
Abstract
Introduction
There is growing evidence that a substantial number of people diagnosed with ADHD in childhood continue to be affected into adolescence and adulthood (Barkley, Fischer, Smallish, & Fletcher, 2002; Davidson, 2008; Fischer & Barkley, 2007). Prevalence studies indicate that about 2% to 7% of the adult population meet the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) criteria for the diagnosis (Barkley et al., 2002; Davidson, 2008; Fayyad et al., 2007; Fischer & Barkley, 2007; Kessler et al., 2006; Simon, Czobor, Balint, Meszaros, & Bitter, 2009).
The core symptoms in ADHD, as described in the DSM-IV-TR, are in the domains of hyperactivity, impulsivity, and inattentiveness, and cause difficulties in coping with everyday life. They often lead to psychosocial problems, relationship problems, substance abuse, and problems with work performance and maintaining employment (Barkley, 2002). Adults with ADHD also show high lifetime comorbidity with other psychiatric diagnoses such as antisocial personality disorder, and mood, anxiety, and substance-related disorders (Biederman et al., 2012; Sobanski et al., 2007).
Because there is such a broad range of functional impairments in adults with ADHD, the majority of national and international guidelines on ADHD recommend some form of psychosocial intervention as a complement to stimulant medication, which is still considered to be the first-line treatment for adult ADHD (Seixas, Weiss, & Muller, 2012). Even if stimulant medication can ameliorate the core symptoms, it does not provide the patient with coping skills to manage functional and quality of life impairments. In addition, many adults with ADHD prefer not to take medication and many continue to experience significant residual symptoms (Safren, Sprich, Cooper-Vince, Knouse, & Lerner, 2010).
Research on psychosocial treatment for adults with ADHD is still in its infancy and the most studied treatment is cognitive behavioral therapy (CBT) oriented approaches (Knouse & Safren, 2010; Philipsen, 2012). Two different reviews of CBT for adult ADHD show that the results are generally promising, but there have been few randomized controlled trials (Knouse & Safren, 2010; Mongia & Hechtman, 2012).
Three of the most recent randomized controlled trials used attention-matched comparisons; their results supported the efficacy of CBT in the treatment of adult ADHD. Solanto and colleagues evaluated a 12-week manualized meta-cognitive therapy intervention that targeted time management, organization, and planning (Solanto et al., 2010). Eighty-eight adults with ADHD, stratified by use of ADHD medication, were randomly assigned to either meta-cognitive therapy or supportive therapy in a group modality. The meta-cognitive therapy group showed significantly greater reduction in independent evaluator ratings, collateral report, and self-report of inattention symptoms at posttreatment, than the supportive therapy group. Another study that investigated the efficacy of group-therapy treatment, in this case Dialectical Behavioral Therapy (DBT)-based skills training, was conducted by Hirvikoski et al. (2011). Fifty-one adults with ADHD were randomly assigned to 14 sessions of DBT or a loosely structured discussion group. A per-protocol analysis, excluding patients who were unstable on medication or did not complete the treatment, showed significantly greater reduction in self-reported ADHD symptoms at posttreatment for the DBT group than from the discussion group. However, the difference was not significant when an intention-to-treat (ITT) analysis was conducted. Safren, Sprich, Mimiaga, et al. (2010) assessed the efficacy of 12 sessions of individual CBT for 86 medication-treated adults with ADHD and persistent symptoms. Patients were randomized to either CBT or relaxation with educational support. Patients in the CBT group had lower scores on both assessor- and self-rated ADHD symptoms at posttreatment compared with patients in the control condition. The result was maintained at 6 and 12 months follow-up.
Most of the evaluated treatment programs have offered a high degree of interpersonal support to patients during treatment. We found only one study that investigated the effect of a more self-directed treatment. In a randomized controlled trial, Stevenson and colleagues examined the effect of a self-directed psychosocial intervention with minimal therapist contact (Stevenson, Stevenson, & Whitmont, 2003). The treatment consisted of a self-help book with education about ADHD and content and exercises covering strategies to cope with ADHD-related problems. Thirty-five participants were randomized to either a treatment group or a waiting-list control group. At the end of the 8-week intervention, the treatment group reported a significant reduction in ADHD symptoms, improved organizational skills and self-esteem and better anger control. This study gives an indication that more self-directed psychosocial programs with a minimum of interpersonal support can also be a promising treatment alternative for adults with ADHD.
One form of therapy that provides an opportunity for more self-directive treatment is Internet-based CBT (iCBT) or computer-based CBT (cCBT). This form of treatment has been studied intensely in the last decade, and there are now several reviews and meta-analyses that indicate that iCBT and cCBT are effective for a range of psychological disorders (e.g., depression, panic disorder, social phobia, and generalized anxiety disorder) and other health problems (e.g., insomnia, chronic back pain, headache, and tinnitus; Andersson & Cuijpers, 2009; Andrews, Cuijpers, Craske, McEvoy, & Titov, 2010; Cheng & Dizon, 2012; Cuijpers, van Straten, & Andersson, 2008). Even though most studies on iCBT have been conducted with minimal therapist contact, it has been shown that, at least for depression and anxiety, the amount of support or contact with clients is correlated with the treatment effect; effect sizes are larger when more support is provided (Andersson & Cuijpers, 2009; Berger, Hammerli, Gubser, Andersson, & Caspar, 2011; Spek et al., 2007).
Our aim was to investigate the efficacy of two iCBT program formats, self-help alone (iCBT self-help format [iCBT-S]) and self-help with weekly group-therapy sessions (iCBT group-therapy format [iCBT-G]), for adults with ADHD in outpatient psychiatric care. Our hypothesis was that both treatment groups would show significant reductions in self-rated ADHD symptoms compared with a waiting-list control group. We also wanted to explore whether the iCBT-G group would benefit more from the program than the iCBT-S group, as earlier studies on iCBT have indicated that the degree of support is related to outcome. Finally, we wanted to explore whether the two treatment groups would show reductions in comorbid symptoms compared with a waiting-list control group.
Method
Study Design and Recruitment of Patients
The study used a three-group randomized controlled trial. Patients were randomized to either iCBT in a self-help format (iCBT-S), iCBT with weekly group-therapy sessions (iCBT-G), or a waiting-list control group. After posttreatment measures, the waiting-list controls were randomized to either iCBT-S or iCBT-G.
Adult patients with a diagnosis of ADHD were recruited from psychiatric clinics within the county of Västmanland in Sweden or from those referred for ADHD assessment at the Neuropsychological Clinic (NPC), County Hospital, Västerås, Sweden.
Because resources were limited, the study was only powered to detect a difference in the primary outcome measure (self-rated ADHD symptoms) at posttreatment between each treatment group and the waiting-list control group. A power analysis was performed with the computer program G*Power v. 3.1.9 (Faul, Erdfelder, Buchner, & Lang, 2009). The analysis was based on two pairs of one-way ANOVAs of posttreatment scores; iCBT-G versus waiting-list controls and iCBT-S versus waiting-list controls. The expected effect size (Cohen’s d) was set to 1.2 based on a mean effect size for the psychosocial treatments presented in the review by Knouse & Safren (2010). A power analysis based on an alpha level of .05 showed that a total sample size of 54 patients would be needed for a power of 80%, with 18 patients randomized to each condition.
A randomization protocol was created by an independent statistician where a series of 54 patients were randomized in blocks to one of the study conditions over a period of four semesters (spring 2009 to autumn 2010). The results were kept in sealed envelopes, each coupled to the number in the consecutive series of patients referred to the study and who met the inclusion criteria.
Unfortunately, the study had to be adjusted before the planned sample of 54 patients had been recruited because of the referral of fewer patients than expected, as well as limited financial resources and access to personnel. A total of 45 patients had been randomized to the study at the time of adjustment, resulting in uneven numbers of patients in the three different conditions: 13 in iCBT-S, 14 in iCBT-G, and 18 in the waiting-list control group (Figure 1).
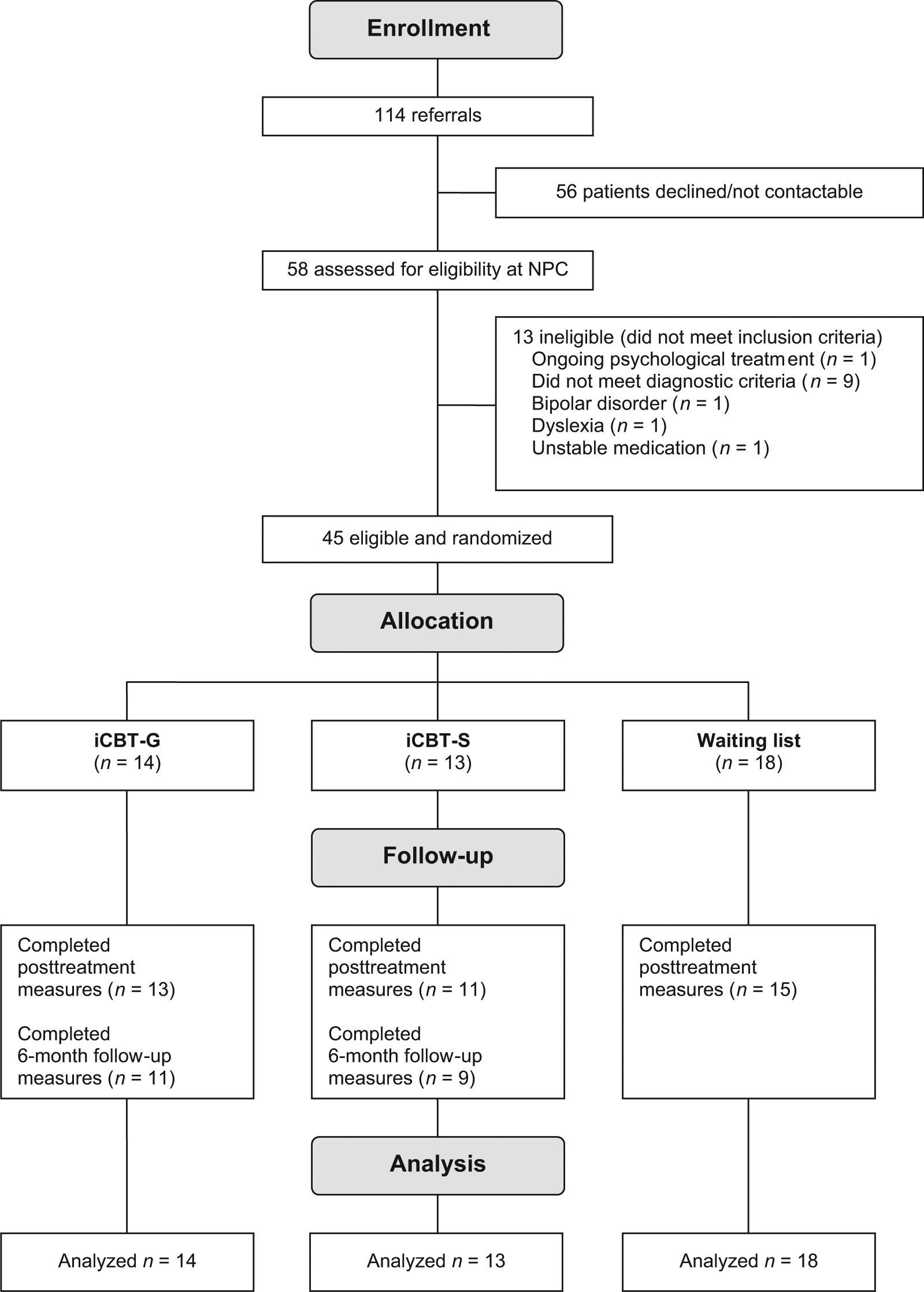
Flow chart of the recruiting process.
Criteria for inclusion were as follows: (a) being at least 18 years old, (b) having ADHD as the primary diagnosis, (c) having access to a computer and the Internet, and (d) being able to set aside one afternoon a week for group meetings. Exclusion criteria were as follows: (a) borderline or antisocial personality disorder, (b) bipolar disorder, (c) ongoing substance abuse, (d) suicidal ideation, (e) dyslexia, (f) mental retardation, and (g) ongoing psychotherapy. Patients who were taking prescribed ADHD medication had to be stable on the medication during the whole study time. Approval of the study was obtained from the Regional Ethical Review Board in Uppsala, Sweden, and all patients gave informed written consent.
Diagnostic Assessment
Forty-three (74%) of the 58 patients assessed for eligibility were assessed for ADHD at the NPC. The basic ADHD assessment consists of self-rating scales concerning current symptoms, a clinical interview with the patient and a significant other, intelligence testing, cognitive screening and a general psychiatric assessment (Axis I and II). If this basic investigation fails to reach a diagnostic conclusion according to the criteria for ADHD in DSM-IV-TR, further assessment is initiated. This consists of a more in-depth investigation that includes hereditary aspects and early childhood symptoms, specific testing of cognitive functions, extended personality assessment, and a semi-structured interview regarding self-care, productivity, and leisure by an occupational therapist. Fifteen (26%) of the referred patients had been diagnosed with ADHD outside the NPC. They were screened with a shorter procedure to confirm diagnosis during the introductory assessment at the NPC.
Evaluations and Measures
Independent evaluators, blinded to group assignment, administered the self-report measures and conducted the semi-structured interview listed below at pretreatment, posttreatment, and 6-month follow-up.
Primary outcome measure
The Current Symptoms Scale—Self-Report Form (CSS; Barkley & Murphy, 2006) was used as the primary outcome measure. The scale includes items based on DSM-IV Criterion A symptoms of adult ADHD. Each item is estimated on a scale from 0 to 3 (not at all or rarely, sometimes, often, very often). A total score—the sum of all scores in the scale across all items—was used in the analysis.
Secondary outcome measures
Comorbid symptoms of depression and anxiety were measured by the Beck Depression Inventory (BDI-II; Beck, Steer, Brown, & Lindfors, 2006) and the Beck Anxiety Inventory (BAI; Beck, Steer, & Järvå, 2012), respectively. Quality of life was measured by the ADHD Impact Module–Adult (AIM-A), a self-report questionnaire designed to capture different dimensions of quality of life of adults with ADHD. It is comprised of four global quality of life items, five economic impact items, and five multi-item scales. Two multi-item scales (“Living with ADHD” and “Work, Home and School Performance and Daily Functioning”) were chosen a priori to be included in the study because the primary interest was to investigate whether it was possible to alter the patients’ diagnosis-associated problems and their ability to cope with daily life using the techniques of the treatment regimen. The original article describing the development of the AIM-A and an evaluation of its psychometric properties was based on a sample of 317 adult patients with ADHD. It showed that the scale had good internal consistency, Cronbach’s alpha between .83 and .91, satisfying convergent and discriminant validity and indicated that it was sensitive to change (Landgraf, 2007). To capture the patient’s perspective about his or her occupational performance, the Canadian Occupational Performance Measure (COPM) was used. The COPM is a semi-structured interview where the therapist asks the patient to identify and rate issues in areas of self-care, productivity, and leisure, using a scale from 1 to 10. Two scores, performance and satisfaction with performance, are obtained. In a review of articles examining the psychometric properties, research outcomes, and practice related to COPM, the authors found 19 articles examining the psychometric properties of COPM (Carswell et al., 2004). Three studies that had examined the reliability of the instrument showed strong test–retest reliability, ranging between .84 and .92. Eleven studies had evaluated the validity of COPM in different settings and for various populations. Generally, the studies supported the COPM as a valid measure of occupational performance. Sensitivity to change was evaluated in five studies and all reported that the COPM was very responsive to change.
Intervention
Both the iCBT-G and iCBT-S groups followed the iCBT program In Focus developed by the Swedish company Livanda—Internet Clinic, Ltd., in collaboration with the NPC. The content of the program was based on the cognitive behavioral model formulated by Safren, Sprich, Chulvick, & Otto (2004). According to this model, neuropsychological deficits are at the core of the disorder and these deficits contribute over time to functional impairments by hindering the individual from acquiring and using compensatory strategies, which results in a history of failures and underachievement and dysfunctional beliefs. The model supports the use of behavior skills training for the acquisition of compensatory skills and techniques that target dysfunctional cognitions and emotional distress. The In Focus program is based on therapeutic methods from CBT and focuses mainly on teaching compensatory techniques to handle ADHD-related difficulties, such as behavior analyses, time management, problem solving, and organization and planning but also on how to handle dysfunctional thinking (cognitive restructuring) and emotional distress (mindfulness and acceptance techniques). These methods have previously been used with promising results in treatment programs for adults with ADHD (Knouse & Safren, 2010; Mongia & Hechtman, 2012; Philipsen, 2012).
In Focus consists of nine treatment modules and a follow-up module that are worked through in a sequential order. Each module consists of an information component that is related to the theme of the module and an exercise component with therapeutic techniques. Two optional therapeutic techniques, relaxation training and strategies to handle sleeping problems, were chosen for inclusion based primarily on our experience of working in our clinic with adult ADHD patients who expressed stress and sleeping problems and requested methods for managing these problems. Although these techniques are commonly used in the treatment of stress, anxiety, and insomnia, we have not found any scientific support for their efficacy in the treatment of ADHD and associated problems. The therapeutic techniques included were as follows: (a) Behavior analysis, (b) Mindfulness and acceptance, (c) Time management, (d) Gauging attention span, (e) Reducing distractors, (f) Organization and planning, (g) Problem solving, (h) Behavior activation, (i) Cognitive restructuring, and (j) Anger control training.
Behavior analysis
The behavioral analysis exercise is based on applied behavioral analysis (Cooper, Heron, & Heward, 2007) but was adapted and simplified to be easier for nonprofessionals to understand and learn. The goals of the exercise are to provide insight into how behavior is formed and maintained and to stimulate motivation to change. The exercise consists of four parts: (a) identification of behavior that the patient wants to change, (b) analysis of short-term and long-term effects, (c) identification of preceding events/triggers, and (d) analysis of consequences if the behavior is modified.
Mindfulness and acceptance
Mindfulness- and acceptance-based interventions are divided into two different exercises. The mindfulness exercise consists of meditation and attention skills. It was adapted from Kabat-Zinn (1996, 2005), and is divided into three parts. Part 1 is restricted to the practice of observation and description of both internal experiences and those that are determined by the environment. In Part 2, the concept of a nonjudgmental attitude is added and examples of how to practice mindfulness in everyday activities are given. Part 3 introduces the concept of acceptance and gives examples of how to use mindfulness as a method to cope with strong and negative emotions. The acceptance exercise is built upon principles from acceptance and commitment therapy (ACT; Hayes, Strosahl, & Wilson, 1999) and is an informative text component with stories, images, and metaphors to illustrate how thoughts and emotions are related, the difficulty and effect of suppressing unwanted and intrusive thoughts and feelings, and an introduction to the concept of observation and acceptance as an alternative approach.
Time management
The time management exercise consists of examples of and rationale for traditional skills and strategies to manage time, such as using a calendar, making a to-do list, and using reminders. In addition to these strategies, an exercise was developed based on the theory that people with ADHD could have an impairment in their sense of time as a consequence of poor inhibition and working memory difficulties (Barkley, 2006), which could hypothetically be a cause of difficulties with keeping track of time and appointments. The aim of the exercise is to give patients the opportunity to investigate their own ability to estimate how much time different tasks in everyday life take and to gain knowledge that could be useful when planning chores and activities.
Gauging attention span
This exercise was adapted from Safren and colleagues’ treatment program (Safren, 2005). The purpose of the exercise is to make patients aware of how long they can sustain their attention in various tasks before distractions get in the way. In the original exercise, patients are instructed to choose only tasks that are boring or unattractive and to time how long they can sustain their attention. We did not restrict the exercise to boring or unattractive tasks because we also wanted to make patients aware of how they function in very stimulating tasks; in some activities, they may actually be hyperfocused and indulge in activities for longer than they had planned. Experience gained from the exercise is then used in the “Problem solving” exercise later in the program.
Reducing distractors
This was a text-based component with examples of strategies to arrange the environment to reduce distractors (e.g., disturbing sounds and aspects of the environment that attract visual attention), to use visual cues as a memory aid, and to establish routines. Patients are reminded to take advantage of the experiences they have gained from the “Behavioral analysis” and “Gauging attention span” exercises when planning changes in their everyday lives.
Organization and planning
This exercise contains two components. The first is a text-based part with examples of strategies to organize papers, bills, clothes, and the like. In the second part, the patient uses the Internet program to develop schedules for activities and tasks in a step-by-step procedure: (a) identify chores and activities that the patient knows from experience are problematic and need to be planned, (b) prioritize and divide them into smaller parts/steps, and (c) implement the planned activity and evaluate the result.
Problem solving
Problem solving has been shown to be effective in the treatment of depression (Mynors-Wallis, Gath, Day, & Baker, 2000). Depression is a common secondary problem for those with ADHD, and problem solving has been incorporated into other CBT treatments for adult ADHD (Philipsen, 2012). It is probable that the psychological symptoms of anxiety, stress, and depression may be linked to psychosocial problems and if the patient is given the tools to solve these problems the symptoms may improve. An important part of problem solving methodology is to divide problems into achievable parts or goals. This can potentially serve as an effective coping strategy for persons with ADHD, with their reduced attention span and susceptibility to distractions, and it could have a positive effect on procrastination. In the Internet program, the patient is guided through the exercise in consecutive steps: (a) identify problems that need to be solved, (b) redefine vague problems into specific terms, (c) prioritize and select a task to start with, (d) divide the task into manageable parts, (e) schedule a first activity to start with, and (f) evaluate the result.
Behavior activation
Behavior activation is an intervention that has been shown to be effective in the treatment of depressive symptoms (Cuijpers, van Straten, & Warmerdam, 2007). Symptoms typical of depression, such as apathy and social withdrawal, have been found to be more prominent in persons with ADHD, particularly in those types where inattention predominates (Marshall, Evans, Eiraldi, Becker, & Power, 2014; Torrente et al., 2011). The exercise was adapted from a treatment manual published by Martell, Addis, and Jacobson (2001). Patients are encouraged to begin an activity diary integrated with the Internet program and to schedule activities that prevent passivity, create positive emotions, and enhance well-being.
Cognitive restructuring
This exercise was built upon standard cognitive interventions based on the cognitive model and treatment manual by Beck and colleagues (Beck, 1979). It was adapted and simplified to fit an Internet-based format. It focuses on the relationships between environment, thoughts, emotions, physiological reactions, and overt behavior and is restricted to the identification of negative thoughts, thought traps, and simple techniques to find alternative, more balanced, and realistic thoughts.
Anger control training
Symptoms of deficient emotional self-regulation, such as low frustration tolerance, temper outbursts, and emotional impulsivity, have been shown to be relatively common in adults with ADHD (Surman et al., 2013). This exercise was based on the anger control component of Aggression Replacement Training, a treatment intervention originally developed for working with aggressive youths (Goldstein, Glick, & Gibbs, 1998). The exercise consists of a diary integrated into the program, in which the patient enters situations that triggered aggression and external and internal stimuli that the patient has identified as triggers. Different techniques to control aggression are presented, and the patient tries and evaluates these in their everyday life.
The content of the program is summarized in Table 1.
Themes and Content of Modules in the Internet-Based CBT Program In Focus.

Note. CBT = cognitive behavioral therapy.
iCBT-G—Internet-based CBT program with weekly group sessions
The iCBT-G group used In Focus in the context of group therapy. The groups consisted of four to six individuals who started treatment at the beginning of each semester and met for 3 hr once a week for 10 weeks. The group sessions followed the content of the 10 In Focus modules and were led by two experienced therapists: a psychologist specialized in clinical psychology and neuropsychology, and an occupational therapist with an undergraduate diploma in CBT and basic therapy training in ACT. The structure of the group sessions was as follows: (a) a short summary of the previous session, (b) review and feedback on the previous session’s homework, (c) introduction of a new module and corresponding strategies, (d) in-session exercises to illustrate the new strategies, and (e) new homework assignments. The participants also had the opportunity to ask the therapists questions between sessions via an encryption-protected contact function in the program.
iCBT-S—Internet-based CBT program in a self-help format
The iCBT-S group received the Internet-based program and instructions on how to work with the program on their own. Patients also had the optional and nonscheduled support function of being able to ask the NPC therapists questions via an encryption-protected contact function in the program. The therapists at NPC monitored the patients’ engagement in the program. If they had failed to work on a task or had failed to continue to the next module within 10 days, patients were prompted by e-mail to continue to work with the program and were encouraged to ask for support if they had difficulties.
Statistical Analyses
Differences in demographic and pretreatment measures were analyzed with one-way ANOVA for continuous variables and χ2 for categorical and nominal data. Differences in outcome measures at posttreatment and 6-month follow-up were analyzed by general linear model ANCOVA using pretreatment scores as the covariate. These analyses were based on the ITT sample using the Last-Observation-Carried-Forward (LOCF) method, meaning that data missing at posttreatment and 6-month follow-up were replaced with pretreatment scores. For ANCOVAs showing a significant main effect, post hoc pairwise comparisons were conducted using the LMATRIX (contrast coefficients matrix) syntax subcommand in SPSS, which maintains the appropriate error term. Between-groups effect sizes (Cohen’s d) were calculated from significant post hoc analyses using data from the contrast, that is, dividing the contrast estimate (mean difference between the estimated marginal means) by the square root of the mean squared error corrected for unequal group sizes (d = (Mi − Mc) / √{MSE[(ni + nc − 2) / (ni + nc)]}). Differences between posttreatment and 6-month follow-up for the iCBT-G and iCBT-S groups were tested with paired-sample t tests. All statistical analyses were conducted using IBM SPSS version 20.
Results
After randomization, the groups did not differ in any of the demographic variables listed in Table 2. There were no significant differences between the groups in pretreatment scores on the primary outcome measure (CSS) or secondary outcome measures (BDI, BAI, COPM, AIM-A).
Sample Characteristics.
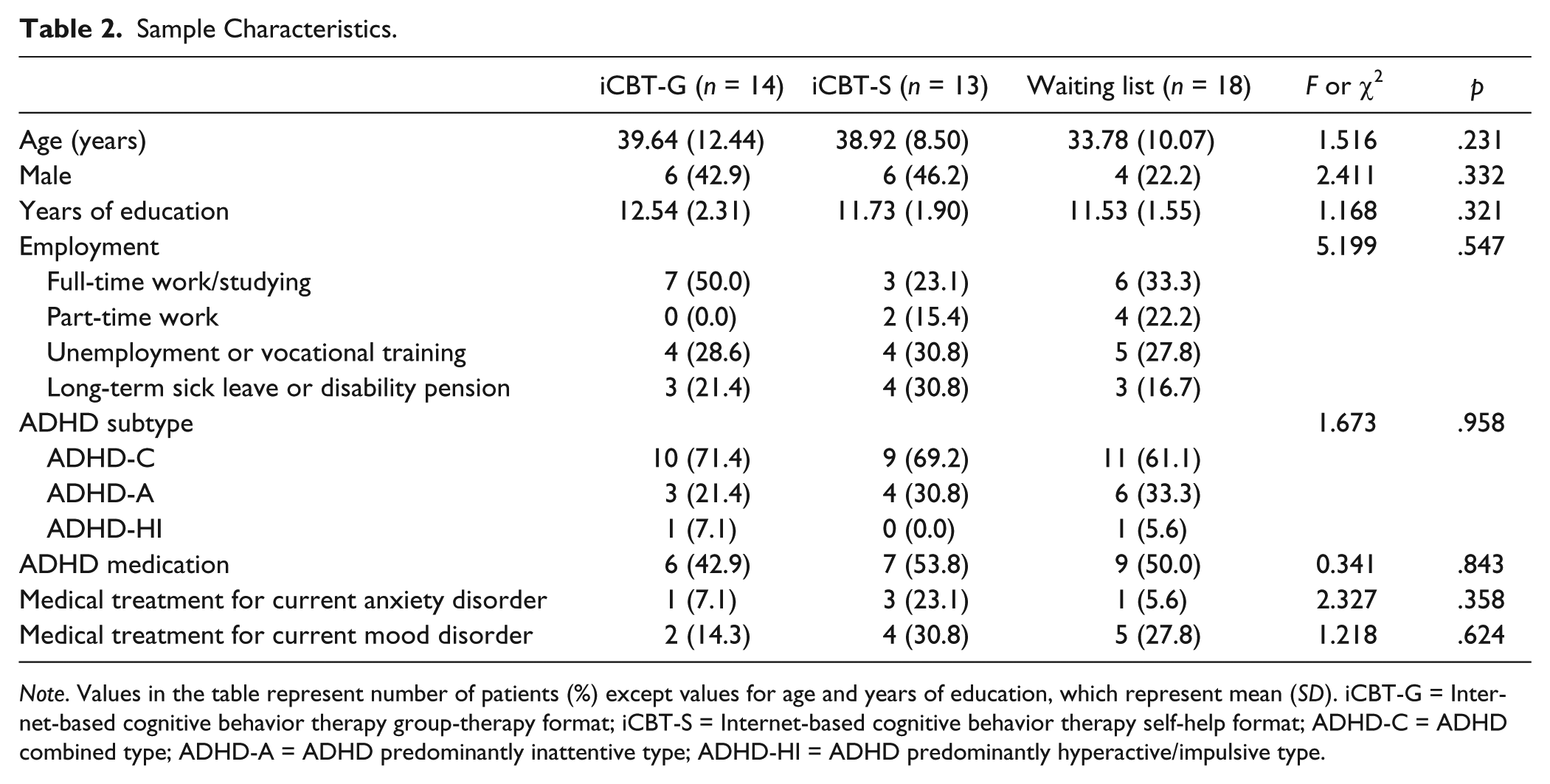
Note. Values in the table represent number of patients (%) except values for age and years of education, which represent mean (SD). iCBT-G = Internet-based cognitive behavior therapy group-therapy format; iCBT-S = Internet-based cognitive behavior therapy self-help format; ADHD-C = ADHD combined type; ADHD-A = ADHD predominantly inattentive type; ADHD-HI = ADHD predominantly hyperactive/impulsive type.
Estimate of Treatment Effect
Results for the primary and secondary outcome measures at each assessment point are presented as means and standard deviations in Table 3. Comparisons at the 6-month follow-up were made only between the iCBT-G and iCBT-S groups as patients in the waiting-list control group had ongoing treatment at this time.
ANCOVA Results From the Intention-to-Treat Sample and Descriptive Statistics for Outcome Measures.
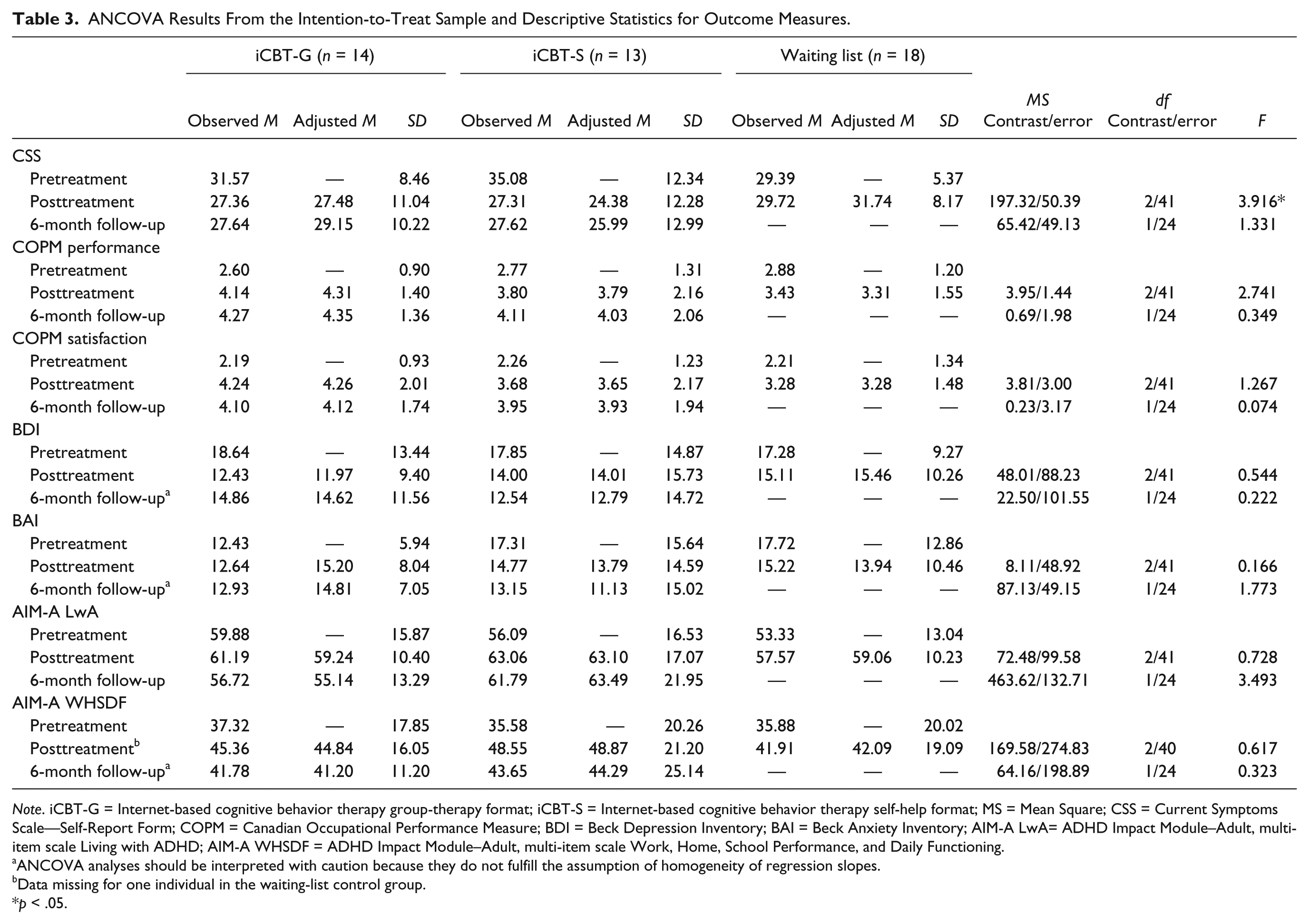
Note. iCBT-G = Internet-based cognitive behavior therapy group-therapy format; iCBT-S = Internet-based cognitive behavior therapy self-help format; MS = Mean Square; CSS = Current Symptoms Scale—Self-Report Form; COPM = Canadian Occupational Performance Measure; BDI = Beck Depression Inventory; BAI = Beck Anxiety Inventory; AIM-A LwA= ADHD Impact Module–Adult, multi-item scale Living with ADHD; AIM-A WHSDF = ADHD Impact Module–Adult, multi-item scale Work, Home, School Performance, and Daily Functioning.
ANCOVA analyses should be interpreted with caution because they do not fulfill the assumption of homogeneity of regression slopes.
Data missing for one individual in the waiting-list control group.
p < .05.
Posttreatment
ANCOVA of posttreatment scores for the primary outcome measure showed a significant main effect of the group factor on the CSS. Bonferroni-adjusted pairwise post hoc comparisons showed that the iCBT-S group had improved significantly more than the waiting-list controls; the patients rated themselves to have less severe ADHD symptoms, F(1, 41) = 7.558, p = .027, with a between-group effect size of d = 1.07. The between-group effect size for the posttreatment difference between the iCBT-G and the waiting-list control group in the CSS was moderate (d = 0.62), but not significant, when corrected for multiple comparisons, F(1, 41) = 2.810, p = .303. Exploratory analysis of the secondary outcome measures showed no significant differences between the three groups, but there was a trend toward a significant difference between the groups on the secondary dependent outcome measure COPM subscale performance. Post hoc comparisons showed that this trend was related to the iCBT-G group rating themselves higher on daily life functioning than the waiting-list controls, F(1, 41) = 5.470, p = .072, d = 0.87.
One of the inclusion criteria was that patients were stable on medication targeting ADHD. However, during the treatment period, patients in all three study groups had changes in their medication; one patient in the iCBT-G group had a changed dose, four patients in the iCBT-S group had changed doses, and three patients in the waiting-list control group had medication changes (two had started medication and one had changed the type of medicine). Because of the small subsample of patients with unstable medication, it was not possible to control for these changes in the analysis. Instead, we performed, a posteriori, a second analysis that excluded patients whose medication had changed to determine whether this would affect the significant result in the CSS. This ANCOVA showed a significant main effect of the group factor, F(2, 33) = 5.312, p = .010 in the CSS, and post hoc comparisons showed that the iCBT-S group was significantly more improved than the waiting-list controls, F(1, 33) = 9.189, p = .015, with a between-group effect size of d = 1.40. This analysis indicates that patients who did not have changes in medication had a greater reduction of ADHD symptoms.
Six-month follow-up
Exploratory analysis of the 6-month follow-up scores showed no significant between-group effect for the iCBT-G and iCBT-S groups on any of the primary or secondary outcome measures. Paired-sample t tests between posttreatment and follow-up for each group did not show any significant changes for any of the outcome measures, indicating that the iCBT-S group maintained their gains in the CSS 6 months after treatment.
Program Usage and Dropout Rate
The pretreatment dropout rate (i.e., patients who did not start treatment) was 31% (four patients) in the iCBT-S group and 0% in the iCBT-G group. Of the patients who started treatment, the mean number of completed modules was 6.93 (SD = 2.87) in the iCBT-G group and 6.11 (SD = 2.93) in the iCBT-S group, a difference that was not significant, t(21) = 0.661, p = .516. The treatment dropout rate, defined as patients who did not complete all nine treatment modules, was 50% (seven patients) in the iCBT-G group and 46% (six patients) in the iCBT-S group. This gives a total dropout rate of 50% in the iCBT-G group and 77% in the iCBT-S group.
The optional contact and support function in the program was used infrequently by patients in both the iCBT-S and iCBT-G groups. A total of 55 questions were addressed to the therapists, of which 27 were technical in nature and 28 related to the therapeutic work. In the iCBT-S group, two patients asked 22 questions (2 technical and 20 therapeutic), and in the iCBT-G group, eight patients asked 33 questions (25 technical and 8 therapeutic).
Discussion
This is the first report of a randomized controlled trial investigating the effect of an iCBT program for adults with ADHD. Patients from psychiatric outpatient clinics diagnosed with ADHD were randomized to iCBT in a self-help format (iCBT-S), iCBT with weekly group-therapy sessions (iCBT-G) or a waiting-list control group. ITT analysis showed a significant reduction in self-rated ADHD symptoms in the iCBT-S group in relation to waiting-list controls at posttreatment with a large between-group effect size (d = 1.07). The improvement at posttreatment was maintained at 6-month follow-up. No significant difference was found between the iCBT-S and the iCBT-G groups. None of the secondary outcome measures, BDI, BAI, COPM, or AIM-A, showed any significant difference between the groups.
The strengths of this study are its randomized controlled trial design and the recruitment of the sample from outpatient psychiatric care. The inclusion criteria were relatively broad and, with the exception of the comorbid disorders of borderline or antisocial personality disorder, bipolar disorder and ongoing substance abuse, the sample is representative of patients seeking help or evaluation for symptoms of ADHD at psychiatric or ADHD specialty clinics. Patients in this study reported, on average, a high degree of self-rated ADHD symptoms and comorbid levels of depression and anxiety (as measured by BDI and BAI), and a high proportion of them were unemployed and/or on long-term sick leave.
The major limitation of this study is the small sample size. The adjustment of the originally intended study resulted in small and uneven group sizes. One effect of this is that the study may have been underpowered to detect small to moderate differences. For example, the between-group effect size for the posttreatment difference between the iCBT-G and the waiting-list control group on the CSS was moderate but not significant, and there was a trend toward a significant difference between the iCBT-G and the waiting-list control group on the COPM subscale performance measure. Another effect of the small sample size was that not all of the analyses and distributions fulfilled the assumptions of normality, homogeneity of variance, and homogeneity of regression slopes. Of the 56 distributions (8 groups × 7 instruments) included in the analyses, 10 did not fulfill the assumption of normality. Two analyses at 6-month follow-up did not fulfill the assumption of homogeneity of variance and three analyses at 6-month follow-up did not fulfill the assumption of homogeneity of regression slopes. Data transformations improved the distributions and ensured that the analyses fulfilled the assumptions of homogeneity of variance and homogeneity of regression slopes. Analyses using transformed data did not affect the results, and for this reason we chose to report only the original data.
Another limitation of this study is that it did not include any form of attention-matched control condition. Because the patients in the treatment groups received more attention, nonspecific therapeutic effects could have influenced the results. Yet, another limitation was that only self-ratings were used. It is common practice in psychotherapeutic and pharmacological studies to use clinical expert rating scales as primary outcome measures. This has also been the standard practice in studies, particularly pharmacological studies, on adult ADHD, where the most frequently used instruments have been the ADHD-Rating Scale–IV (ADHD-RS-IV) and the Conners’ Adult ADHD-Rating Scale–Observer Version (CAARS-O-18; Rosler, Retz, & Stieglitz, 2010). Unfortunately, none of these instruments, or other similar observer rating scales, have been translated into Swedish or psychometrically evaluated in Sweden, and such tasks were beyond the scope of this study. Studies that have investigated the concordance between self- and other (investigator or informant) ratings of current ADHD symptoms have, in general, shown moderate to high agreement (Adler et al., 2008; Kooij et al., 2008), including the CSS (Barkley, Knouse, & Murphy, 2011). In a meta-analysis of the efficacy of methylphenidate, Faraone, Spencer, Aleardi, Pagano, and Biederman (2004) found that physician ratings of ADHD symptoms were associated with larger effect sizes. Based on the research available today concerning the source (self or others), Barkley and colleagues state that you cannot tell which of these sources is more valid than the other in indicating the degree of ADHD (Barkley et al., 2011). Until more research has been done and it has been determined which source is the better predictor of impairment or treatment response, it is desirable to include both sources of ratings of ADHD symptoms.
One hypothesis in this study was that the support provided by weekly group meetings would benefit the patients of the iCBT-G group and result in better outcomes for them than for those who worked alone with the Internet-based program. This proved not to be the case. Group CBT-based treatment programs for adults with ADHD have been evaluated more frequently than individual therapy programs (Philipsen, 2012). In their review of CBT trials for adults with ADHD, Knouse and Safren (2010) stated that when comparing the different CBT-based treatment packages from both open and controlled trials, neither number of treatment sessions or format (group vs. individual) appeared to have any association with treatment effect. In contrast to the current study, which had an individual self-help format with minimal therapist contact, studies included in Knouse and Safren’s analysis used traditional individual therapy with regular contact between therapist and patient. There is therefore no obvious reason why the iCBT-G group did not improve as much as the iCBT-S group in the current study. Few studies have examined individual therapy regardless of the degree of support, and as far as we know, no study has directly compared individual therapy with group CBT-based therapy for adults with ADHD. Hypothetically, there are some characteristics of the group format that may make it less effective for ADHD patients: (a) participating in group discussions and exchanging experiences with other patients can become the main reason some patients participate in the treatment, at the expense of less focus on treatment techniques—in the current study, the group leaders often found themselves in the position of having to remind patients of the meeting agenda when, for example, the group got caught up in sharing the encounters they had experienced in their dealings with previous health care providers; (b) the reduced attention span and susceptibility to distraction typical of patients with ADHD could make them less suited to the group format, with its high degree of complex information processing; (c) participants in a group might feel that they have done what is expected of them simply by attending group meetings, rather than also spending additional time and effort on homework assignments. Unfortunately, there was no documentation of the level of compliance with homework assignments in the current study.
Internet-delivered treatments potentially have several advantages over more traditional treatments; they may reduce therapist time and waiting lists, reach patients in areas where psychological or psychosocial treatment is not available, and offer more flexibility for the patient. However, delivering treatment via the Internet could also have disadvantages; it may not be suitable for people with limited computer skills, reading and/or writing difficulties or cognitive impairments, and not all patients want to communicate through computers. These factors could potentially affect results and dropout rates.
In a review of 19 studies of Internet-based treatment for psychological disorders, Melville and colleagues found that the total average dropout rate was 31% (range 2%-83%) and the average dropout rate during treatment was 21% (range 0%-78%; Melville, Casey, & Kavanagh, 2010). However, only 10 of the 19 studies reported dropouts at different stages of the treatment process. In comparison, the dropout rate in the current study was relatively high with an average dropout rate during treatment of 48%. At the same time, the average number of completed modules among those who started treatment was relatively high in both groups, 6.93 (SD = 2.87) in the iCBT-G group and 6.11 (SD = 2.93) in the iCBT-S group, which may account for the positive result of a reduction in ADHD symptoms. Evidence for any specific variable that could influence dropout rates in Internet-based treatments for psychological disorders is still limited (Melville et al., 2010). The high dropout rate of the current study suggests it could be that, because of the symptoms of their disorder, patients with ADHD are at greater risk of dropout when the content is too demanding or not sufficiently stimulating, or when there is no immediate gain from the intervention. Other possible factors that could influence dropout rates are the characteristics of the sample being studied and the degree of support or guidance offered during treatment. In a majority of studies conducted on iCBT, participants have been recruited through newspaper, television, or website advertisements (Cuijpers et al., 2008). It has been proposed that self-referred participants who have expressed interest in Internet-based treatment are probably very motivated (Cuijpers et al., 2008). Research results imply that different referral sources refer patients with differing levels of comorbidity, severity, functional disability, and motivation and that self-referred participants are more likely to have less severe symptoms, be more motivated, and have fewer work or social disabilities (Mataix-Cols, Cameron, Gega, Kenwright, & Marks, 2006). In this study, we used a clinical psychiatric sample with a relatively high degree of self-rated ADHD symptoms and comorbid levels of depression and anxiety, which could be one possible explanation for the high dropout rate in relation to other studies on iCBT. In a randomized controlled trial of a CBT-based 10-module Internet self-help treatment of depression, Berger and colleagues (2011) compared guided with unguided self-help. Participants in the unguided condition received the program without any support. Besides access to the program, participants in the guided condition could contact the therapist whenever they wanted and received a weekly scheduled e-mail with feedback based on their work with the program. At posttreatment, both groups showed significant symptom reduction compared with a waiting-list group, with between-group effect sizes of d = 1.14 for guided self-help and d = 0.66 for unguided self-help. The dropout rate during treatment was 64% in the unguided condition with an average of completed modules of 6.8. The corresponding numbers were 44% and 8.52% in the guided condition. These results indicate that both the treatment effect and the dropout rate can be affected by the degree of support. Based on the high dropout rate in our study, which has been seen in other Internet-based treatments, it is important that future research explore variables that could influence dropout.
Although the number of studies on CBT-based programs for adult ADHD is increasing, and the overall results from these interventions are promising, it is still unclear what constitutes optimal treatment in terms of format (individual or group), selection of interventions and intensity and duration of treatment (Knouse & Safren, 2010). These are all variables that need to be addressed in future studies.
The preliminary findings from this study indicate that CBT treatment in an Internet-based self-help format with minimal therapist contact can be a promising alternative treatment for adults with ADHD. However, the study was small with some major limitations and the results should be considered as preliminary. Larger studies, with more rigorous methodology, preferably including attention-matched controls, assessment of primary outcomes by independent assessors, and strategies to minimize dropout, are needed to investigate further the efficacy of iCBT for this group of patients.
Footnotes
Acknowledgements
We thank Gunnar Ganse, Eva Holmkvist, and Tuula Wallsten for their participation and invaluable contribution in the implementation of this study.
Authors’ Note
R. P., S.S., and K.E.-S. were responsible for the study concept and design. R.P. performed the data analysis and drafted the first version of the manuscript. S.S. and K.E.-S. contributed to the acquisition of data. All authors critically reviewed content and approved the final version for publication.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.P. is a partner and shareholder in the company Livanda—Internet Clinic, Ltd., that constructed and owns the rights to the Internet-based treatment program In Focus. RP was also involved in the design and construction of the program.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by the “Sjukskrivningsmiljarden,” an economic fund established by the Swedish government to encourage Swedish county councils to give higher health care priority to sick leave and to develop processes and methods to reduce its frequency. In addition, research grants for K.W.N., as the principal investigator, have been received from Forskningsrådet för samhällsvetenskap och arbetsliv (FAS), Systembolagets råd för alkoholforskning (SRA), Swedish Brain Foundation, The Uppsala and Örebro Regional Research Council, Fredrik and Ingrid Thurings Foundation, the County Council of Västmanland, the König-Söderströmska Foundation, The Swedish Psychiatric Foundation, and Svenska Spel Research Foundation. None of these organizations had a role in the study design, data collection, data analysis, data interpretation, or writing of the report.