
Abstract
Introduction
Given that in adolescence, parental control diminishes and a need for independence arises (Spear & Kulbok, 2004), planning is an important skill to secure an independent lifestyle (Nurmi, 1991). Ample research shows that planning skills of typically developing adolescents (TDA) increase during adolescence (Anderson, Anderson, Northam, Jacobs, & Catroppa, 2001), but no studies have investigated the planning skills of adolescents with ADHD in detail using multiple measures of planning, and few studies have focused on subtype differences (but Qian, Shuai, Chan, Qian, & Wang, 2013). To investigate planning skills of adolescents with ADHD in more detail, this study assesses planning skills of adolescents with different subtypes of ADHD using a multi-method assessment with both cognitive tasks and parental ratings of planning.
Executive Functions (EFs) play a pivotal role in most theories of ADHD (Barkley, 1997; Sonuga-Barke, 2003; Sonuga-Barke, Bitsakou, & Thompson, 2010). EFs are described as neurocognitive processes that enable self-control (Lezak, 1995). EFs are necessary to maintain an appropriate problem solving set to attain a future goal (Welsh & Pennington, 1988). Individuals with ADHD (mainly based on results of studies with children younger than 12 years) show most problems with the EFs inhibition and working memory (Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). In adolescence, the symptomatology of ADHD changes, as the symptoms of hyperactivity and impulsivity decrease in comparison with childhood (Fischer, Barkley, Smallish, & Fletcher, 2005), and in daily life, problems with the EF planning are described to be more pronounced (Barkley, 2004; Wolraich et al., 2005). Planning is generally defined as the process of formulating a sequence of operations intended to achieve a goal in an organized, strategic, and efficient manner (e.g., Hayes-Roth & Hayes-Roth, 1979).
In adolescence, the control and help of parents and teachers diminishes as compared with childhood, while at the same time, the transition to secondary school increases the need for EFs, particularly for planning skills. For example, in secondary school, adolescents have to change classes and teachers every hour, are expected to be where they are supposed to be on time, and are expected to bring necessary materials for all their classes. Adolescents are expected to independently manage planning for long-term projects, study for tests, and complete and turn-in assignments for multiple classes and teachers on time (Evans et al., 2009). Therefore, it is not surprising that planning aspects of EF are highly predictive of academic functioning in adolescents with ADHD (Langberg, Dvorsky, & Evans, 2013).
Even though planning problems appear to have important consequences for adolescents in particular, studies assessing planning skills in ADHD focusing on the adolescent age are sparse (Gau, Chiu, Shang, Cheng, & Soong, 2009; Gau & Shang, 2010; Qian et al., 2013; Toplak, Bucciarelli, Jain, & Tannock, 2009). Planning problems in adolescents with ADHD have been described on a behavioral level (Barkley, 2004; Wolraich et al., 2005) and by using a parent-rated questionnaire (using the Behavior Rating Inventory of EF: Langberg et al., 2013; Toplak et al., 2009). However, the few studies using neuropsychological measures of planning skills in adolescents with ADHD show mixed results. In three studies, adolescents with ADHD show significantly impaired performance on a neurocognitive measure of planning, the computerized Stockings of Cambridge task of the Cambridge Neuropsychological Test Automated Battery (CANTAB; Gau et al., 2009; Gau & Shang, 2010; Toplak et al., 2009) as compared with TDA. However, in contrast, a recent large study investigating the development of planning skills of children and adolescents using another neurocognitive measure of planning (Tower of Hanoi) showed no significant differences in planning skills between adolescents with ADHD and TDA (Qian et al., 2013). Studies focusing on children younger than 12 years of age show the same contradiction: even though studies predominantly found children with ADHD have impaired planning skills on neurocognitive measures as compared with controls (e.g., Gioia, Isquith, Kenworthy, & Barton, 2002; McCandless & O’Laughlin, 2007; Nigg, Blaskey, Huang-Pollock, & Rappley, 2002; O’Brien, Dowell, Mostofsky, Cenckla, & Mahone, 2010; Shimoni, Engel-Yeger, & Tirosh, 2012; Wodka, Loftis, et al., 2008), some studies did not find these differences (Qian et al., 2013; Riccio, Homack, Jarratt, & Wolfe, 2006; Wodka, Loftis, et al., 2008; Wodka, Mostofsky, et al., 2008).
In addition, there are few studies on subtype differences in planning skills. The only study conducted in an adolescent sample shows no subtype differences in planning skills as assessed by a neurocognitive measure (Qian et al., 2013), whereas studies focusing on subtype differences in planning skills of children younger than 12-year old show inconsistent results. Two studies show that children with the ADHD combined subtype (ADHD-C) showed significantly more planning problems in comparison with the inattentive subtype (ADHD-I; Klorman et al., 1999; Lockwood, Marcotte, & Stern, 2001); other studies did not find significant differences between subtypes (Nigg et al., 2002; Riccio et al., 2006; Salcedo-Marin, Moreno-Granados, Ruiz-Veguilla, & Ferrin, 2013; Wodka, Loftis, et al., 2008; Wodka, Mostofsky, et al., 2008). Different factors may account for these inconsistencies in the literature.
First of all, planning skills go through major developments during late childhood and adolescence and some studies draw conclusions regarding planning skills based on samples with broad age ranges from childhood to adolescence. These studies thereby possibly do not detect differences in planning skills or finding differences that may not be there when focusing on a specific developmental stage (Gioia et al., 2002; Riccio et al., 2006; Salcedo-Marin et al., 2013; Wodka, Loftis, et al., 2008; Wodka, Mostofsky, et al., 2008). Second, studies often use only one task to measure planning. Between these studies, there is a large variability of the measures used, while research shows only small and non-significant correlations between these different measures of planning (Welsh, Satterlee-Cartmell, & Stine, 1999). In addition, these different measures of planning differ greatly in level of ecologic validity (Gau et al., 2009; Gau & Shang, 2010; Gioia et al., 2002; Harrier & DeOrnellas, 2005; Klorman et al., 1999; Kofman, Larson, & Mostofsky, 2008; Lockwood et al., 2001; McCandless & O’Laughlin, 2007; Qian et al., 2013; Salcedo-Marin et al., 2013; Toplak et al., 2009). Ecological validity refers to the extent to which the results of controlled tests generalize to performance in naturalistic settings (Wilson, Alderman, Burgess, Emslie, & Evans, 2003). Whether a neuropsychological task to assess planning skills (low ecologic validity) measures the same construct as a parent-rated questionnaire (high ecologic validity) is debatable (Toplak, West, & Stanovich, 2013). Therefore, to get a clear picture of planning skills of adolescents with ADHD in this specific developmental stage, it may be important to use multiple neuropsychological tests and complement them with questionnaires to get a broad assessment of planning skills.
Given the importance of planning skills for the daily life of adolescents and the planning impairments that are reported within samples of adolescents with ADHD, a broad assessment of planning skills of adolescents with ADHD as compared with adolescents without ADHD is needed. Therefore, the first goal of this study is to assess planning skills of adolescents with ADHD as compared with planning skills of TDAs. To do this, multiple tasks are used that have varying levels of ecological validity. First, neuropsychological tasks are utilized that are proposed to be pure measures of planning but often have relatively low ecologic validity. Second, neuropsychological tasks are used with higher ecologic validity (i.e., are more comparable with daily life situations; Wilson et al., 2003). Finally, in this study, the most ecologically valid assessment of planning skills is the parental rating of daily life planning problems (Langberg et al., 2013; Toplak et al., 2013). Group differences between adolescents with ADHD and TDA are assessed and, in addition, the clinical relevance of results will be assessed by comparing the percentage of adolescents scoring within the clinical range in both groups of adolescents. Based on behavioral descriptions of ADHD in adolescence (Barkley, 2004; Wolraich et al., 2005) and in line with previous research (Gau et al., 2009; Gau & Shang, 2010; Toplak et al., 2009 but Qian et al., 2013), it is hypothesized that compared with TDAs, adolescents with ADHD will show clinically impaired planning skills on all planning measures and thus on all three levels of ecologic validity.
The second goal is investigating subtype differences in planning skills, with focus on differences between ADHD-I and ADHD-C, because the hyperactive/impulsive subtype (ADHD-H) is uncommon during adolescence (Faraone, Biederman, & Mick, 2006). Given that the only study assessing subtype differences within adolescence (with only one neurocognitive measure) showed no significant differences between subtypes (Qian et al., 2013), no differences are expected between the ADHD-C and ADHD-I subtypes (Qian et al., 2013).
Method
Participants
Thirty-four TDAs, 77 adolescents with ADHD-I, and 38 adolescents with ADHD-C participated. The participants met the following inclusion criteria: (a) age range between 12 and 17 years, (b) attending a regular middle or high school, (c) no active non-pharmacological treatment for ADHD or associated symptoms, and (d) IQ above 80, measured by two subtests (Vocabulary and Block Design) of the Dutch Wechsler Intelligence Scale for Children–III (WISC-III; Kort et al., 2005); these two subtests correlate highly with Full Scale IQ (FSIQ; Sattler, 2001). The study was approved by the Ethics Committee of the University of Amsterdam.
Selection of the groups
ADHD group
All adolescents applied for psychosocial treatment at 1 of 16 participating outpatient mental health institutes in the Netherlands. Before receiving treatment, they participated in the current study. All of these adolescents (N = 201) had a prior clinical Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) diagnosis of ADHD. Diagnosis was confirmed by parent versions of the Dutch Disruptive Behavior Disorder (DBD) rating scale (Oosterlaan, Scheres, Antrop, Roeyers, & Sergeant, 2000; Pelham, Gnagy, Greenslade, & Milich, 1992) and the Diagnostic Interview Schedule for Children for DSM-IV (DISC-IV; Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000). The DBD contains four scales composed of the DSM-IV (APA, 1994) criteria for ADHD Inattention, ADHD Hyperactivity/Impulsivity, Oppositional Defiant Disorder, and Conduct Disorder. Adequate psychometric properties have been reported (Oosterlaan et al., 2000). Only adolescents with a clinical score on any of the two ADHD scales of the DBD were included in this study; 47 adolescents did not meet this criterion and were excluded. Also, 15 adolescents were excluded because their parents failed to complete the questionnaires due to technical problems with the questionnaire software.
The DISC-IV, a structured diagnostic interview, establishes ADHD group membership and subtype status based on a diagnostic algorithm, including a check of cross-situational impairment (Shaffer et al., 2000). Only adolescents with an ADHD-I or ADHD-C diagnosis on the DISC-IV were included; 15 adolescents did not reach ADHD criteria and 6 adolescents met criteria for the ADHD-H subtype and were excluded. Another 3 adolescents had an FSIQ below 80 and were excluded from the study. This resulted in an ADHD-I group of 77 and an ADHD-C group of 38 participants. The adolescents with ADHD taking methylphenidate discontinued medication at least 24 hr before testing, allowing for a complete wash out (Paykina & Greenhill, 2007).
TDA group
TDAs were recruited from a community school in the Netherlands (n = 39). All typically developing participants scored below the 90th percentile on the DBD. Parents of one adolescent failed to complete the questionnaires, one adolescent had a prior ADHD diagnosis, and three adolescents had an FSIQ under 80: They were excluded from the study, resulting in 34 TDAs.
Instruments
Neuropsychological measures
Two subtests of the Delis–Kaplan Executive Function System (D-KEFS; Delis, Kaplan, & Kramer, 2001) were used: the Tower Test and the Trail Making Test (TMT). The D-KEFS has good reliability and validity (Homack, Lee, & Riccio, 2005).
Tower Test
The Tower Test assesses several key EFs, including planning. The objective of this subtest is to move disks, varying in size from small to large, across three pegs to build a designated tower in the fewest number of moves possible. In constructing the target towers, the examinee must follow two rules: (a) move only one disk at a time and (b) never place a larger disk over a smaller disk.
Two scores from the Tower Test were used: the “total achievement score” and the “move accuracy ratio.” The total achievement score gives an overall planning score and is based on the number of moves to build the tower, rule violations, completion time, and final tower correctness. Scores range from 0 to 30, with higher scores indicating better overall planning skills. The move accuracy ratio is calculated by dividing the total number of moves set by the minimum number of moves necessary to build the designated tower. Scores range from 0 to 3.1: The lower this score, the less moves were necessary to obtain the correct tower; therefore, a lower score indicates good planning skills.
TMT
We used three conditions of the TMT to calculate mental flexibility (that is considered necessary for planning). In the “switching” condition, adolescents were instructed to connect items on a page, switching between numbers and letters beginning with 1 and A, and connecting them in numerical and alphabetical order, respectively. To control for possible differences in motor speed and familiarity with numbers and letters, the “number” condition (connecting numbers in numerical order) and the “letter” condition (connecting letters in alphabetical order) were also administered. In this study, mental flexibility is measured, using the time to complete the switching condition minus the average time to complete the number and letter conditions. Scores can range from −150 to 240 s, with a higher score indicating more difficulty to switch between two sets.
Ecologically valid neuropsychological measures
Two subtests of the Behavioral Assessment of the Dysexecutive Syndrome (BADS; Wilson, Alderman, Burgess, Emslie, & Evans, 1996) were used: Key Search and Zoo Map. These subtests improve the ability to predict daily planning difficulties by assessing more complex, real-life situations than do neuropsychological measures (Wilson et al., 2003). Inter-rater reliability was found to be high (r = .88) and discriminative validity was supported (Baron, 2007). Usually the BADS is used for ages 16 and older and, for children, the Behavioral Assessment of the Dysexecutive Syndrome in Children (BADS-C) is used (norms up to 16 years). As ceiling effects are reported for subtests of the BADS-C (Henry & Bettenay, 2010; Shimoni et al., 2012) and our sample is on the older end of the norm group of the BADS-C, we decided to use the BADS.
Key Search
To examine the ability to plan an efficient, systematic plan of action, adolescents are presented with a drawing of a 100-mm square that represents a field in which they have lost their key. The adolescents are asked to draw a pathway through which it would be reasonable to search for the lost key. Two measures were used: (a) the strategy score (ranging from 0 to 16, with a higher score indicating a better performance), based on whether the rater believes the strategy to be systematic, efficient, and likely to be effective; and (b) completion time.
Zoo Map
This subtest consists of two conditions. In Condition 1, adolescents are asked to plan a route on a given zoo map, passing through a list of animals (the ability to formulate and implement a plan). In Condition 2, they have to pass the list of animals in a given order (follow a pre-formulated plan), thereby making less of an appeal to planning skills than Condition 1. For each condition, two measures were used: (a) the order score, based on successful implementation of the plan (ranging from minus the number of errors to 8, with a higher score indicating a better performance); and (b) completion time.
Parental rating of daily life planning
The Dutch Behavior Rating Inventory of Executive Function (BRIEF; Gioia, Isquith, Guy, & Kenworthy, 2000; Smidts & Huizinga, 2009) is a normative behavioral rating scale for children 5 to 18 years old, designed to elicit everyday EF as observed by the parents in natural everyday environments. The internal consistency, the test–retest stability, and convergent and discriminant validity of the Dutch version of the BRIEF are considered good (Huizinga & Smidts, 2010).
The BRIEF consists of 75 items of which each item pertains to specific everyday behavior, relevant to EF. Parents were asked to indicate how often their child displayed a given behavior in the past 2 weeks by giving one of three responses, “Never,” “Sometimes,” or “Often.” The items of the BRIEF are categorized into eight clinical scales: Inhibit, Shift, Emotional Control, Initiate, Working Memory, Plan/Organize, Organization of Materials, and Monitor.
In this study, three scales were used: (a) Plan/Organize, (b) Metacognition Index (MI), and (c) Global Executive Composite (GEC). The Plan/Organize scale measures the child’s capacity to anticipate future events, set goals, develop appropriate steps to carry out associated tasks or actions, and manage current and future-oriented task demands (12 items, scores range from 12 to 36). The MI is a composite score of the scales Initiate, Working Memory, Plan/Organize, Organization of Materials, and Monitor Scales, and represents the ability to plan, organize, initiate, and hold information in mind for future-oriented problem solving (44 items, scores range from 44 to 132). The GEC is a summary score that includes all eight clinical scales (72 items, scores range from 72 to 216). Higher scores on the subscales of the BRIEF indicate more EF problems.
Procedure
Prior to face-to-face testing, a telephonic interview was conducted with parents to obtain demographic information and check inclusion criteria. After completion of informed consent by parent and adolescent, the parent was interviewed using the DISC-IV and questionnaires were filled out. At the same time, the adolescent was tested. As the tasks administered were part of a multi-center study on treatment of adolescents with ADHD, in addition to the tasks described above, other tasks were also administered. Duration of assessment was 2.5 hr including breaks. All assessments started with the WISC-III followed by the neuropsychological batteries (BADS/D-KEFS), which were presented in counterbalanced order across participants, to account for order effects. After assessment, participants received a small gift (worth approximately 2 euro).
Missing data and outliers
Either examiner error or adolescent non-compliance led to missing data. The number of missing cases ranged from 0 to 5 (D-KEFS, n = 5; BADS, n = 0; BRIEF, n = 0). Of all tests, only the subtest Key search showed outliers (n = 2). As analyses with and without outlier truncation showed similar results, original analyses without outlier truncation are reported.
Statistical analysis
Correlations between dependent measures were calculated (Table 1). Next, differences in planning skills between diagnostic groups (TD, ADHD-I, ADHD-C) on three levels of measurement (D-KEFS, BADS, BRIEF) were tested using MANOVAs on the raw scores. As assumptions of normality and homogeneity of variances were not retained for all dependent variables, Pillai’s trace was chosen as a test statistic. Pillai’s trace has been shown to be most robust to violations of unequal sample sizes (Stevens, 1996). In case of main group effects, Games–Howell post hoc tests (accurate with unequal sample sizes; Field, 2009) were performed. Analyses were conducted with and without covarying for medication use (yes/no); when medication use affected results, this will be reported.
Correlations Between IQ, Symptoms, and Planning Measures.
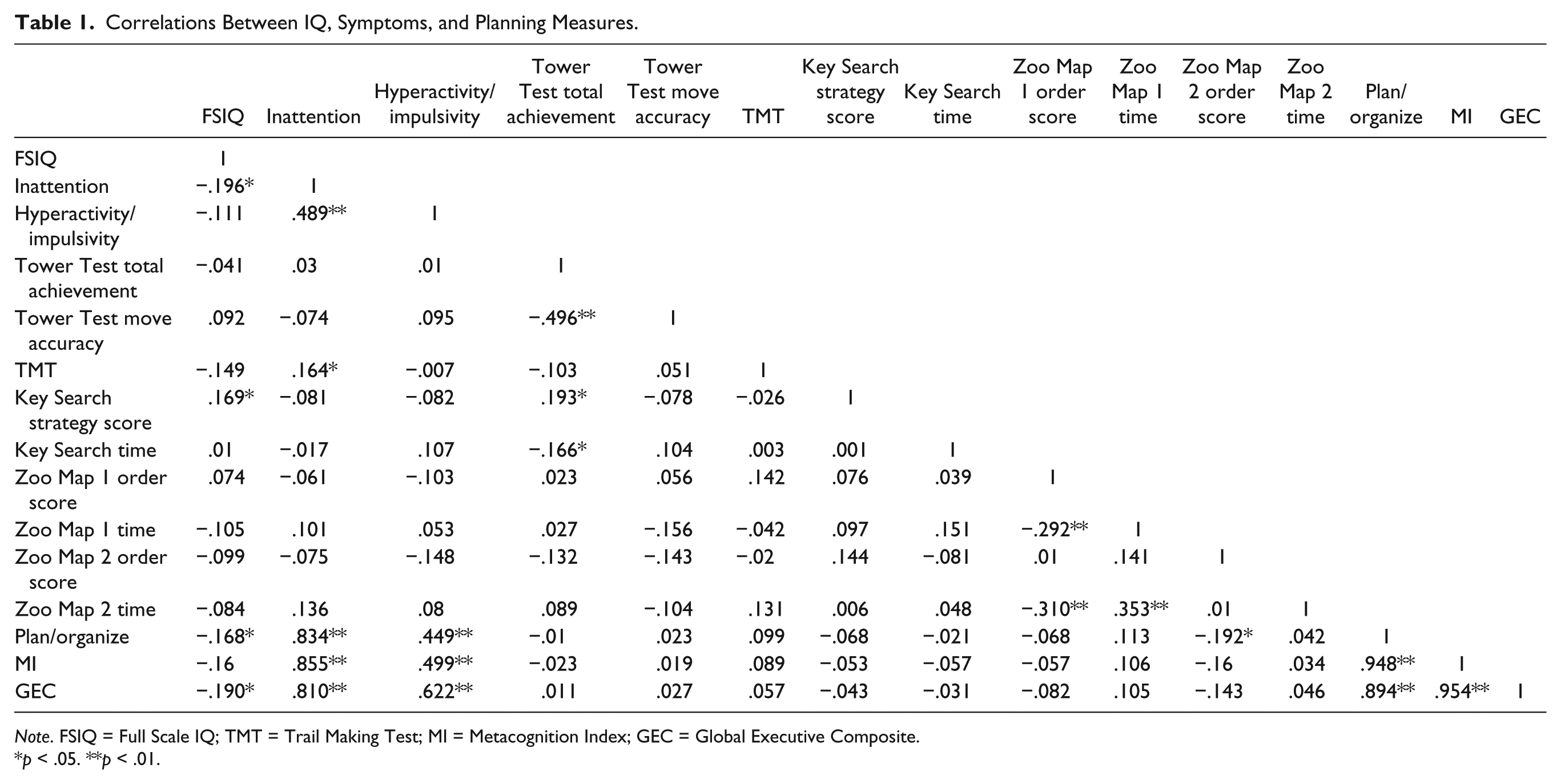
Note. FSIQ = Full Scale IQ; TMT = Trail Making Test; MI = Metacognition Index; GEC = Global Executive Composite.
p < .05. **p < .01.
Finally, based on age-based norms, adolescents’ scores were classified as “clinical” or “non-clinical.” The D-KEFS has been standardized with large normative and patient samples of different age ranges (Homack et al., 2005): On the TMT and the Tower Test (Delis et al., 2001) scaled scores (M = 10, SD = 3) of 6 or below (comparable with the 10th percentile) are considered to represent clinical planning problems. The norms of the BADS are based on 216 healthy individuals (M age = 46.6, SD = 19.8), but age-based data on the individual tasks are not provided. As EF develops dramatically during adolescence, age-based norms are important. Therefore, we used the best available norm group: the scores of our TDA. On all BADS measures, the average score of TDA was calculated, and based on their standard deviation, the 10th or 90th percentile was calculated (depending on the measure used) to represent the cutoff score for clinical planning problems. On the BRIEF, age-based norms lead to T-scores: T-scores greater than 65 (comparable with the 90th percentile) are considered to represent clinical planning problems. Differences between groups in clinical status are assessed with chi-square analyses.
Results
Sample description
Groups did not differ from each other with respect to age, gender, and FSIQ (Table 2). As expected, ADHD groups showed more symptoms than the typically developing (TD) group and the ADHD-C group showed more hyperactive/impulsive symptoms than did the ADHD-I group. Also, the ADHD-C group showed more inattentive symptoms than the ADHD-I group on the DISC-IV. The ADHD groups showed no differences in the number of methylphenidate (MPH) users or average school week dosage of immediate release MPH.
Demographic and Clinical Description of the Sample.

Note. TDA = typically developing adolescents; I = inattentive subtype; C = combined subtype; ns = not significant; FSIQ = Full Scale IQ; DBD = Disruptive Behavior Disorder Rating Scale; DISC-IV = Diagnostic Interview Schedule for Children; MPH = methylphenidate; IR = all medication was converted into immediate release dose.
p < .05. **p < .01.
MANOVA
Main group effects of the MANOVAs for both the D-KEFS tasks (TMT and Tower Test) and the BADS tasks (Key Search and Zoo Map Test) were non-significant (respectively p = .40,
Group Comparison of Subtypes of ADHD and TDA on Planning Measures.

Note. The number of participants differs for some dependent variables due to missing data (see text). TDA = typically developing adolescents; I = inattentive subtype; C = combined subtype; D-KEFS = Delis–Kaplan Executive Function System; ns = not significant; TMT = Trail Making Test; BADS = Behavioral Assessment of the Dysexecutive Syndrome; BRIEF = Behavior Rating Inventory of Executive Function; MI = Metacognition Index; GEC = Global Executive Composite.
When covarying for medication use, this comparison becomes significant.
When covarying for medication use, this comparison is no longer significant.
p < .05. **p < .01.
There was a significant main group effect for the BRIEF, V = .92, F(6, 290) = 43.26, p < .0001,
Clinical significance
Chi-square tests were conducted, examining group differences in the number of adolescents scoring in the clinical range of all three measures (Table 4). On the D-KEFS and BADS, most group effects were non-significant (Tower Test total achievement score, move accuracy, and TMT, p = 1.00, p = .25, p = .46, respectively; BADS Key Search strategy score, p = .76; time, p = .63; Zoo Map 1 order score, p = .67; Zoo Map 2 order score, p = .46; time, p = .83), except for completion time of Zoo Map Condition 1, χ2(2) = 6.11, p = .05, in which more adolescents with ADHD-I showed a longer completion time than in the other two groups.
Number of Adolescents Scoring Within the Clinical Range.
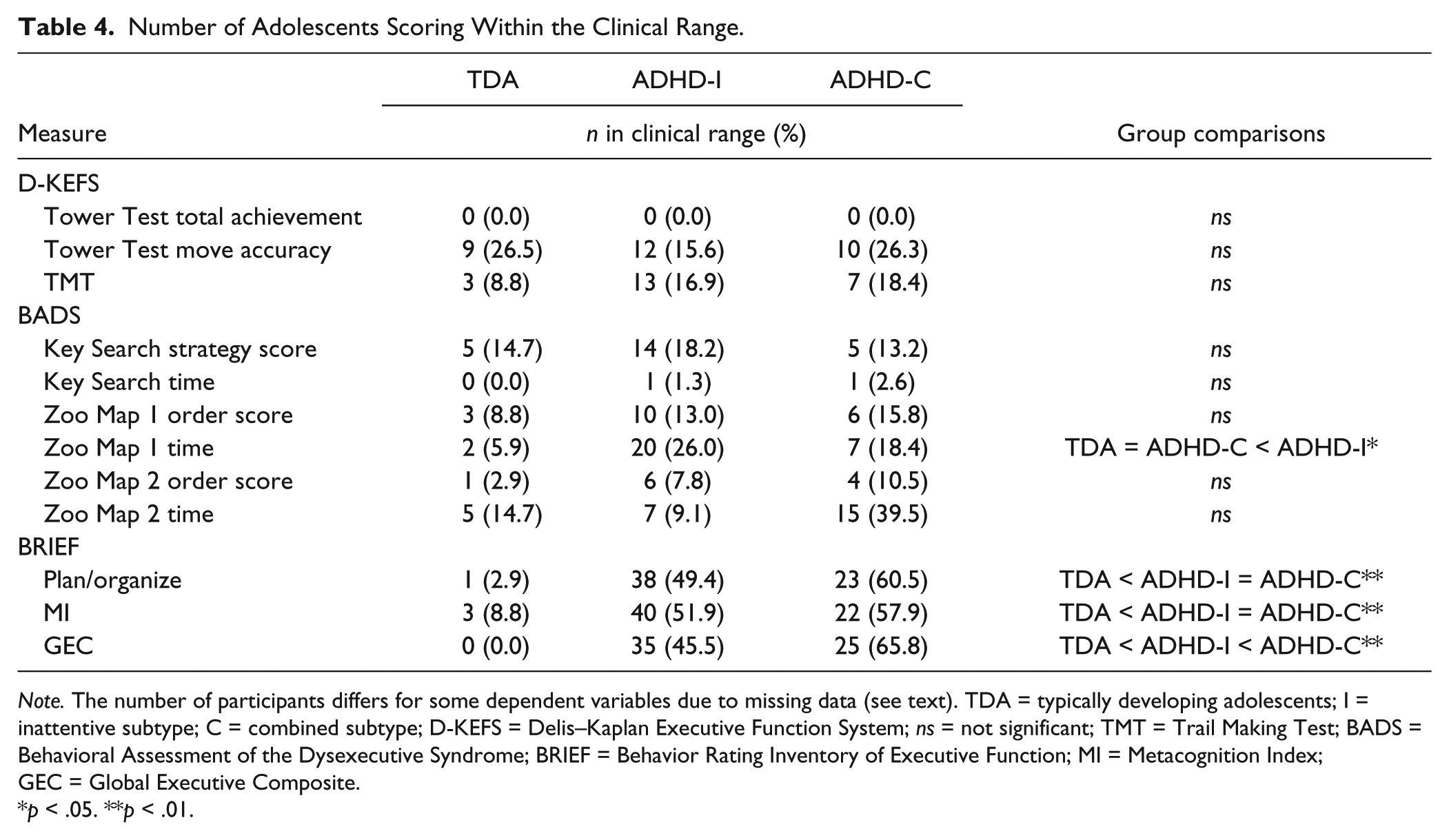
Note. The number of participants differs for some dependent variables due to missing data (see text). TDA = typically developing adolescents; I = inattentive subtype; C = combined subtype; D-KEFS = Delis–Kaplan Executive Function System; ns = not significant; TMT = Trail Making Test; BADS = Behavioral Assessment of the Dysexecutive Syndrome; BRIEF = Behavior Rating Inventory of Executive Function; MI = Metacognition Index; GEC = Global Executive Composite.
p < .05. **p < .01.
On the BRIEF, there were significant differences between groups on the Plan/Organize scale, χ2(2) = 28.42, p < .0001; MI scale, χ2(2) = 22.06, p < .0001; and GEC, χ2(2) = 34.19, p < .0001. On all scales of the BRIEF, significantly more ADHD adolescents (both subtypes) than TDA scored within the clinical range. Furthermore, on the GEC, significantly more adolescents with ADHD-C than with ADHD-I scored within the clinical range.
Discussion
This study investigated planning skills of adolescents with ADHD and subtype differences using a multi-method assessment on different levels of ecological validity. In general, on our neuropsychological measures, adolescents with ADHD (both subtypes) showed few planning deficits, which is in contrast to our predictions and other studies (Gau et al., 2009; Gau & Shang, 2010; Toplak et al., 2009; but see Qian et al., 2013). Only on one outcome, of the more ecologically valid task (BADS), there was a group difference, showing that adolescents with ADHD-I need more time for adequate planning than TDAs and ADHD-C. Finally, parents of adolescents with both subtypes of ADHD reported more daily life planning problems than parents of TDAs. In addition, parents of adolescents with ADHD-C reported more overall EF problems than those with ADHD-I. Our findings are comparable with the mixed findings of previous studies investigating planning skills of adolescents with ADHD (Gau et al., 2009; Gau & Shang, 2010; Qian et al., 2013; Toplak et al., 2009).
These findings lead to the question what is the best way to measure planning skills in adolescents with ADHD, by questionnaires or by neurocognitive measures. Unfortunately, there is no “golden standard” on how to adequately measure daily life planning problems. Even though observations of daily life planning skills by independent raters would probably be the most ecologically valid measure of planning, in general, parent-rated questionnaires are considered to capture these real-life planning problems (Siu & Zhou, 2014; Toplak et al., 2013). On parent-rated questionnaires, children (Gioia et al., 2002; Shimoni et al., 2012; Siu & Zhou, 2014) as well as adolescents with ADHD (this study; Toplak et al., 2009) consistently show more planning problems than controls. With regard to neurocognitive tasks of planning skills, a discrepancy is visible: On “paper-and-pencil,” tasks results are mixed in both child and adolescent samples (this study; Galasso et al., 2014; Klorman et al., 1999; Nigg et al., 2002; O’Brien et al., 2010; Qian et al., 2013; Shimoni et al., 2012; Siu & Zhou, 2014; Wodka, Loftis, et al., 2008; Wodka, Mostofsky, et al., 2008), whereas on computerized tasks, studies consistently show planning deficits in both children and adolescents with ADHD (Gau et al., 2009; Gau & Shang, 2010; Song & Hakoda, 2014; Toplak et al., 2009). In line with the literature, also in our study on parent-rated measures, planning deficits were found, and in our paper-and-pencil neuropsychological measures, we found a significant deficit on one task (BADS) but not on another (D-KEFS). In summary, in the literature, the two measures consistently showing planning problems in children and adolescents with ADHD are on both ends of the continuum of ecological validity: parent-rated measures on one end and computerized neurocognitive tests on the other. Thus, the degree of ecologic validity does not seem to be the best explanation for the mixed findings of studies assessing planning skills of adolescents with ADHD.
A better explanation may be that parent ratings of planning skills, neurocognitive paper-and-pencil and computerized planning measures, assess different components of planning (Toplak et al., 2013). However, another plausible influence to performance on planning measures, or to planning skills overall, are motivational incentives. Studies using a computerized tower test and parent report showed impaired planning skills of adolescents with ADHD (Gau et al., 2009; Gau & Shang, 2010; Toplak et al., 2009), whereas studies using paper-and-pencil tests did not (this study; Qian et al., 2013). Paper-and-pencil tests inevitably require more involvement of an examiner, create a more structured environment, and are more “hands-on,” therefore possibly causing adolescents to be more actively involved and more engaged in the task (Power, 1992; Toplak et al., 2013). As a result, these motivational incentives could improve their performance as compared with computerized tests or daily life tasks without such incentives, for example, homework. If this is the case, one might argue that adolescents with ADHD know how to plan, as long as they are motivated enough.
Another explanation for mixed findings between planning measures could be that tasks, used to assess planning skills, differ in the extent to which they appeal to other EFs. As finding your way in a zoo in the BADS Zoo Map Test could be considered less structured and possibly posits more distracters than building a tower in the Tower Test, it could make a stronger appeal to, for instance, working memory (remembering the assignment) or inhibition (not being distracted by other animals in the zoo). Therefore, our results could imply that planning problems observed in daily lives of adolescents with ADHD are not caused by deficits in underlying planning skills but by other underlying EF deficits (Phillips, Wynn, Gilhooly, Della Sala, & Logie, 1999; Salcedo-Marin et al., 2013; Sonuga-Barke, Dalen, Daley, & Remington, 2002). This is consistent with the idea that planning skills are part of the later developing “higher-order” EFs such as set shifting, whereas, for example, working memory and inhibition are “lower order” earlier developing EFs (Best, Miller, & Jones, 2009; Lin, Hsiao, & Chen, 1999; O’Brien et al., 2010). It may well be that planning problems in daily life derive from problems in these lower order EFs or from other basic cognitive processes such as sustained attention. Unfortunately, assessment of any EF also implicates other cognitive processes that are not directly relevant to the target EF (Miyake, Friedman, Emerson, Witzki, & Howerter, 2000). Therefore, it cannot be determined to what extent the different EFs have contributed to performance on our neurocognitive measures. More work in this field is needed to investigate to what extent daily life planning problems in individuals with ADHD are caused by deficits in other cognitive processes or “lower order” EFs.
In line with Barkley’s behavioral description of planning problems of adolescents with ADHD (Barkley, 2004), prior research with children (Gioia et al., 2002; McCandless & O’Laughlin, 2007; Riccio et al., 2006; Shimoni et al., 2012) and adolescents (Toplak et al., 2009), in our study adolescents with ADHD did show impairments on daily life planning skills as rated by their parents. However, only half to two third of the adolescents with ADHD scored within the clinical range of planning or EF problems as rated by parents. This is in line with studies showing that only a proportion of children with ADHD have EF deficits (Willcutt et al., 2005). In addition, this study also shows that there are differences between the subtypes of ADHD in planning skills. Both subtypes of ADHD show planning problems as perceived by parents but when assessing performance on neurocognitive tasks that resemble daily life, the ADHD-I subtype needed more time to adequately plan, whereas the ADHD-C subtype showed no deficits in planning. This could imply that within both subtypes, planning problems are apparent in daily life, but these planning problems may have different causes, with the ADHD-I subtype needing more time to plan. This is in accordance with the sluggish cognitive tempo that especially the ADHD-I subtype has been associated with (Langberg, Becker, & Dvorsky, 2014).
This study has several limitations. First, although we already had a multi-method assessment, having additional raters of planning problems (self-report, teacher report) would have given an even more all-round picture of EF. Furthermore, one could argue about the accuracy and/or validity of parental report in adolescence, as parents are likely to spend less time with their adolescent child in comparison with childhood (Achenbach, McConaughy, & Howell, 1987). Second, the TMT could be questioned as a measure of planning. Even though the TMT is designed to measure mental flexibility or set shifting, one could argue that the switching condition does make an appeal to planning skills, as planning is defined as the ability to formulate actions in advance and to approach a task in an organized, strategic, and efficient manner (Hayes-Roth & Hayes-Roth, 1979). Third, given that on most measures, we show no differences between ADHD and control groups, one may argue that our sample was selective or relatively unimpaired. However, one could argue that the sample may be biased (more severe), given that all adolescents applied for psychosocial treatment. However, cross-situational impairment was part of the diagnostic procedure; 71.3% of the adolescents were taking medication for their ADHD and still applied for additional treatment at an outpatient mental health institute, implying a non-selective, impaired, and clinical representative sample of adolescents with ADHD. Finally, it has been proposed that some of the BRIEF items overlap with symptoms of ADHD (Gioia et al., 2000), and our study also showed strong correlations between ADHD scores on the ADHD rating scale and the three BRIEF scales used. However, after removing items from the BRIEF subscales that based on face validity, reflected DSM-IV-TR ADHD symptoms (APA, 2000), analyses still showed significant differences between adolescents with ADHD and TDAs (data available from first author).
This study brings forward some clinical implications. Only a proportion (about half to one third) of adolescents with ADHD appears to have planning deficits according to parents. Although both the ADHD-I and ADHD-C subtypes can experience planning problems, these problems seem to arrive from different underlying deficits: In ADHD-I, this may be related to a more sluggish cognitive tempo (Langberg et al., 2014). In the literature, planning deficits in ADHD have most consistently been shown using parent-rated measures and computerized neurocognitive tests: Given that questionnaires reporting daily life behavior might assess different components of planning skills than neurocognitive measures, it seems important to use them complementary to get an overall picture of planning skills (Barkley & Edwards, 2006; Toplak et al., 2013). As the mixed findings on more “hands-on” neurocognitive tests suggest that motivation positively affects planning skills, enhancing motivation by adding structure and dividing large tasks in smaller steps to keep the adolescent actively involved may help resolve daily life planning problems in adolescents with ADHD.
All in all, in this study, a multi-method assessment was used to investigate planning skills in a large sample of adolescents with ADHD, while exploring differences between the two most prevalent subtypes in adolescence. More than half of adolescents with ADHD showed planning deficits as reported by parents, with the ADHD-C subtype showing additional overall EF deficits. However, “hands-on” neurocognitive measures showed mixed results. Future research is needed to investigate the causal processes that give rise to planning deficits in ADHD and to determine the best way to assess these deficits. For now, to capture planning deficits in adolescents with ADHD, the combined use of rating scales and “less structured” neurocognitive measures is recommended.
Footnotes
Acknowledgements
We thank ZonMW for providing this research grant. We are grateful to the participating Mental Health providers, families, and research assistants for their participation and collaboration.
Declaration of Conflicting Interests
Saskia van der Oord has been a paid consultant for Janssen pharmaceuticals in the development and evaluation of a serious game “Heelseeker” aimed at training cognitive functions. The other author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by ZonMW; project number 15700.3006.