
Abstract
Introduction
ADHD is a neurodevelopmental disorder marked by significant inattention, hyperactivity, and impulsivity (Diagnostic and Statistical Manual of Mental Disorders [5th ed.; DSM-5]; American Psychiatric Association [APA], 2013). There is growing evidence that ADHD has important developmental aspects and its symptoms change considerably over time (Berger, Slobodin, Aboud, Melamed, & Cassuto, 2013; Faraone, Biederman, & Mick, 2006). Leading researchers (Barkley, 1997; Gillberg, 2010; Sonuga-Barke, & Halperin, 2010) have long argued that ADHD is a developmental disorder with early onset and that deficits in inhibition appear in early childhood leading to a cascade of other problems in self-regulation, encompassed under the rubric of executive functioning (Berger et al., 2013). It is commonly argued that ADHD symptoms are associated with maturational delay that gradually changes during adolescence (Faraone et al., 2006). This tenet is supported by a long line of neuropsychological (Kalff et al., 2003), neuroanatomical (Krain & Castellanos, 2006; Smith, Taylor, Brammer, Toone, & Rubia, 2006), and electrophysiological (Yordanova, Kolev, & Rothenberger, 2009) studies that showed a developmental delay in attention functions in ADHD children. Using computational neuroanatomical techniques, Shaw and his colleagues (Shaw et al., 2007, Shaw et al., 2012) found a corresponding delay in the development for both cortical thickness and surface area in ADHD children that probably represents a global perturbation in the mechanisms that guide cortical maturation. In both groups (ADHD and typically developing children), the maturation of cortical surface area progressed in centripetal waves, both lateral (starting at the central sulcus and fronto-polar regions, sweeping toward the mid- and superior frontal gyrus) and medial (descending down the medial prefrontal cortex, toward the cingulate gyrus). However, the surface area developmental trajectory was delayed in ADHD. For the right prefrontal cortex, the median age by which 50% of cortical vertices attained peak area was 14.6 years in ADHD, significantly later than in typically developing group at 12.7 years. Similar delay was found in the left hemispheric lobes. There were no such diagnostic differences in the developmental trajectories of cortical gyrification. These studies suggested that children with ADHD follow a similar sequential pattern of cortical development as their typically developing peers, yet were delayed by as much as 2 to 3 years, depending on the specific cortical region. However, the fact that two thirds of childhood cases of ADHD persist into adolescence and adulthood (Biederman et al., 2006; Rowland, Lesesne, & Abramowitz, 2002) raised the question whether ADHD may represent a deviant developmental trajectory rather than a developmental delay. Indeed, a growing body of evidence from brain imaging studies (Castellanos et al., 2000; Zhu et al., 2008) indicated that ADHD characteristics shared little in common with the pattern of brain activity seen in younger control children. Currently, there is no consensus concerning the relation between ADHD symptoms and the concepts of biological and psychological maturity (Gustafsson, Holmström, Besjakov, & Karlsson, 2010).
Importantly, continuity and discontinuity in a neurodevelopmental disorder are strongly associated with the particular ways in which the malfunction is shown and diagnosed across ages. Longitudinal clinical studies indicated that ADHD subcategories systematically change with increasing age (Biederman, Mick, & Faraone, 2000; Fischer, Barkley, Smallish, & Fletcher, 2005). As seen in these studies, the symptoms of inattention tend to persist from childhood into adolescence to a greater extent than symptoms of hyperactivity-impulsivity (Larsson, Dilshad, Lichtenstein, & Barker, 2011). Because there is a general decline in hyperactivity-impulsivity symptoms across the development, it means that ADHD subcategories cannot be viewed as discrete and stable categories, and an individual variation in the development course must be considered (Biederman et al., 2000; van Lier, van der Ende, Koot, & Verhulst, 2007). ADHD also becomes more heterogeneous and subtle in adults. Prevalence and natural history data suggest that of all the children diagnosed with ADHD, only some (one to two thirds) continue to manifest appreciable ADHD symptoms into adult life (Wender, Wolf, & Wasserstein, 2001). This reported drop in the prevalence of ADHD with age may reflect reporter differences, because the investigators depended solely on self-report for the adult cohorts, whereas for child cohorts, both the participants and parents were used as informants (DeQuiros & Kinsbourne, 2001; Wender et al., 2001).
Because both prospective and retrospective studies largely rely on diagnostic categories using similar criteria across the age span, it is impossible to draw any unequivocal conclusion on the ways in which ADHD symptoms vary with age (Rutter, 2013). Thus, objective and reliable markers of ADHD across life span could provide a valuable addition to the assessment of age-related changes in ADHD.
The Continuous Performance Test (CPT), which was originally developed as a measure of vigilance and detection of deficits in sustained attention (Cornblatt, Risch, Faris, Friedman, & Erlenmeyer-Kimling, 1988; Rutschmann, Cornblatt, & Erlenmeyer-Kimling, 1977), has been widely used and is reported to be the most popular clinic-based measure of sustained attention and vigilance (Edwards et al., 2007). Recent study described CPT measurements and abilities of sustained attention and omission errors among ADHD children compared with non-ADHD children (Cassuto, Ben-Simon, & Berger, 2013). In a previous study that used a CPT to measure age-related changes in attention performance of ADHD and non-ADHD children (ages 6-11 years), it was found that despite improvement across childhood, ADHD children continued to demonstrate impaired cognitive functioning as compared with non-ADHD children (Berger et al., 2013). Detailed results suggested that sustained attention, characterized as the ability to concentrate on a specific stimulus over a period of time, develops slower but normally. Meanwhile, other functions, such as inhibitory control, an important component of executive function that allows for the suppression of actions and resistance to interference from irrelevant stimuli (Sonuga-Barke, Brandeis, Holtmann, & Cortese, 2014), do not show a clear developmental trajectory (Berger et al., 2013). These conclusions were based on a limited age range; therefore, they did not allow observation on developmental changes during adolescence.
Thus, the aim of the current study was to elaborate previous findings about age-related changes in CPT performance by including a wider spectrum of age.
This study focused on the impact of development on the ability to sustain attention in the presence of environmental visual and auditory distractors. To preserve an effective CPT performance in the presence of distractors, people are required to attend target stimuli while inhibiting non-goal-related information. These inhibitory control mechanisms are associated with developmental changes in frontal structures, including the anterior cingulate cortex, the inferior frontal gyrus, and the dorsal lateral prefrontal cortex (Curtis, Cole, Rao, & D’Esposito, 2005). Pediatric populations with inhibitory impairment such as ADHD are usually characterized by reduced frontal cortical thickness (Batty et al., 2010). However, behavioral research on age-related changes in distractibility among children with ADHD is still scarce.
Given the clear impact of development on general inhibition control and on distractibility (Luna, Garver, Urban, Lazar, & Sweeney, 2004), the current study was guided by two hypotheses:
Method
Participants
Participants were 839 children aged 7 to 18 years, of which 526 were boys and 313 were girls. The clinical group included 478 children and adolescents previously diagnosed with ADHD. The control group included 361 children and adolescents without ADHD. Data were analyzed separately for children (age 7-12 years) and for adolescents (age 13-18 years). These age groups correspond to the school age and teen life periods, respectively, and are commonly used in mental health and neuroscience research.
Demographic data are presented in Table 1. In children aged 7 to 12 years, no age difference was found between the ADHD and the control groups. The rate of boys was significantly higher in the ADHD group than in the control group. However, gender did not have a significant effect on the rate of omission errors, F(1, 659) = 1.05, p = .31. In adolescents aged 13 to 18 years, no differences were found in age or gender distributions of ADHD and controls.
Demographic Variables of Participants.

p < .05. **p < .01. ***p < .001.
Participants in the ADHD group were recruited from children who were referred to out-patient pediatric clinics of a neuro-cognitive center, based in a tertiary care university hospital. The referrals to the center were made by pediatricians, general practitioners, teachers, psychologists, or parents. All participants in the ADHD group met the criteria for ADHD according to Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) criteria, as assessed by a certified pediatric neurologist. The diagnostic procedure included an interview with the patient and parents, medical or neurological examination, and filling of ADHD diagnostic questionnaires (DuPaul, Power, Anastopouls, & Reid, 1998). Participants in the control group were randomly recruited from regular primary and high school classes. The inclusion criteria for participants in the control group were (a) score below the clinical cutoff point for ADHD symptoms on ADHD DSM-IV scales (APA, 2000; DuPaul et al., 1998) and (b) absence of academic or behavioral problems based on parent and teacher reports.
The exclusion criteria for all participants were intellectual disability, other chronic condition, chronic use of medications, and primary psychiatric diagnosis (e.g., depression, anxiety, and psychosis). All participants in this study studied in regular classes in regular schools.
All participants agreed to participate in the study, and their parents provided a written informed consent to the study, approved by the Helsinki Committee (Institutional Review Board [IRB]) of Hadassah-Hebrew University Medical Center Jerusalem, Israel.
Tools
The MOXO-CPT
The current study used the MOXO-CPT version (Berger & Goldzweig, 2010). The term MOXO derives from the world of Japanese martial arts and means a “moment of lucidity.” The MOXO-CPT (Neuro-Tech Solutions Ltd.) is a standardized computerized test designed to diagnose ADHD-related symptoms. As in other CPT, the MOXO-CPT task not only requires a participant to sustain attention over a continuous stream of stimuli and to respond to a prespecified target, but it also includes visual and auditory stimuli serving as measurable distractors. Due to the large age spectrum, this study used two different versions of the test, one for children (Cassuto et al., 2013) and one for adolescents (Berger & Cassuto, 2014).
Children’s test
The test consists of eight stages (levels). Each level consists of 53 trials and lasts 114.15 s. The total duration of the test is 15.2 min. In each trial, a stimulus (target or non-target) is presented in the middle of the computer screen for a duration of 0.5, 1, or 3 s and is followed by a “void” of the same duration (Figure 1). Fifty-three stimuli are presented in each level, of which 33 are target stimuli and 20 are non-target. Each stimulus remains on the screen for the full duration of the designated presentation time, regardless of whether a response was given or not. This practice allows the measuring of the timing of the response as well as its accuracy.

Definition of the time line.
The screen size is 125 high and 166 wide. The child is located 60 cm from the screen and is instructed to respond to target stimulus as quickly as possible by pressing the space bar once and only once. The child is also instructed not to respond to any other stimuli but the target, and not to press any other key but the space bar.
Test stimuli
Both target and non-target stimuli are cartoon pictures free of letters or numbers. The absence of letters and numbers in the stimuli is important given the fact that ADHD children tend to have learning difficulties (e.g., dyslexia, dyscalculia) that may be confound with CPT performance (Seidman, Biederman, Monuteaux, Doyle, & Faraone, 2001). Target stimulus is always a cartoon image of a child’s face. Non-target stimuli include five different images of animals. Both target and non-target stimuli are 41 × 41 mm large and are always presented in the center of the screen.
Distracting stimuli
To simulate everyday environment, the MOXO-CPT includes visual and auditory distracting stimuli, which are not part of the non-target stimuli. The distracting stimuli are of various degrees of similarity to the target stimulus. Distractors are short animated video clips containing visual and auditory features, which can appear separately or together. All distractors are typical elements in the child environment, a unique feature to the MOXO-CPT. Overall, six different distractors are included, each of them could appear as pure visual (e.g., three birds moving their wings), pure auditory (e.g., birds singing), or as a combination of them (birds moving their wings and singing simultaneously). Each distractor was presented for a different duration ranging from 3.5 to 14.8 s, with a fixed interval of 0.5 s between two distractors. Visual distractors include six different stimuli: a gong (presented for 6.8 s), a bowling ball (3.5 s), birds (9.25 s), warrior (Jedi) with saber (14.8 s), saber (6.8 s), and a flying airplane (8.6 s).
Visual distractors appear at one of four spatial locations on the sides of the screen: down, up, left, or right. Visual distractors that appear on the left or right axis are 200 to 400 pixels high and 100 to 200 pixels wide. Visual distractors that appear on the up or down axis are 100 to 200 pixels high and 100 to 600 wide. The distance between visual distractors and target or non-target stimuli is always 21 mm.
Auditory distractors include the six corresponding sounds of all visual distractors (e.g., a gong sound, sound of a bowling ball, birds singing, etc.). The sound is delivered through loudspeakers located on both sides of the screen (about 60 cm distance from the child’s ears). The sound intensity is about 70% of the maximal intensity of the loudspeakers. Distractors’ onset is not synchronized with target or non-target’s onset and could be generated during target or non-target stimulus or during the void period.
Test levels
The test consists of 8 levels, with 53 trials in each level. The stimuli and their presentation time are identical across all levels; however, the levels differ in the visual and auditory distractors present in the trials. Different levels of the MOXO-CPT are characterized by a different set of distractors: Levels 1 and 8 did not include any distractors but only target and non-target stimuli, Levels 2 and 3 contained pure visual stimuli, Levels 4 and 5 contained pure auditory stimuli, and Levels 6 and 7 contained a combination of visual and auditory stimuli. The sequence of distractors and their exact position on the display are constant for each level. The load of the distracting stimuli increases in the odd number levels: During the second, fourth, and sixth levels, only one distractor is presented at a time. During the third, fifth, and seventh levels, two distractors are presented simultaneously.
Adolescents’ test
The MOXO-CPT version for adolescents and adults differs from the children version in several aspects. First, each one of the eight levels consists of 59 trials (34 targets and 25 non-targets) and lasts 136.5 s, so that the total duration of the test is longer (18.2 min). Second, in each trial, the stimulus (target or non-target) is presented for 0.5, 1, or 4 s, followed by a “void” period of the same duration. Third, eight different distractors, and not six, are used. Distractor types are borrowed from everyday life of adults and adolescents (e.g., crying baby, people arguing, car driving). Fourth, all distractors were presented for 8 s, with a fixed interval of 0.5 s between two distractors. Overall, eight different distractors were included, each of them appearing as pure visual, pure auditory, or as a combination of them. Visual distractors include burning cigarette, arguing people, crying baby, barking dog, police car, car breaks, pouring wine, and a bag full of coins. All other aspects are identical to the children version.
Performance indices—the MOXO-CPT includes four performance indices:
Attention: The number of correct responses (pressing the key in response to a target stimulus) that are given either during the stimulus presentation on the screen or during the following void period. The difference between the total number of the target stimuli and the number of correct responses produces the number of omission errors.
Timing: The number of correct responses that are given while the target stimulus is still presented on the screen.
Impulsivity:The number of commission errors performed only during the time in which a non-target stimulus is present on the screen.
Hyperactivity: The number of all types of commission responses that are not coded as impulsive responses (e.g., multiple responses, random key pressing). For more detailed description of performance indices, see Online Supplementary 1.
Although data for all indices were collected, this study focused on the rate of omission errors—the number of times the participant did not respond to target stimuli either during the stimulus presentation or during the void time. The rate of omission errors is regarded as a measurement of difficulty in sustained attention, which is not dependent on response speed.
Procedure
In the current study, the test was administered by a technician who made sure that the participant understood the instructions. The technician was present throughout the entire session. All participants (including the ADHD group) were drug naive (not medicated at all) before and during their participation in the study.
Data Analyses
All analyses were conducted with SAS software for Windows Version 9.2. Data were analyzed separately for children (age 7-12 years) and adolescents (age 13-18 years). First, chi-square analyses and t tests for unpaired samples were used to examine group differences in background variables. Second, effects of background variables, ADHD, and test level on omission errors were examined through a linear repeated-measures model with Tukey’s post hoc comparisons. Omission errors were the dependent variable, whereas age, gender, group, and test’s level were the independent variables. In addition, Level × Group interaction was calculated.
Results
To examine study hypotheses, a linear repeated-measures model with Tukey’s correction for multiple comparisons was conducted. Results for children aged 7 to 12 years showed that although gender was not associated with CPT performance, age had a significant effect on it, F(1, 659) = 97.59, p < .001. When controlling for age and gender, group affiliation had a significant effect on the rate of omission errors, F(1, 659) = 92.59, p < .001.
As can be seen in Table 2, ADHD children demonstrated significantly higher rate of errors than non-ADHD children in all CPT conditions (no distractors, visual distractors, auditory distractors, and a combination of visual and auditory distractors). Most importantly, Group × Level interaction revealed that the differences between the two groups varied as a function of the task demands, F(3, 659) = 15.55, p < .001. Results for adolescents aged 13 to 18 years revealed that both gender, F(1, 172) = 5.26, p < .05, and age, F(1, 172) = 9.10, p < .01, were associated with CPT performance. When controlling for age and gender, group affiliation had a significant effect on the rate of omission errors, F(1, 172) = 28.45, p < .001. As presented in Table 2, ADHD adolescents demonstrated higher rate of omission errors than their unaffected peers in all CPT conditions (no distractors, visual distractors, auditory distractors, and a combination of visual and auditory distractors). Group × Level interaction showed that the difference between the two groups varied as a function of task demands, F(3, 172) = 4.98, p < .01.
Differences in Omission Rates Between ADHD and Non-ADHD Children and Adolescents.
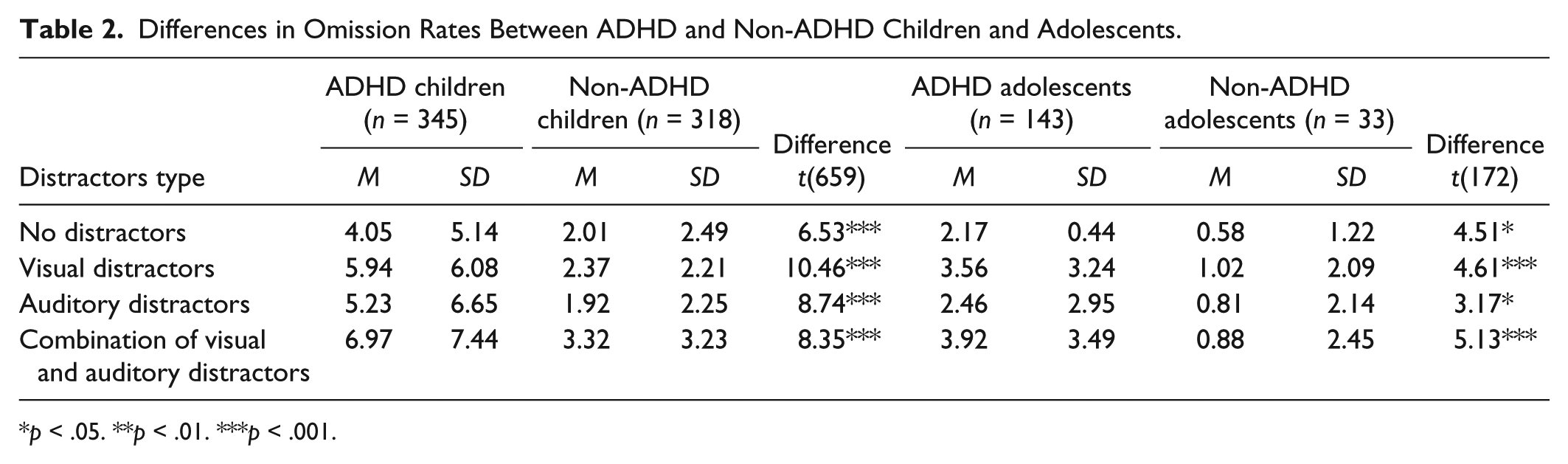
p < .05. **p < .01. ***p < .001.
Tables 3 and 4 present within-groups analyses of the differences in omission rates between baseline level (no distractors) and distractors conditions for ADHD and non-ADHD children and adolescents, respectively. As seen in Table 3, ADHD children demonstrated higher rate of omission errors in all distractors conditions and all levels of distractibility (low and high) compared with baseline. In the presence of visual or combined distractors, children with ADHD performed significantly more omission errors in low-distractibility condition (one distracting stimuli presented at a time) than in high-distractibility condition (two distractors presented simultaneously). The opposite pattern was found for auditory distractors.
Differences in Omission Rates Between Baseline Level and Distractors Conditions for ADHD and Non-ADHD Children Aged 7 to 12 Years.
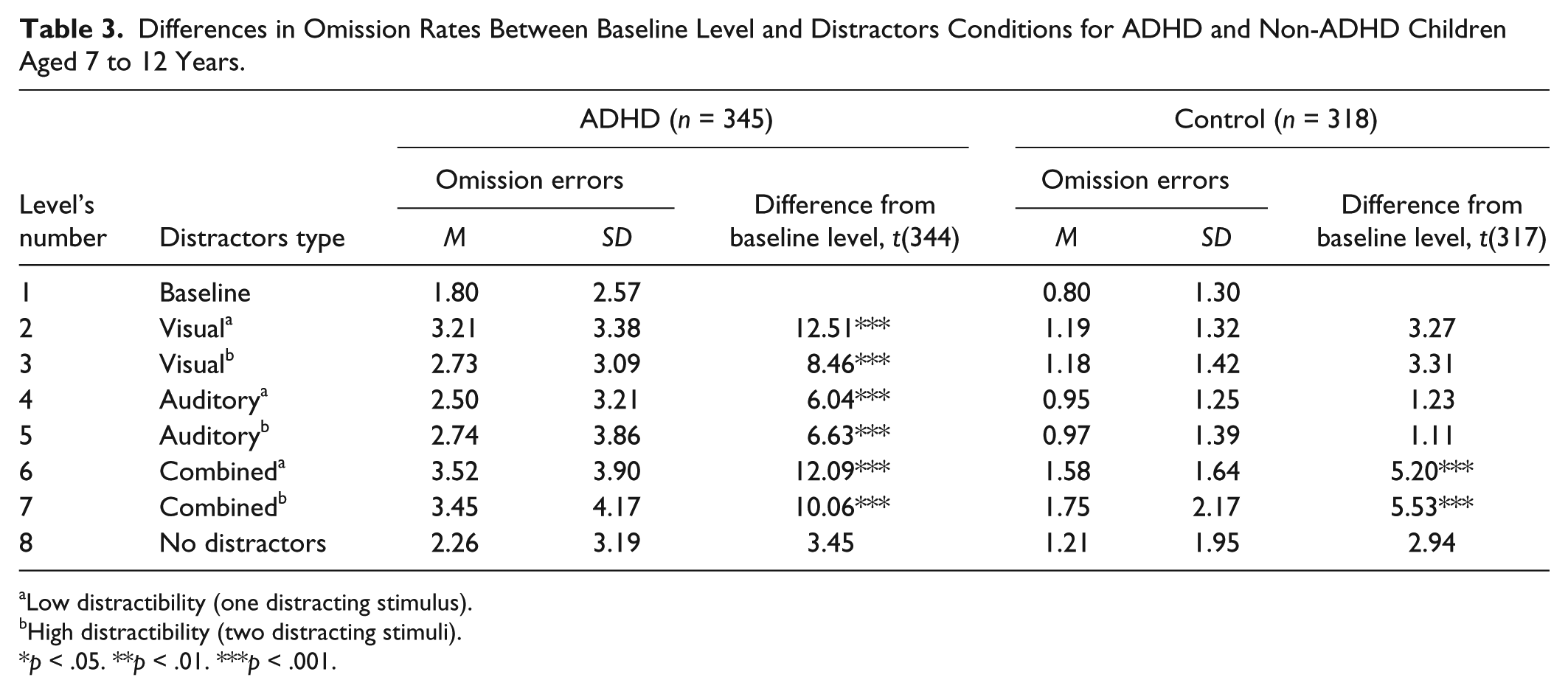
Low distractibility (one distracting stimulus).
High distractibility (two distracting stimuli).
p < .05. **p < .01. ***p < .001.
Differences in Omission Rates Between Baseline Level and Distractors Conditions for ADHD and Non-ADHD Adolescents Aged 13 to 18 Years.

Low distractibility (one distracting stimulus).
High distractibility (two distracting stimuli).
p < .05. **p < .01. ***p < .001.
However, in the control group, only combined distractors increased the rate of omission errors. The number of distracting stimuli did not affect the number of omission errors in non-ADHD children. ADHD adolescents produced more omission errors in the presence of visual distractors and the combination of visual and auditory distractors than in baseline level (Table 4). This finding was consistent for both low and high levels of distractibility. By contrast, the presence of pure auditory distractors did not increase the amount of omission errors as compared with baseline. In the control group, the presence of distractors did not significantly affect the amount of omission errors, as compared with baseline. The number of distracting stimuli does not affect the number of omission errors in adolescents with or without ADHD. In addition, neither children with ADHD nor controls (of any age group) demonstrated higher amount of omission errors in the last level of the test (no distractors) than at the beginning of it (baseline). Omission error rates for all groups and conditions are presented in Figure 2.
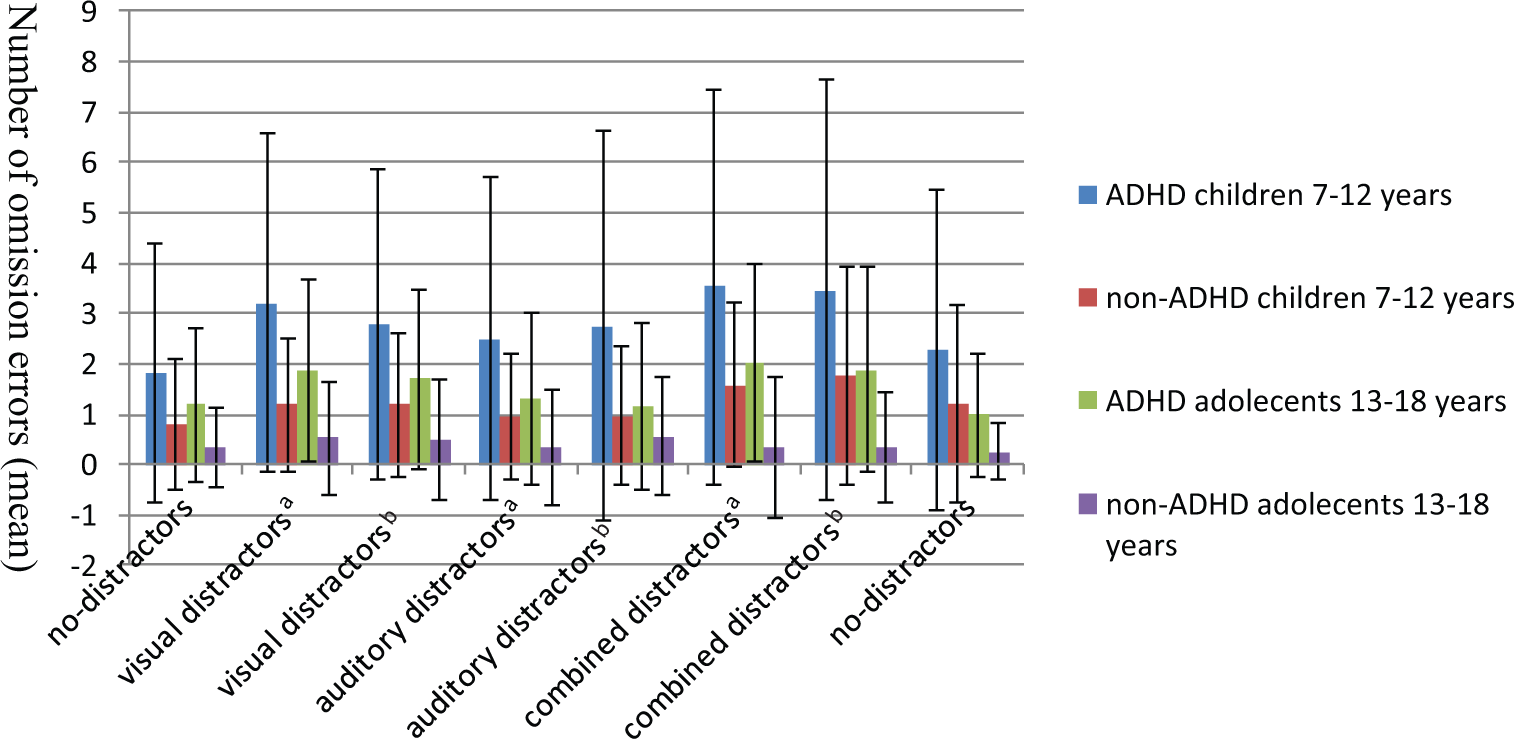
Omission errors in the presence of CPT distractors.
Discussion
The present study used a CPT task to investigate age-related changes in distractibility among children and adolescents with ADHD (7-18 years old) compared with their typically developing peers. Using the rate of omission errors as a marker of sustained attention, responses of two age groups of ADHD participants (children: age 7-12 years, and adolescents: age 13-18 years) were compared with those of their unaffected peers. Results showed that ADHD children and adolescents were more distracted than their typically developing peers. Although distractibility diminished in healthy adolescents, those with ADHD continued to be distracted in a way that resembled younger control children.
The current study provides further support for the association between healthy maturation and the increased ability to inhibit distracting information (Gumenyuk et al., 2001; West, Mendizabal, Carrière, & Lippé, 2014). A recent work by West et al. (2014) showed a strong relation between participants’ age (especially below 18 years old) and the degree of saccadic curvature away from the distractor stimulus. These results suggested that the increased development in frontally mediated inhibitory mechanisms is a significant factor contributing to the developmental trajectory slope. However, this strong impact of age on inhibitory processes is probably less clear for ADHD children. Similar to a previous CPT study in a narrower age span (Berger et al., 2013), examination of the age-related changes in distractibility in the MOXO-CPT revealed both continuity and discontinuity of ADHD phenomenology. In line with other studies showing a developmental lag in attention functions in ADHD children (El-Sayed, Larsson, Persson, & Rydelius, 2002; Lazzaro, Gordon, Whitmont, Meares, & Clarke, 2001), the current study found that distractibility of ADHD adolescents mirrored that of younger control children rather than of healthy adolescents. This study demonstrated that despite age-related improvement in attention functions in both groups, distractibility tended to diminish in non-ADHD adolescent, whereas ADHD participants were still sensitive to distractors even in their late adolescence. Taken together, these findings suggest that although part of the difficulties in ADHD could be explained by developmental delay that improves with time, other deficits, such as increased distractibility causing more omission errors, do not show a clear developmental trajectory.
In seeking the mechanisms that mediate the continuities and the discontinuities of ADHD over time, it is necessary to consider how a certain phenomenology is assessed and diagnosed across the life span (Rutter, 2013). Because ADHD phenomenology changes dramatically over time (Larsson et al., 2011), the use of similar criteria across the age span can be highly misleading. Hence, the marked drop between childhood and adulthood in the proportion of individuals who have ADHD—from 9.5% in children (Visser et al., 2014) to 4.4% in adults (Kessler et al., 2006)—should not be automatically interpreted as a major improvement in overall functioning but rather may indicate that the diagnostic definition, ways of assessment, and clinical manifestation change with age. Given these challenges, including additional objective measurements (such as the CPT) as aiding tools that can consistently evaluate ADHD phenomenology in different age groups parallel to diagnostic clinical criteria (Vaughn et al., 2011) may be of significance.
The question of why distractibility in response to auditory distractors reduced with increasing age, whereas distractibility in response to visual distractors persisted in ADHD participants, can have several explanations. Previous research confirmed that visual stimuli are more potent distractors for ADHD patients than auditory ones (Pelham et al., 2011). In case of visual tasks, such as the MOXO-CPT, visual distractors are even more interfering because they use the same cognitive modality as the main task (Wickens, 2008). It is also possible that due to impaired visual attention in ADHD (Kofler, Rapport, & Alderson, 2008), additional visual information easily overload the cognitive or the physiological system, thus interfering with performance (Armstrong & Greenberg, 1990). Furthermore, our results mirror a long line of electrophysiological work showing age-related Evoked Response Potential (ERP) changes in response to novel auditory sounds in healthy participants (Gumenyuk, Korzyukov, Alho, Escera, & Näätänen, 2004; Gumenyuk et al., 2001). This may offer a possible link between age-related physiological changes reflected by ERP and the development of attention control as observed in distractibility during CPT.
Interestingly, children with ADHD performed more omission errors in low-distractibility condition (visual and combined), in which one distractor was presented at a time than in high-distractibility condition, where two distractors were presented simultaneously. This finding could be attributed to the constant order of conditions presentation (i.e., low-distractibility condition was always followed by high-distractibility condition). Practice effects or adjustment to the distractor type could explain why children with ADHD found it more difficult to sustain their attention in the earlier stages of the test than in later ones, despite the growing number of distracting stimuli. The fact that adolescents and control children were not affected by the number of distracting stimuli may offer an alternative developmental route of responding to distractors. However, variable test conditions are needed to confirm this hypothesis.
Several limitations of this study should be considered. The most important shortcoming of this study is its cross-sectional design that prohibited the ability to draw within-subject, age-related changes in distractibility. Another limitation of this study is the limited information about participants’ personal and clinical characteristics, especially IQ level and ADHD subtypes, which can be associated with CPT performance (Collings, 2003; Mahone et al., 2002). In addition, because different levels of the MOXO-CPT were presented in a constant manner (namely, Levels 1-8), distractors’ effect may be confounded with time effects. However, our findings suggest that it might not be the case. In the current study, both ADHD and control groups did not perform more omission errors at the last level of the test (Level 8) than at the first one (Level 1). Moreover, in all groups, there was no linear increase in omission errors as the test progressed as we would expect if time was negatively associated with sustained attention. Finally, although the exclusion of ADHD children with severe comorbidities may clarify differences between ADHD and non-ADHD groups (Adisetiyo et al., 2014), it could also limit the generalization of our results.
In conclusion, the present results suggest that including environmental distractors in a CPT can improve the test’s ability to consistently distinguish ADHD from typically developing children as well as to measure age-related changes in attention performance. This study also demonstrates that distractibility problems tend to persist in ADHD, suggesting that deficit in inhibitory control might be the core of ADHD (Barkley, 1997, 1999). A confounding factor to nearly all ADHD studies is medication use, mainly stimulants (Heal, Cheetham, & Smith, 2009). Two recent meta-regression analyses suggested that stimulant use has a normalizing effect on neural abnormalities (Frodl & Skokauskas, 2012; Nakao, Radua, Rubia, & Mataix-Cols, 2011), thus questioning existing findings about age-related changes in ADHD symptoms. The fact that the entire sample of this study was drug naive strengthens our conclusions about persistence of attention deficits into adolescence.
Nevertheless, it should be noted that the present results were obtained at a group level and that further research is needed to assess normal and deficient development in individual children, adolescents, and adults. Current research (Bidwell, Willcutt, Defries, & Pennington, 2007; Rommelse et al., 2008) proposes that the use of intermediate phenotypes (endophenotypes) relevant to ADHD (e.g., response inhibition, working memory, temporal processing) can produce more consistent finding regarding neuropsychological and genetic correlations in ADHD compared with the classical approach centered on the categorical division of the syndrome (Kebir, Tabbane, Sengupta, & Joober, 2009). Indications of age-related changes in CPT performance may leave room for differentiating ADHD persisters from remitters in the future. This measure underscores the need to further examine potentially mediating effects of genetic and environmental risk factor, endophenotypes, and phenotype in ADHD.
Footnotes
Acknowledgements
The authors wish to acknowledge the dedicated help of Merav Aboud, Julia Melamed, and Ofra Haviv, and thank them for their professional, warm, and kind attitude toward the participants and their families.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In previous years, Dr. Berger was on Scientific Advisory Board or participated in continuing medical education programs sponsored by Janssen, Novartis, and Neuro-tech Solutions Ltd. All other co-authors declare no potential conflicts of interest with respect to this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.