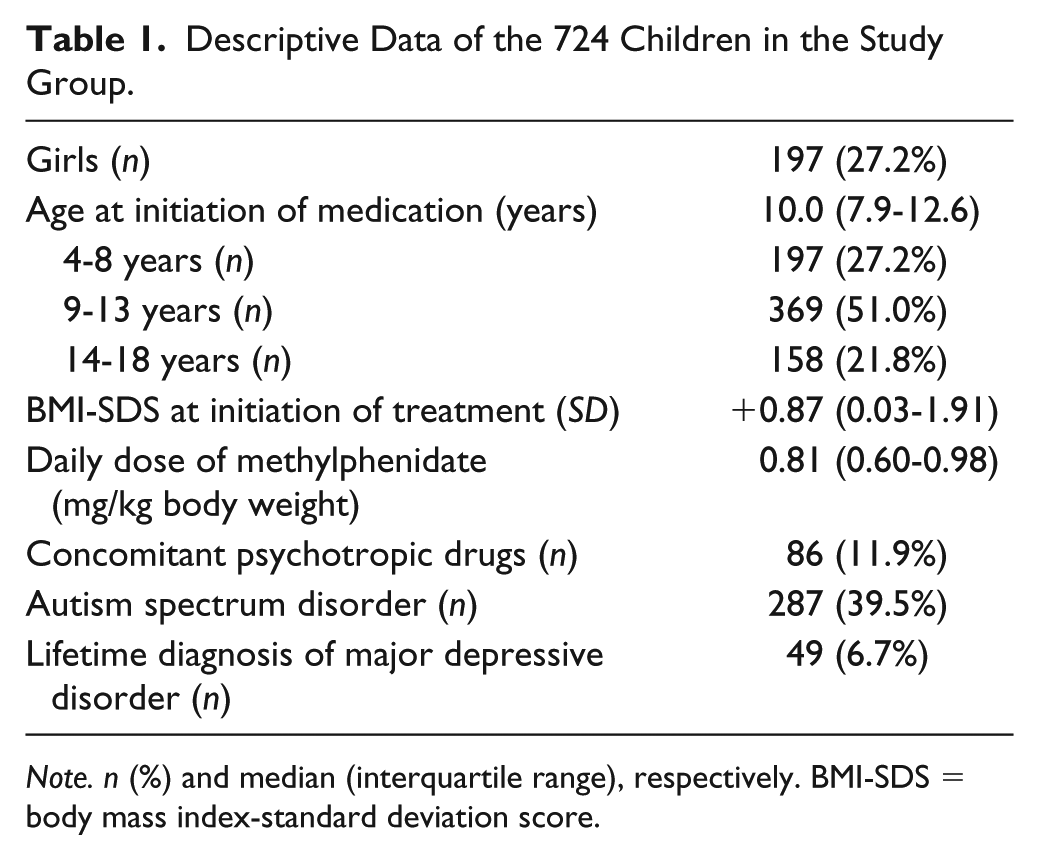
Note. n (%) and median (interquartile range), respectively. BMI-SDS = body mass index-standard deviation score.
Prevalence and ORs for Overweight and Obesity
The prevalence of overweight and obesity in the study group and reference group is presented by age in Table 2, together with ORs. In the total ADHD sample, there were clearly increased ORs for overweight and obesity. Girls had higher ORs for overweight from the middle school years as compared with boys, and a higher OR for obesity (Table 2). Comparing children within the ADHD group, the overweight prevalence was not different in children with ADHD and ASD (39.8%) as compared with children with ADHD only (35.7%), with OR = 1.16 (95% CI: [0.85, 1.58]) for this comparison. Children with ADHD and a lifetime diagnosis of major depressive disorder (n = 49), however, had an additionally increased risk of overweight as compared with children with ADHD but no affective disorder, with OR = 1.84 (95% CI: [1.03, 3.28]).
Prevalence and Odds Ratios for Overweight and Obesity at the Initiation of Methylphenidate Treatment.
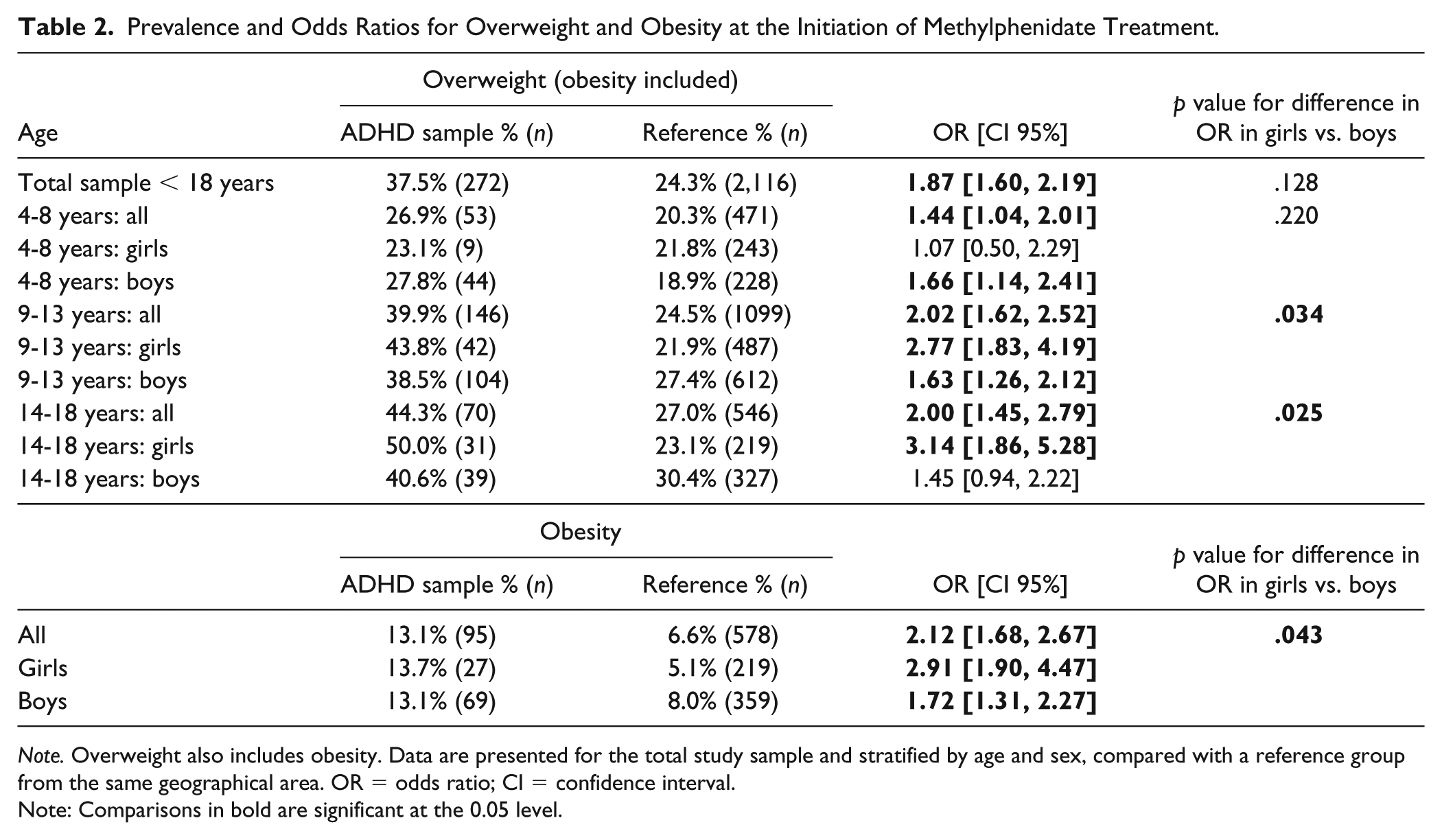
Note. Overweight also includes obesity. Data are presented for the total study sample and stratified by age and sex, compared with a reference group from the same geographical area. OR = odds ratio; CI = confidence interval.
Note: Comparisons in bold are significant at the 0.05 level.
Changes in BMI-SDS During Medication
A significant decrease in BMI-SDS from the initiation of medication was identified at all three measurement points, with the largest decrease at I + 3y. Children with overweight decreased their BMI-SDS more than normal weight children (Table 3). In stepwise multivariate regression models, BMI-SDS(I) correlated with the reduction in BMI-SDS from the initiation of MPH medication at all three measurement points: the regression coefficients B (p value) for BMI-SDS(I) as predictor of change in BMI-SDS were −0.12 (p < .001) at I + ½y; −0.19 (p < .001) at I + 1½y and −0.24 (p < .001) at I + 3y. With BMI-SDS(I) assessed by quartiles, the subsequent decrease in BMI-SDS until I + 3y was larger for every quartile of BMI-SDS(I) above the first (Figure 1). A larger proportion of the children identified as overweight at MPH initiation reduced their BMI-SDS by ⩾0.5 at I + 1½y and I + 3y, as compared with children of normal weight at MPH initiation (Figure 2).
Change in BMI-SDS From the Initiation of Medication.
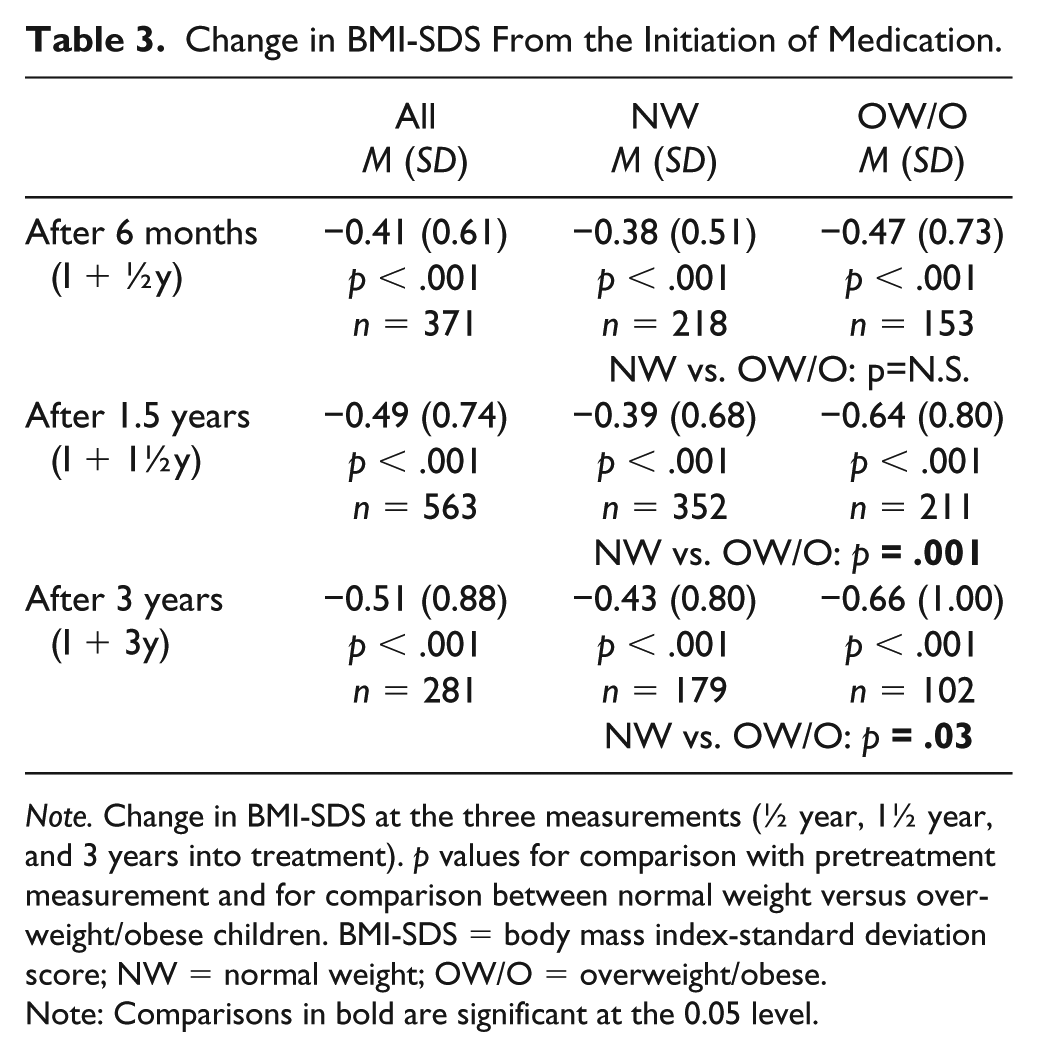
Note. Change in BMI-SDS at the three measurements (½ year, 1½ year, and 3 years into treatment). p values for comparison with pretreatment measurement and for comparison between normal weight versus overweight/obese children. BMI-SDS = body mass index-standard deviation score; NW = normal weight; OW/O = overweight/obese.
Note: Comparisons in bold are significant at the 0.05 level.
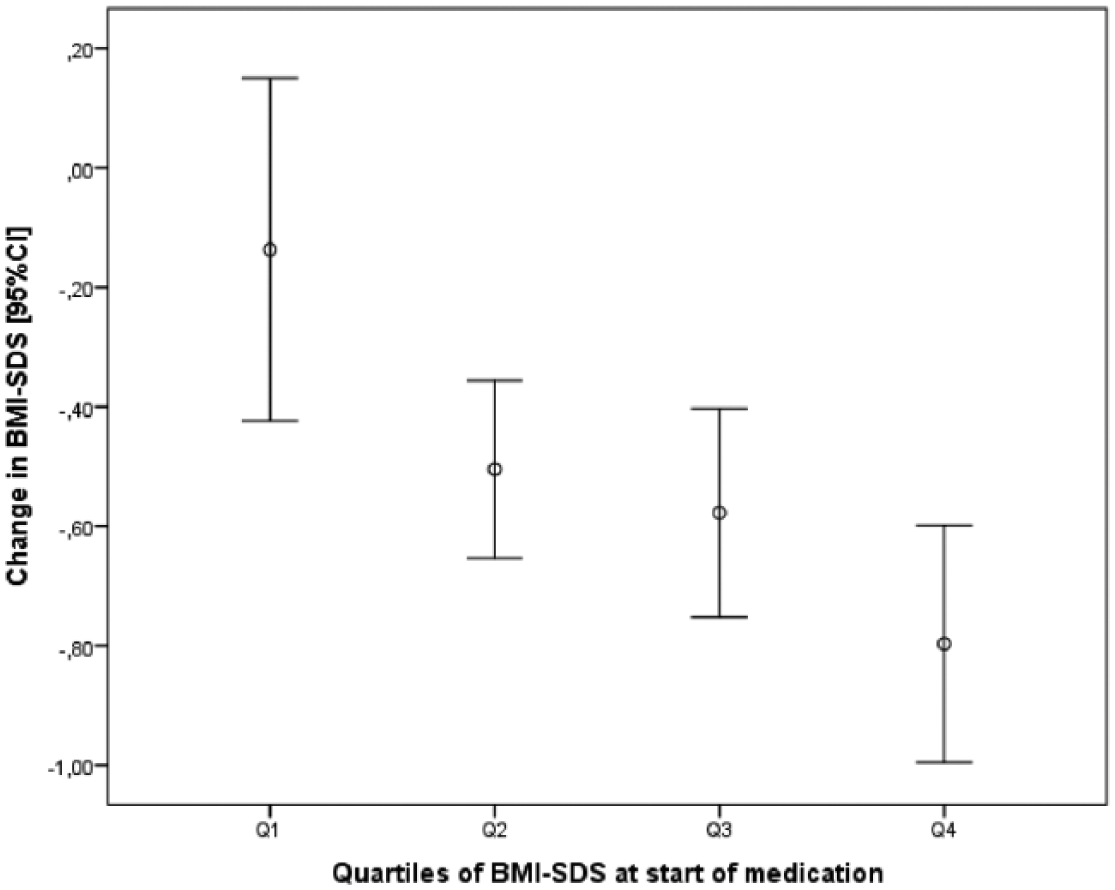
Change in BMI-SDS from initiation of methylphenidate medication.
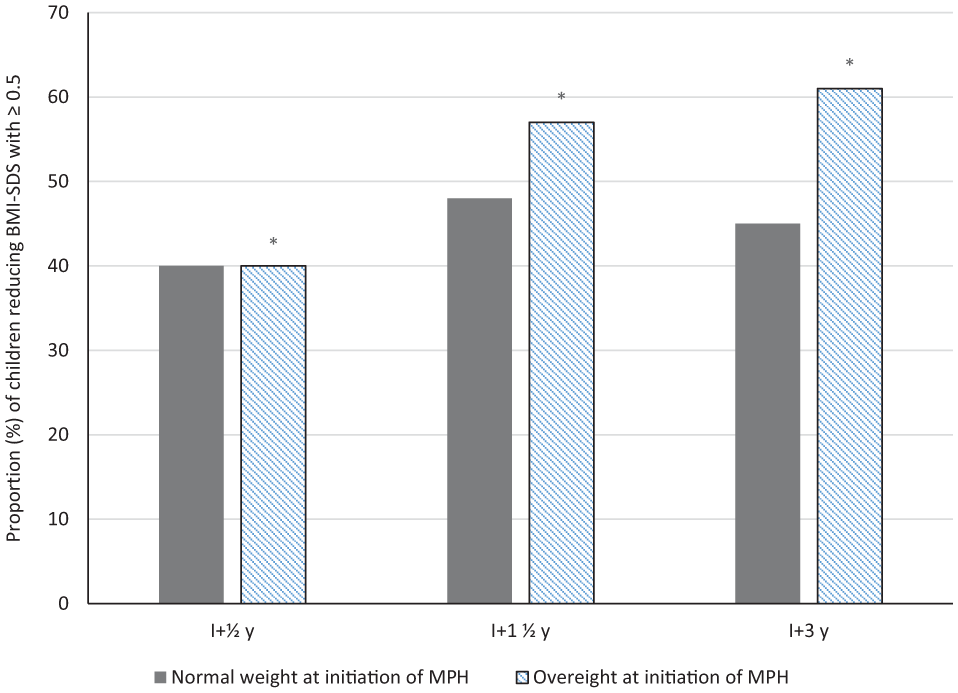
Proportions of children, normal versus overweight/obese at the initiation of methylphenidate treatment with a BMI-SDS reduced by ⩾ 0.5 from the start of medication until ½ year, 1½ years, and 3 years into treatment, respectively.
The importance of the covariates differed somewhat between the three measurements. At I + 1½y, where the largest sample size (n = 549) was obtained, the following significant predictors were identified with regression coefficients B (p value) for the prediction of change in BMI-SDS from MPH initiation: sex (girl) = −0.16 (p = .023), age (years) = .002 (p = .013), maximum daily dose of MPH (mg/kg body weight) = −0.24 (p = .045), and concomitant psychotropic drug treatment (yes) = .24 (p = .016). There were no associations between a diagnosis of ASD and the change in BMI-SDS at any measurement point.
Discussion
In this population-based study on central stimulant-naive children, we found an association between ADHD and overweight as well as obesity, irrespective of gender. We also showed that MPH medication was associated with a larger decrease in BMI for age in children with established overweight or obesity as compared with normal weight children, over a period of up to 3 years.
ORs for Overweight/Obesity
We found ORs for overweight and obesity in both boys and girls with ADHD slightly higher than those identified in meta-analyses by Cortese et al. (2016) and Nigg et al. (2016). This might be partly explained by the inclusion criteria restricted to children qualifying for pharmacological intervention, which could indicate patients with more severe ADHD symptoms and functional impairment. Racicka et al. (2015) found a higher prevalence of obesity in children treated with MPH, supporting this.
Comorbid Conditions
That a large proportion of children in the present sample had considerable functional impairment is also indicated by the high prevalence of ASD (almost 40%) in addition to ADHD. This reflects that MPH prescriptions centralized to the present clinic, a referral center for neurodevelopmental disorders, included ASD as well as ADHD, where medical priority was influenced by the degree of functional impairment. This may consequently have resulted in an inclusion bias to some degree, but it also means that diagnostic investigations included a thorough evaluation of ASD as a routine, which may partly explain the high prevalence of autism in this sample. Interestingly, when stratifying the study group, an additional diagnosis of ASD did not influence overweight or obesity prevalence. In a recent systematic review and meta-analysis, an association was shown between ASD and obesity (Zheng et al., 2017). The authors stated that individuals with ASD often have eating problems, such as food selectivity and other dietary habits, which make standard dietary interventions and obesity prevention less effective. Moreover, they spend less time on physical activities and they have more chance of being treated with antipsychotic medication. Furthermore, some have comorbidities that are associated with obesity such as ADHD, sleeping disorders, and gastrointestinal problems.
The prevalence of overweight in children with ADHD and a lifetime diagnosis of depression reached 50%, which is significantly higher than in the remaining sample of children with ADHD. The overall ORs of overweight/obesity were, however, practically unchanged if children with comorbid depression were excluded from the analyses (data not shown), unlike the study by Nigg et al. (2016) where the authors concluded that the association between ADHD and obesity was accounted for by covarying conditions. With our study design, it was not possible to determine whether depression caused overweight or the other way around. A meta-analysis found inconsequential results investigating the direction of the relationship between depressive disorder and body weight, including both cross-sectional and longitudinal studies in adolescents (Roberts & Duong, 2015). However, this patient group might be particularly vulnerable, suffering from three conditions, all of which could impair a patient’s social life, as well as physical and mental health (Byrd et al., 2013; Fliers et al., 2013; Hanc et al., 2015).
Gender Differences
There have been limited investigations into the association between ADHD and overweight or obesity in girls. In our population-based sample, which included 197 girls with ADHD, girls in the middle school years and older were shown to be at increased risk of being overweight; the risk of obesity was also significantly higher in females with ADHD than in the reference group. In the reference group, height and weight data from ages 10 and 13 years together served as comparison with the ADHD group of 9 to 13 years. During this typical age of puberty onset, variations in changes of height and weight may be marked, and data on specific age group boundaries should be interpreted in the light of absent puberty status reports. Despite this, the results clearly support an association between ADHD and overweight/obesity in girls. In the interval 9 to 18 years, even higher ORs for overweight and obesity were identified in girls as compared with boys. This is in line with the limited research on children and adolescents (Cortese et al., 2016; Fliers et al., 2013; Nigg et al., 2016), as no similar gender effect has been reported in adults. In our study, girls also had, compared with boys, a larger decrease in BMI-SDS after the start of MPH treatment.
BMI Development After MPH Initiation
Considering both the magnitude of the association according to mean values, as well as the proportions of children with a major reduction (⩾0.5 SD) in BMI for age, we considered the relationship between MPH medication and BMI-SDS reduction in already overweight/obese children to be clinically relevant. We furthermore identified an association between age at the start of medication and subsequent development in BMI for age, with less of a reduction in BMI-SDS in older children, supported by previous findings (Schwartz et al., 2014). Based on our results, we hypothesize that MPH medication, in addition to its effects on core ADHD symptoms, may also have a favorable effect on BMI development in overweight and obese children and adolescents with ADHD.
Although previous data on MPH medication and body weight development in already overweight/obese children are scarce, the present results are in line with two early and small studies. Schertz et al. (1996) showed that pretreatment weight (adjusted for age, gender, and height) was associated with the degree of weight loss in a sample of 60 children (54 boys) treated with MPH or dextroamphetamine. In another small sample, greater initial weight was related to a higher degree of loss in weight percentile during 1 to 4 years of MPH medication (Mattes & Gittelman, 1983). On the contrary, Dubnov-Raz et al. (2011) found no significant change from baseline in mean BMI for age in a likewise small sample of 28 overweight children and a follow-up period of 1 year. Replication of the present findings in prospective clinical trials is warranted to establish the beneficial effect of MPH on BMI development in overweight and obese children with ADHD. Bearing in mind the difficulty in obtaining healthy BMI development with increasing age in conventional obesity (Chamay-Weber et al., 2016; Fiechtner, Cheng, Lopez, Sharifi, & Taveras, 2017), the present findings may however indicate that a delay of otherwise indicated medication should be avoided.
There is limited research on the mechanisms behind an association between ADHD and overweight/obesity. A multifactorial etiology is suggested, including impulsivity-related binge eating, executive dysfunction, less physical activity (e.g., due to inattention giving trouble when attending organized activities), genetic factors and sleep disturbances (Hanc & Cortese, 2018). The association between ADHD and obesity also seems bidirectional, that is, obesity is common in individuals with ADHD and the prevalence of ADHD is also high in individuals with obesity (Levy, Fleming, & Klar, 2009). The present relationship between MPH treatment and favorable BMI development supports the value of early ADHD evaluations in obese children. Some evidence for a similar strategy in adults with refractory obesity has previously been presented (Levy et al., 2009), where better self-directedness, a reduction in novelty seeking, and increased capacity for persistence (rather than the temporary anorexigenic effect of stimulants) were suggested to mediate the effect.
Recent studies have suggested that ADHD symptoms are associated with binge eating and loss of control eating (Egbert et al., 2018). The effect of MPH on binge eating needs to be examined in further studies.
Strengths and Limitations
The population based retrospective design is a major strength as well as limitation of the present study; the risk of inclusion bias (in addition to what was discussed above in terms of impairment) is strongly reduced. In contrast to clinical trials where weight development may be heavily affected by short-term lifestyle changes, the present observational and natural setting represents daily life in clinical practice. Here, BMI values were collected at the start of stimulant treatment, thus in a drug-naive population, in contrast to several previous studies. Another strength is that medication was individually titrated to appropriate doses according to symptoms and functional impairment. The difference in BMI-SDS development between normal versus overweight children with ADHD was clinically important and statistically significant, and hence the main finding of our study. In future studies, it would also be useful to take puberty development into account. Because, through statistical adjustment in a large sample, we found no impact of comorbid ASD on BMI development, we did not find that the rate of ASD in the present study group influenced the clinical importance of the present findings.
With the present study design, a strict medication effect on BMI can of course not be evaluated. It should also be noted that we were unable to adjust for socioeconomic status, family BMI patterns, or ethnicity. Finally, the lack of compliance data is a further limitation. Low socioeconomic status is associated with both ADHD and childhood obesity and is a possible confounder in the association between ADHD and increased weight, but we do not expect this to be an important confounder in the relationship between premedication BMI-SDS and subsequent weight development. In cases where staff or parents have concerns regarding slow or excessive weight gain, children are likely to have been weighed more often. Here, we reduced such bias by using measurements at fixed points in time after the initiation of medication rather than including all available measurements. Additional strengths of the present study are that ADHD was diagnosed according to DSM-IV criteria after multiprofessional team investigations, and BMI values were based on measurements performed by trained medical staff; no self-reports were used.
Conclusion
In a stimulant-naive population of children and adolescents with ADHD, overweight or obesity were considerably more common than in the reference population from the same area. The results indicate that the association is strongest in girls starting in the middle school years. During medication with methylphenidate in this group with a comparably high prevalence of ASD, children with ADHD and overweight or obesity reduced their BMI-SDS more than children who were at a normal weight. The reduction of BMI in children with ADHD and obesity is challenging to achieve, and the promising indication of favorable weight development with methylphenidate medication warrants prospective research in other clinical populations.
Footnotes
Acknowledgements
We thank the patients and staff of the Child and Adolescent Psychiatry unit in Karlstad Sweden, as well as the School Health Care staff of the County of Värmland, Sweden, for the valuable data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Lisbet Engh was supported by Karlstad University, Maria Unenge Hallerbäck by the Child and Adolescent Psychiatry clinic in Karlstad, and Sverre Wikström by Örebro University, Sweden.