
Abstract
Children with ADHD are vulnerable to developing conduct problems (CPs), such as antisocial and disruptive behaviors, hostile and defiant behavior, and overt and covert aggression. In particular, children with ADHD often present with oppositional defiant disorder (ODD) or conduct disorder (CD). Comorbidity estimates for ADHD and ODD or CD range from 55% (Barkley, 2006) to 30%-60% (Biederman, 2005). The coexistence of ADHD and comorbid CPs is high in nonreferred community samples and even greater in populations referred for treatment (Connor & Doerfler, 2008). Boys have higher rates of comorbid ADHD/ODD or CD than girls do (Kutcher et al., 2004).
Individuals with ADHD and comorbid mental disorders exhibit greater symptom severity and impairment than individuals who do not experience a co-occurring disorder (Pliszka, Carlson, & Swanson, 1999). For example, children with comorbid ADHD/CPs have more intense ADHD symptoms (Waschbusch, 2002), with more pronounced neurocognitive deficits (Moffitt, 1990) than children with ADHD alone. In comparison with children with ADHD alone, hyperactive and impulsive features tend to persist longer across development for children with ADHD and comorbid CPs (Biederman, Petty, Clarke, Lomedico, & Faraone, 2011; Tandon, Si, & Luby, 2011).
Among children diagnosed with CPs, those children with comorbid ADHD exhibit greater CP impairment and symptomatology than children with CPs alone. Children with comorbid ADHD/CPs have more severe ODD and CD across all age groups. Moreover, behavioral features of these disruptive behavior syndromes develop earlier (Lynam, 1996; Waschbusch, 2002) and persist longer (Odgers et al., 2007; Odgers et al., 2008) in children with the comorbid presentation. Finally, compared with children with CPs alone, children with comorbid ADHD/CPs exhibit more severe features of juvenile delinquency at a younger age (Sibley et al., 2011).
Across development, ADHD behaviors typically precede the onset of CPs and not vice versa (Thapar, van den Bree, Fowler, Langley, & Whittinger, 2006). We present an integrative developmental psychopathology analysis of the development of CPs in children with ADHD, illustrating the dynamic interaction between some important variables that increase the risk that CPs will develop among children with ADHD. Genetically based neurodevelopmental ADHD impairment is associated with subtle but critical skill deficits as well as genetically based features related to ODD and CD. These deficits might interact with environmental risk factors to portend the development of CPs or contribute to coercive parent–child interactions that further exacerbate faulty development. In addition, weak executive functions, particularly verbal working memory, may compound parent/child conflict. Finally, the manner in which parenting stress and attributions for parent/child conflict exacerbate this dynamic is considered. The analysis reveals the transactional impact of genetics, neurodevelopmental skill deficits, coercive interactions, and parent stress and attributions.
Diagnostic labels for ADHD have changed over time and labels for disruptive behavior disorders vary across time and culture. For this analysis, “ADHD” is a term encompassing all variations of the nomenclature. If research specifically describes participants as having ODD or CD, then those terms are used. Otherwise, consistent with precedent established by Lynam (1996) and Waschbusch (2002), the analysis uses the phrase “Conduct Problems” to encompass the wide array of terms indicating disruptive behavior disorder, excluding ADHD.
Genetic Risk Factors
Heritable and genetic factors may be useful to help explain the heterogeneity found in ADHD, including symptom severity and comorbidity. Genetic risk factors may then interact with adverse environments across development to facilitate the expression of at-risk behaviors. The combination of ADHD with CPs has been shown to be more strongly familial than ADHD alone (Faraone, Biederman, & Monuteaux, 2000) and more heritable (Thapar, Harrington, & McGuffin, 2001).
ADHD and CPs
Common genetic factors in part account for the covariation between ADHD and antisocial behavior. For example, a meta-analysis of 51 twin and adoption studies conducted to estimate the magnitude of genetic and environmental influences on CP behavior revealed moderate proportions of variance due to genetic influences (0.41), shared environmental influences (0.16), and nonshared environmental influences (0.43; Rhee & Waldman, 2002). Shared environmental factors (e.g., poverty) affect all family members. Nonshared environmental factors are unique to the individual (e.g., experiencing physical or sexual abuse). In a study of CD, the results of behavior genetic modeling suggest that although the nonaggressive and aggressive domains of CD are influenced by both environmental and genetic influences, a large percentage (61%) of the covariation between CD types (aggressive and nonaggressive) was due to genetic factors (Gelhorn et al., 2006). In a sample of 1,219 twin pairs, aged 9 to 10 years, a latent externalizing behavior factor was found to explain the covariance among ADHD, ODD, and CD symptoms. Genetic influences explained 57% of the variance in this externalizing behavior factor (Tuvblad, Zheng, Raine, & Baker, 2009). In another study of child twins examining the heritability and comorbidity of ADHD, CD, and ODD, structural equation model fitting revealed that heritabilities were substantial: 0.82 for ADHD, 0.74 for CD, and 0.61 for ODD (Coolidge, Thede, & Young, 2000). In a meta-analysis examining whether there is evidence that CPs could be parsed between aggressive and rule-breaking forms of CP behaviors, results showed that aggressive CP behavior was highly heritable (genetic factors accounting for 65% of the variance) and rule-breaking CP behavior contained both genetic influences (48% of the variance) and also shared environmental effects (18% of the variance; Burt, 2009). Studies in clinical samples show that aggression in ADHD children is mostly reactive aggression which is an angry, frustrated response to real or perceived threat or frustration in goal-directed behaviors (Connor, Chartier, Preen, & Kaplan, 2010). Longitudinal analyses of twin data show that continuity across development in reactive aggression is explained by both genetic (48%) and environmental (52%) influences (Tuvblad, Raine, Zheng, & Baker, 2009). Thus, in addition to common environmental risk factors exacerbating risk for CPs, aggression, ODD symptoms, and CD problems in ADHD children, these studies suggest a substantial genetic influence on these behaviors.
Associated Traits
In addition to CP behaviors, many other behavioral and personality traits commonly occur in individuals with ADHD. These traits include impulsivity, novelty seeking, specific types of aggression, and emotion regulation problems. Except for impulsivity, these traits are not part of the ADHD symptom domain, yet may frequently occur in individuals with ADHD and/or CPs. All of these traits have substantial genetic effects on expression of their behavioral trait phenotype.
Impulsivity is a behavioral trait of key importance in CP behavior and ADHD. Impulsivity is a multidimensional trait with both cognitive and behavioral dimensions. The dimensions include a sense of urgency, lack of planning, lack of persistence, and novelty or sensation seeking. A meta-analysis of 41 twin, family, and adoption studies shows that about half the variance in impulsivity is explained by genetic factors (Bezdjian, Baker, & Tuvblad, 2011).
Novelty seeking is a behavioral trait with elements of frequent high risk-taking behaviors, exploration, and sensation seeking. These traits are characteristic of adolescents and found in children with externalizing behaviors such as ADHD, and in CD. In the context of a developmental analysis and the features of ADHD/CP described above, it is important to note that novelty seeking emerges at an earlier age in children with comorbid ADHD/CP, whereas it is somewhat typical to see these traits in adolescents. Twin and adoption studies reveal a large genetic component to novelty seeking as a personality trait with an association found between dopamine neurotransmission and novelty seeking (Nemoda, Szekely, & Sasvari-Szekely, 2011).
Aggression has a large heritable component that varies depending on the type of aggression investigated. Proactive aggression is planned behavior with low emotional and sympathetic nervous system arousal. Reward contingencies drive this form of aggression. Proactive aggression has a large genetic component with 85% of the variance explained by genetic factors. The presence of callous-unemotional traits designates a subgroup of CP children with a more severe aggressive and stable pattern of CP behavior along with a specific neurocognitive profile indicative of affective processing deficits. This subgroup shows strong heritability even after controlling for hyperactive-impulsive behaviors, with a heritability estimate of 0.71 (Viding, Jones, Frick, Moffitt, & Plomin, 2008). In contrast, reactive aggression appears mediated by both genetic and environmental factors (see above). Relational aggression involves social manipulation such as gossip and peer exclusion which is considered an indirect form of aggression (Crick & Grotpeter, 1995). Relational aggression has both genetic and environmental influences. In boys, relational aggression appears explained by genetic factors (42%) and environmental factors (22%). In girls, 21% of the variance is explained by genetic factors with 46% explained by environmental factors (Tuvblad & Baker, 2011).
Deficient emotion self-regulation is a characteristic of many children with externalizing behavior disorders. Difficulties with emotion regulation may lead to reactive aggression and temper tantrums. This deficit in emotional self-regulation may have heritable components (Biederman et al., 2012).
Overall, there is strong evidence that behaviors and personality traits like impulsivity, novelty seeking, and aggression have substantial genetic components. Children with comorbid ADHD/CPs frequently exhibit these behaviors and personality traits.
Candidate Genes and Behavioral Outcomes
Heritability defines the proportion of the variance across certain phenotypes such as ADHD + ODD/CD that is explained by genetic factors, and is estimated by comparing the concordance rates of monozygotic (100% shared genes) and dizygotic (50% shared genes) twins (Nemoda et al., 2011). Two methods are currently used to identify the specific candidate genes accounting for heritability. The first technique aims to identify specific chromosomal regions that relate to the disorder in question by analyzing the whole genome. Genome-wide association studies are an example of whole-genome searches. Candidate gene analysis is a second technique that seeks to identify genetic variants of specific protein-coding genes thought to be of importance for the disorder being studied. In ADHD, CD, antisocial behavior and criminality, and aggression, these techniques have led to a focus on polymorphisms in the monoamine (dopamine, serotonin, and norepinephrine) receptor and transporter genes (Caspi et al., 2002; Nemoda et al., 2011; Retz & Rosler, 2009).
So, what might be inherited? Table 1 identifies candidate genes with risk alleles (polymorphisms) associated with outcomes such as impulsivity, aggression, novelty seeking, hyperactivity, CP behaviors, and externalizing behaviors of interest in ADHD individuals who exhibit CP behavior.
Candidate Genes With Risk Alleles Associated With Outcomes of Interest for ADHD and Disruptive Behavioral Symptoms.

Note. CNS = central nervous system; CP = conduct problem; G × E is gene-by-environmental interaction; G × G is gene-by-gene interaction; DA = dopamine; NE = norepinephrine; Epi = epinephrine; 5HT = 5-hydroxytryptamine (serotonin).
Most of these candidate genes code for proteins important for monoaminergic neurotransmission in the central nervous system (CNS). To date, nearly two-dozen candidate genes important for CPs and ADHD have been identified in human and animal studies (Niv & Baker, 2013).
Gene by Environment Interaction
Many of these risk alleles express their phenotypic properties most strongly in certain environments. In other words, genes are not destiny. The influence of genetic factors in ADHD and CPs, oppositional behaviors, and aggression has repeatedly been shown to vary across different environmental conditions and is referred to as gene-by-environmental interaction (Niv & Baker, 2013). Table 2 presents some of these gene-by-environmental interactions in ADHD and disruptive behavior problems.
Examples of Gene-by-Environment Interaction in Children With ADHD and/or Disruptive Behavior Problems.
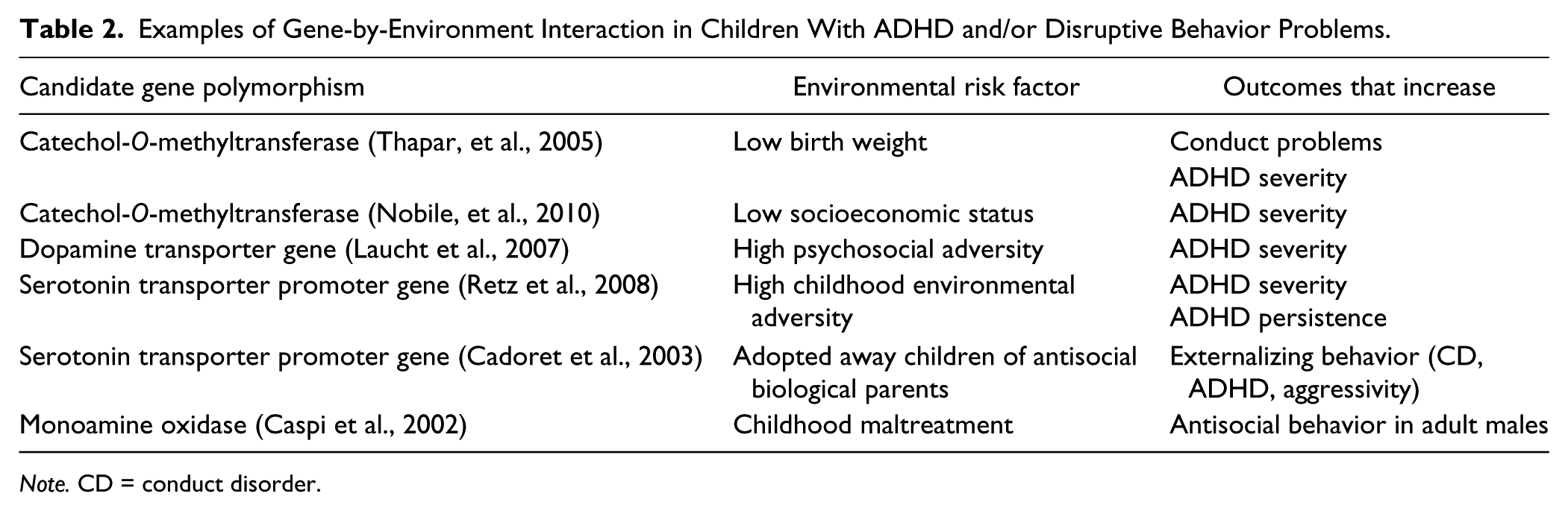
Note. CD = conduct disorder.
Catechol-O-methyltransferase (COMT) is an enzyme that functions to metabolize catecholamines such as norepinephrine and dopamine in the CNS prefrontal cortex. In a study of ADHD children, early onset CP behavior was predicted by a specific COMT gene variant such that those ADHD children possessing the COMT variant were more susceptible to the adverse effects of low birth weight in terms of developing eventual CP (Thapar et al., 2005). In other words, the genetic risk expressed itself most strongly in an adverse environment characterized by low birth weight and not in other types of environments. In another study, ADHD adolescents with a polymorphism in the dopamine transporter gene (important for dopamine neurotransmission in the prefrontal cortex) who grew up in an environment characterized by more psychosocial adversity exhibited significantly more severe ADHD symptoms than adolescents with other genotypes or who lived in less adverse family conditions (Laucht et al., 2007). The serotonin transporter promoter gene codes for proteins that help regulate serotonin uptake from the neuronal synaptic cleft after serotonin neuronal transmission. Serotonin is an important neurotransmitter that is associated with mood regulation, impulse control, and inhibition. A study investigating ADHD children found that risk alleles in the serotonin transporter promoter gene interact with childhood environments high in adversity to predict ADHD severity and persistence across development (Retz et al., 2008). In a fourth gene-by-environment example, a functional polymorphism in the gene encoding the neurotransmitter-metabolizing enzyme monoamine oxidase A (MAOA) was found to moderate the effects of child maltreatment. Abused and maltreated male children with a genotype conferring high levels of MAOA expression were less likely to develop eventual antisocial problems as adults (Caspi et al., 2002).
As these examples show, behavior is not solely or uniquely determined by one’s genome. Genetics is not deterministic. However, the mean heritability estimate for ADHD is 76% (Faraone & Mick, 2010) making it among the most heritable of psychiatric disorders, and about half of the variance in CP behavior and aggression appears determined by genes that encode for proteins associated with CNS monoaminergic neurotransmission (Tuvblad & Baker, 2011). Gene-by-environment research is beginning to reveal that risk genes phenotypically express themselves most powerfully in certain adverse environments, which helps explain why some children are differentially sensitive to certain environmental insults and risks. Thus, the presence of certain risk genes and a developmental experience characterized by certain types of environments and not others may help to explain in part why some ADHD children develop CPs and others do not.
Psychosocial and Cognitive Processes
Generally, 4 years pass between the diagnosis of ADHD and the onset of disruptive behavior disorders (Biederman, Mick, Faraone, & Burback, 2001). How might ADHD, a genetically influenced neurological disorder that precedes the onset of ODD, develop to include ODD and perhaps CD, which involve problem behaviors that are often learned? An analysis of some psychosocial and cognitive processes shows how genetic risk factors, coercive processes, impaired executive function, and parent stress and attributions interact to facilitate the development of CPs among children with ADHD. The analysis focuses on the transition from ADHD alone to the initial comorbid CP onset, which could be ODD or CD. The article is not exhaustive and we acknowledge additional risks that are beyond the scope of this analysis, including other physiological processes (e.g., low autonomic nervous system arousal) and in-utero exposure to toxins and diseased pre-natal environments, as well as parent psychopathology, including adult ADHD, substance abuse, antisocial personality disorder, and depression. Socioeconomic status (SES), parent conflict, age of mother, individual differences in socioemotional competence, the child’s early school failure, and peer rejection and conflict related to ADHD could either individually or in concert further exacerbate the processes reviewed here.
Coercion
An analysis of coercive interactions examines behavior in the context of molecular, minute-by-minute environmental contingencies that reinforce the development and maintenance of behavior patterns. There is a body of literature implicating the role of coercion in the development of CPs among children with ADHD. Patterson’s analysis of coercive interaction among aggressive children (Granic & Patterson, 2006; Patterson, 1976, 1982) is applicable to ADHD behavior. While acknowledging substantial diagnostic overlap between ADHD and CP behavior, this analysis addresses the functionally adaptive features of ADHD and CP behavior separately.
The negative reinforcement paradigm is central to Patterson’s coercion analysis. Negative reinforcement is a process whereby a child or parent response functions to allow them to avoid or escape an aversive stimulus. Because of this contingency, the response is strengthened. For example, in lax parenting, (a) a parent may present a direction (parent antecedent), (b) the child may defiantly yell (child response), and (c) the parent may acquiesce or withdraw the direction (parent consequence). In this case, defiant child yelling is strengthened because it functions to allow the child to avoid doing the task described in the direction. In an analysis of parent behavior, (a) the child may defiantly yell (child antecedent), and (b) the parent may acquiesce or withdraw the direction (parent response), after which the child ceases to yell (child consequence). In this case, parent acquiescence is strengthened because it allows the parent to escape defiant child yelling.
Coercion and ADHD
Children with ADHD and their parents present a high rate of behavior that is aversive to the other party, and the discontinuation of this aversive behavior may reinforce any response that leads to its cessation. These parent–child interactions are inherently primed with features conducive to coercion. Direct observation of interactions between parents and their ADHD children has long suggested that parents of children with ADHD give frequent attention to overactive and impulsive behaviors. Repeated commands and verbal reprimands are common. Parents also give fewer rewards for compliance and generally attend less to appropriate behavior. The aversive properties of the hyperactive behavior may generalize to the child himself or herself, as parents tend to ignore children with ADHD behavior when they behave well. These parent–child interaction patterns are found in preschool ages, middle childhood ages, and into adolescence, and remain stable over development in families that have children with hyperactive behavior. Chronic, intense ADHD can set the occasion for parents to acquiesce more readily (Chronis-Tuscano et al., 2011; Danforth, Barkley, & Stokes, 1991; DuPaul, McGoey, Eckert, & VanBrakle, 2001; Rogers, Wiener, Marton, & Tannock, 2009).
A separate body of direct observation research suggests that the administration of an efficacious ADHD medication regime can weaken coercive parenting styles in families of children with ADHD. Improved attention, decreased hyperactivity, impulsivity, and noncompliance following the administration of stimulant medication serve to modify the way parents respond to their children with ADHD. Following the administration of efficacious medication, parents reduce the number of commands presented, thereby reducing the opportunity for defiant behavior to be reinforced by the withdrawal of commands. When medication is efficacious, parents are less likely to respond to children with aversive controlling strategies. The implication is that the coercive methods used by parents in an attempt to control ADHD behavior, and in reaction to ADHD behavior, may be a function, in part, of the child’s disruptive, noncompliant behavior and relentless motor hyperactivity, and when that behavior is attenuated, coercive parent behavior also attenuates (Danforth et al., 1991).
Parent training for children with ADHD is an evidence-based treatment (Pelham & Fabiano, 2008). Components of this treatment include teaching parents to present clear instructions about chores and required activities, command/instructions presented in the imperative form (not interrogative) that do not signal impending parent acquiescence, praise, reprimands that do not escalate into harsh interactions, and discipline (e.g., time-out) that does not allow the child to escape from the command/ instruction. Among mother’s with ADHD who participated in such successful parent training programs, observed improvements in child behavior were mediated primarily by decreases in mother’s negative behavior during free play and homework completion with their children (Chronis-Tuscano et al., 2011).
Coercion and comorbid ADHD/CPs
It seems natural that one outcome of genetically influenced ADHD behavior would include the development of learned coercive interactions between parent and child. The role of coercion in the development of CPs in children with ADHD has been studied in observational research that compares families of children with ADHD alone, families of children with comorbid ADHD/CPs, and control families. The data support the relevance of coercion in the development of CPs in children with ADHD (Johnston & Mash, 2001). As expected, children with comorbid ADHD/CP had higher levels of misbehavior and their interactions with parents were more conflictual. Generally, mothers of comorbid ADHD/CP children were the least rewarding and consistent, and the most directive, negative, and rejecting.
Rating scales of parenting behavior may assess lax and over-reactive parenting styles. Lax parenting includes excessive permissiveness and inconsistent follow-through after parent directives and after parents warn of impending disciplinary consequences. Over-reactive parenting includes harsh parenting. Although the two styles seem incompatible, research suggests that parents of children with ADHD often use both styles. Harvey, Danforth, Ulaszek, and Eberhardt (2001) examined the validity of the Parenting Scale (Arnold, O’Leary, Wolff, & Acker, 1993) with families of children with ADHD. Parents of children with comorbid ADHD/CPs were more likely to use both lax and harsh parenting compared with families of children with pure ADHD and families of control children. Keown and Woodward (2002) showed that over-reactive parenting influences the extent of child CPs among boys with ADHD. This study also found that boys whose mothers used lax parenting were twice as likely to be hyperactive.
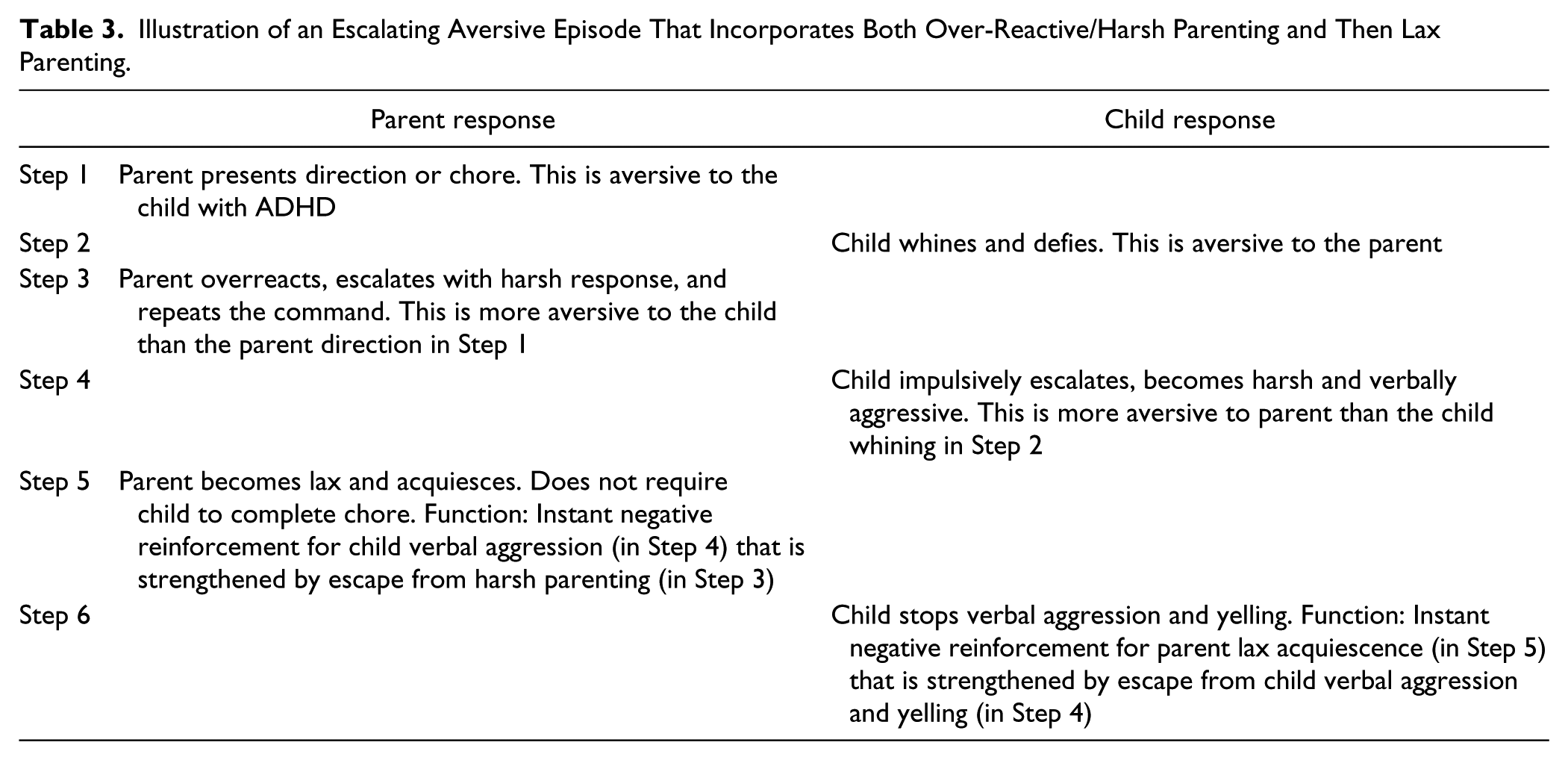
Table 3 exemplifies a simple escalating parent–child interaction incorporating first over-reactive/harsh parenting and then lax parenting. Note how reinforcement is immediate for both parent and child behavior. Children with comorbid ADHD/ODD are particularly sensitive to this process (Luman et al., 2009). Note also that as more severe child misbehavior and over-reactive harsh parenting are introduced into the interaction and then withdrawn, the strength of learning is enhanced because the strength of reinforcement is a function of the magnitude of reduction of aversive stimuli; the more aversive the event, the more reinforcing the termination of that event. At first, the parent overreacts harshly (Step 3), but when parent acquiesces in Step 5, escape from the child’s harsh verbal aggression (Step 4) is stronger reinforcement than escape from whining defiance (Step 2). When the child becomes verbally aggressive in Step 4, escape from over-reactive harsh parenting (Step 3) is stronger reinforcement than escape from a simple direction (Step 1).
Illustration of an Escalating Aversive Episode That Incorporates Both Over-Reactive/Harsh Parenting and Then Lax Parenting.
Parent nonresponsiveness and over-reactivity are more pronounced in families of children with comorbid ADHD/ODD (Seipp & Johnston, 2005). Furthermore, poor parent limit setting (i.e., lax parenting) may prevent the development of internal self-control by children with ADHD (Campbell, 1990), consistent with the conceptualization of self-control in children with ADHD (Barkley, 1997a) that is reviewed next. Clinical parent training outcome data with families of children with comorbid ADHD/ODD find that after successful parent training, both over-reactive and lax parenting are reduced (Danforth, 2007). This may account for some declines in child disobedience and hyperactivity.
The role of coercion in the development of CPs among children with ADHD has been examined by Patterson and colleagues. In a study that used structural equation modeling, Patterson, DeGarmo, and Knutson (2000) hypothesized that ADHD represents the first stage in the development of CPs, and antisocial behavior a second stage, with coercion serving as a shared mechanism. Participants included 206 families with their fourth-grade boys. First, a path coefficient showed that hyperactive and CPs were significantly related (yet discriminable). This path became nonsignificant when coercion was entered as a third variable that both hyperactivity and CPs shared, indicating that coercion accounted for most of the variance in the development from hyperactive behavior to CPs. Patterson et al. (2000) contended that “the control of contingencies by parenting practices is the most proximal mechanism controlling the child negative outcomes from infancy through elementary grades” (p. 103). In a review of functional assessment research of ADHD behavior, DuPaul and Ervin (1996) acknowledged biological factors associated with ADHD, individual differences, and the role that adult and peer attention may have in reinforcing ADHD behavior, but they concluded, The most likely function of ADHD behaviors is to avoid and/or escape task demands. The latter may include directives from a parent to complete a chore or homework as well as instructions from a teacher to work on an academic assignment. (p. 614)
Avoidance of work requiring sustained mental effort remains a defining symptom of ADHD.
As part of an analysis of reciprocal relationships between parenting behavior and the development of disruptive behavior, Burke, Pardini, and Loeber (2008) made an important point that parenting behavior might be more influenced by ODD than CD. ODD symptoms such as negativistic, defiant, disobedient, and hostile behavior toward authority figures “introduces direct, intense, and emotional conflict into the parent/child relationship whereas the conflict presented by CD is relatively more distant, often introduced into the relationship by community intermediaries such as school and police” (p. 680). In their study, boys aged 7 to 12 years were followed for 10 years. Among children with ADHD, timid discipline was the more significant of two variables that predicted ODD. Furthermore, ODD presented as the only significant predictor of timid discipline, “indicating a reciprocally influential relationship.” From year-to-year, parents who were reluctant to discipline even moderate misbehavior such as crying, whining, and complaining had children whose ODD symptoms increased the following year. Parenting behaviors such as these are evident when children are very young, suggesting that coercive processes may have a greater influence over the initial development of CPs when children are younger, compared with association with deviant peer group and poor parental supervision that have greater impact during adolescent development.
Genetically influenced ADHD behavior introduced early into the parent–child interaction, when the child is young, potentiates the developmental of CPs in children with ADHD. The symptoms of ADHD may be aversive to parents, thus potentiating both harsh responses to the child and lax acquiescence that allows the parent to escape conflict. These factors, which are found less often in typical parent/child dyads where ADHD is absent, may contribute to the escalated rate of development of CPs in children with ADHD.
The Role of Impaired Self-Regulation
The phenotypic expression of genetically influenced ADHD can take many developmental forms and expressions. A theory of ADHD, Barkley’s model of self-regulation, exemplifies one phenotypic developmental process that could interplay with coercive processes to potentiate the development of CPs. Barkley’s theory of ADHD informs the present analysis (Barkley, 1997a, 1997b, 2001).
Deficiencies in behavioral inhibition
Neurophysiological infirmity in the prefrontal cortex is associated with the fundamental impairment in ADHD: a delay in the development of response inhibition. In simple terms, Barkley’s model of ADHD has seven parts. (a) The essential deficit in children with ADHD is a neurologically based impairment in behavioral inhibition that is associated with (b) poor self-control. The deficit in behavioral inhibition, in turn, interferes with the performance of four interrelated executive functions: (c) nonverbal working memory, (d) verbal working memory, (e) self-regulation of emotion, and (f) planning. These executive functions are the fundamental self-directed actions the child uses to help self-regulate behavior. As a result, (g) motor action is overwhelmingly influenced by the immediate environment rather than past experience and future-oriented goals. This analysis focuses on the impaired verbal working memory executive function.
During normal development, behavioral inhibition allows for a delay between preceding or concurrent stimulus events (the setting and antecedent events) and a child’s response. The delay in responding allows the child to perform acts of “self-control” or “self-regulation” that can influence persistent goal-directed behavior. “In that sense, inhibition permits, supports, and protects the executive functions” (Barkley, 1997a, p. 51).
The fundamental failure of response inhibition in children with ADHD prevents a necessary delay and buffer between the child’s response and the overwhelming influence of events that immediately precede (antecedents) and follow (consequences) the response. There is a short latency between the environmental events and a child’s response. A child’s quick response limits the opportunity for self-directed behavior, characterized as executive functions, which regulates behavior directed toward the future. These executive functions are diminished in children with ADHD because the primary deficit, failure of response inhibition, interferes with the implementation of the executive functions. Thus, the executive functions are not impaired, but rather rendered less effective by the deficient behavioral inhibition.
Verbal working memory
Verbal working memory is one of the executive functions impaired by the failure of response inhibition. Verbal working memory is the internal representation of speech or private speech. Such self-directed speech is important to the development of self-control and subsequent control of motor behavior. For example, prior to responding to an antecedent event, self-directed private speech facilitates quiet and calm thinking describing the event and perhaps reflecting upon similar past events and their outcomes. Private speech also enables language-based self-questioning inherent to problem solving that in turn serves as a means to generate rules.
A private rule of the form we are speaking of in verbal working memory might have significant positive impact over the overt behavior in typical children, but seems to have less impact on the overt behavior of children with ADHD. For children with ADHD, the impairment in behavioral inhibition blocks the verbal working memory component of executive function, and this leads to delays in the development of rule-governed behavior, particularly that controlled by self-speech. The outcome is diminished internalized speech with less effective description of and reflection on the extant contingencies, and motor response less influenced by such self-description and reflection, with inadequate problem solving in the context of immediate dilemmas.
The issue of time is relevant. An advantage of the rule-governed behavior component of verbal working memory is that the description of the contingency (event/response/outcome) provided by the internal self-rule helps the child bridge the gap between current behavior and delayed outcomes. Rather than being influenced by the immediate context, self-rules allow a typical child to behave toward future goals. Lacking this, immediate rewards unduly influence the child with ADHD, including rewards for misbehavior. Recall that negative reinforcement within a coercive process is typically reinforced immediately.
Failure of behavioral inhibition prevents effective use of self-directed speech
ODD typically includes a learned defiant refusal to follow directions presented by parents and others. Over the course of development, this defiance is juxtaposed with neurological impairment that leads to inherent failure to follow parent and self-directed speech. These factors exacerbate the risks posed by genetic predisposition. Children with ADHD are unlikely to master control of their behavior by self-directed private speech, thus requiring control by the language of others. However, coercive family processes make it unlikely that parental directives will be followed by the child.
Barkley attributes the failure of self-speech to influence the pertinent overt nonverbal behavior of the child to neurological deficits. In addition to the neurological deficit, our analysis suggests that parent reaction to their child’s ADHD further exacerbates the inherent failure to develop effective self-speech for behavioral self-control.
Parents may not condition self-directed speech
Influenced by an array of theorists who studied the relationship between language and behavior, Barkley postulates that during the development of typical children, language’s influence on behavior occurs in three stages. First, the language of others controls a child’s behavior. Then, the child’s parents and teachers progressively teach the child to control his or her own behavior by self-directed and subsequently private speech. Finally, the child’s self-directed questions lead to the creation of new rules by the child that come to control his or her motor behavior. The influence of language over behavior is a developmental progression from control of language by others to control by self-directed speech.
Over the course of development, parent reaction to ADHD behavior is incompatible with effective parenting that teaches a child to control his or her behavior with self-directed speech. Effective self-directed speech might be further abrogated in children with hyperactive behavior because adults in their environment seem less likely to provide the context to condition or shape self-directed speech, thereby increasing the risk for CP behavior. As noted above, a child’s hyperactive behavior may be aversive to adults in whose presence such behavior frequently occurs. When children with hyperactive behavior are well behaved and likely to attend, their parents give fewer rewards for compliance, initiate fewer verbal interactions, and attend less to appropriate behavior and vocalizations initiated by the child. Children with hyperactive behavior often have family environments that are different from the environment of typical children. When children with ADHD are well behaved and perhaps prone to attend, adults in their environment are less likely to question them about past, present, or future behavior, or the variables and contingencies of which their behavior is a function. Parents are far more likely to engage them when they are particularly overactive and disruptive, but the children do not seem prone to attend when overactive (i.e., when the child is most active, it is not a good teaching moment). Furthermore, compared with families without ADHD children, the form of the interaction when the child is disruptive is more likely to be harsh discipline, not constructive teaching or directed questioning. As such, parents and other adults are less likely to condition or model self-directed speech and self-directed questions. Subsequent analyses illustrate how parent stress and attribution also render it less likely that parents will behave in a manner that effectively teaches self-directed speech critical to the development of nonverbal working memory.
Thus, the essential impairment in behavioral inhibition that prevents effective utilization of self-directed speech is further impaired by adult reaction to ADHD behavior that does not contribute to the development of self-directed speech. The outcome is increased risk for CP behavior.
Parenting Stress
Parenting stress is another risk factor that may influence the development of co-occurring CPs in children with ADHD. This type of stress occurs when a parent’s perception of the demands of parenting exceeds his or her resources to cope with these demands (Deater-Deckard, 1998). Parenting stress is a distinct type of stress that has been shown to play a role in the development of dysfunctional parent–child interactions (Deater-Deckard, 1998; Theule, Wiener, Tannock, & Jenkins, 2013).
Abidin’s (1992, 1995) model has guided much of the research that examined the relationship of parenting stress and child psychopathology. Abidin presented a multifactorial model involving characteristics of both the child and parent. The child domain reflects the stress of parenting a child with difficult characteristics (e.g., “My child turned out to be more of a problem than I had expected.”). The parent domain reflects parental distress related to the parenting role (e.g., “I find myself giving up more of my life to meet my children’s needs than I ever expected.”).
Considering the behaviors that characterize ADHD, it is not surprising that parents of children with this disorder experience significantly higher levels of parenting stress than parents of children in nonclinical comparison samples (Theule et al., 2013). The overall severity of ADHD symptoms has a large effect on the severity of parenting stress (Theule et al., 2013). For example, Anastopoulos, Guevremont, Shelton, and DuPaul (1992) found that children with ADHD report extremely high levels of parenting stress. In this study, the overall severity of the child’s ADHD predicted the level of parenting stress. This relationship has been reported for both hyperactive symptoms (Breen & Barkley, 1988) and inattentive/distractible symptoms (Podolski & Nigg, 2001). Children with comorbid ADHD/CPs have more intense ADHD symptoms and the combination of ADHD symptoms with oppositional defiant, aggressive, or other externalizing behavior has an even greater impact on parenting stress (Anastopoulos et al., 1992; Baker, 1994; Goldstein, Harvey, & Friedman-Weieneth, 2007; Podolski & Nigg, 2001).
Parenting stress is important in the present analysis because a higher level of stress is associated with poorer parenting behavior. More specifically, “parents who report high levels of parenting stress are more likely to be authoritarian, harsh, and negative in their parenting” (Deater-Deckard, 1998, p. 318). Moreover, parents who report high levels of parenting stress tend to be less involved and are less likely to interact with their children (Deater-Deckard, 1998). For example, in a sample of low SES mothers who were considered to be “at risk” for child abuse, Adamakos et al. (1986) found that high parenting stress mothers who received little social support provided significantly less stimulation to their 2-year-old children. As noted earlier, harsh punishment, coupled with inattention and lack of reinforcement for appropriate or prosocial behavior, increases the risk for escalation of a pattern of coercive behavior between parent and child (Granic & Patterson, 2006; Patterson, 1982). Furthermore, when parents are harsh or less involved with and interact less with their children, they are less likely to engage in conversation that teaches the child the parameters of self-directed speech that is important in the development of verbal working memory and self-control. This further compromises a neurophysiological weakness in executive function and limits the influence of distal consequences and language-based problem solving. Finally, genetic risk is expressed most strongly in environments characterized by psychosocial adversity that intensify stress, adding further to the cyclical impact on the development of CPs among children with ADHD.
Parenting stress also can affect the efficacy of parent training interventions designed to reduce children’s behavioral problems. In an evaluation of an evidence-based treatment for children’s CPs, Kazdin (1995) reported that parental stress was related to children’s levels of deviant behavior and prosocial functioning at the end of treatment.
Parental Attributions
A child’s impulsive, hyperactive, and inattentive behaviors are associated with increased parenting stress, but research also shows that parents’ interpretation of the child’s behavior influences the parents’ reactions to these negative behaviors (Bugental & Johnston, 2000; Johnston & Ohan, 2005). There is strong evidence that parents are more distressed by their child’s misbehavior if they believe that their child is intentionally misbehaving or if they believe that their child is capable of behaving differently (Miller, 1995).
Parental attributions have an effect that extends beyond parents’ emotional reactions. Research has shown that parental attributions about their child’s misbehavior are also linked to parenting behaviors (Bugental & Johnston, 2000; Johnston & Ohan, 2005; Miller, 1995). More specifically, when parents perceive the child’s misbehavior as intentional or willful, they are more likely to use harsh, coercive, or other power assertive discipline strategies. For instance, MacKinnon-Lewis, Lamb, Arbuckle, Baradaran, and Voling (1992) reported that coercive mother–child interactions were more likely to occur when mothers reported negative attributions for their child’s behavior. Even more noteworthy was the finding that the most aggressive interactions were those where both the mother and the child perceive hostile intent in the other’s actions.
There is strong evidence that, in comparison with parents of well-behaved children, parents of children who present with disruptive behavior disorders tend to be more negative about their children (Johnston & Ohan, 2005; Miller, 1995). Moreover, there is evidence “that blame-oriented attributions precede and foster harsher parental tactics” (Bugental & Johnston, 2000, p. 322). These findings raise the concern that parents of children who exhibit difficult-to-manage disruptive behaviors (such as impulsive or oppositional behaviors) have a “child blaming” attributional style, which leads parents to use harsh and coercive, but ineffective, discipline strategies.
Even though ADHD and CP behaviors are characterized by behaviors that parents find distressing and difficult to manage, there are important differences in how parents attribute the causes of these problematic behaviors. Parents of typically developing children tend to attribute the causes of their child’s negative behaviors to external and unstable factors (e.g., “He was angry” or “His friends were with him”; Dix, Ruble, Grusec, & Nixon, 1986; Gretarsson & Gelfand, 1988; Strassberg, 1995). For children with ADHD, both parents and professionals who care for these children tend to view the behaviors characteristic of ADHD as more internally caused, more uncontrollable by the child, and more stable over time (Chen, Seipp, & Johnston, 2008; Collett & Gimpel, 2004; Dryer, Kiernan, & Tyson, 2006; Gerdes & Hoza, 2006; Johnston & Ohan, 2005; Markel & Wiener, 2012). As noted by Chen et al. (2008) and Johnston and Freeman (1997), this pattern of attributions reflects a view of ADHD as a neurobiological disorder, not intentional or willful behavior.
Rather than blaming the child for these ADHD behaviors, parents of children with ADHD tend to view these behaviors as enduring symptoms of an underlying disorder (Saltmarsh, McDougall, & Downey, 2005). Furthermore, because these behaviors are not considered intentional misbehavior, parents tend to respond empathically toward their children (Chen et al., 2008). Despite attributing their child’s ADHD behavior to the underlying disorder, mothers of children with ADHD are still frustrated and upset by their child’s negative behavior (Freeman, Johnston, & Barth, 1997; Johnston & Freeman, 1997). Just as important, these mothers report using harsher, power assertive strategies to manage their child’s behavior than mothers of nonclinical comparison children (Gerdes & Hoza, 2006; Johnston & Freeman, 1997).
There is evidence that parents of children with ADHD distinguish behaviors that characterize ADHD (i.e., impulsive, hyperactive, inattentive behaviors) from oppositional defiant behaviors like arguing, defiance, and oppositional rule violations (Johnston & Patenaude, 1994). This finding is noteworthy because these are important differences in the pattern of parental attributions for ADHD and oppositional defiant behaviors. Parents of children with ADHD tend to perceive oppositional behaviors as more controllable than impulsive behaviors (e.g., Chen et al., 2008; Johnston, Chen, & Ohan, 2006; Johnston & Patenaude, 1994). Unlike impulsive or inattentive behaviors, which many parents consider to be symptoms of a biological disorder, these findings suggest that parents are likely to see oppositional behaviors as more malicious and intentional than the core ADHD behaviors. If parents interpret oppositional behavior as the child’s attempt to manipulate parent–child interactions, they may conclude that oppositional behaviors are more deserving of harsh parenting responses than the core ADHD behaviors (Johnston & Patenaude, 1994).
As noted earlier, there is strong evidence linking biased parental attributions to harsh, coercive, or authoritarian parental behaviors (Bugental & Johnston, 2000). In a study that compared children with comorbid ADHD and oppositional defiant behaviors with children who had ADHD without co-occurring oppositional behavior, Johnston et al. (2006) reported that mothers of children with comorbid ADHD and oppositional defiant behavior provided attributions for their child’s behavior that were more negative than mothers of children with ADHD alone. “These results suggest that negative parent attributions are linked more to the presence of comorbid oppositional behavior than to ADHD alone, although the direction of this relation remains unknown” (Johnston et al., 2006, p. 68).
Overall, there is strong evidence that parents of children with ADHD tend to report negative, blame-oriented attributions for their child’s negative behaviors. Parents tend to view behaviors that are widely acknowledged the core symptoms of ADHD as internally caused, persistent, and not controllable by the child. Even though this pattern of attributions does not lead parents to blame the child for misbehavior, there is strong evidence that parents of children with ADHD often respond to misbehavior with harsh, power assertive strategies. If parents see noncompliant or oppositional defiant behavior as more intentional or willful, they are likely to respond with even harsher discipline tactics, exacerbating the coercive cycle. The research on parental attributions converges with the findings on parenting stress to indicate that parents of children with ADHD are more likely to use harsh and coercive discipline. Parents may view ADHD as immutable, rendering constructive criticism pointless. Conversely, parents may view CP behavior as willful, leading to harsh parenting practices that are intensified if the child has the comorbid presentation (Johnston et al., 2006). Neither style promotes the development of their child’s self-directed speech (and both styles are associated with the development of CPs). For children with ADHD, the most opportune time for parents to present verbal instructions and commands would be when the child is well behaved. However, in these instances, parents of children with ADHD initiate fewer verbal interactions and attend less to the vocalizations of the child. As a result, children with ADHD are less likely to develop self-regulatory skills and more likely to develop oppositional and other disruptive behaviors.
Summary
Children with ADHD often develop CPs. “The rate with which this comorbidity occurs greatly exceeds what would be predicted based on probability estimates derived from the prevalence of each disorder alone” (Newcorn & Halperin, 2000, p. 173). This example of an integrative developmental psychopathology analysis combines various approaches and posits one model of how a limited range of diverse risk factors, including both distal biogenic risk factors and proximal parenting behavior and cognition, operate together to contribute to the development of CPs among children with ADHD. It is apparent that a single cause for the development of CPs is improbable.
The development of CPs and their associated features is influenced in part by genetic, heritable predisposition. Candidate genes that encode for proteins associated with CNS monoaminergic neurotransmission with risk alleles for ADHD and CP behavior are identified. The genetic risk is expressed most strongly in environments characterized by psychological adversity and stress. Neurophysiological impairment in the prefrontal cortex is associated with heritable child behavior characterized by a failure in response inhibition. Impaired response inhibition interferes with executive function, including impaired verbal working memory that limits effective goal-directed future-oriented behavior and enhances the influence of immediate environmental circumstances. Genetic and neurophysiological impairments increase the probabilistic risk for CPs because ADHD symptoms influence the way parents act toward and think about their child. Compared with children without ADHD, children with ADHD not only have a different biological substrate, but intense and relentless ADHD behavior makes it more likely that coercive interactions between the parent(s) and child will occur, or the parent will disengage altogether when the child is well behaved.
These coercive interactions contribute directly to the development of CPs, especially in the early years of life. Coercive parent behavior is incompatible with a parenting style that teaches a child to control his or her behavior with self-directed and eventually private speech. Greater levels of child domain and parent domain stress, and blame-oriented attributions among parents of children with comorbid ADHD/CPs further enhance the risk for harsh parenting and coercive interactions and diminish the likelihood parents will constructively engage in conversation that teaches the child to control his or her behavior with self-directed or private speech. CPs such as ODD include a learned defiant refusal to follow directions presented by parents. Such behavior raises parent stress levels. Defiance, a hallmark of ODD, is the type of behavior parents are likely to consider willful, leading in turn to negative, harsh parenting behavior and less involvement, less interaction, less stimulation, and less warmth that further aggravates coercive processes and further reduces the development of self-directed and private speech that helps the child to control his or her own behavior. Over the course of development, this defiance is juxtaposed with ongoing neurological impairment associated with an inherent failure to follow parent and self-direction, and sensitivity to immediate consequences so apparent in the coercive process. These foibles interact and exacerbate the risks posed by genetic predisposition. Children with comorbid ADHD/CPs not only have different genetic risk factors, but their parents also present with different behavioral and cognitive styles that simultaneously interact in a transactional manner to exacerbate the disruptive behavior of the child, limit the development of verbal working memory, and alter the parent’s emotional and cognitive reaction to the child.
As noted earlier in our discussion of behavioral and cognitive processes, many contributing factors are omitted from this analysis. If the entire range of contributing variables was included in the analysis, there would be scant detail addressing how the variables interact together to contribute to the development of CPs. There are likely numerous pathways to CPs for children with ADHD. Nonetheless, this relatively limited analysis of the impact of genetic and neuropsychological processes, together with distressed parenting and cognition, is a complex nonlinear perspective. The magnitude of the influence of coercion and parenting attribution and stress may be greater in this situation where the young child’s behavior and executive functions are inherently outside the range of typical development. Sometimes referred to as a transactional development of risk factors over time (Dodge & Pettit, 2003), the child’s ADHD temperament and executive function weakness evoke predictable parent behavior, with bi-directional, reciprocal parent–child interaction developing when the child is young and progressing over time until the emergence of CP behavior, which tends to present a younger age in children with the co-occurring disorders. The reciprocal parent–child influences are frequent, many times a day, and proximal to parent and child behavior, excellent features for any learned developmental process, and more so for a child with ADHD (and maybe their ADHD parent). When the child is young, the impact of each parent–child interaction is small, but the transactional outcome is an enduring effect enhanced by each interaction and the chronic nature of ADHD symptomatology.
Footnotes
Acknowledgements
Daniel F. Connor and Leonard A. Doerfler contributed equally to the study. The authors wish to thank Russell A. Barkley for assistance with the conceptualization of behavioral inhibition and self-control.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.