
Abstract
Keywords
Introduction
Children with Gilles-de-la-Tourette syndrome (TS) show involuntary tics that can be withheld for short intervals. TS is also often associated with a variety of comorbid symptoms that involve poor response inhibition including obsessive-compulsive behavior (OCB), ADHD, oppositional behavior, and explosive outbursts (Leckman & Cohen, 1999).
Difficulties in response inhibition can refer to a number of distinct problems affecting either involuntary or voluntary movements and actions. In voluntary movements, response inhibition problems can affect the decision whether or not to initiate a movement, the control of interference between competing movements, or the capacity to wait for the appropriate time to initiate the movement. Much work has examined the first two types of inhibition problems. For example, there is evidence that TS can be associated with some mild difficulties in the control of interference between competing responses (Channon et al., 2009; Channon, Gunning, Frankl, & Robertson, 2006) but when comorbid ADHD is present, much more pronounced difficulties are observed (Eddy, Rizzo, & Cavanna, 2009). Moreover, many studies have examined the decision of whether to initiate a response in ADHD. For example, in Go/NoGo reaction time tasks children with ADHD (Itami & Uno, 2002; Shallice et al., 2002; Sherman, Shepard, Joschko, & Freeman, 1998) but not children with TS (Eichele et al., 2010; Roessner, Albrecht, Dechent, Baudewig, & Rothenberger, 2008) can show problems inhibiting erroneous Go responses to NoGo signals. Moreover, children with ADHD can show slowed performance in countermanding prepared responses immediately before their execution in stop-signal reaction time tasks but their general slowing in response initiation prevents a clear interpretation of these difficulties (Oosterlaan, Logan, & Sergeant, 1998; Overtoom et al., 2002; see Lijffijt, Kenemans, Verbaten, & van Engeland, 2005, for a review).
Responses that are initiated prematurely in relation to situational demands are a prime example of response inhibition difficulties and they are often observed in people with ADHD (Barkley, 1997; Sagvolden & Sergeant, 1998) but also sometimes in people with OCB (Chamberlain et al. 2007; Müller et al., 2003). Previous work suggests that ADHD can bias action toward rapid responses (Sonuga-Barke, Taylor, Sembi, & Smith, 1992) even when participants are instructed to favor accuracy (Mulder et al., 2010). However, if response inhibition problems are linked to a lack of temporal control of responses independently of response selection, it should increase the frequency of premature responses in situations that do not involve selecting whether to respond but only involve selecting when to release a prepared response.
Children with ADHD can show premature responding as well as high temporal variability in response timing tasks that involve reproduction of predictable intervals or synchronization of responses with temporally predictable signals (Ben-Pazi, Gross-Tsur, Bergman, & Shalev, 2003; Rubia, Halari, Christakou, & Taylor, 2009; Rubia, Noorloos, Smith, Gunning, & Sergeant, 2003; Rubia, Smith, & Taylor, 2007; Rubia, Taylor, Taylor, & Sergeant, 1999; Toplak, Dockstader, & Tannock, 2006). However, if ADHD is linked to a difficulty in withholding a response during a brief period, premature responses should appear even when the trigger stimulus is temporally unpredictable.
With the present evidence, it is still unclear whether TS or ADHD is associated with a specific difficulty in withholding preprogrammed movements, that is, waiting for the appropriate time to respond, when no response selection is necessary, and whether triggering stimuli are temporally predictable. The goal of the present study was to determine whether TS or TS + ADHD increases the frequency of premature responses in a simple reaction time task to targets that are either temporally predictable or unpredictable. We compared the performance of children with TS with and without ADHD and controls on a fast-paced target detection task requiring a decision as to when to respond but no decision as to whether or what to respond. We compared a response timing task with a fixed foreperiod to tasks with a variable foreperiod to dissociate problems linked to the attentional requirements of the task from difficulties in waiting to respond.
Method
Participants
Participants were children and adolescents aged between 7 and 16, including children diagnosed with TS or chronic tic disorder (CTD) and ADHD (n = 17; TS: 12, CTD: 5), children diagnosed with TS or CTD without ADHD (n = 17; TS: 14, CTD: 3) and healthy controls (n = 17). The three groups were matched for age and gender. All children were French Canadian and attended regular schools. Patients were recruited at the Tourette clinic of Sainte-Justine hospital. Patients (above 14 years) or their parents gave written and informed consent to the research coordinator that was not involved in their care. The research was approved by the institutional research ethics board. Exclusion criteria were (a) inability to provide consent, (b) a history of head injury or other neurological disorder that may cause tics, (c) tics linked to drugs, (d) a psychotic disorder, or (e) a pervasive developmental disorder.
ADHD was evaluated by trained professionals through a clinical interview using the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV-TR; American Psychiatric Association, 2000) criteria. To be included in the TS + ADHD group, children had to show at least six hyperactivity-impulsivity criteria. Among children with ADHD, 13 children showed the mixed ADHD subtype and 4 showed hyperactive-impulsive ADHD. Participants with the inattentive ADHD subtype were excluded from the study as the study was aimed at hyperactivity-impulsivity symptoms. To be included in the TS without ADHD group, children had to show three criteria or less on both inattention and hyperactivity-impulsivity dimensions.
Tics were evaluated by trained professionals using the Yale Global Tic Severity Scale (YGTSS; Leckman et al., 1989). Obsessive-compulsive symptoms were evaluated with the Yale–Brown Obsessive-Compulsive Scale (YBOCS; Goodman et al., 1989). Behavioral symptom ratings were obtained using the Conners’ Parent Rating Scale–Revised (CPRS-R; Conners, Sitarenios, Parker, & Epstein, 1998).
Of the 34 participants with TS, 15 were without medication. In the TS-only group, 3 children took selective serotonin reuptake inhibitors (SSRIs) and 1 also took neuroleptics and benzodiazepines. In the TS + ADHD group, 7 took stimulants at the time of the evaluation and 8 took other drugs (neuroleptics n = 6, Clonidine n = 4, or SSRIs n = 1).
Procedure
The task involved the detection of a target letter in brief letter streams presented at nine letters/s, often called a rapid serial visual presentation (RSVP). Participants were told to press a key as quickly as possible after the detection of the target but not before. The tasks were presented using E-Prime software (PST Inc.). The stimuli were presented in the center of an LCD screen. Each trial consisted of a cross presented for 800 ms, followed by a rapid sequence of nine random capital letters, eight black, and one white (the target), 1.5 cm high, presented during 83 ms on a dark gray background. After each trial, the response time (RT) was shown on the screen for 1 s; RTs equal or inferior to 0 ms (premature responses) were shown as 0 ms. The high stimulation rate and the feedback on RT were designed to create an incentive to respond rapidly and maximize attention to the letters. Participants were told to try to keep RT as low as possible while avoiding RTs of 0 ms.
In the high-predictability condition, the target always appeared in the middle of the stream (fifth position) corresponding to a fixed foreperiod of 332 ms. In the moderate-predictability condition, the target appeared in positions 4, 5, or 6 with equal probability (foreperiod range = 249-415 ms). In the low-predictability condition, the target appeared in positions 2, 5, or 8 with equal probability (foreperiod range = 83-581 ms). All children were tested in three blocks of 100 trials each (one per condition) in the following fixed order (High predictability–Moderate predictability–Low predictability) and participants were verbally informed of the possible target positions before each block. This sequence of conditions was used to train participants at the 332 ms foreperiod, the average foreperiod in all conditions, before testing their capacity to adapt to temporal variations around this foreperiod in the following conditions. Because of this methodological choice to train participants on the fixed foreperiod, differences between conditions were confounded with the order of presentation of conditions and condition effects were therefore not considered except to determine that group differences were present when fixed and variable foreperiods were used.
Results
Clinical scores are summarized in Table 1. Compared with the TS-only group, the TS + ADHD group showed a significantly higher worst lifetime tic severity and more opposition symptoms but did not differ in terms of OCB or anxiety symptoms.
Summary of Demographic and Clinical Characteristics: Mean (SD).
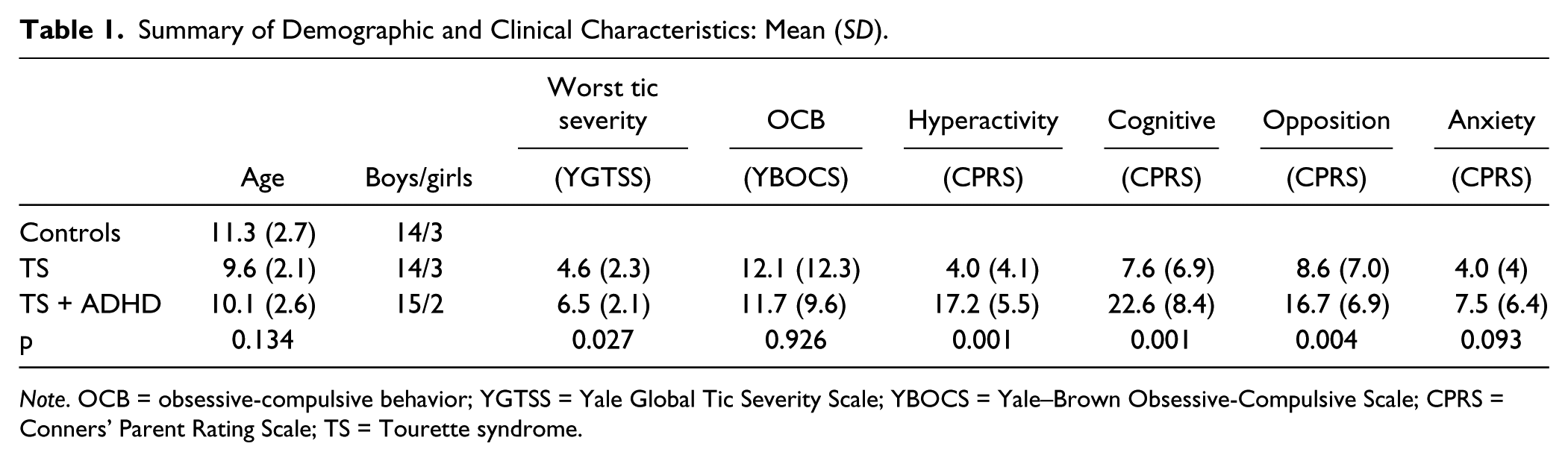
Note. OCB = obsessive-compulsive behavior; YGTSS = Yale Global Tic Severity Scale; YBOCS = Yale–Brown Obsessive-Compulsive Scale; CPRS = Conners’ Parent Rating Scale; TS = Tourette syndrome.
Figures 1, 2, and 3 summarize the performance of the three groups in each condition for the proportion of premature responses (Figure 1), mean reaction time (Figure 2), and the coefficient of variation (COV) of RT (Figure 3).
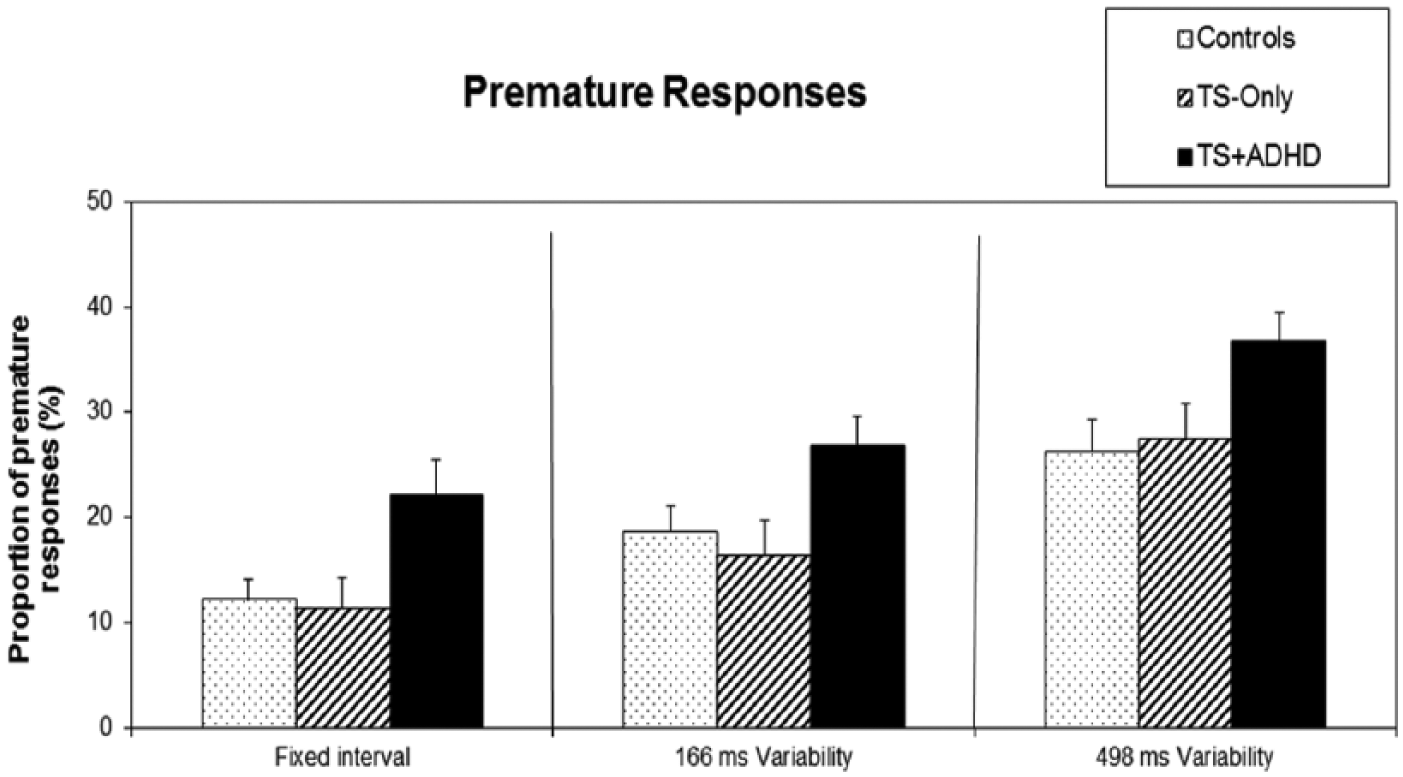
Proportion of premature responses across the three different predictability conditions, for each group (Controls, TS-only, and TS + ADHD).
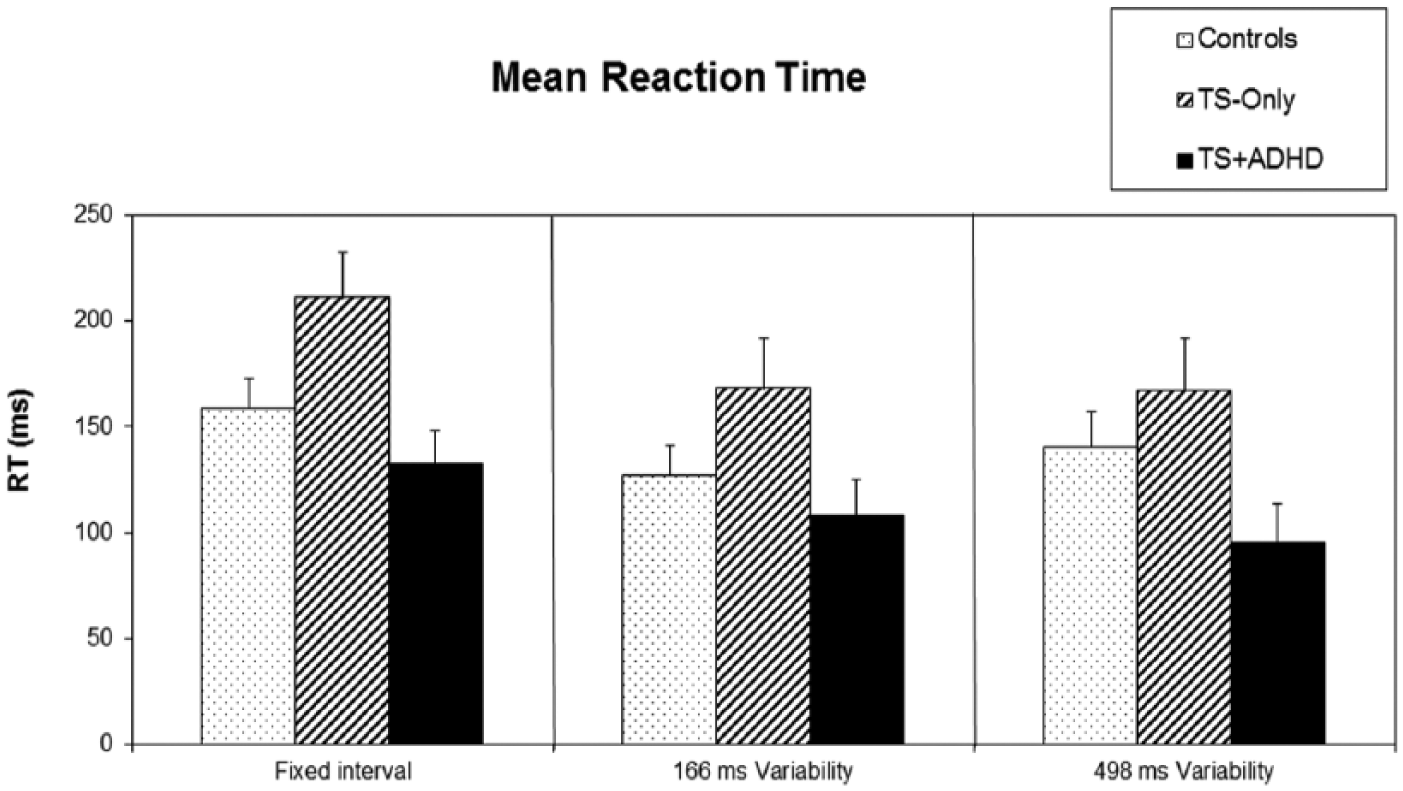
Mean reaction time across the three different predictability conditions, for each group (Controls, TS-only, and TS + ADHD).
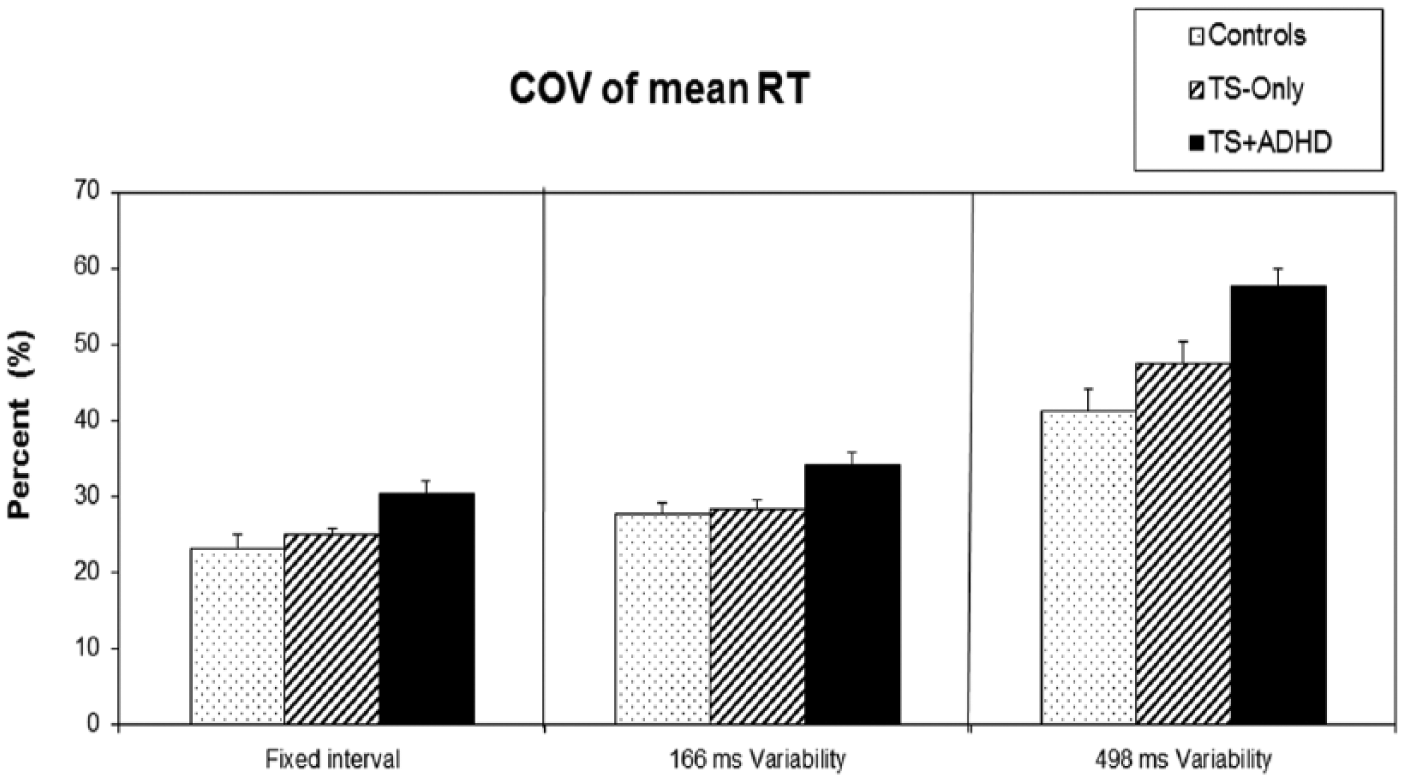
Coefficient of variation of mean reaction time across the three different predictability conditions, for each group (Controls, TS-only, and TS + ADHD).
Premature Responses
The proportion of responses occurring before the target (premature responses) was analyzed using non-parametric tests because of the high frequency of zero values in some groups. In the high-predictability condition, the proportion of premature responses differed significantly among the groups, Kruskal–Wallis χ2(2, 48) = 7.9, p = .019. Pairwise comparisons using Mann–Whitney U tests revealed that the TS + ADHD group produced more premature responses than the other groups: TS + ADHD versus TS-only, U = 71.0, p = .011; TS + ADHD versus controls, U = 80.0, p = .026; and TS-only versus controls, U = 125.5, p = .518. The group difference in the proportion of premature responses was also observed in the moderate-predictability condition, Kruskal−Wallis χ2(2, 48) = 6.36, p = .043; TS + ADHD versus TS-only, U = 80.5, p = .026, TS + ADHD versus controls, U = 87.0, p = .048; and TS-only versus controls, U = 120.0, p = .413; and in the low-predictability condition: Kruskal−Wallis χ2(2, 48) = 6.31, p = .043, TS + ADHD versus TS-only, U = 81.0, p = .029, TS + ADHD versus controls, U = 82.5, p = .031, and TS-only versus controls, U = 139.5, p = .865.
RT
Mean RT was analyzed using ANOVAs followed, when appropriate, by post hoc analyses using least significant difference (LSD) criteria. In the high-predictability condition, the mean RT was significantly slower in the TS-only group, F(2, 48) = 5.01, MSE =27,362.8, p = .011 (TS + ADHD vs. TS-only p = .003, TS + ADHD vs. controls p = .307 and TS-only vs. controls p = .043). Mean RT was not significantly different among the groups in the moderate-predictability condition, F(2, 48) = 2.59, MSE =16,045.3, p = .086, and in the low-predictability condition, F(2, 48) = 2.98, MSE = 22,202.4, p = .06.
RT Variability
The variability of RT was examined through the COV of RT. In the high-predictability condition, an ANOVA showed that RT variability was significantly higher in the TS + ADHD group than the other two groups, F(2, 48) = 5.701, MSE = .02, p = .006, (TS + ADHD vs. TS-only p = .022, TS + ADHD vs. controls p = .002, and TS-only vs. controls p = .369). Similar results were obtained in the moderate-predictability condition, F(2, 48) = 6.19, MSE = .02, p = .004, TS + ADHD versus TS-only, p = .005, TS + ADHD versus controls, p = .003, and TS-only versus controls, p = .871, and also in the low-predictability condition, F(2, 48) = 8.7, MSE = 0.12, p = .001, TS + ADHD versus TS-only, p = .013, TS + ADHD versus controls, p < .001, and TS-only versus controls, p = .127.
To evaluate whether the groups differed in the distributions of the latency of premature responses, we examined the COV of RTs for premature responses. We applied a square root transformation to the data to correct for non-normal distributions. In the high-predictability condition, RTs of premature responses were not significantly more variable in the TS + ADHD group than in the other two groups, F(2, 43) = 2.95, MSE = .03, p = .063 (TS + ADHD vs. TS-only, p = .022, TS + ADHD vs. controls, p = .138, and TS-only vs. controls, p = .387), but they were more variable in the moderate-predictability condition, F(2, 47) = 4.41, MSE = .03, p = .021 (TS + ADHD vs. TS-only p = .009, TS + ADHD vs. controls, p = .033, and TS-only vs. controls p = .535) and in the low-predictability condition, F(2, 48) = 3.2, MSE = .04, p = .05 (TS + ADHD vs. TS-only p = .047, TS + ADHD vs. controls, p = .025, and TS-only vs. controls, p = .784).
Effects of Practice and Post-Error Slowing on RT
An ANOVA on the effect of practice in the high-predictability condition showed that mean RT decreased significantly between the first and last third of trials, F(2, 48) = 8.05, MSE = 11,429.15, p = .005, and the effect of practice was not significantly different among the three groups, F(2, 48) = .70, MSE = 936.09, p = .503, indicating a similar improvement in response speed in the fixed foreperiod in all groups.
To evaluate if the groups differed in the amount of slowing of the response following a premature response, we compared RT on trials immediately following a premature response and those following non-premature responses in the high-predictability condition. The ANOVA showed a significant effect of the error feedback, F(2, 45) = 23.968, MSE = 84,365.68, p < .001, showing that all groups slowed their responses following a feedback indicating a premature response, and there was a significant difference between the groups, F(2, 45) = 4.927, MSE = 41885.45, p =.012 (TS + ADHD vs. TS-only, p =.004, TS + ADHD vs. controls, p = .444, TS-only vs. controls, p =.034), but the interaction of Group and Feedback was not significant, F(2, 45) = 1.55, MSE = 5473.14, p = .222.
Delay-Dependent Speeding
In the low-predictability condition, we also evaluated the size of the delay-dependent speeding effect in the different groups. We computed the difference in mean RT between the middle (332 ms) and the late target (581 ms) for each participant and compared groups on the size of this difference. We did not consider the earliest target position due to the extremely short foreperiod used (83 ms). An ANOVA showed a significant effect of group, F(2, 48) = 2.29, MSE = 24,238.1, p = .004, patient groups showing a significantly increased delay-dependent speeding compared with controls (TS + ADHD: M = 242.2, SD = 38.92, vs. TS-only: M = 252.19, SD = 46.75, p = .641; TS + ADHD vs. controls: M = 182.37, SD = 88.67, p = .007; and TS-only vs. controls, p = .002).
Correlations Between Performance and Tic Severity
Because the two patient groups differed in worst tic severity (YGTSS), we examined the correlations between this measure and performance measures in the first condition and in patients with tic disorders (N = 31). None of the performance measures showed significant correlations with worst tic severity, proportion of premature responses: r(29) = .07, p = .70; mean RT: r(29) = .005, p = .98; COV of RT: r(29) = .22, p = .24.
Stimulant Medication
We also examined differences between children under stimulant medication (n = 7) and those without stimulants (n = 10) in the TS + ADHD group using t tests. No significant differences were found between these two subgroups on mean RT, RT variability, or the proportion of premature responses in any condition.
Discussion
The goal of this study was to determine whether patients with tic disorders show difficulties in withholding a preprogrammed response independently of selecting whether to respond. The results indicate that patients with ADHD but not patients with tic disorders without ADHD showed more frequent premature responses, as well as more variable RTs than controls in our simple reaction time task whether the foreperiod was fixed or variable.
The effects observed here were not related to obsessive-compulsive traits or anxiety as the severity of these symptoms was similar in the two patient groups. Moreover, worst lifetime tic severity was higher in the ADHD group but we found no correlation between performance and tic severity.
One could suggest that ADHD children may have had an impaired capacity to attend to the target stimulus. However, ADHD children showed more premature responses even in the first task when the timing of the stimulus was completely predictable. This suggests that the premature responding of ADHD children was not linked to the temporal uncertainty of targets and thus cannot be explained by problems in attending to the target.
Another hypothesis is that the increase in premature responses in children with ADHD was due to poor response timing. However, children with ADHD also showed more frequent premature responses with variable foreperiods when timing cannot be predicted, suggesting that a response timing difficulty cannot explain the increase in premature responses in the ADHD group.
The present results parallel those observed in patients with traumatic brain injury (TBI) who show premature responses when the stimulation delay is predictable (Robertson, Manly, Andrade, Baddeley, & Yiend, 1997). In rats, dorsomedial prefrontal cortex (dmPFC) inactivation has been shown to increase the frequency and temporal variability of premature responses in a simple reaction time task (Broersen & Uylings, 1999; Narayanan, Horst, & Laubach, 2006; Risterucci, Terramorsi, Nieoullon, & Amalric, 2003). This effect appears whether the triggering stimulus is temporally predictable or not and is thus independent of attention to the triggering stimulus (Narayanan et al., 2006). Medial frontal cortex is a key portion of the mesocorticolimbic system involved in guiding response choices based on previous actions and outcomes (Kennerley, Walton, Behrens, Buckley, & Rushworth, 2006). There is evidence that dmPFC activity can modulate delay-related activity in motor cortex (Narayanan & Laubach, 2006) and this modulation may contribute to the inhibition of premature responses. Studies using paired-pulse transcranial magnetic stimulation (TMS) in motor cortex have shown evidence of reduced resting intra-cortical inhibition (ICI) in children with ADHD (Buchmann et al., 2007; Moll, Heinrich, Trott, Wirth, & Rothenberger, 2000), and a positive correlation has been observed between the reduction of ICI and the severity of symptoms (Gilbert et al., 2006; Schneider et al., 2007). TMS studies have also reported reduced resting motor cortex ICI in TS (Heise et al., 2010; Orth, Amann, Robertson, & Rothwell., 2005; Ziemann, Paulus, & Rothenberger, 1997), which may be correlated with the severity of tics (Gilbert et al., 2004; Orth, Münchau, & Rothwell, 2008). However, there is also evidence of a reduced motor excitability before movement execution in TS, suggesting that cognitive control processes may help compensate for reduced ICI in patients used to witholding tics (Heise et al., 2010; Jackson et al., 2013).
Increased variability of RT has often been reported in ADHD (e.g., Castellanos & Tannock, 2002; Leth-Steensen, Elbaz, & Douglas, 2000; Rubia et al., 2003). We found that premature responses also showed an increased temporal variability in ADHD, suggesting that very early responses were frequent in children with ADHD and not just premature responses immediately prior to the target. This indicates that the problem is not only one of precision timing but a poor control in maintaining response inhibition even in early portions of the foreperiod, whether the exact timing of the target is known.
When the foreperiod was highly unpredictable, all groups showed faster RTs in trials with longer delay, the well-known delay-dependent speeding effect (Naatanen, 1970). This effect is thought to be due to a reduction in temporal uncertainty or an increase in target anticipation as a trial progresses. Both patient groups showed a larger delay-dependent speeding effect than controls. This may reflect an increased anticipation effect in patients either because of emotional or motor factors. This will have to be explored systematically.
Children with ADHD can show difficulties in error processing including a poorer detection and autonomic sensitivity to errors (O’Connell et al., 2009; van Meel, Heslenfeld, Oosterlaan, & Sergeant, 2007). However, all groups reacted similarly to the feedback signaling a premature response by slowing their response in the following trial, suggesting that all groups noticed the feedback to a similar degree. Moreover, all groups showed an improved performance with practice in the fixed foreperiod task. The results may still reflect a different valuation of errors in children with ADHD. In our task, the high stimulation rate, the brief foreperiod, and the feedback on RT were designed to induce an incentive toward fast responses. Premature responses may be linked to priority management, reflecting an urge to respond early in the trial at the expense of avoiding premature responses. Quick response timing often involves a fast increase in motor excitability and a probabilistic decision on the release of the response based on approximate relative cost/benefit analyses. ADHD can bias action toward rapid responses (Sonuga-Barke et al., 1992) even when participants are instructed to favor accuracy (Mulder et al., 2010). Many factors could be contributing to this bias toward speed. ADHD has been linked to risk neglect in betting decisions (DeVito et al., 2008; Luman, Oosterlaan, Knol, & Sergeant, 2008). In the present task, the goal was to obtain a low RT but to avoid zero as RT that signaled premature responding. The increase in premature responses observed here may be linked to a risk evaluation bias in patients with ADHD who may be less inclined to avoid very fast responses than other groups. Future work should evaluate the effects of different penalties associated with premature responses or different rewards associated with temporal precision to help understand the sources of premature responses in ADHD.
In children with ADHD, clinical impulsivity is often linked to difficulty in waiting for one’s turn and interruptions. The links between these behavioral symptoms and waiting to initiate a prepared motor response at the appropriate time is probably complex. The urge to initiate an action may vary with numerous factors including risk-benefit evaluation, time constraints, and social factors. Impulsivity also often refers to frequent changes in goals, poor anticipation of consequences, and general excitability that may be less related to a difficulty in waiting to respond. The development of objective measures of waiting to respond should help inform neuroscience-based models of impulsivity.
The TS group was often slower than the TS + ADHD group. As mentioned before, in TS years of training trying to inhibit tics may have facilitated cognitive control processes aimed at compensating for reduced ICI (Heise et al., 2010; Jackson et al., 2013). These control processes may slow responses in children with TS without ADHD but may be canceled by ADHD neuropathology. Children with ADHD also showed more frequent slow responses in our task as is often observed with other tasks. These may reflect fluctuations in attention or increases in inhibitory control to compensate for a tendency toward premature responses. More work will be needed to shed light on these competing hypotheses.
A number of factors should be considered in evaluating the generality of the present findings. The study did not include patients with ADHD without tics that could potentially differ in some respects to our TS + ADHD group. However, there is evidence from cortical excitability measures that TS + ADHD shows an additive profile compared with groups with TS alone or ADHD alone (Moll et al., 2001). Nevertheless, TS + ADHD often involves OCB and training in tic inhibition strategies. These factors may affect reaction times and premature responses may be more frequent in patients with ADHD without tics. Moreover, some patients were tested under stimulant medication and this may have decreased the group differences, even if there was no significant difference in performance between patients with and without stimulants. Stimulant effects should be systematically tested in conditions inducing frequent highly premature responses to determine if they affect these reactions specifically. Moreover, future work should examine in more detail age differences in the frequency and distribution of premature responses in ADHD to determine their possible link to the evolution of clinical symptoms. Finally, ADHD is probably a heterogeneous disorder and the impairment in response control may vary with sub-phenotypes.
In conclusion, the present data indicate that ADHD is associated with a difficulty in waiting to release a preprogrammed response independently of selecting whether to respond, response timing, or attention to the target.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the Natural Sciences & Engineering Research Council of Canada (NSERC) and the Fonds Québecois de Recherche sur la Société et la Culture (FQRSC).