
Abstract
Keywords
Introduction
ADHD is a chronic, common, inherited, and disabling developmental disorder with early onset, and core symptoms of inattentiveness, impulsivity, and hyperactivity (Polanczyk & Rohde, 2007). Cognitive deficits in executive functioning, including attention, working memory, and inhibition (Seidman, 2006), are common in ADHD.
Many patients also experience difficulties in arousal, motivation, and emotional regulation (Nigg & Casey, 2005). The diagnosis is associated with drug abuse, sick leave, unemployment, and criminality (Barkley & Cox, 2007). Comorbidity is common and up to 80% of adults also fulfill diagnostic criteria for disorders such as depression, anxiety disorders, sleep disorders, and personality disorders (Biederman, Newcorn, & Sprich, 1991; Kessler et al., 2006). Thus, when left untreated, costs for the individual and society are high.
The core symptoms of ADHD contribute to impairments in executive functioning and inhibitory control, in working memory, and in motivation. These deficits prevent the acquisition and implementation of compensatory skills with a disruption in adaptive behaviors like organizing and planning, leading to difficulties in handling everyday challenges.
Due to years of chronic underachievement and multiple experiences of failure, adults with ADHD often develop maladaptive negative beliefs and emotions, which increase avoidance behavior and mood disturbance (Mongia & Hechtman, 2012).
Further, deficits in emotional regulation are common in ADHD (Barkley, 2010; Marx et al., 2011) as well as feelings of emptiness, and brief recurrent depressive or dysphoric states. The literature reveals a possible comorbidity between ADHD and borderline personality disorder. Deficits in affect regulation, impulse control, low self-esteem, and destructive behaviors such as substance abuse are common features in both ADHD and borderline personality disorder (Lampe et al., 2007; Philipsen, 2006). Because of difficulties in impulse control and emotional instability, there is an increased probability of interpersonal conflicts in ADHD (Hesslinger et al., 2002).
A majority of patients who receive an ADHD diagnosis are only offered pharmacological treatment, which is not enough for about 50% of the adults due to insufficient response, lack of response, and side effects (Torgersen, Gjervan, & Rasmussen, 2008). Thus, a need for complementary interventions such as psychological treatments is strongly emphasized (CADDRA, 2011; Seixas, Weiss, & Müller, 2011). A recent study also demonstrated that the highest proportion of long-term outcomes was reported to improve with combination treatment (Arnold, Hodgkins, Caci, Kahle, & Young, 2015).
Research regarding psychological interventions for adults with ADHD is limited. Cognitive behavioral therapy (CBT) oriented approaches have been studied the most (Knouse & Safren, 2010; Philipsen, 2012) and studies of CBT for adult ADHD show promising results (Bramham et al., 2009; Emilsson et al., 2011; Mongia & Hechtman, 2012; Ramsay & Rostain, 2011; Safren, Otto, et al., 2005; Weiss et al., 2012; Solanto et al., 2010). Dialectical behavior therapy (DBT), modified according to the special needs of patients with ADHD, has also shown promising results with moderate to large effect sizes in treatment of adult ADHD (Hesslinger et al., 2002; Hirvikoski et al., 2011; Philipsen, Jans, Graf, et al., 2015).
Moreover, studies of CBT and DBT show that structured short-term therapies are promising in reducing ADHD-related symptoms and increasing quality of life (Hirvikoski et al., 2011).
In the treatment of ADHD, CBT has mainly been used to enhance executive functions such as planning, structuring, and organizing everyday life (Safren, 2005a). DBT has mainly focused on mindfulness interventions, as well as enhancing skills to handle relationships, low self-esteem, impulsivity, and consequence thinking (Hesslinger et al., 2002).
A combination manual based on elements from both manuals could offer patients a treatment which addresses the complexity and variety of problems associated with ADHD in a way that we consider each manual, when used separately, cannot do. However, no previous study has evaluated the effects of a treatment manual that combines techniques from both of these therapeutic treatments.
The primary objective of this pilot study was to investigate whether a novel treatment, primarily based on selected components from established CBT and DBT treatment manuals (Hesslinger, Philipsen, & Richter, 2004; Safren, 2005b), was feasible and showed a preliminary positive effect on symptoms, functioning, emotional regulation, depression, and quality of life, for adults with ADHD.
Secondary objectives were to further examine feasibility in terms of level of use, comprehension, and perceived benefit of the various treatment components as well as explore the relation between the use of each component and treatment outcome.
Method
Study Design
In this uncontrolled pilot study, patients were assessed pretreatment, posttreatment, and at 1 and 6 months follow-up. The study was approved by the Regional Ethics Committee of Stockholm with registration number (2012/333-31) and conducted at the Neuropsychiatric Unit at the Psychiatry Southwest Clinic, Stockholm County Council Health Care Services. Moreover, the study was registered at Clinicaltrials.gov with registration ID: NCT01659164.
Patient Characteristics and Recruitment
Patients with a primary ADHD diagnosis according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994), confirmed by their medical records, were recruited through specialized neuropsychiatric units in Stockholm. The units were chosen due to their generally high level of comprehensive diagnostic assessments of ADHD. The assessments included urine and blood tests (to rule out drug abuse and other primary somatic causes to the symptoms), semistructured childhood interview about ADHD symptoms with the patient and parents/relatives, diagnostic assessments for coexisting disorders, self-rating questionnaires about past and current ADHD symptoms, and physical assessment performed by a psychiatrist. Moreover, a neuropsychological assessment was conducted in most cases.
Interested patients who preliminarily met the inclusion criteria were screened by phone through a semistructured interview and received short information about the study and the planned intervention. If the patient fulfilled the inclusion criteria, a 2-hr assessment interview was conducted by a clinical psychologist with extensive training and experience in the field of ADHD. This interview was semi-structured and contained questions regarding the inclusion criteria (such as in depth examination of current medication use) in order to determine eligibility for the study. Consequently, the final decision regarding inclusion was made. Urinary drug screening was performed in cases where information about substance use was difficult to find through medical records. During the interview, ADHD symptoms were also assessed with the Adult ADHD Self Report Scale version 1.1 (ASRS-v1.1; Kessler et al., 2005) and with the clinician-rated ADHD Rating Scale IV (for adults; DuPaul, Power, Anastopoulos, & Reid, 1998 which gave the clinician the possibility to examine the patient`s reported symptoms and level of impairment in depth). Depressive symptoms were assessed via the patient-rated Montgomery-Åsberg Depression Rating Scale (MADRS-S; Svanborg & Asberg, 1994). All patients signed a written informed consent form.
To be eligible for the study, an individual was required to be 18 to 65 years old with an ADHD diagnosis according to DSM-IV, and to have current problems with inattention and/or impulsivity/hyperactivity defined as 17 or more points on at least one of the subscales of the ASRS. Another requirement was stable or no medication for ADHD or other psychiatric conditions 1 month before baseline, and no practical barriers to participate in the study that could be foreseen. Individuals were excluded from the study if data from medical records or from patients themselves indicated evidence of substance misuse up to 3 months before baseline, or if substance use was detected through a urine dipstick test. Other exclusion criteria were diagnosed organic brain injury, diagnosed intellectual disability (IQ ≤ 70), suicidality, an unstable psychiatric or somatic condition that could potentially affect treatment negatively, depression (assessed by a clinical psychologist or psychiatrist), and ongoing treatment with focus on reducing symptoms of ADHD.
Eighteen individuals met the study criteria and were asked to fill out pretreatment questionnaires. After completing these, patients could initiate treatment. Patients were divided into two groups: the first group underwent treatment from September to December 2012, and the second group from December 2012 to March 2013. The study flowchart is presented in Figure 1.
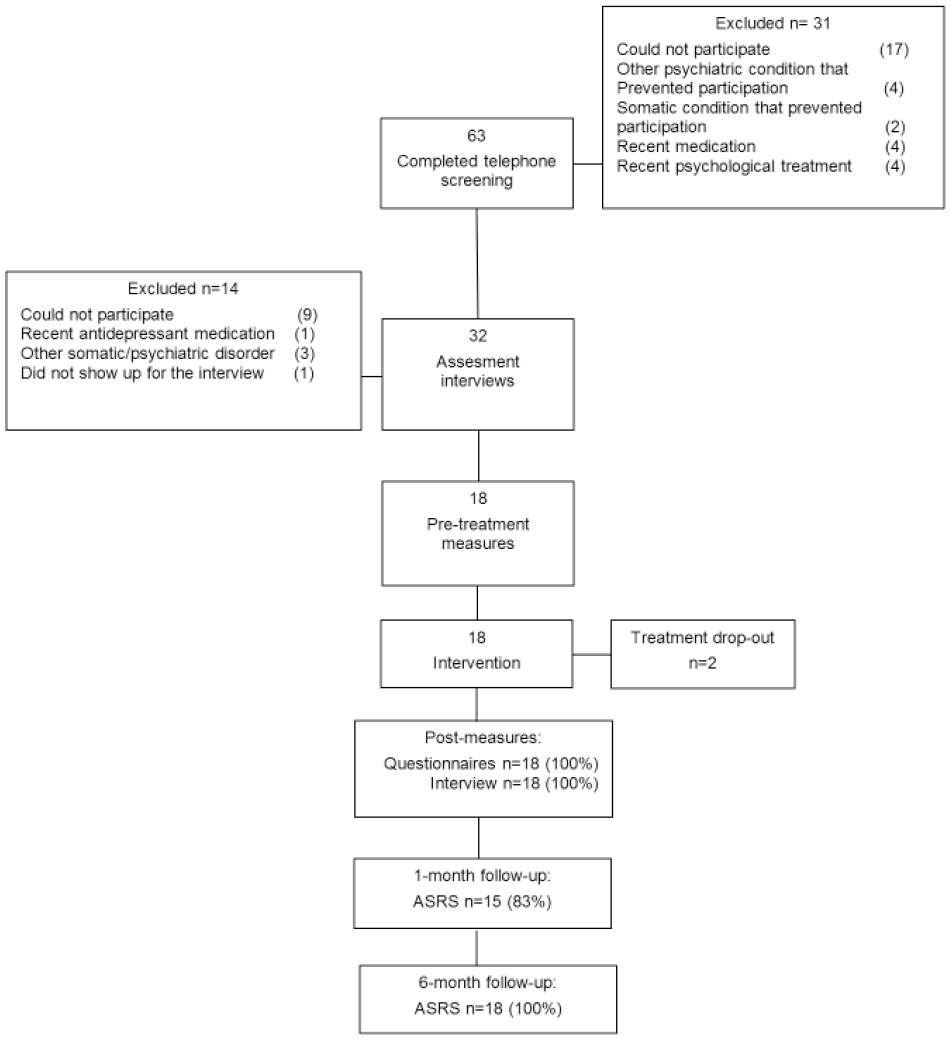
Participant flowchart.
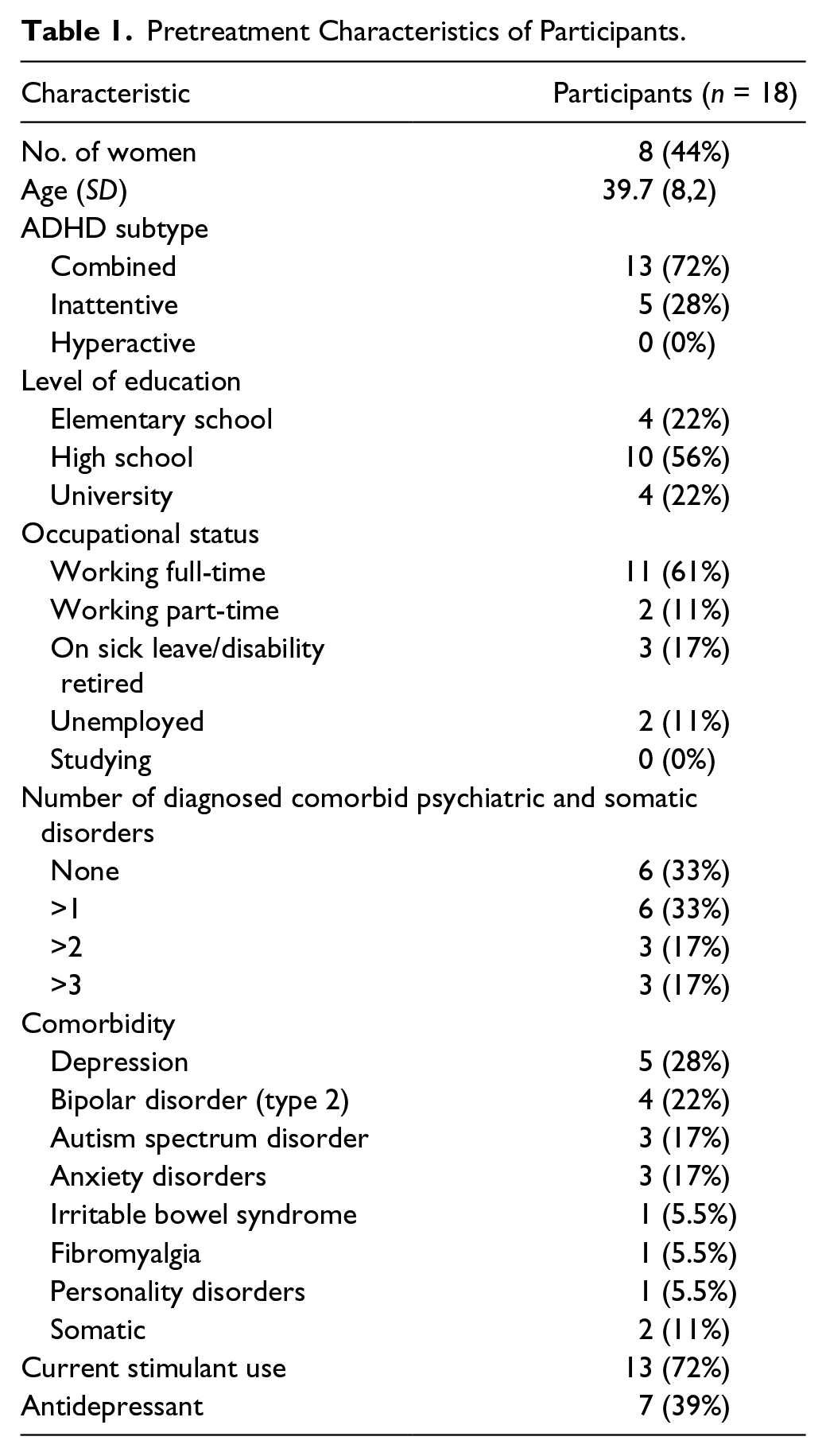
In total, 28% of patients had a comorbid depression and 22% had bipolar II disorder. Moreover, according to the medical records, 17% of the patients also fulfilled criteria for autism spectrum disorder and at least one anxiety disorder. Descriptive data and sample characteristics are presented in Table 1.
Pretreatment Characteristics of Participants.
Measures
Assessments of symptoms were made pre- and posttreatment, and at follow-up 1 and 6 months after end of treatment. Demographic information was obtained mainly from medical records and during the assessment interview. For ASRS, we used at least a 30% reduction in symptoms to classify responders (Hirvikoski et al., 2011; Safren, Sprich, Mimiaga, & et al., 2010; Solanto et al., 2010).
Primary outcome
ASRS-v1.1, a self-rating scale containing the 18 symptom items for ADHD from the DSM-IV, was used as the primary outcome measure. It comprises two subscales, one scale measuring problems with inattention (nine questions), the other measuring problems with hyperactivity and impulsivity (nine questions). The 5-point Likert scale has the options “never” (0), “rarely” (1), “sometimes”(2), “often” (3), or “very often” (4) as response types. The maximum score of ASRS is 72 and 36 points on the two subscales Inattention and Hyperactivity/Impulsivity, respectively. Test–retest reliability of ASRS is 0.88 (Kim, Lee, & Joung, 2013). For each subscale, cutoffs are the following: 0 to 16 means unlikely to have ADHD, 17 to 23 means likely to have ADHD, 24 to 36 means highly likely to have ADHD. ASRS was filled out before and after treatment, as well as at follow-up 1 and 6 months after treatment was completed.
Secondary outcomes
A clinician-rated scale, ADHD Rating Scale IV, containing 18 items based on the DSM-IV criteria for ADHD with the same response options as ASRS was administered before and after treatment for assessment of treatment response. Self-rating questionnaires assessing symptoms of stress and comorbidity were completed by the patients before and after treatment. MADRS-S, containing nine items (scored 0-6) was used as a measure of depressive symptoms with total scores ranging from 0 to 54. The Swedish four-item version of the Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, 1983; Eskin & Parr, 1996) scored 0 to 4 was used to measure the degree to which situations in one’s life are appraised as stressful. Moreover, EuroQol (EQ-5D; Brooks, 1996) was used as a measure of general health status and quality of life. EQ-5D covers five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has three levels: no problems, some problems, extreme problems. To calculate the results from each patient, the scores are combined into an index. Also, a visual-analogue-scale (VAS) records the self-rated health of the respondent with the endpoints “best imaginable health state” (100) and “worst imaginable health state” (0). Sheehan Disability Scale (Sheehan, Harnett-Sheehan, & Raj, 1996) was used to measure functional impairment in three domains; work/school, social, and family life, each scored from 0 (not at all) to 10 (very much). Finally, the 36-item self-report questionnaire Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) scored 0 (almost never) to 5 (always) with a total score of 180 points was used to assess multiple aspects of emotion dysregulation. This questionnaire has been used in several studies, for example, showing improvement in the ability to regulate emotions in patients with borderline personality disorder (Goodman et al., 2014).
Changes in medications and other interventions during treatment period
At posttreatment assessment, patients were asked if they had made changes in any psychotropic medication including ADHD medication, or had been engaged in any other kind of possible therapeutic interventions during the treatment period.
Attendance during sessions and use, comprehension, and benefit of treatment components
Adherence was measured as average attendance rate during the treatment sessions, as well as how many of the scheduled, weekly phone calls the patients responded to.
Another way to measure adherence was through a weekly self-report questionnaire measuring the degree of use, understanding, and perceived utility of the treatment components. This questionnaire was designed specifically for this study. The scale was completed by the patients at the beginning of each group session, where they rated the previous session and homework. Three questions were asked in relation to each treatment component: (a) “How much have you used the specific treatment component?” (b) “How much did this treatment component help you in your everyday life?” and (c) “Was it easy or difficult to understand how the treatment component could be used?”
The response options for questions (a) and (b) were not at all (0), a little (1), to some extent (2), a lot (3), and very much (4). For question (c), the response options were very difficult (0), difficult (1), neither difficult nor easy (2), easy (3), and very easy (4).
A similar measure was designed for the clinicians delivering the treatment. Homework assignments were reviewed both at a phone call 2 to 3 days after each group session and more thoroughly during the next session. Clinicians used the same 0 to 4 scale to rate to what extent the patient had understood, used, and perceived benefit of the components. The same ratings were also made for components from previous sessions if the patient had used them during the week.
To compare the components with regard to use, benefit, and comprehension, the mean of all weekly ratings for each specific component was used. This measure was used to enable comparisons between components regardless of how many weeks they were used. Also, to evaluate the total use (question (a)) of a specific component, all weekly ratings for that component were summed. As the manual stipulated that some of the components were to be used more often during treatment, some components received more weekly ratings than others and thus would receive a higher total just for that reason. Due to this, the total score regarding use was not used to compare components, only to explore relations between the total use of a specific component and outcome.
Furthermore, components which were considered to belong to either Safren’s or Hesslinger’s intervention were merged into blocks labeled Organizing (including to-do list, distraction list, and stimulus control) and DBT (including Problem Solving, Impulse Control, Emotion Regulation, and Communication). All the different mindfulness exercises constituted a block of their own.
Patient satisfaction and evaluation of treatment
Treatment satisfaction and many different aspects of the treatment, such as experience of the group setting, treatment content, and time invested in treatment, were evaluated through a self-rated questionnaire at posttreatment assessment, including both quantitative and qualitative questions. Due to lack of a comparison group and the relatively small number of participants, both types of questions were used as a base for a general, qualitative summary of themes that emerged from the answers. Satisfaction with treatment was also assessed with the established eight-item Client Satisfaction Questionnaire, (CSQ-8; Attkisson & Zwick, 1982). The CSQ-8 consists of eight items that can be scored on a scale from 1 to 4. The total score, therefore, ranges from 8 to 32.
The Intervention
The treatment manual was assembled by the first author (B.N.) and combined, with some adjustments, treatment components from CBT and DBT manuals for adults with ADHD (Hesslinger et al., 2004; Safren, 2005b). Moreover, some other components were added to the manual, such as communication training (to increase presence during conversations), strategies on how to handle obstacles when working with homework assignments, and valued living as inspired by Acceptance and Commitment Therapy (Hayes, Strosah, & Wilson, 2011). The latter was added to the intervention to increase the commitment and motivation of patients to continue working with treatment interventions after treatment was ended.
The components are described in detail in Table 2.
The Content of the Newly Developed Combination Manual.

Mindfulness exercise (defined as attention training during the treatment).
During the 14 weeks of treatment, each weekly 3-hr session started with a short exercise in mindfulness labeled as “attention training,” to enhance ability to focus on the session content. These exercises were provided from Hogrefe (publishing house). Following this short exercise, homework assignments from the previous session were presented by the patients and rated by the observers. After a short break, the theme of the current session was introduced by one of the two group leaders. Sometimes the patients were divided into subgroups to enhance learning, tailor interventions, and make the session more efficient.
At the end of each session, new homework assignments were given to the patients. In general, the same assignments were given to everyone. These were later tailored during the individual call. Patients were encouraged to work with the weekly homework assignments on a daily basis, preferably 30 to 60 min per day. The homework assignments were often carried out during a prescheduled time each day labeled as “planning time,” also used to increase structuring and time-managing skills.
The session content was presented through power point slides, and a white board was often used to highlight the themes of the session. Each patient received a binder during the first session, in which session material was collected at the beginning of each new session. The material provided to the patients consisted of a copy of the homework assignments, a summary of the session content, and individual goals set for the treatment. All patients signed a contract regarding the rules of participation during the first session.
An individual phone call lasting 10 to 20 min was scheduled a few days after the group session. As described before, the purpose of these calls was to support patients in their homework assignments and tailor the components according to the individual needs and capacity of each patient. These calls were placed by group leaders and observers. One day before the session, a text message was sent to the patient’s mobile phone as a reminder to attend the group session next day. Another text message was sent 2 days after the session as a reminder of the importance to work with the homework assignments.
To maintain patients’ attention during the session, 15 minute breaks were scheduled each hour. During the sessions, patients were kept active through active discussions and a flexible way to present materials. We also actively worked on group discussion skills in order to maintain structure during sessions. The skills included exercises such as writing down impulsive thoughts and wait for a few minutes before expressing them, getting prompts through time cards (from the group leaders) as a cue for rounding off a discussion and another non-verbal cue from the therapist to stick to the conversation topic when needed. Through these exercises, key conversation skills were repeated which patients were encouraged to use also outside the session context.
There were two follow-up sessions; one and six months after the end of treatment for the study completers. These sessions focused mainly on problem solving and challenges and difficulties associated with treatment components. Behavior analysis was used as a tool for preventing and handling setbacks in different situations.
Two psychologists led the treatment groups. The first psychologist had extensive training and more than 10 years of experience in CBT and basic knowledge in DBT, with several years of experience in ADHD treatment. The other psychologist had basic training in and one year experience of CBT, with some experience of working with adults with ADHD. The supervisor was both a senior licensed psychologist and psychotherapist specialized in neuropsychology with extensive training and experience in both CBT, DBT and ADHD treatment.
As a support to the group leaders, two students in their final year of their masters in psychology participated in each session as observers to rate the homework assignments of the patients. They also provided feedback to the group leaders regarding the session.
Statistical Analyses
T-tests were used to compare means before and after treatment on all outcome measures, except for ASRS where a repeated-measures analysis of variance (ANOVA) was performed with time (pre-, post-, 1- and 6-month follow-up) as the within subject variable. Bonferroni-corrected post hoc tests for ANOVA’s were used to explore differences between baseline and each of the measurement points after treatment. The same procedure was used to compare differences between components regarding use, comprehension, and benefit. Pearson’s correlation analysis was performed to identify the relationships between measures of adherence and various outcome measures. The significance level specified for all statistical analyses was p < .05. All analyses were performed using SPSS Statistics 22 for Windows.
Results
Primary Outcome
ADHD symptoms improved significantly between pre- and posttreatment, as measured with both the total sum-score of ASRS and its two subscales. Observed improvements were maintained at follow-up, 1 month, and 6 months after the end of treatment (Table 3 and Figure 2). These results were confirmed through post hoc analyses, where pretreatment measures were compared with posttreatment, 1-month, and 6-months follow-up measures respectively. Analysis of responders showed 11 patients (61%) as treatment responders with at least a 30% decrease in ADHD symptomatology.
Means, Standard Deviations of Outcome and Variables at Pre- and Posttreatment, Test Statistics, and Effect Sizes.
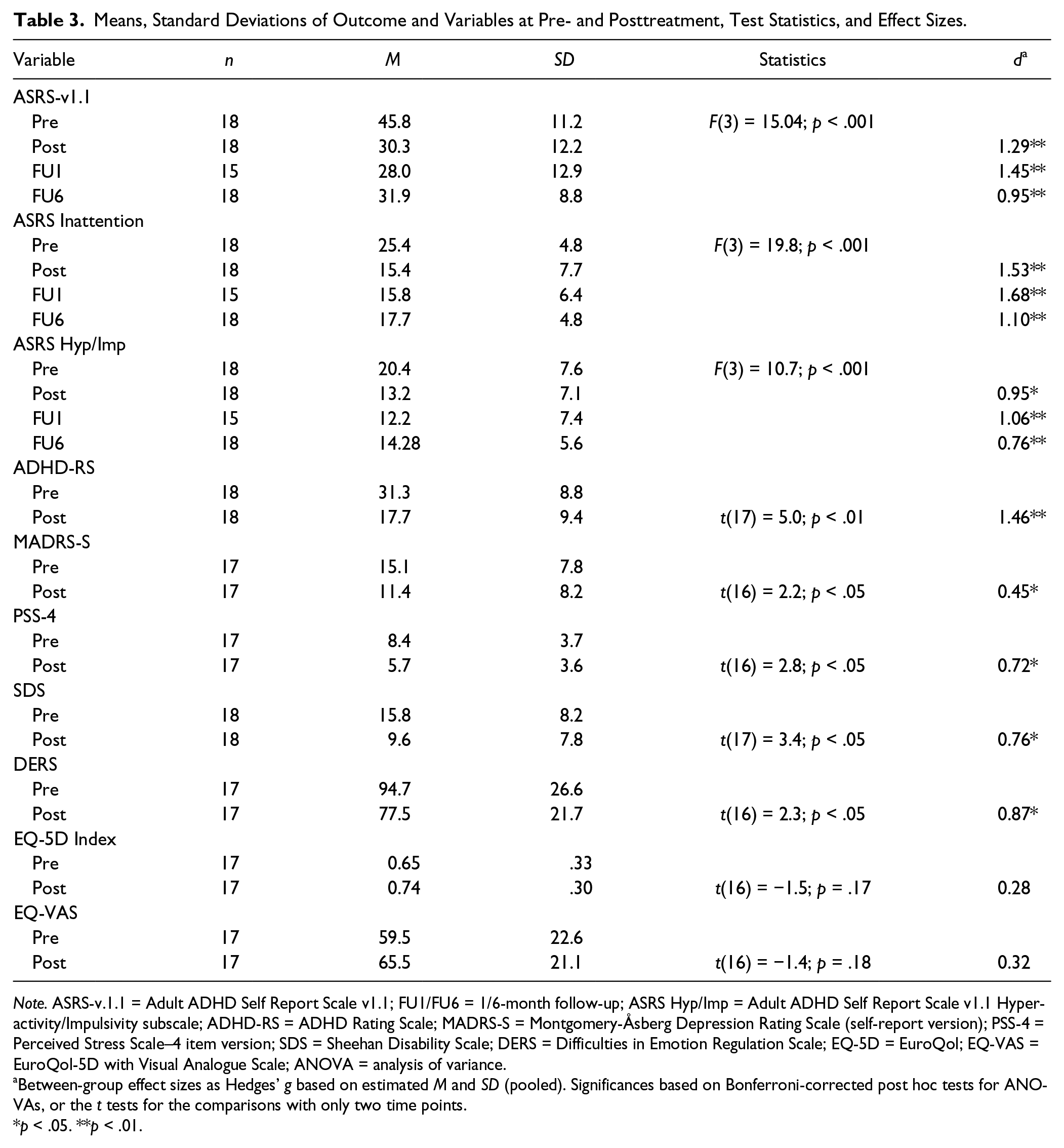
Note. ASRS-v.1.1 = Adult ADHD Self Report Scale v1.1; FU1/FU6 = 1/6-month follow-up; ASRS Hyp/Imp = Adult ADHD Self Report Scale v1.1 Hyperactivity/Impulsivity subscale; ADHD-RS = ADHD Rating Scale; MADRS-S = Montgomery-Åsberg Depression Rating Scale (self-report version); PSS-4 = Perceived Stress Scale–4 item version; SDS = Sheehan Disability Scale; DERS = Difficulties in Emotion Regulation Scale; EQ-5D = EuroQol; EQ-VAS = EuroQol-5D with Visual Analogue Scale; ANOVA = analysis of variance.
Between-group effect sizes as Hedges’ g based on estimated M and SD (pooled). Significances based on Bonferroni-corrected post hoc tests for ANOVAs, or the t tests for the comparisons with only two time points.
p < .05. **p < .01.
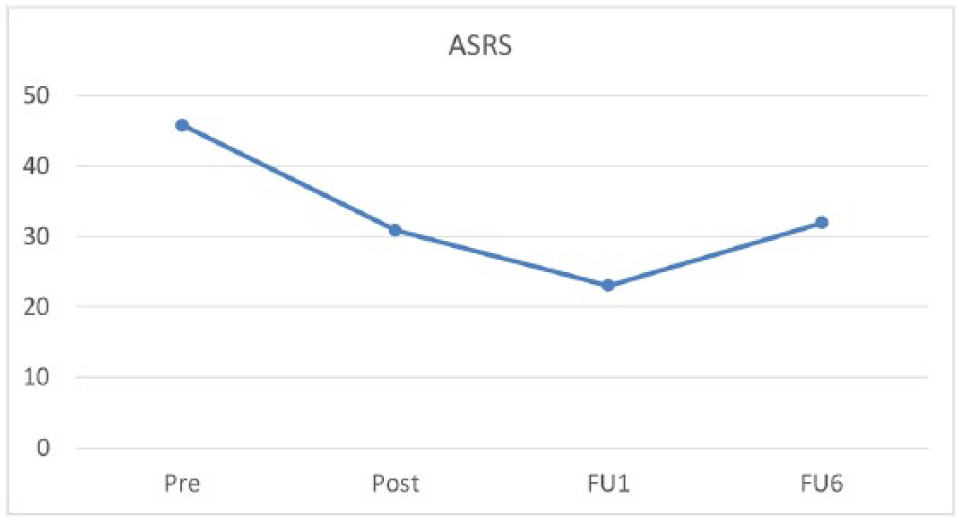
Course of improvement on the primary outcome measure ASRS-v1.1.
A majority of the patients (72%) were taking ADHD medication and in a post-hoc sub-analysis, we explored the differences in ASRS between medicated (n = 13) and non-medicated patients (n = 5). The former went from mean 45.4 (8.6) to 33.6 (9.7) and the latter from 47.2 (17.4) to 26.4 (16.9), but this difference was not significant (t (15) = 0.33; p = .74).
Secondary Outcomes
Significant improvements were observed for all secondary outcome measures (ADHD-RS, MADRS-S, PSS, SDS, and DERS) with the exception of EQ-5D and EQ-VAS, as shown in Table 3.
Changes in Medications and Other Interventions During Treatment Period
None of the patients reported changes in any psychotropic medication including ADHD medication or engagement in any psychological intervention during the treatment period.
Attendance During Treatment and Attrition
For attrition rate at different assessment points, see Figure 1. Dropout from treatment was defined as a patient aborting the intervention after a mutual agreement with the group leader. Two patients (11%) dropped out of treatment after six sessions. Data from both drop-outs were collected post treatment and included in the intent-to-treat analysis.
Sixteen patients were active the whole treatment period and the overall attendance was 85%. Each session was attended by between 56% and 100% of the patients, with the lowest attendance in Session 12. This was mainly due to a snowstorm, which prevented the majority in the first treatment group from attending the session. The overall response rate to the weekly telephone calls was 83%, conversations lasted about 20 min for each patient (M = 19.7 and SD = 5.1).
Use, Comprehension, and Benefit of Treatment Components
When comparing the patients’ weekly ratings with the observers’, we found that the interrater reliability was high and significant for degree of use (r = .90; p < .01), and for perceived benefit (r = .75; p < .01), but not for comprehension (r = .44). Because of the low interrater reliability regarding comprehensiveness, only patient-rated data were used in subsequent analysis and presented in Table 4.
Use, Comprehension, and Perceived Benefit of Treatment Methods as Rated by the Patients During Treatment, and the Correlation of Total Use and Change in Different Outcomes.
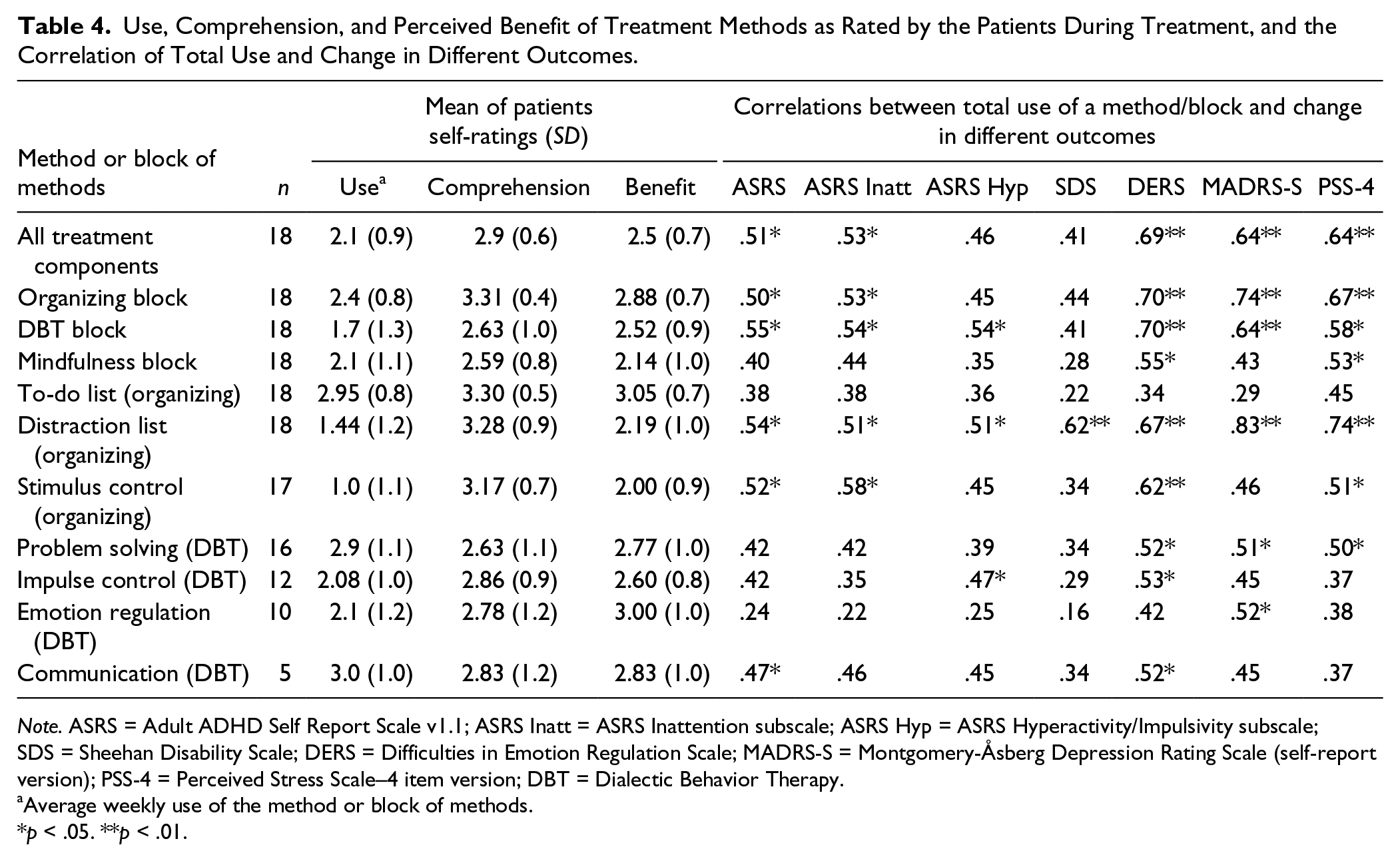
Note. ASRS = Adult ADHD Self Report Scale v1.1; ASRS Inatt = ASRS Inattention subscale; ASRS Hyp = ASRS Hyperactivity/Impulsivity subscale; SDS = Sheehan Disability Scale; DERS = Difficulties in Emotion Regulation Scale; MADRS-S = Montgomery-Åsberg Depression Rating Scale (self-report version); PSS-4 = Perceived Stress Scale–4 item version; DBT = Dialectic Behavior Therapy.
Average weekly use of the method or block of methods.
p < .05. **p < .01.
The use of the three main component blocks differed significantly (F(2) = 7.92; p < .01). The Organizing components (p < .01) and the Mindfulness block (p < .05) were more used than the DBT components. The comprehension also differed significantly (F(2) = 8.2; p < .05), where patients’ understanding of the Organizing block were higher than both Mindfulness (p < .01) and DBT (p < .01). There were also significant differences in perceived benefit (F(2) = 4.58; p < .05), where the Organizing block were rated higher than Mindfulness (p < .01).
Correlations Between Use of Treatment Components and Outcome
The change in ASRS correlated significantly with total use of all treatment components r = 0.51 (p < .05; also seen in Table 4) and with perceived benefit r = 0.50 (p < .05), but not with comprehension r = 0.36 (p = .081).
As shown in Table 4, significant correlations were found between total overall use of components and all outcome measures except for SDS and the hyperactivity/impulsivity subscale of ASRS. The usage of Organizing and DBT components were significantly correlated with reductions in ADHD symptoms, but this was not the case for usage of Mindfulness. Finally, an increased use of treatment components was also related to reductions in therapist-rated ADHD Rating Scale (r = .66; p < .01).
As seen in Table 4, significant correlations were found between total use of all treatment components and all outcome measures used in the analysis except for SDS and the Hyperactivity/Impulsivity subscale of ASRS. In general, the same tendencies were found for total use of organizing components and DBT components, whereas total use of mindfulness components did not influence outcome except for the relationship with DERS and PSS.
Degree of use of organizing tools such as distraction list and stimulus control correlated significantly with reduced symptoms of inattention (measured with the Inattention subscale of ASRS). Furthermore, use of the to-do list did not seem to improve inattention. Interestingly, the Impulsivity/Hyperactivity subscale of ASRS seemed to be the only outcome measure (except for DERS) that was positively influenced by degree of use of the impulse control tools in the DBT block. Moreover, DERS was the only outcome measure which was significantly affected by usage of almost all of the components. The opposite results were true for PSS and particularly SDS, where few correlations were found between these measures and degree of use of different components.
Patient Satisfaction and Evaluation of Treatment
Patients who completed the CSQ-8 after treatment (n = 18) scored an average of 29.33 (SD = 4.28) out of a possible 32. This result shows an “excellent” level of satisfaction (Smith et al., 2014) with the treatment intervention.
A qualitative review of the additional questions regarding the patients’ retrospective evaluation of the treatment revealed that almost all patients were very satisfied with the treatment content and scope, as well as with the group format. The general experience was that their attitude toward their diagnosis had improved. Although the treatment program was stated as challenging by almost all of the patients, they all agreed that it was worth the challenge.
Furthermore, homework assignments were rated as very relevant and useful. In general, patients stated that they had used the new treatment components actively 2 to 3 times per week.
The individual weekly phone calls were highly important for almost all of the patients because of their motivating and problem-solving aspects. Some of the patients reported that they could have benefited from additional treatment time, and some commented that the homework sheets could be improved and simplified. None of the modules were assessed as unhelpful. In general, the behavior analysis, the organizing, and the valued living sessions were rated as very valuable by the majority of the patients. On the other hand, mindfulness was rated as challenging and sometimes difficult to understand by some patients. Furthermore, some individuals commented that they had difficulties understanding and processing the session content due to cognitive impairments.
One specific event which occurred during the valued living session was rated by several patients as a negative experience in the retrospective evaluation questionnaire. A mindfulness exercise named “Meeting myself as a 90-year-old” was performed with the first group to increase the patients’ motivation to work with the life compass. This exercise was experienced as very emotionally challenging for three patients who received special attention from the group leader after the session ended. The therapists also addressed the event in the routine phone call. In general, the exercise contributed to a stressful session environment for the whole group. As a consequence, it was substituted with another mindfulness exercise in the second group.
Discussion
The present study demonstrated the feasibility and preliminary effects of a new combination of CBT and DBT components for adults with ADHD. We observed a significant reduction of ADHD symptoms, maintained at follow-up, 1 month, and 6 months after the end of treatment, with large effects on inattention, hyperactivity, and impulsivity. The largest effects were found on the inattention subscale of ASRS, indicating an increase in executive functioning (or skills to better compensate for low executive functioning), working memory and attention. Compared to previous studies of psychotherapy for adults with ADHD, where treatment response rate ranged from 32-67% (Hirvikoski et al., 2011; Safren, Sprich, Mimiaga, & et al., 2010; Solanto et al., 2010), the proportion of responders was high, especially considering the broad inclusion criteria in the current study. Symptoms of depression and perceived psychological stress also decreased as well as everyday disability and difficulties in emotion regulation.
A majority of the patients (72%) were concurrently using ADHD medication throughout the treatment. None of them reported changes in medication during the period from one month prior treatment and till the end of treatment. This indicates that positive effects of psychological treatment can be obtained also among patients with current medication, something that is supported by the non-significant post-hoc test comparing outcome for patients on medications with those without medications.
The weekly patient ratings of degree of usage, comprehension, and benefit of treatment components were generally high. On average, each session was attended by 85% of the patients, a high rate considering that motivational deficits are common in adults with ADHD (Volkow et al., 2011). In addition, overall attendance to group sessions and phone calls was very high. A high degree of satisfaction with the treatment was reported in the structured self-report as well as the qualitative evaluation of the intervention. In total, this indicates that the tested treatment was feasible and accepted by the patients.
The relevance of the treatment components was also supported by the association between use of components and changes in symptoms of ADHD, depression, and stress, as well as emotion regulation.
Symptom reduction was seen on a range of measures, but no effect was found on self-measured general health status and quality of life as measured with EQ-5D. This is in line with previous findings (Payakachat, Ali, & Tilford, 2015). EQ-5D detects perceived symptoms of depression and anxiety as well as reduced function in daily activities.
The studied participants were partly stabilized with counseling and pharmacotherapy which possibly explains the lack of sensitivity of EQ-5D. However, we observed significant reductions in a closely related estimate, Sheehan Disability Scale, which measures everyday functionality in a more direct way.
Individuals with ADHD are characterized by general novelty seeking and deficits in attention and working memory. A major challenge during development and implementation of this treatment was to create a balance between repetition and introduction of new treatment components. Our solution was to provide the patients opportunity to rehearse the main components through in-depth training in the subsequent session.
The high attendance rate indicates that our approach was successful and may also have been a consequence of the weekly telephone calls. Most patients emphasized the importance of these calls, an impression they shared with the therapists. This is considered to be one of the main findings in this study. Through individual follow-ups, the content of treatment and homework assignments could be explained, modified, and tailored to meet the needs of each individual. The treatment outcome would probably have been different without these individual follow-ups. In future studies, we suggest that treatment with and without weekly calls be examined to investigate the possible additional effects of the individual follow-ups.
Additional strengths of this study were that all patients who were screened and finally considered as eligible for study inclusion were recruited through mental health professionals from units specialized in diagnostic assessment of ADHD. The inclusion criteria were broad, with a blend of medicated and non-medicated individuals where we also included two high functioning individuals with autism spectrum disorder. However it is not possible to give any clinical recommendations on how the evaluated treatment worked for these individuals based on limited data. Furthermore, as the patients were stable on medication before and after treatment, the treatment effects are most probably not explained by medication effects alone.
Other objectives were to examine if the level of use, understanding, and perceived benefit of treatment components were related to treatment outcome, to preliminary explore their clinical usefulness and also to evaluate if these factors differed when comparing the components of Safren’s and Hesslinger’s manuals (Hesslinger et al., 2004; Safren, 2005b). Overall, adherence was considered as to be high due to the high percentage of patients that attended and responded to the weekly calls, and also due to the overall high ratings of use, comprehension, and perceived benefit of the treatment components.
Our findings show that organizing components were generally more used than DBT components. They were generally also considered as easier to understand than the DBT and mindfulness components by the patients and also perceived as more beneficial than the mindfulness components. There may be several explanations for these findings. One explanation could be that the organizing components were introduced early in the treatment. Consequently, patients continued to practice these methods during the entire treatment period. In the comparison analysis, the average scores of use controlled for these effects, yet there is a possibility that, for example, practice effects could have influenced our results. Furthermore, the organizing components could have been considered as more emotionally neutral and therefore easier to work with, as well as more concrete and easy to grasp compared with other components. Furthermore, the time allowed to learn and use the DBT components might have been too short. This could indicate that combining CBT and DBT components within a limited treatment period might decrease engagement and effects for one of them. However, our effect sizes are comparable with similar studies on CBT (Safren, 2005) and DBT interventions for adults with ADHD (Hirvikoski et al., 2011), indicating that a combination manual can be effective in reducing core symptoms. In future revisions of the manual, simplification and reduction of the DBT components, and possibly also the CBT parts should be considered. Another strategy could be to individualize the treatment, e.g. by spending more time on DBT for patients with emotional dysregulation. Overall, a preliminary impression is that further simplification of session content and homework assignments would be advantageous, so that individuals with more severe attentional and executive impairments could benefit from this treatment. Moreover, an extended analysis on treatment components should be conducted in a larger trial, further exploring the effectivity and usefulness of each component in order to refine the treatment..
In general, degree of use was related to positive outcome. However, use of mindfulness was not related to reduction in ADHD symptoms. This is a rather surprising finding given that mindfulness training has been recognized as a way to regulate attention (Bishop et al., 2004; Brown & Ryan, 2003) and appears to improve self-regulation of attention and emotion (Teasdale, Segal, & Williams, 1995) as well as impulsivity in patients with borderline personality disorder (Bohus et al., 2004).
One possible explanation could be that the mindfulness exercises in this study, unlike the referred studies, were provided only as a limited part of the treatment in combination with other “key” components which got more attention. If this finding is confirmed in future studies, it could indicate that mindfulness interventions provide greater value if given more attention in an intervention, rather just being a limited part of treatment.
Moreover, we found a relationship between amount of treatment use and reduced symptoms of stress as well as problems with emotion regulation. This finding is supported by previous studies (Arch & Craske, 2006; Baer, 2003) but should be interpreted cautiously due to methodological limitations of the present study. Another interesting finding in the correlational analyses was that use of almost all of the treatment components correlated significantly with increased ability to regulate emotions. Furthermore, in comparison with other secondary outcome measures, DERS had the largest effect size. There is emerging evidence for emotion dysregulation as a key area of impairment for many patients with ADHD (Barkley, 2010; Martel, 2009). Hence, our findings could indicate that use of a majority of the components in the treatment also influenced another core symptom in addition to those measured by the primary outcome.
Limitations
Being a pilot study with a small sample size and lack of a control group, the study findings have limited robustness and generalizability.
The scale used to measure use, understanding, and benefit of each component was specifically designed for this study and has not been validated elsewhere. Patient ratings of use and benefit were highly correlated to therapist ratings of the same constructs, which indicates that they are valid. However, patient ratings of understanding could not be verified by high correlations with observer ratings, and must therefore be interpreted more cautiously. It should also be noted that comparison between components, in regard to use, benefit, and comprehension, is biased by the fact that the manual prescribed that some components be used more often than others during the course of treatment. Even though average ratings for these comparisons were used, learning effects or effects due to repeated measures could have influenced the results.
Furthermore, the time allowed to learn and use the DBT components might have been too short. This could indicate that combining CBT and DBT components within a limited treatment period might decrease engagement and effects for one of them. However, our effect sizes are comparable with similar studies on CBT (Safren, 2005) and DBT interventions for adults with ADHD (Hirvikoski et al., 2011), indicating that a combination manual can be effective in reducing core symptoms. In future revisions of the manual, simplification and reduction of the DBT components, and possibly also the CBT parts should be considered. Another strategy could be to individualize the treatment, e.g. by spending more time on DBT for patients with emotional dysregulation. Overall, a preliminary impression is that further simplification of session content and homework assignments would be advantageous, so that individuals with more severe attentional and executive impairments could benefit from this treatment. Moreover, an extended analysis on treatment components should be conducted in a larger trial, further exploring the effectivity and usefulness of each component in order to refine the treatment.
Furthermore, using patient rated ASRS instead of blind observer ratings as the primary outcome could have influenced the results due to potential expectancy effects. The clinician ratings with the ADHD Rating Scale showed an even larger treatment effect, but these were not blind and could have been influenced by the clinician’s expectancies.
Finally, it should be underscored that the relationships between use of treatment components and outcome are only correlational, and causality could therefore not be inferred from this data.
Future Research and Clinical Applications
Our findings regarding this novel treatment are encouraging. However, they need to be considered as preliminary in lack of controlled studies. If results are confirmed in the future, ADHD patients could be offered this treatment, containing a combination of effective components from state-of-the-art CBT and DBT, as part of recommended multimodal treatment. Consequently, clinicians would not have to choose between these approaches, but could offer patients a treatment providing them with effective tools for managing many of the everyday challenges of having ADHD.
Conclusions
In summary, the reduction in ADHD symptoms following treatment was maintained over 6 months. The positive effect on measures of depression, perceived stress, emotion regulation, and everyday disability, as well as the high attendance and high treatment satisfaction, imply that this combined treatment manual is feasible and promising. Use, comprehension, and perceived benefit of treatment components varied from medium to high, and a higher degree of use was very often related to more positive outcomes. Future studies with larger samples and a randomized controlled design are needed to verify these findings.
Footnotes
Acknowledgements
We would like to express our deepest gratitude to all the patients in the pilot group who contributed generously to the sessions through their enthusiastic, constructive and creative feedback.
We also would like to thank Niels Eék for his invaluable contribution as co-therapist and Tatja Hirvikoski for her professional supervision and advice during the treatment.
A special thanks also to Kristina Harsanyi and Ljiljana Milivojevic for invaluable help in the screening of medical records and administration of the screening survey, to Seija Sirviö for her wise advice during development of the manual and to Charlotte Ulfsparre for her significant linguistic contribution. Last, but not least, we want to express our gratitude to Hogrefe who kindly and generously provided us access to mindfulness exercises through their website.
Authors’ Note
VK designed the study, contributed to critical editing of text and figures, approved the final version of the manuscript and supervised BN. BN participated in the design of the study, wrote the treatment manual, performed the statistical analysis and analyzed data (together with VK), supervised students MC and PF, and had the main responsibility for writing the manuscript, including writing the first draft. Together with MC and PF, BN also collected data, conducted the treatment (as the senior therapist) and the pre- and post-measurements. YG and NL contributed to the design of the study. All authors read and commented on the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted as part of the clinical work at Neuropsychiatric Unit, Psychiatry Southwest, Stockholm County Council. The project was funded by Stockholm County Council and the Bror Gadelius memory foundation, the Söderström-Königska Sjukhemmet foundation, and the Boethius foundation. The funding sources were not involved in the work of the authors.