
Abstract
Keywords
Adults with ADHD typically trail behind various negative educational, occupational, and relational experiences and detours, suffering from poor self-concept, poor self-esteem, and functional impairment in several areas of life (e.g., Mannuzza & Klein, 2000). In many cases, psychotherapeutic support is crucial for coping with these burdens, but even more so to alleviate ADHD core symptoms, that is, inattention, hyperactivity, and impulsivity. However, only a small number of studies achieved to demonstrate the effects on core ADHD symptoms following randomized and controlled study designs. To date, all evidence-based psychotherapies for adults with ADHD are grounded in cognitive behavior therapy (CBT), which emerged as effective in improving ADHD symptoms in single (Safren et al., 2005) and group settings (Emilsson et al., 2011; Solanto et al., 2010; Weiss et al., 2012). In search of adjuncts or alternatives to drug treatment, certain other (“third wave”) behavioral therapies, that is, acceptance and mindfulness-based approaches, have been adapted to the specific requirements of adults with ADHD (Hesslinger et al., 2002; Mitchell et al., 2013; Philipsen et al., 2007; Zylowska et al., 2008). Hesslinger and co-workers were the first to transform Marsha Linehan’s dialectical behavior therapy (DBT) for borderline personality disorder (BPD) into a group-based skills training program for adults with ADHD (Hesslinger et al., 2002; Philipsen et al., 2007). The DBT-derived concept assumes significant symptom overlap between BPD and ADHD, for example, stress intolerance, hot temper, and emotion dysregulation, which are known to be associated with impulsive behaviors and interaction conflicts. Primary DBT strategies, such as acceptance, validation, commitment, and behavioral analysis, were adjusted to support patients to “control ADHD rather than to be controlled by ADHD.” The program also entails the principle of mindfulness as a core DBT feature. Mindfulness, which may enrich “western” cognitive behavior approaches substantially, derives its origin from eastern, mainly Buddhist, meditation practices. Mindfulness denotes constant, non-reactive, and accepting awareness of present thoughts, emotions, and body states. To engage with and to disengage from these inner states in a reflective way facilitates the reduction of inner stress and automatic responding (Bishop et al., 2004; Kabat-Zinn, 2003).
There is growing evidence from empirical research that mindfulness training has an impact on attention control functions (Malinowski, 2013), which principally encourages its adaptation to and application in patients with ADHD. Philipsen and colleagues (2007) reported that their patients considered the mindfulness elements incorporated in their DBT-derived group psychotherapy as most helpful. Moreover, Zylowska et al. (2008) demonstrated that an ADHD-adapted 8-week mindfulness training program for adolescents and adults with ADHD, comprised of weekly 2.5-hr group sessions and daily at-home meditation practice, and including psychoeducational components to ameliorate self-esteem and self-regulation, was feasible (with high adherence and satisfaction rates), and might reduce ADHD and comorbid pathology. Recently, Mitchell and co-workers (2013) conducted a randomized pilot study on adults with ADHD to assess the feasibility, acceptability, and preliminary efficacy (as to ADHD core symptoms, executive functioning, and emotion dysregulation symptoms) of an 8-week group-based mindfulness treatment (n = 11) compared with a waitlist group (n = 9). The authors found positive treatment feasibility and acceptability, and reported improvement for the treatment group in self-reported and clinician-rated ADHD symptoms, and furthermore in executive functioning and emotion dysregulation.
Given the growing empirical evidence for the application of mindfulness training in ADHD, we designed and conducted an explorative open study to assess the possible treatment effects of an ADHD-adapted mindfulness-based group training compared with the abovementioned DBT-oriented skills training, which has already been established in some European countries. We expected that the mindfulness-based training would be similarly feasible and acceptable, similar to the skills training, and that ADHD symptoms would decrease in both groups to a similar extent, as measured with the Wender–Reimherr Interview (WRI) total score. However, we anticipated group differences with respect to the particular ADHD symptom domains and the non-ADHD features, such as self-efficacy and mindfulness.
Method
Participants
Ninety-one adults with ADHD who have been diagnosed according to the full Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) criteria for ADHD were recruited from our outpatient unit for adults with ADHD. Pre-study ADHD diagnoses were established using the short version of the Wender Utah Rating Scale (German WURS-k; Retz-Junginger et al., 2002) to retrospectively assess childhood ADHD symptoms, in addition to self-rating Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung im Erwachsenenalter: Selbstbeurteilungsskala (ADHS-SB; German “ADHS-SB”) and interviewer rating (German “ADHS-DC”) instruments (Rösler et al., 2004).
Groups were balanced regarding gender, age, education, ADHD subtypes, ADHD severity, Axis I and Axis II comorbidity (except BPD, see below), and medication status (see Table 1).
Participant Baseline Characteristics.
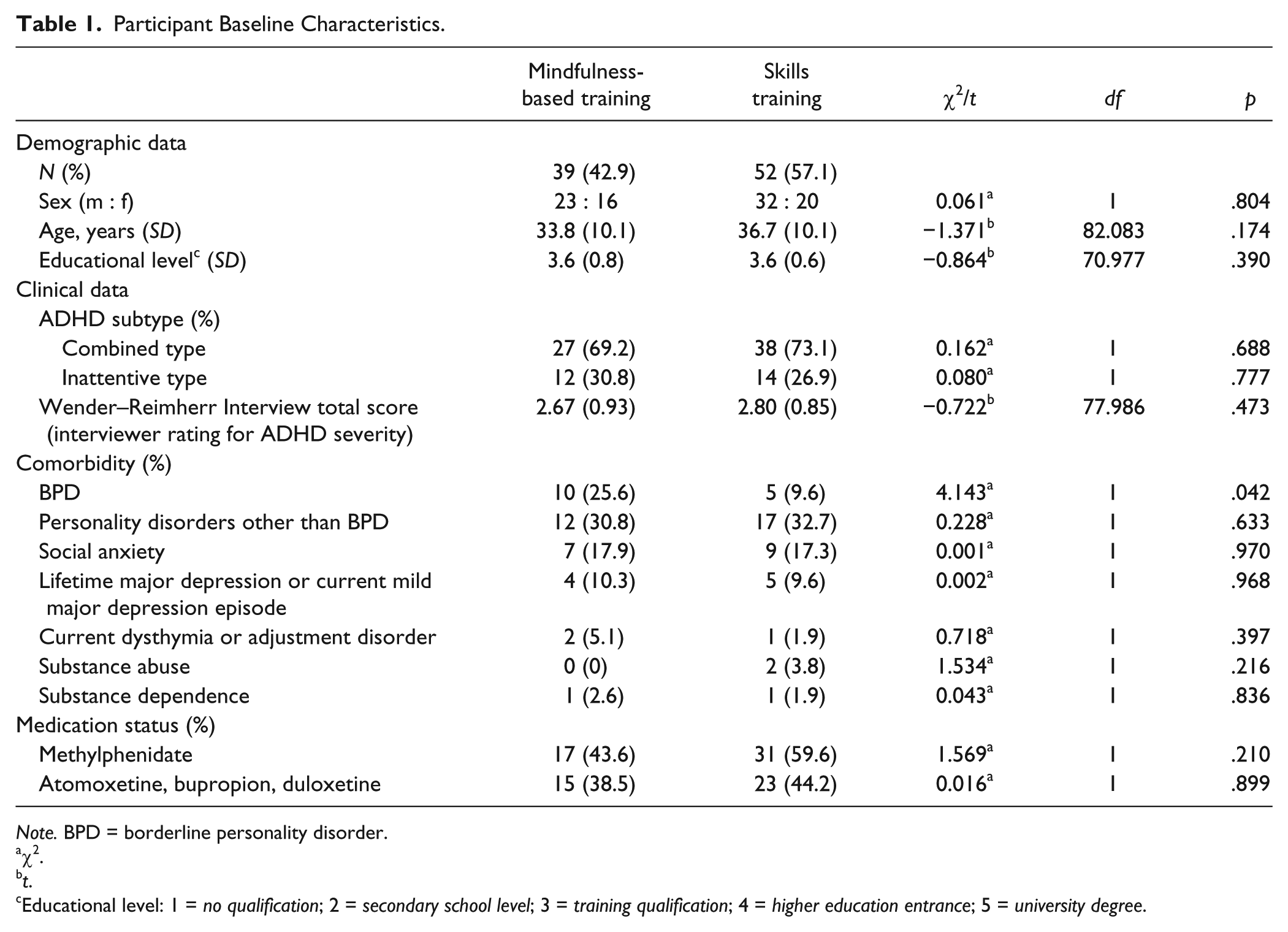
Note. BPD = borderline personality disorder.
χ2.
t.
Educational level: 1 = no qualification; 2 = secondary school level; 3 = training qualification; 4 = higher education entrance; 5 = university degree.
All participants gave full informed consent, and the Ethics Committee of the Medical Faculty of the Ruhr University Bochum approved the study.
Study Design, Exclusion Criteria, and Procedures
We chose a pragmatic open design to compare two active behavioral interventions. Participants with a current moderate or severe major depression episode, Bipolar I disorder, lifetime psychotic disorders, or current general anxiety disorder or panic disorder (with or without agoraphobia) were excluded from the study.
Participants were assigned for the first time either to a mindfulness-based training group (MBTG) or to a DBT-oriented skills training group (STG), that is, none of the participants were familiar with either approach. Group allocation followed individual requirements, such as patient- or therapist-estimated, need to improve organizational skills (which was addressed primarily by the skills training), patients’ preferences, or individual scheduling issues. The MBTG and STG with 5 to 10 patients each were performed concurrently on different week days. Participants were only allowed to miss a maximum of two sessions.
Measures
The WRI (Rösler et al., 2008) and four self-designed Likert-type scales (ranging from 0 = none, not present to 10 = extremely present, most often true), covering the nine inattention items and nine hyperactivity/impulsivity symptoms of the A-criterion of the DSM-IV (APA, 1994), were used for pre- and post-assessment of ADHD symptoms. The WRI is an expert-rated scale comprising the seven symptom domains of the Utah Criteria: attentional difficulties, hyperactivity/restlessness, (hot) temper, affective lability, emotional overreactivity, disorganization, and impulsivity. Each domain section includes an interview part with several questions about the respective ADHD symptom domain—each question scored from 0 to 2; (a) none/not present (score 0), (b) mildly/rarely present (score 1), (c) moderately/sometimes present (score 2), (d) severely/often present (score 2*), and (e) very severely/very often present (score 2*)—and a scale for synoptic expert rating scoring from 0 (none/not present) to 4 (very severely/very often present). Because of possible ceiling effects when using the first scale (*), we decided to use the second (synoptic) expert rating scale with levels from 0 to 4. Therefore, our WRI total score, as the primary outcome parameter, summarizes the seven synoptic expert ratings of the symptom domains.
The first two of four self-designed DSM-IV (APA, 1994)-based Likert-type scales served for self-rating the subjective impairment (1) and burden (2) of the 18 ADHD symptoms on the participant, and the second two scales were for other-ratings (partners, relatives) concerning the perceived quantity of the ADHD symptoms (3), and how much the other person feels disturbed by the ADHD symptoms of the participant (4).
The Mindful Attention Awareness Scale (MAAS; Brown & Ryan, 2003) is a 15-item questionnaire with scores between 1 (almost always) and 6 (almost never). Because the items depict non-mindful cognitive style and behavior, higher scores reflect higher levels of mindfulness.
Self-efficacy as an important basis for motivation, change commitment, and actual change was measured by means of the Generalized Self-Efficacy Scale (GSES; Schwarzer & Jerusalem, 1995). The GSES is a self-rating instrument comprised of a 10-item Likert-type scale scored from 1 (not true) to 4 (completely true).
Treatment Programs
The DBT-oriented skills training exactly followed the Freiburg program (Hesslinger et al., 2002; Philipsen et al., 2007) with thirteen 2-hr sessions: (a) introduction and clarification, (b) neurobiology/mindfulness I, (c) mindfulness II, (d) chaos and control, (e) dysfunctional behavior/behavior analysis I, (f) behavior analysis II, (g) emotion regulation, (h) depression/medication in ADHD, (i) impulse control, (j) stress management, (k) substance dependency, (l) ADHD in relationships/self-respect, and (m) retrospect and outlook.
Accordingly, the mindfulness-based training was comprised of 13 weekly 2-hr sessions: (a) introduction, (b) about mindfulness, (c) first exercises, (d) further exercises, (e) “Body Scan” (Jon Kabat-Zinn), (f) to be mindful with emotions and body sensations, (g) to be mindful with sudden impulses and reactions, (h) how to accept emotions, (i) let go (breathing exercise), (j) being mindful while walking, (k) going into depth, (l) repetition, and (m) finish and farewell.
The mindfulness-based training was created by the authors and based on Jon Kabat-Zinn’s Mindfulness-Based Stress Reduction (MBSR) program (Kabat-Zinn, 1982) and the mindfulness part of Marsha M. Linehan’s DBT for patients with BPD (Bohus & Wolf, 2009). The first two sessions are psychoeducative and address the principle of mindfulness, its origins, and possible effects on ADHD symptoms. Session 3 (“First exercises”) is a brief introduction into (a) three aspects of being mindful, that is, to observe, to describe, and to fully participate in the current situation; and (b) how mindfulness works, that is, non-judging, perpetually concentrated, and effective, which is followed by two short exercises, that is, to observe the texture and taste of a truffle and to observe one’s breath. Sessions 4 to 6 provide further exercises, all taken from the MBSR program. Sessions 7 to 10 mainly convey self-created adaptations to the specific situation of adults with ADHD, complemented by MBSR exercises. Session 11 concentrates on individual difficulties with the mindfulness exercises, dealing with two or three representative problems in corresponding group exercises.
In all sessions of both interventions, PowerPoint slides were provided for didactic reasons. Sessions 1 to 12 of both interventions were formally followed by home exercises using printed instructions and memos in the STG, and, either formally by written instructions for particular mindfulness meditation (but not yoga) exercises, or informally by practicing mindfulness during everyday activities (such as washing the dishes.) in the MBTG. Sessions of both interventions were divided into two parts of about 1 hr each, with the first section dealing with the home exercises and the second section providing new issues.
Therapists
Sessions were conducted by an experienced psychologist and psychotherapist (T.H.) and an experienced consultant in psychiatry and psychotherapy (M.A.E.), both with several years of experience in diagnosing and treating adults with ADHD, and at least 5 years of experience in leading DBT groups including mindfulness skills training and other mindfulness-based groups, such as mindfulness-based cognitive therapy (MBCT), for patients with depression.
Statistical Analyses
Statistical analyses were carried out using SPSS Version 20 for Mac (IBM Corp., Armonk, New York, United States). The one-sample Kolmogorov–Smirnov test was used to confirm normal distribution of all interval-scaled variables. Group comparisons with respect to gender, age, education, ADHD symptomatology, ADHD subtypes, comorbidities, and medications were conducted by applying t tests and Pearson’s chi-square tests. Correlations between the MAAS and ADHD symptom scales assessing inattention were established using Pearson’s r. Possible treatment effects were investigated by performing general linear models (GLMs) with repeated-measures analyses of variance. Cohen’s measure of sample effect size for comparing two sample means, that is, pre- and post-comparisons of means, was then applied to assess the possible treatment effects. Due to multiple testing, only results with a value of p < .01 were considered significant.
The prevalence of BPD in the MBTG was twice (n = 10, 25.6%) as high as in the STG (n = 5, 9.6%; χ2 = 4.143, df = 1, p = .042). Therefore, all GLMs with repeated-measures analyses of variance were controlled for borderline personality. Moreover, control for medication, that is, treatment with methylphenidate and other catecholaminergic drugs (atomoxetine, bupropion, and duloxetine) as covariates, was taken into account in the GLMs.
Results
Outcome Variables
With respect to the main outcome variable, the WRI total score (synoptic interviewer rating), an absence of a significant interaction (time by group) indicated that neither group was superior relative to the other regarding the reduction of total ADHD symptoms (see Table 2). However, there was a tendency toward a greater response quote (i.e., a WRI total score decrease ≥30%) in the MBTG compared with the STG: 12 from 39 (30.8%) participants in the MBTG compared with 6 from 52 (11.5%) participants in the STG exhibited such a response (χ2 = 5.194, df = 1, p = .023).
ADHD Symptomatology, Mindfulness and Self-Efficacy at Baseline and After Therapy.
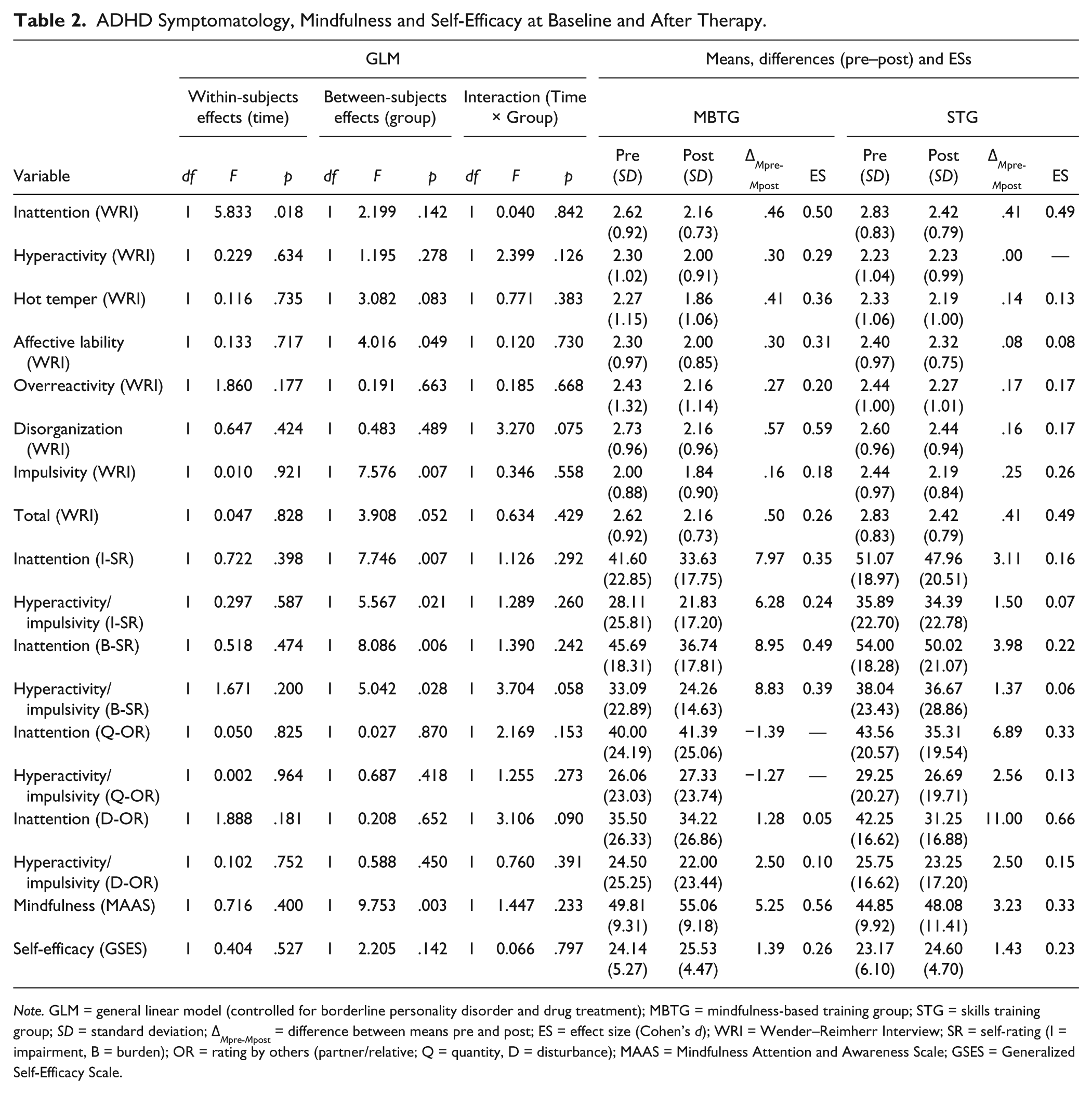
Note. GLM = general linear model (controlled for borderline personality disorder and drug treatment); MBTG = mindfulness-based training group; STG = skills training group; SD = standard deviation; ΔMpre-Mpost = difference between means pre and post; ES = effect size (Cohen’s d); WRI = Wender–Reimherr Interview; SR = self-rating (I = impairment, B = burden); OR = rating by others (partner/relative; Q = quantity, D = disturbance); MAAS = Mindfulness Attention and Awareness Scale; GSES = Generalized Self-Efficacy Scale.
Concerning all the secondary outcome variables (ADHD-related, MAAS, and GSES scores), no significant time by group interactions emerged, which indicates similar pre- and post-effects in both groups.
Of note, significant interaction effects (time by BPD status) occurred in the GLMs regarding two WRI scores: “affective lability” (F = 7.305, p = .009) and the WRI total score (F = 9.628, p = .003), which implies that the participants with borderline comorbidity (of both intervention groups) displayed greater symptom reduction over time than the other participants. Moreover, a significant interaction term for “time by methylphenidate treatment” in the GLM with “disorganization” of the WRI as the outcome variable suggests a greater (possible treatment) effect over time in patients (of both intervention groups) with methylphenidate medication compared with patients without such medication (F = 7.189, p = .009).
The effect sizes for the primary outcome parameter and all other variables were in the small-to-moderate range.
Adherence and Acceptability
All participants completed the study, that is, participants missed a maximum of 2 of 13 sessions, which suggests the practicability of the interventions. In all, 21 (53.8%) participants of the MBTG and 29 (55.7%) participants of the STG missed one session. Three (7.7%) participants of the MBTG and 6 (11.5%) participants of the STG missed two sessions. Sessions were missed mainly due to clashing appointments. Absence from one (χ2 = 0.033, p = .855) or two (χ2 = 0.370, p = .543) sessions was equally distributed in the two groups. The majority of patients gave (unrequested) positive verbal feedback concerning the acceptability and subjective effectiveness of the interventions.
Discussion
There is worldwide expert agreement about the requirement of combined treatment strategies, that is, integrating pharmacotherapy, psychoeducation, and psychotherapy, to meet the specific needs of adults with ADHD, but we still face a paucity of evidence-based psychotherapy approaches. “Third-wave” behavior therapies for ADHD (mindfulness-based, dialectic, and meta-cognitive approaches) are still in the early stages of development, and clarification-oriented programs are completely lacking. The present study sought to compare two third wave programs in adult outpatients with ADHD: first, a novel mindfulness-based training and, second, a skills training using a well-established German program (Hesslinger et al., 2002; Philipsen et al., 2007), derived from DBT for BPD.
As expected, overall ADHD symptoms, measured by the WRI total score as the primary outcome parameter, decreased to a similar extent in both groups. Unexpectedly, however, no “time by group interactions” emerged, neither regarding the other WRI scores nor the scores of the ADHD scales for self- and others-ratings, or the scores of the MAAS and the GSES.
Compared with the results of Mitchell et al. (2013) who found highly significant “time by group” interaction effects in GLMs and large effect sizes for a mindfulness meditation training (vs. a waitlist group), our interventions did not result in any such significant interaction effects as an indicator of superiority of one program over the other, and the effect sizes were in the small to maximally medium range in our study. Moreover, Mitchell and co-workers reported that 63.6% of the participants in the mindfulness treatment group displayed a reduction of ADHD symptoms ≥30%. In comparison, the proportion of participants in our MBTG with such symptom decreases indicating that possible treatment response was only 30.8% (compared with 11.5% in the STG). However, the difference between groups in our study was not significant at p < .01, and it may be, at least in part, due to the higher prevalence of BPD comorbidity in the MBTG and a higher reduction of ADHD symptoms in participants of both groups with BPD comorbidity.
The latter finding reveals one important limitation of this study, which is the lack of matching groups concerning BPD (and other comorbidities). Regarding group assignment, therapists possibly felt that the MBTG might be more suitable for the patients with obvious emotional instability, and the STG would better address organizational problems. Perhaps some patients with BPD comorbidities preferred the novel mindfulness-based approach, which might be another reason for this bias. Moreover, we did not control for depression and anxiety.
Furthermore, to assess the efficacy (and feasibility) of a novel treatment, for example, a mindfulness-based intervention, a randomized controlled trial (RCT) with a waitlist group for comparison, as performed in the study of Mitchell et al. (2013), would have been suitable, but non-randomization caused marked biases in this study.
Another central weakness is that, in particular, the new mindfulness-based intervention lacked impact and structured treatment monitoring. Regarding impact, the use of a CD audio program with (instructions for) formal meditation exercises, as incorporated in the “Mindfulness Prescription for Adult ADHD” (Mindfulness Awareness Practices (MAPs) program; Zylowska, 2012), would have been helpful. As to structured monitoring, the administration of electronic diaries using handheld computers, as performed by Mitchell et al. (2013), may enhance both the accuracy of the follow-up assessment and treatment consistency. Moreover, a flowchart to assess participant progress, as suggested by Solanto et al. (2010), and an explicit assessment of the reasons for missing sessions, as performed in many other intervention studies, could improve patients’ commitment, adherence, and outcomes. Unfortunately, we did not incorporate such flowcharts and were limited to pre- and post-assessment comparisons.
Further limitations pertain to some of our assessment instruments. First, to compare ADHD symptom reduction between workgroups, a common instrument for the rating of ADHD symptoms and the associated psychosocial implications should be used, for example, the Current ADHD Symptom Scale (Barkley & Murphy, 2006). Instead, we used the expert rating of the WRI. Second, the MAAS and other mindfulness scales have been criticized for measuring a component of one’s daily attention rather than the essence of mindfulness (Grossman, 2011). Accordingly, we found small-to-moderate negative correlations between the MAAS and inattentive ADHD symptoms at baseline, as measured with the WRI Inattention subscale and the DSM-IV (APA, 1994)-based Likert-type scales assessing self-rated impairment and burden by inattention. This finding indeed suggests partial overlap between mindfulness and features of attention. However, attention control functions might actually be part of the condition of being mindful (Malinowski, 2013), and from a therapeutic perspective, the overlap between mindfulness and attention functions is desirable rather than problematic. Third, an additional limitation is the use of self-designed Likert-type scales, which have not been validated.
Finally, raters and evaluators were not blind to the assignment of participants to the two intervention arms.
In conclusion, this pilot study supports the practicability and acceptability of a MBTG compared with an established STG program in adults with ADHD. Both programs had a similar impact on ADHD symptomatology, facets of mindfulness, and self-efficacy with small-to-medium range effect sizes. Possible reasons for the comparatively weak outcome of this study are discussed.
Footnotes
Authors’ Note
Marc-Andreas Edel and Tanja Hölter contributed equally to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.