
Abstract
Sleep accounts for 40% of total time in the daily activities of children (Meltzer & Mindell, 2008). Poor sleep quality can have negative effects on child development and on child functioning on many dimensions (Lewandowski, Toliver-Sokol, & Palermo, 2011). Longitudinal studies show that sleep problems among school-aged children predict anxiety disorders in adulthood (Gregory et al., 2005). These elements justify the importance of understanding sleep problems among children and better treating them.
ADHD and anxiety disorders are among the mental health problems associated most often with sleep problems in children. ADHD is a frequent neurodevelopmental disorder among school-aged children, with a prevalence ranging from 3% to 7% (American Psychiatric Association, 2000; Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007). In a meta-analysis, Cortese, Faraone, Konofal, and Lecendreux (2009) compared sleep problems in children with ADHD without anxiety comorbidity with children from a normal control group. Of the studies reviewed, 13 undertook objective measures to assess sleep problems (polysomnography in the sleep laboratory or actigraphy) whereas 6 administered a subjective questionnaire. The results with objective measures indicated that children with ADHD had longer sleep onset latency and more daytime somnolence. The questionnaires studies determined that children with ADHD had more bedtime resistance, longer sleep onset latency, more night awakenings, more difficulty getting up in the morning, more respiratory disorders during sleep, and more daytime somnolence. Data from this meta-analysis and more recent investigations tend to support the idea of cerebral hypoactivation among children with ADHD (Owens, 2008; Prihodova et al., 2010). Sleep deprivation in children may increase their attentional problems, underscoring the importance of detecting and treating sleep problems (Gruber et al., 2011).
The impact of medication on sleep problems in ADHD is controversial (Konofal, Lecendreux, & Cortese, 2010). Studies involving questionnaire measures suggest that children with ADHD on medication have more sleep problems than those not on medication, regardless of psychostimulant type and dosage (Cohen-Zion & Ancoli-Israel, 2004; Sangal et al., 2006). However, more recent investigation of carefully selected patients based on parental reports as well as objective measures do not confirm these results, and conclude that the severity of ADHD symptoms and psychiatric comorbidity, rather than medication, is associated with more severe sleep problems (Mayes et al., 2009; Moreau, Rouleau, & Morin, 2014; Stein, Weiss, & Hlavaty, 2012), stressing the importance of documenting symptom severity in such studies.
About a third of children and adolescents with ADHD are diagnosed as having anxiety disorders, the latter being present before age 6 years in 50% of cases (Adler, Barkley, Newcorn, Spencer, & Weiss, 2007; Brown, 2000; Jensen et al., 2001; Mayes et al., 2009; Merikangas et al., 2010). Having both ADHD and anxiety disorders may substantially worsen the outcome among children (Spencer, Biederman, & Mick, 2007). Alfano, Ginsburg, and Newman Kingery (2007) reported that 88% of young people with anxiety disorders also show at least one sleep problem, and 55% had three or more problems. The most frequent sleep problems are insomnia, nightmares, and fear of sleeping alone. The severity of anxiety symptoms is associated with the number of sleep problems. In a study of sleep measures in the sleep laboratory by Forbes et al. (2008), youths with anxiety disorders reported more night awakenings and longer sleep onset latency than young people with depression or normal controls. Two studies established that sleep problems were frequent among children with obsessive-compulsive disorder (Ivarsson & Larsson, 2009; Storch et al., 2008). The frequency of sleep problems in children with anxiety does not seem to vary by gender except for nightmares that are more common in girls (Alfano et al., 2007; Chase & Pincus, 2011). Despite their clinical relevance, all previously described studies were limited by the use of non-standardized sleep measures composed only of four to eight items.
Two studies examined the effect of treatment of anxiety symptoms on sleep problems among children. In the first study, cognitive-behavioral treatment of obsessive-compulsive disorder produced a small reduction of sleep problems, more specifically a decrease of nightmares and an increase in the capacity of children to sleep alone in bed (Storch et al., 2008). In the second study, pharmacological treatment (fluvoxamine) reduced insomnia and refusal to sleep alone more than placebo (Alfano et al., 2007). However, as mentioned above, previously published reports were limited to non-standardized sleep measures containing only a few items.
Anxiety comorbidity may explain, in part, the relationship between ADHD and sleep problems in children, according to questionnaires completed by parents (Corkum, Moldofsky, Hogg-Johnson, Humphries, & Tannock, 1999; Mick, Biederman, Jetton, & Faraone, 2000; Yürümez & Kılıç, 2013). Ivanenko, McLaughlin Crabtree, O’Brien, and Gozal (2006) compared five groups of children aged 5 to 18 years: ADHD alone, ADHD with psychiatric comorbidities, mood and anxiety disorders alone, other psychiatric disorders (adjustment disorder, pervasive development disorder, Tourette’s syndrome [impulse control disorder], conduct and oppositional-defiant disorder, reactive attachment), and healthy controls. Patients were recruited from a university child psychiatric outpatient clinic, and controls without reported psychiatric or medical problems came from the community. Combining the results from various questionnaires, these authors found that children with psychiatric disorders had more sleep problems than mentally healthy controls. ADHD children with mood and anxiety disorders had a higher frequency of nocturnal awakenings than ADHD children without psychiatric comorbidity and those with other psychiatric diagnoses. ADHD children with mood and anxiety disorders (and, to a lesser extent, ADHD alone) also experienced more bedtime resistance than children with mood and anxiety disorders alone. Unfortunately, the large age range (5-18 years) was a confounding factor as age may have an effect on some characteristics associated with sleep and the expression of psychopathology.
Hansen, Skirbekk, Oerbeck, Richter, and Kristensen (2011) were the first to compare sleep among children in selective and specific diagnostic groups recruited from two psychiatric outpatient clinics: ADHD, anxiety disorders, ADHD + anxiety disorders, and healthy controls recruited from nearby schools. Age range was not reported separately for each group but means (M) varied from 9.8 to 10.9 (standard deviation [SD] = 1.5-2.3). Administering a standardized sleep questionnaire, the Children’s Sleep Habits Questionnaire (CSHQ) completed by parents, Owens, Spirito, McGuinn, and Nobile (2000) found that children in the clinical groups experienced more sleep problems than the normal controls. Furthermore, children with ADHD + anxiety presented more sleep problems than children with ADHD only, but not children suffering from anxiety disorder only. Bedtime resistance was associated with anxiety disorders, whereas a greater number of nocturnal awakenings occurred in the ADHD + anxiety group. Daytime somnolence did not differ between the clinical groups.
Moreau et al. (2014) used actigraphy (at least five nights) and questionnaires completed by parents to characterize sleep in children with ADHD (Mage = 9.74 years), three quarters of whom were medicated for at least 1 year. Symptoms of anxiety were pooled together with those of depression and oppositional behavior on the Anxiety/Depression Subscale of the Child Behavior Checklist (Achenbach & Rescorla, 2001) completed by all parents. The results clearly showed that sleep problems were linked with anxiety/depression/oppositional comorbidity, but a formal diagnosis of anxiety disorders was established in only three children.
Treatment studies in children with ADHD and comorbid anxiety disorders have focused on sleep-oriented interventions and mostly targeted sleep-related anxiety (see, for example, Hiscock et al., 2015). To the best of our knowledge, no one has yet examined the effect, on sleep quality, of behavioral treatment specifically targeting anxiety disorders in children with ADHD and comorbid anxiety disorders. Data on this topic are critically needed as many sleep problems in children with ADHD may be explained by their anxiety symptoms (see above).
The first aim of the present study was to examine sleep problems in school-aged children with ADHD, anxiety disorders, or the two disorders in comorbidity, compared with Healthy Controls. The second aim was to explore the effect of cognitive-behavioral therapy (CBT) for anxiety on sleep problems in ADHD children with comorbid anxiety disorders.
Based on the literature, the following hypotheses were tested:
Method
Participants
The sample included 57 children (42 boys, 15 girls) aged between 8 and 12 years (M = 10.54; SD = 1.51) distributed in four groups: ADHD (n = 20), ADHD + Anxiety Disorder (n = 20), Anxiety Disorder (n = 8), and Healthy Controls (n = 9). Participants from the three clinical groups were consecutively referred children, recruited through the ADHD Clinic and the Anxiety Disorders Clinic of a university psychiatric hospital for children from a large city. The inclusion criteria were (a) age between 8 and 12 years, (b) diagnosed by a child psychiatrist to have ADHD or anxiety disorder or both, and (c) fluency in French. The exclusion criteria were post-traumatic stress disorder, obsessive-compulsive disorder, Tourette’s syndrome, mood disorder, autism, and intellectual disability. A subgroup of 10 children with ADHD + Anxiety Disorder participated in a CBT program treating symptoms of anxiety disorders. Among these 10 children, seven had two anxiety disorders or more, and four were diagnosed to have oppositional-defiant disorder.
Procedure
The study was approved by the Ethics Committee of Hôpital Rivière-des-Prairies. Children from the clinical groups were recruited at the ADHD Clinic and the Anxiety Disorders Clinic. Evaluation and diagnosis were performed by a multidisciplinary team comprised of a child psychiatrist, nurse, psychologists, and social workers. After parental consent was given for their children to participate in the study, the French version of the Anxiety Disorders Interview Schedule for Children (ADIS-C; Silverman & Albano, 1996) was administered to each child and to the parent who best knew the child, to assess the presence and severity of ADHD, anxiety disorders, and other disorders such as depression and oppositional-defiant disorder. Children were included in the study if they met the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) diagnostic criteria for ADHD, anxiety disorders, or both. Parents also completed a series of questionnaires described below.
Children from the healthy control group were recruited by letters sent to hospital personnel. The exclusion criteria were: (a) History of medical problems, including psychiatric, neurological, or sleep, (b) taking medication; and (c) signs of intellectual disability.
Treatment in the present study was adapted from “Super Squirrel,” a CBT treatment program designed for 9- to 12-year-old school-aged children with anxiety disorders (Turgeon & Brousseau, 1998). It was developed in French from well-known empirically based treatment programs, such as Coping Cat (Kendall, Safford, Flannery-Schroeder, & Webb, 2004) and FRIENDS (Barrett, Farrell, Ollendick, & Dadds, 2006). It involves ten 2-hr group sessions with parents and children, using the usual cognitive-behavioral strategies targeting anxiety symptoms such as education, relaxation training, problem-solving, cognitive restructuring, and exposure in vivo. The results of a clinical trial on 84 families assigned to either the treatment or control waiting-list group divulged a significant decrease of anxiety in children at 1-year follow-up (Turgeon, Marchand, Vitaro, & Brousseau, 1998). In the present study, the program was adapted to take into consideration the specific characteristics of children with ADHD (Berthiaume, Verreault, Turgeon, & Brousseau, 2008; Verreault, Berthiaume, Turgeon, & Brousseau, 2008). For example, all sessions followed the same structure with predictable routines as well as alternation between clinical tasks and activities for rest or play. Visual material and reinforcement strategies were also implemented to facilitate the children’s attention. The CBT groups each included three to four children only, once again to facilitate conditions for optimal attention. Children with only an anxiety disorder were not subjected to this treatment program because it was developed specifically to address ADHD with anxiety comorbidity. These children were rather oriented toward standard treatment of anxiety disorders in the Anxiety Clinic.
Measures for participant selection are described below, with follow-up for 3 weeks after the end of the treatment period.
Measures
Anxiety Disorders Interview Schedule for Children (ADIS-C), a semi-structured interview coherent with DSM-IV-TR diagnostic criteria, assesses anxiety disorders and other conditions in children and adolescents aged 7 to 17 years (Silverman & Albano, 1996). The severity of each disorder is ascertained by a trained clinician on an 8-point scale where a score of 4 or more indicates the presence of a problem that causes significant distress and/or interference in daily functioning. As recommended in the literature (Grills & Ollendick, 2003; Jensen et al., 1999), the diagnosis of ADHD and oppositional-defiant disorder is based on parent interview, whereas the diagnosis of anxiety and depression derives from both parent and child interviews. The ADIS-C may also specify ADHD subtypes. Silverman, Saavedra, and Pina (2001) reported that the ADIS-C shows good test–retest reliability, with correlations ranging from .78 to .95. Kappa coefficients are also good—from .80 to .90—for the combined diagnosis of anxiety based on parent and child interviews. Kappa coefficients for ADHD are excellent (1.00). Many studies have shown that the ADIS-C is sensitive to treatment (Brooks & Kutcher, 2003). The questionnaire has been translated into French by Turgeon and Brousseau (2001).
ADHD Rating Scale–IV: Parent Version
This questionnaire was considered as an additional measure of ADHD to compare the severity of ADHD symptoms between groups. The questionnaire comprises 18 items and is completed by parents to discern the frequency of ADHD symptoms coherent with DSM-IV-TR criteria (DuPaul, Anastopoulos, Power, Murphy, & Barkley, 1994; DuPaul, Anastopoulos, et al., 1998). The questionnaire showed good internal consistency and good stability over a 4-week period in a population of ADHD children (DuPaul, Power, McGoey, Ikeda, & Anastopoulos, 1998). Global score was significantly correlated with Conners’ Parent Rating Scales–Revised (DuPaul, Power, et al., 1998). Factorial analyses disclosed the presence of two factors (inattention and hyperactivity-impulsivity [HI]), corresponding to the conceptualization of ADHD in DSM-IV-TR (DuPaul, Anastopoulos, et al., 1998). Finally, ADHD Rating Scale–IV allows children with ADHD to be distinguished from healthy controls (Power et al., 1998).
Multidimensional Anxiety Scale for Children (MASC), in the present study, was an additional measure comparing anxiety symptomatology among groups. It is an adequate measure of anxiety in a standardized way in children and adolescents aged 8 to 19 years (March, Parker, Sullivan, Stallings, & Conners, 1997). It comprises a global scale and an index score that usually discriminate children with or without anxiety disorders. The MASC assesses four dimensions associated with anxiety: (a) physical symptoms, (b) avoidance, (c) social anxiety, and (d) separation and panic. The MASC is sensitive to treatment (Brooks & Kutcher, 2003). In a clinical population, the test–retest fidelity of global scores shows good intra-class correlations—from .79 to .93 on 3-week and 3-months intervals, respectively (March et al., 1997; March, Sullivan, & Parker, 1999). March, Conners, et al. (1999) reproduced the original factorial structure of the MASC in a clinical sample of 571 children with ADHD. According to Hinshaw et al. (1997), the MASC is valid in assessing anxiety in a population with ADHD. The questionnaire has been translated into French by Turgeon, Chartrand, Robaey, and Gauthier (2006). The French version reproduces factorial structure with four factors, and internal consistency for all scales is good.
The Children’s Sleep Habits Questionnaire (CSHQ: Owens, Spirito, et al., 2000) comprises 33 items and 8 dimensions associated with sleep bedtime resistance, sleep onset latency, total sleep time, anxiety related to sleep, night awakenings, parasomnias, respiratory problems during sleep, and daytime somnolence. For each item, the parent reports if the problem is observed rarely (0-1/week), sometimes (2-4 times), or often (5-7 times). Parents also indicate if behavior is problematic for the child. A global scale includes all sleep problems (“total score”). In the present study, another scale was created by computing the number of items considered as problematic by the parents. The CSHQ has good validity according to criteria of the Evidence-based Assessment Task Force (Lewandowski et al., 2011). The CSHQ also has good validity and good reliability in assessing sleep in school-aged children (Owens, Maxim, Nobil, McGuinn, & Msall, 2000). Among clinical samples, Cronbach’s alpha for global scale is .78 and ranges from .56 to .93 for subscales (Lewandowski et al., 2011). Sensitivity of the CSHQ is .80 and its specificity is .72 (receiver operating characteristic [ROC curve] = 0.41). The CSHQ was translated into French by one of the authors of the present article (R.G.), with permission from authors of the original version.
Medications
Medication type and dosage were assessed through reports from the parents. In children who participated in the treatment intervention program, medication type and dosage were evaluated during the CBT period to monitor changes. No changes in medication occurred in any of the participants.
Statistical Analyses
Statistical analyses were performed with SPSS Version 15.0. Because some variables did not show normal distribution and sample size was small in two of the groups, the non-parametric Kruskal–Wallis test was mainly conducted for group comparisons. Independent sample t tests were used when appropriate. Preliminary analyses compared groups for potential confounding variables. Then, analyses were performed on sleep variables. Post hoc analyses were undertaken according to the least significant difference method, which uses the Mann-Whitney U test. Cohen’s d coefficients measured the impact of treatment on variables that showed differences between the ADHD + Anxiety and ADHD groups (Cohen, 1988). Cohen’s d value of .20 reflects a small effect size, a value of .50 represents a medium effect size, and a value equal to or above 0.80 indicates a large effect size; positive d values suggest improvements in pre- to post-treatment scores.
Results
Preliminary Analyses
Age was not statistically different between the four groups, F(3, 57) = 6.52, p = .09, but gender ratio was, χ2(3) = 9.17, p = .03. There were more boys than girls in the control (100%), ADHD (80%), and combined ADHD + Anxiety groups (70%), whereas there were more girls in the anxiety group (57%), reflecting the bias observed in prevalence studies of childhood psychopathology (Beesdo-Baum & Knappe, 2012; Breton et al., 1999; Lecendreux, Konofal, & Faraone, 2011; Zahn-Waxler, Shirtcliff, & Marceau, 2008). The distribution of ADHD subtypes was comparable in the ADHD and ADHD + Anxiety groups (inattention type: 13 vs. 13; mixed type: 6 vs. 7; hyperactive-impulsive type: 1 vs. 0). The proportion of children with oppositional-defiant disorder did not differ in the same two groups (6 and 5 cases, respectively). Concerning the distribution of anxiety disorders, one half of children in the Anxiety and ADHD + Anxiety groups presented separation anxiety disorder or generalized anxiety disorder as the primary disorder, whereas the other half reported social anxiety or specific phobia. Table 1 reports the results of the four groups on other covariables. To summarize, the severity of ADHD symptoms was similar in the ADHD and ADHD + Anxiety groups. The severity of anxiety symptoms was similar in the Anxiety and ADHD + Anxiety groups. The two groups with ADHD did not differ in oppositional-defiant disorder.
Severity of ADHD, Anxiety and Oppositional-Defiant Disorder as a Function of Clinical Groups.
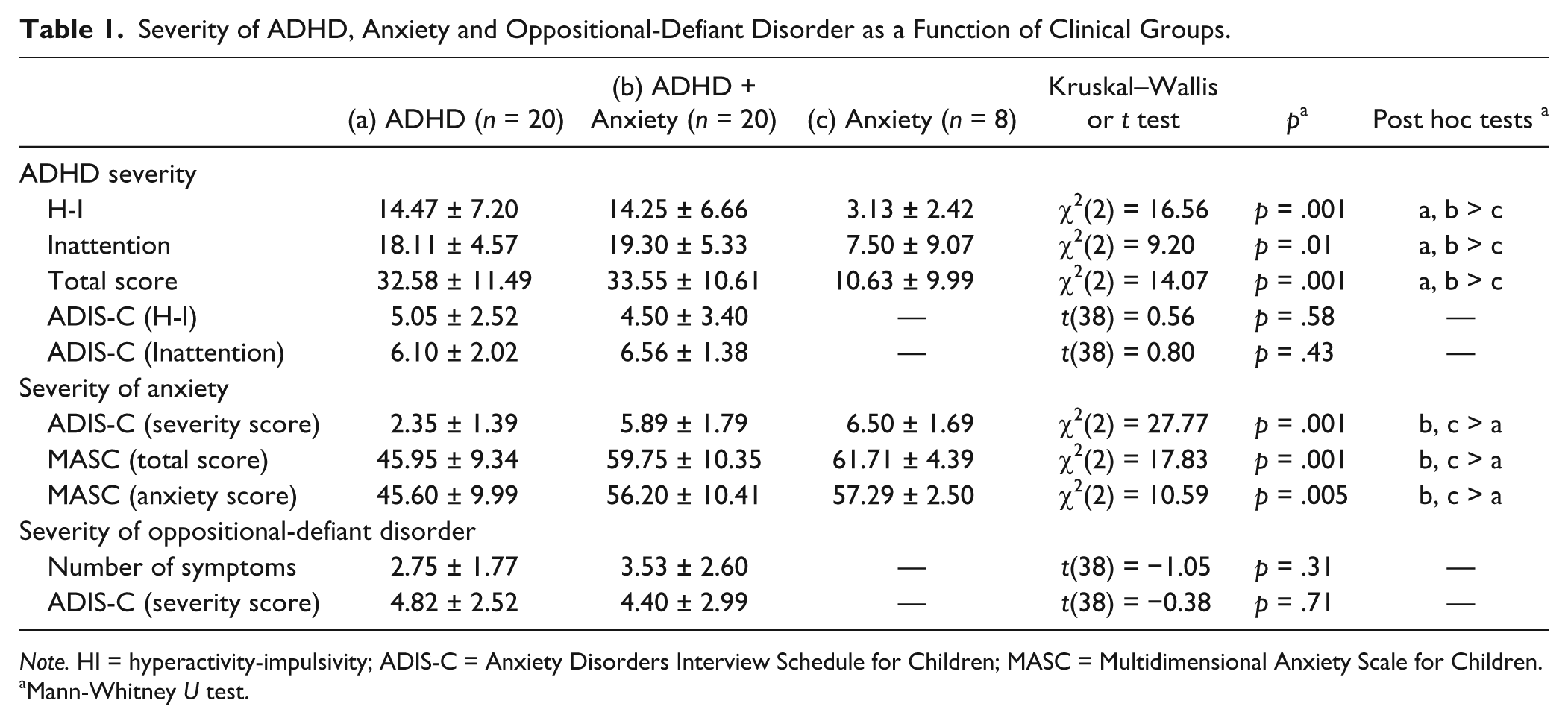
Note. HI = hyperactivity-impulsivity; ADIS-C = Anxiety Disorders Interview Schedule for Children; MASC = Multidimensional Anxiety Scale for Children.
Mann-Whitney U test.
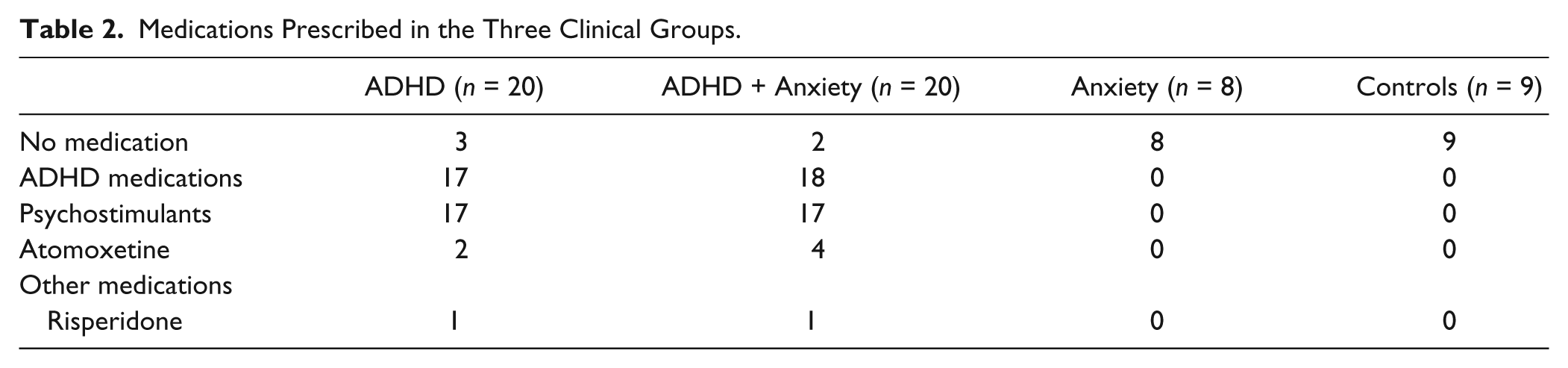
Table 2 portrays the use of medication in children as a function of groups. As Sangal et al. (2006) reported that atomoxetine (a non-psychostimulant medication) has less negative effects on sleep onset latency in children with ADHD than methylphenidate (a psychostimulant), we compared the distribution of medication types in the two groups of children with ADHD (psychostimulants vs. non-psychostimulants) and found no difference. The treatment regimen (medication and dosage) was monitored and proved to be stable for all participants.
Medications Prescribed in the Three Clinical Groups.
Sleep Problems Among Clinical Groups
The first aim of this study was to compare the specific effects of ADHD, anxiety disorders, and combined conditions on sleep problems in school-aged children. The three clinical groups and a control group were compared on two global scales and eight subscales of the CSHQ.
The two global scales (total score and number of problems) had significantly higher values in each clinical group compared with the control group (Table 3). Furthermore, these two scales had significantly higher values in the ADHD + Anxiety group than the ADHD group. Concerning specific sleep problems (scales 1 to 8), sleep onset latency and anxiety related to sleep were significantly greater in the three clinical groups compared with the Healthy Controls. Bedtime resistance and parasomnias were more severe in the two clinical groups with ADHD than the Healthy Controls. Daytime somnolence was more severe in the ADHD + Anxiety group compared with ADHD alone and the Healthy Controls whereas sleep latency was longer in the ADHD + Anxiety group than ADHD alone. Sleep duration revealed a non-significant trend to be shorter in the ADHD + Anxiety group compared with ADHD alone. No significant differences were evident between any pairs of groups for nocturnal awakenings and respiratory disorders.
Scores on the CSHQ at Baseline as a Function of Groups.
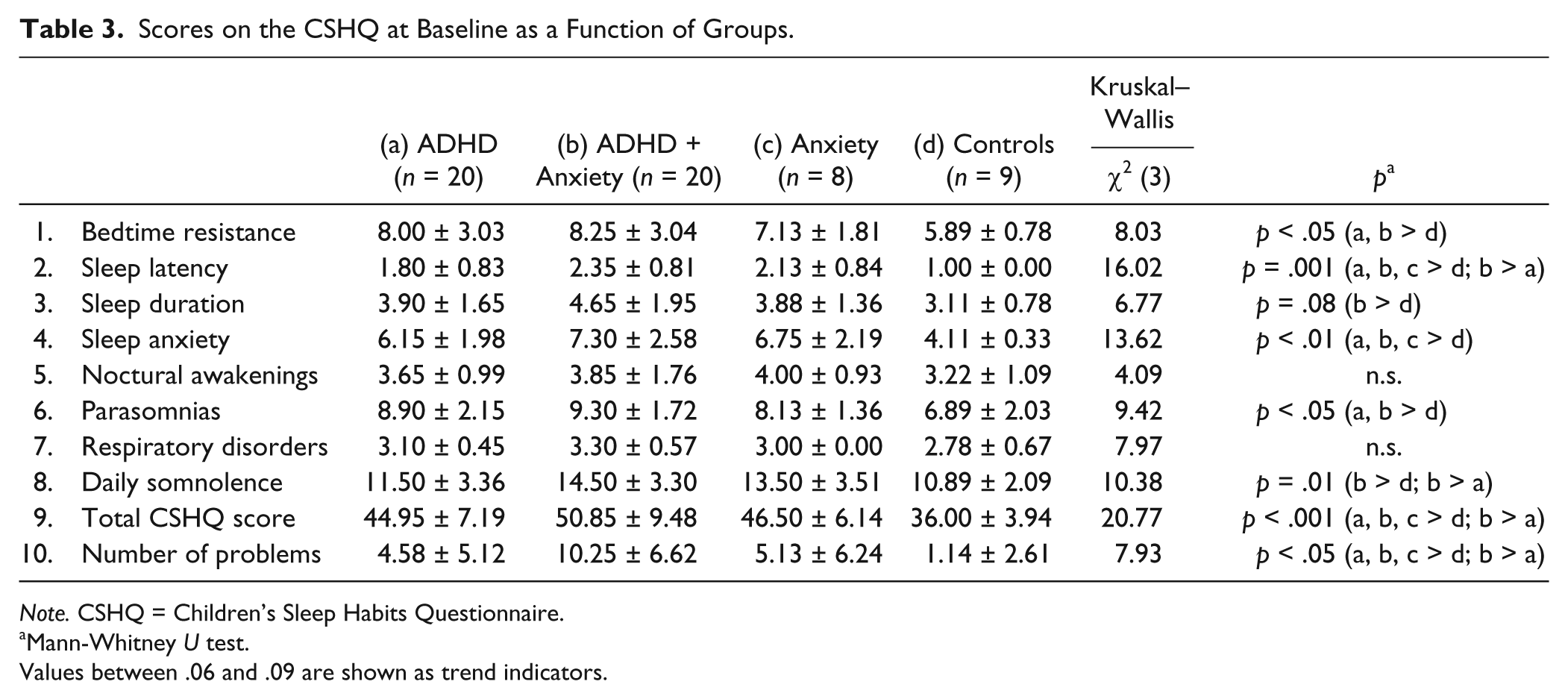
Note. CSHQ = Children’s Sleep Habits Questionnaire.
Mann-Whitney U test.
Values between .06 and .09 are shown as trend indicators.
Compared with the Healthy Controls, children with ADHD + Anxiety manifested more problems on six subscales whereas children with ADHD alone reported more problems on four subscales (Table 3). Finally, relative to the Healthy Controls, children with Anxiety Disorders showed more problems on two subscales. The Anxiety Disorder only group presented no significant differences whatsoever from either ADHD group.
Effect of Anxiety Treatment on Sleep Problems
The second objective of this study was to explore the effects of a CBT intervention for anxiety in a subsample of children with ADHD and comorbid anxiety. Table 4 reports pre- and post-treatment scores. As expected, treatment significantly decreased anxiety. On the standardized interview (ADIS-C), both primary and secondary anxiety disorders decreased, with large effect sizes. Considering the severity scale of the ADIS-C, the severity of primary anxiety disorder changed from severe to moderate, and the severity of secondary anxiety disorder went from moderate to low. With the questionnaire assessing child anxiety (MASC), mostly medium effect sizes were observed, with “Avoidance” showing only a small effect size. Among the sleep measures that were significantly different between the ADHD + Anxiety and ADHD groups, only sleep latency showed improvement with a large effect size: Other variables disclosed small effect sizes.
Effects of Cognitive-Behavioral Treatment of Anxiety on Anxiety Scales and Sleep Problems in 10 Children With ADHD + Anxiety.
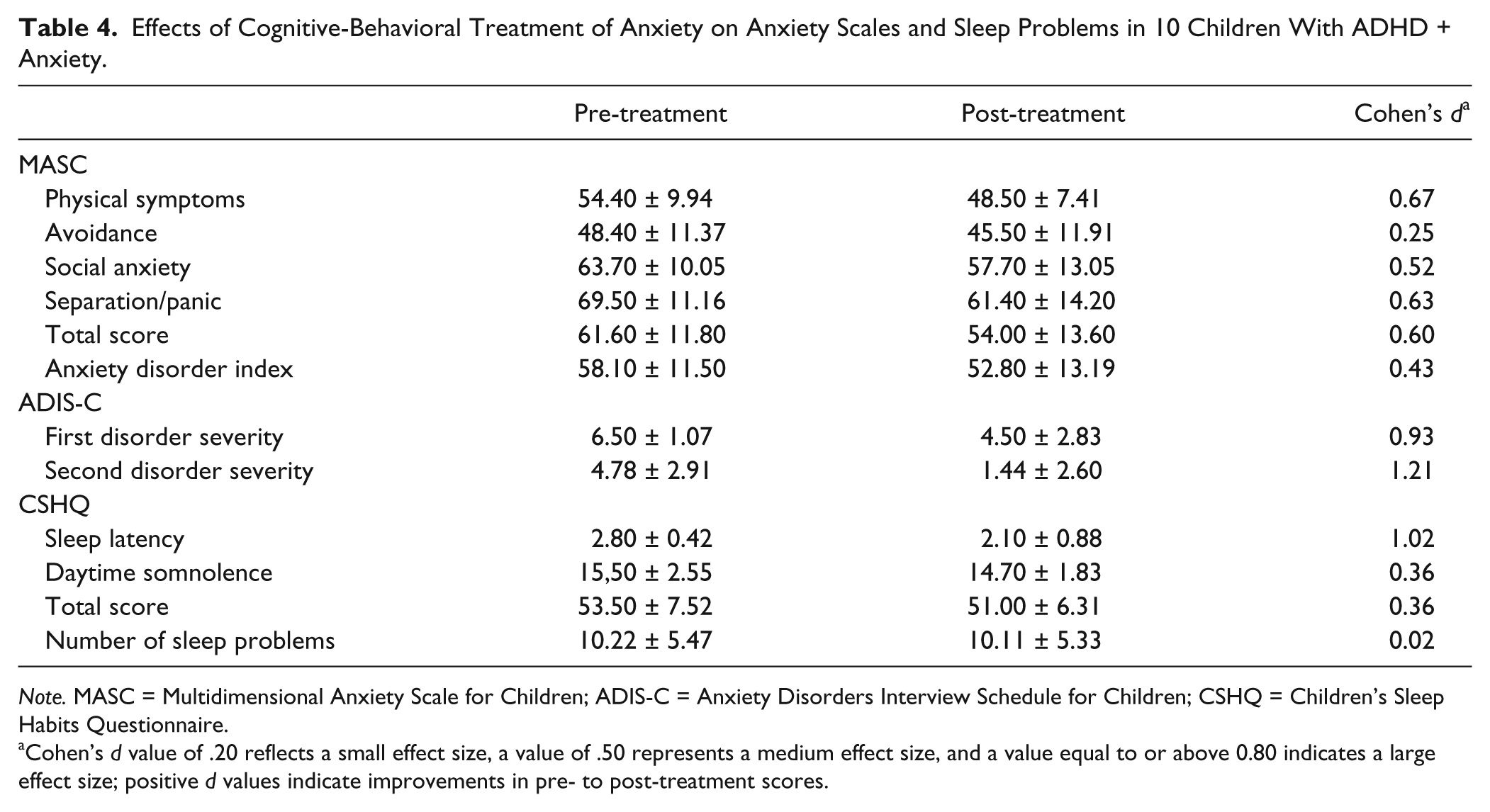
Note. MASC = Multidimensional Anxiety Scale for Children; ADIS-C = Anxiety Disorders Interview Schedule for Children; CSHQ = Children’s Sleep Habits Questionnaire.
Cohen’s d value of .20 reflects a small effect size, a value of .50 represents a medium effect size, and a value equal to or above 0.80 indicates a large effect size; positive d values indicate improvements in pre- to post-treatment scores.
Discussion
The first aim of this study was to compare sleep problems in children aged 8 to 12 years with ADHD, Anxiety Disorders, both ADHD and Anxiety Disorders, and healthy controls. The first hypothesis was that the three clinical groups would show a higher total amount of sleep problems and a greater number of specific sleep problems on the CSHQ than healthy controls, which proved to be the case.
The second hypothesis was that children with ADHD + Anxiety Disorder would display more sleep problems than the two other clinical groups. As expected, children with ADHD + Anxiety Disorder had the poorest sleep quality. Overall, this group showed more sleep difficulties as well as more specific problems in comparison with the Healthy Controls and the two other clinical groups. Hansen et al. (2011) reported that children with anxiety disorders and children with comorbid ADHD and anxiety had more sleep problems than children with ADHD alone, which was not supported in the present study. When compared with the Healthy Controls, the ADHD-only group experienced more sleep problems on four subscales whereas the anxiety group had more problems on two subscales. It is thus not possible to conclude, as in this previous study (Hansen et al., 2011), that sleep problems in children with ADHD and anxiety are better associated with anxiety than with ADHD itself. Alternatively, we propose that comorbid anxiety in ADHD children has a cumulative effect of sleep-related and non-sleep-related problems selectively associated with ADHD and anxiety alone, leading, in turn, to a more severe and possibly qualitatively more complex clinical picture.
The third and fourth hypotheses of the present study predicted that specific sleep problems would be coupled with each clinical condition. The third hypothesis was not confirmed as children with anxiety disorders (with or without ADHD) had more anxiety associated with sleep than Healthy Controls, but not more than children with ADHD only. This result could be at least partly explained by the fact that the primary symptoms of anxiety in half of our samples were usually less associated with sleep problems, that is, social anxiety and specific phobias. We learned later that five of the eight children in the Anxiety Disorder only group had two to four sessions of psychological treatment for anxiety symptoms before entering our study. It is thus possible that these sessions may have contributed to decreased anxiety and sleep problems in this group. Table 1, however, reports that MASC scores of the ADHD + Anxiety Disorder and Anxiety Disorder only groups were not different from one another and were higher than the ADHD-only group.
The prediction, according to which children with ADHD (with or without an anxiety disorder) would display more bedtime resistance and more daytime somnolence, compared with Healthy Controls and children with Anxiety Disorders (fourth hypothesis), was only partly confirmed. Bedtime resistance was higher in the two groups with ADHD (with or without comorbid anxiety) than the healthy controls, confirming that bedtime resistance seems to be associated with ADHD itself and not with anxiety. Sleep onset was longer in the three clinical groups compared with the control group of healthy children and it was longer in the ADHD + Anxiety than in the ADHD-only group.
It is known that the restless legs syndrome (RLS) can increase sleep onset latency and RLS can co-occur with ADHD (Cortese et al., 2013; Cortese et al., 2005; Picchietti & Picchietti, 2010) and with anxiety disorders (Earley & Silber, 2010; Picchietti & Picchietti, 2010). As treatment in the present study specifically improved sleep onset in children with ADHD + Anxiety Disorder, and although one cannot rule out the possible beneficial effects of behavioral interventions on the RLS (Pigeon & Yurcheshen, 2009), a parsimonious interpretation would be that RLS was not the main factor behind the observed delayed sleep onset at baseline.
Daytime somnolence was higher in children with ADHD and anxiety whereas children with ADHD only did not differ from the Healthy Controls. This result was unexpected because many studies have demonstrated that children with ADHD show longer sleep onset latency and more daytime somnolence than Healthy Controls (Cortese et al., 2009), suggesting that daytime somnolence is better associated with comorbidity than with ADHD itself. The possibility should be tested in studies with larger samples and with assessment tools specifically designed for daytime somnolence in children as those with anxiety disorders are reported not to show daytime somnolence despite the presence of sleep disturbances (Hudson, Gradisar, Gamble, Schniering, & Rebelo, 2009). Still, it has been proposed that symptoms of ADHD in children could be explained by daytime somnolence (Cortese et al., 2009). In the present study, children with ADHD + Anxiety Disorder were the only ones to show shorter sleep duration than Healthy Controls, and this may explain, in part, their greater daytime somnolence.
Part of the fifth hypothesis predicted that a CBT program designed for treating anxiety would decrease anxiety in children with ADHD and anxiety. This was fully supported as treatment was found to be effective in primary and secondary anxiety disorders. The decrease in anxiety after treatment in ADHD + Anxiety Disorder children was paralleled by shortened sleep onset latency. Future studies should assess whether this can be explained by diminished physiological arousal associated with anxiety. We suggest that treating anxiety in children with ADHD + Anxiety Disorder should include specific strategies to improve sleep quality and that such strategies would expectedly lead to more general improvement of sleep in these children. Studies reviewed by Ollendick, Jarrett, Grills-Taquechel, Hovey, and Wolff (2008) show that comorbidity with an externalized problem does not moderate the effect of treatment on anxiety problems. However, these studies use a broad definition of externalizing disorders and are not necessarily useful in understanding the specific effect of comorbidity between ADHD and anxiety disorders. In fact, Sciberras, Fulton, Efron, Oberklaid, and Hiscock (2011) have shown that one to two education sessions on sleep hygiene with parents of children with ADHD contributes to a significant decline of sleep-related behavioral problems in 67% of these children. Thus, it would be important to compare treatment in the present study to standardized CBT sessions for anxiety, to sort out the additional effects on children with ADHD and anxiety.
The results of this exploratory study must be interpreted with caution given some of its inherent limitations. First, the small sample size does not merit generalization of the results, and further research with larger groups is necessary. Second, it was not possible to compare groups on socioeconomic variables and determine whether they may have had an impact on the results. Still, there were no differences in ADHD symptom severity between the two ADHD groups (with and without comorbid anxiety). Third, sleep was assessed by parent-filled questionnaires, and studies have indicated that such measures have a tendency to underestimate sleep problems in children (Fricke-Oerkermann et al., 2007; Owens, Spirito, et al., 2000). Nevertheless, results from the present study disclosed significant sleep problems in children, some of whom were sensitive to group differences and to treatment effects.
In conclusion, this study emphasizes the need to better understand the underlying mechanisms underlying the frequent association between ADHD, anxiety disorders, and sleep disturbances. In that respect, quantification of symptom severity is key to the development and assessment of new treatment protocols.
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of Marjolaine Chicoine, MSc, with manuscript organization. They also thank all participants and parents for their invaluable contribution to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partly supported by the “Fondation Petits trésors de l’hôpital Rivière-des-Prairies” and the Bell Canada Mental Health Research Initiatives Support Program. MB was in receipt of a doctoral studentship award from the Canadian Institutes of Health Research.