
Abstract
Sleep problems are quickly becoming recognized as an international public health concern given rising prevalence estimates and documented associations with impairment (Gradisar, Gardner, & Dohnt, 2011; Stranges, Tigbe, Gomez-Olive, Thorogood, & Kandala, 2012). Recent estimates suggest that one in five children and young adolescents have sleep difficulties (Calhoun, Fernandez-Mendoza, Vgontzas, Liao, & Bixler, 2014). These high prevalence rates are concerning given that sleep problems have been linked to poorer functioning in both naturalistic and experimental studies (Astill, Van der Heijden, Van Ijzendoorn, & Van Someren, 2012; Beebe, 2011; Shochat, Cohen-Zion, & Tzischinsky, 2014).
ADHD and Sleep Problems
Multiple meta-analyses and reviews suggest that sleep problems (broadly defined as behavioral sleep difficulties, organic sleep disorders, and daytime sleepiness; Cortese, Faraone, Konofal, & Lecendreux, 2009) are more common in individuals diagnosed with ADHD in comparison with the general population (Cortese et al., 2013; Cortese et al., 2009; Owens et al., 2013). A diagnosis of ADHD has been linked to a wide range of sleep problems; however, evidence regarding which specific aspects of sleep are most commonly impaired in youth with ADHD is limited and mixed (Cortese et al., 2009; Gruber, 2009). As pointed out by Weiss and colleagues in a recent review (Weiss, Craig, Davies, Schibuk, & Stein, 2015), current prevalence estimates for sleep problems in ADHD vary widely from 9% to 70% (Chiang et al., 2010; Gau & Chiang, 2009; Mick, Biederman, Jetton, & Faraone, 2000) and likely depend upon the domain of sleep being measured and how the presence of a sleep problem is categorically defined (Fisher et al., 2014; Herman, 2015). The authors also note that potential differences across ADHD subtype/presentation (Mayes et al., 2009) and medication use (Kidwell, Van Dyk, Lundahl, & Nelson, 2015) further complicate prevalence estimates. Finally, prevalence estimates may vary considerably as a function of age (Maslowsky & Ozer, 2014; Shinkoda, Matsumoto, Park, & Nagashima, 2000), and the vast majority of research on sleep and ADHD has been focused on younger children and adults.
Prevalence of Sleep Problems in Adolescents With ADHD
Despite the fact that sleep is rapidly changing and is particularly important during the period of adolescence (Becker, Langberg, & Byars, 2015; Colrain & Baker, 2011; Shochat et al., 2014), little is known about sleep problems in adolescents with ADHD (defined as ages 10-18). To date, there have only been a handful of studies examining sleep in adolescents diagnosed with ADHD specifically, and most of these have been clinic-based samples (Fisher et al., 2014; Gau & Chiang, 2009; Mick et al., 2000), which may only identify youth with the most severe problems and/or access to services as compared with other identification methods such as school-based referrals (Atkins, Graczyk, Frazier, & Abdul-Adil, 2003; Kataoka, Zhang, & Wells, 2002). Furthermore, some of these studies have relied on broad measures of sleep problems that do not allow for the evaluation of specific sleep difficulties (Becker, Langberg, & Evans, 2015). Understanding which types of sleep problems are most common in adolescents with ADHD is important because specific sleep problems are differentially related to impairment. For instance, a recent meta-analysis with typically developing youth found daytime sleepiness to be one of the sleep domains most strongly correlated with academic impairment (Dewald, Meijer, Oort, Kerkhof, & Bogels, 2010), a primary domain of impairment in adolescents with ADHD (DuPaul & Langberg, 2014).
Daytime Sleepiness in ADHD
It is clear that daytime sleepiness is common in ADHD samples, with upward of 50% of adolescents with ADHD reporting fatigue or daytime sleepiness during the day (Brook & Boaz, 2005; Fisher et al., 2014). It has even been suggested that chronic underarousal is an etiological contributor to, or phenotypic correlate of, ADHD (Lecendreux, Konofal, Bouvard, Falissard, & Mouren-Simeoni, 2000; Miano et al., 2006). ADHD inattentive symptoms specifically are strongly correlated with daytime sleepiness (Becker, Luebbe, & Langberg, 2014; Oosterloo, Lammers, Overeem, de Noord, & Kooij, 2006), and there is likewise some evidence that daytime sleepiness may be more prevalent in youth with ADHD–Predominantly Inattentive Subtype/Presentation (ADHD-IA) compared with ADHD–Combined Subtype/Presentation (ADHD-C; LeBourgeois, Avis, Mixon, Olmi, & Harsh, 2004; Lecendreux et al., 2000; Mayes et al., 2009).
What is perhaps most intriguing about the high rates of daytime sleepiness in ADHD samples is the fact that elevated sleepiness does not appear to be wholly—or even primarily—attributable to nighttime sleep problems. For instance, there is mixed evidence as to whether adolescents with ADHD actually obtain less nighttime sleep than their peers (Moore et al., 2011), with one study finding that adolescents with ADHD actually obtained more weeknight sleep than adolescents without ADHD (Gau & Chiang, 2009). Furthermore, although youth with ADHD do appear to exhibit higher rates of distinct sleep problems in comparison with peers (Cortese et al., 2009), estimated prevalence rates for these specific problems are much lower than rates of daytime sleepiness. For instance, Mick et al. (2000) found sleep disorder prevalence among youth with ADHD to be 9%. Currently, no studies exist that have explored which specific sleep problems (e.g., night waking, disordered breathing, parasomnia symptoms) are most strongly associated with daytime sleepiness in adolescents with ADHD. This is important information for clinicians charged with assessing for ADHD and comorbid sleep problems. Sleep is multifaceted, and identifying an adolescent with ADHD as having “sleep problems” broadly does little to help clinicians target assessment and treatment efforts (Cortese et al., 2013). Furthermore, if distinct sleep problems and behaviors (e.g., bedtime resistance) are not actually responsible for the high rates of daytime sleepiness, this would have a significant implications for research examining the etiology of daytime sleepiness in youth with ADHD as well as intervention efforts.
Predictors of Daytime Sleepiness in Adolescents With ADHD
In addition to specific sleep problems, comorbid or co-occurring symptoms may account for the high rates of daytime sleepiness witnessed in adolescents with ADHD. Adolescents with ADHD exhibit high rates of comorbid internalizing disorders, such as anxiety and depression (Pliszka, 2000; Schatz & Rostain, 2006). Internalizing symptoms have been shown to predict sleep in ADHD samples (Accardo et al., 2012; Mayes et al., 2009) and found to at least partially explain group differences in sleep in comparing ADHD youth with controls (Bergwerff, Luman, & Oosterlaan, 2016; Gau & Chiang, 2009; Mick et al., 2000). Feeling lethargic and unmotivated are core characteristics of depression. It is possible that comorbid internalizing symptoms predict daytime sleepiness in adolescents with ADHD above and beyond specific sleep problems, but this has not been studied.
Sluggish Cognitive Tempo (SCT) symptoms also commonly co-occur with ADHD and are significantly associated with both ADHD inattentive and internalizing symptoms (Becker, Leopold, et al., 2016). Prior work has shown that SCT and daytime sleepiness, although empirically distinct, are significantly and strongly related (Langberg, Becker, Dvorsky, & Luebbe, 2014). This is not surprising given that some of the core characteristics of SCT include sluggish and sleepy behaviors. For example, in a normative university sample, Becker, Luebbe, and Langberg (2014) found that inattention and SCT predicted daytime sleepiness above and beyond sleep quality. Similarly, in a small sample of college students with ADHD (N = 58), Langberg, Becker, et al. (2014) found that SCT predicted daytime sleepiness above and beyond ADHD symptoms of inattention, anxiety, and depression. Recently, Becker, Garner, and Byars (2016) found that SCT symptoms were associated with greater daytime sleepiness in a sample of sleep-disordered children, even after controlling for ADHD, anxiety, and depressive symptoms. Accordingly, it may be that the slow and sleepy feelings associated with SCT account for the high rates of daytime sleepiness in youth with ADHD, above and beyond specific sleep problems. Interestingly, both SCT (Leopold et al., 2016) and internalizing problems such as depression (Merikangas et al., 2010) increase as children transition into adolescence, paralleling an increase in sleep problems across adolescence (Eaton et al., 2010). It is thus critical to examine the interrelations between comorbid symptoms, nighttime sleep problems, and daytime sleepiness in early adolescence when preventive and intervention approaches may be most optimally implemented.
Present Study
The goals of the present study were to (a) evaluate the prevalence of multiple distinct types of sleep problems in a large school-based sample of adolescents comprehensively diagnosed with ADHD, (b) explore whether sleep problems differ for adolescents with ADHD based on medication use or subtype/presentation, (c) evaluate which specific sleep problems are most strongly associated with daytime sleepiness, and (d) evaluate whether comorbid internalizing and SCT symptoms predict daytime sleepiness above and beyond the presence of specific nighttime sleep problems. This study builds on prior research using a well-validated, multidimensional measure of sleep, using a multiinformant design that includes both parent and adolescent report, focusing on a school rather than a clinic sample, and by simultaneously considering multiple potential predictors of daytime sleepiness.
First, we hypothesized that rates of daytime sleepiness would be significantly higher than rates of other specific sleep problems. Specifically, consistent with Fisher et al. (2014), we hypothesized that approximately half the sample would meet clinical cutoffs for daytime sleepiness. In comparison, we predicted that less than 10% of the sample would endorse significant problems in each of the other domains of sleep (Mick et al., 2000). Given longstanding interest in the roles of medication use and ADHD subtype/presentation in understanding elevated sleep problems among individuals with ADHD (Corkum, Moldofsky, Hogg-Johnson, Humphries, & Tannock, 1999; Mayes et al., 2009), and very few studies examining these factors in adolescents with ADHD, we explored whether sleep problems differed across these factors but did not make specific hypotheses.
In examining predictors of daytime sleepiness, we hypothesized that shorter sleep duration, sleep onset difficulties, and more night wakings would be the specific nighttime sleep domains most strongly associated with daytime sleepiness (Gibson et al., 2006; Saarenpää-Heikkila, Laippala, & Koivikko, 2001). Given prior research suggesting that sleep duration and daytime sleepiness are not highly related in ADHD samples (Langberg, Dvorsky, Marshall, & Evans, 2013), as well as significant associations between SCT and internalizing symptoms with daytime sleepiness (Becker, Leopold, et al., 2016; Langberg, Becker, et al., 2014; Saarenpää-Heikkila et al., 2001), we predicted that symptoms of anxiety, depression, and SCT symptoms would explain a significant proportion of the variance in daytime sleepiness above and beyond nighttime sleep functioning domains.
Method
Participants were 262 young adolescents in sixth through eighth grades (73.7% male) comprehensively diagnosed with ADHD (ages 10-15 years; M = 11.95, SD = 1.05). Self-reported race was 56.5% White (n = 148), 30.2% African American (n = 79), 10.3% biracial (n = 27), 2.3% other race (n = 6), and two participants chose not to respond. Additionally, 11.4% of the full sample (n = 30) identified as Hispanic or Latino. Of the sample, 65.3% were diagnosed with ADHD-IA and 34.7% were diagnosed with ADHD-C (see inclusion criteria below).
Procedure
This study was approved by the institutional review board (IRB) associated with the university where the research was conducted. Participants were recruited through study announcement letters mailed to parents/caregivers at local middle schools and direct referrals by school staff. During the inclusion/exclusion evaluation, adolescents and their parents/guardians independently completed questionnaires and a structured clinical interview. Adolescents were also administered a brief battery of cognitive and achievement testing. Adolescents were considered eligible for study participation if they (a) met full Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for ADHD-IA or ADHD-C on the Parent Children’s Interview for Psychiatric Syndromes, Parent Version (P-ChIPS; Weller, Weller, Fristad, Rooney, & Schecter, 2000), (b) evidenced significant impairment attributed to ADHD symptoms per parent and teacher reports, and (c) had an estimated Full Scale IQ (FSIQ) of ≥80 on the Wechsler Intelligence Scale for Children–Fourth Edition (WISC-IV; Wechsler, 2003). Adolescents were considered ineligible for study participation if they met criteria for psychosis, obsessive-compulsive disorder (OCD), or any bipolar disorder according to parent report on the P-ChIPS. Of note, comorbid oppositional defiant disorder (ODD) and conduct disorder (CD; based on diagnostic interviews with the parent) or anxiety/mood disorders (based on diagnostic interviews with the adolescents) were not exclusionary (30.6% of the sample met criteria for ODD, 3.2% for CD, 25.4% for anxiety, and 5.3% for depression).
ADHD diagnoses were determined using procedures similar to those used in the Multimodal Treatment Study of ADHD (MTA Cooperative Group, 1999). Specifically, to be included in the study, parents needed to endorse the presence of at least six symptoms of ADHD within a domain as occurring often or very often on the P-ChIPS, and these symptoms had to be associated with impairment in multiple settings. Furthermore, all other criteria for DSM-IV ADHD (i.e., age of onset, pervasiveness, impairment, and ruling out the possibility of other causal disorders) also had to be met. As part of the initial evaluation, the Vanderbilt ADHD Rating Scale was mailed to two core class teachers for each participant. The Vanderbilt is a well-validated teacher-report measure of DSM ADHD symptoms. In cases where the parent endorsed four or five symptoms within a domain on the P-ChIPS, supplementation with nonoverlapping symptoms from the teacher Vanderbilt was allowed (i.e., to reach the threshold of six symptoms within a domain). However, supplementation could only occur if the teacher endorsed at least four symptoms in a domain on the DBD. The same supplementation rules were used to make ADHD subtype determinations.
Measures
Children’s Interview for Psychiatric Syndromes (ChIPS)
The ChIPS (Weller et al., 2000) is a structured diagnostic interview which contains a parent (P-ChIPS) and child (ages 6-18) version (ChIPS). The ChIPS demonstrates high internal consistency and test–retest reliability (Fristad, Teare, Weller, Weller, & Salmon, 1998). It also shows high convergent validity with the Diagnostic Interview for Children and Adolescents–Revised–Child Version (DICA-R-C; Fristad et al., 1998). A recent review of child and adolescent diagnostic interviews (Leffler, Riebel, & Hughes, 2015) found five separate studies documenting that the ChIPS has good concurrent validity with other validated diagnostic interviews, including the DICA-R-C and the Kiddie Schedule for Affective Disorders and Schizophrenia for School Aged Children (K-SADS). Furthermore, the ChIPS has good construct validity, with the percentage of agreement between a consensus panel of child psychopathology experts and the results from ChIPS interviews ranging from 97.5% to 100% (Fristad et al., 1998).
Vanderbilt ADHD Diagnostic Rating Scale (VADRS)
The VADRS (Wolraich et al., 2003) is a DSM-IV-based scale that includes the 18 DSM-IV ADHD symptoms (nine inattention and nine hyperactive/impulsive items) as well as the eight DSM-IV ODD items. Parents/caregivers rate how frequently each symptom occurs on a 4-point Likert-type scale (0 = never, 1 = occasionally, 2 = often, 3 = very often). The VADRS produces an Inattention Subscale score (sum of the nine inattention items), a Hyperactive/Impulsive Subscale score (sum of the nine hyperactive/impulsive items), and an ODD score (sum of the eight items). The VADRS is frequently used in the ADHD research and demonstrates excellent psychometric properties (Wolraich et al., 2003). The Inattention (α = .87), Hyperactivity/Impulsivity (α = .90), and ODD (α = .87) scores were included in the regression model.
Behavior Assessment System for Children, Second Edition (BASC-2)
Adolescents completed the BASC-2 Self-Report Version (Reynolds & Kamphaus, 2004). Items are rated on a 4-point rating scale ranging from 1 (never) to 4 (almost always). There are 12 clinical subscales, with higher scores representing increased levels of maladaptive functioning. T scores greater than 65 are considered indicators of clinically significant levels of distress. The BASC-2 demonstrates excellent psychometric properties (Reynolds & Kamphaus, 2004). The Anxiety (α = .88) and Depression (α = .86) subscales from the BASC-2 were examined in the regression models.
Child Sleep Habits Questionnaire (CSHQ)
The CSHQ (Owens, Spirito, & McGuinn, 2000) is a 45-item parent questionnaire developed to evaluate sleep behavior in children. Although initial validation work focused on elementary age children (Owens, Spirito, & McGuinn, 2000), multiple studies with both clinical and community samples have since demonstrated that the CSHQ is also valid for use with adolescent samples (Becker, Ramsey, & Byars, 2014; Beebe, Rose, & Amin, 2010; Goldman, Richdale, Clemons, & Malow, 2012; Pakalnis, Splaingard, Splaingard, Kring, & Colvin, 2009). In reflecting on a recent “typical” week, parents report on a 3-point scale ranging from usually (score of 3) if the sleep behavior happened 5 to 7 times/week, sometimes (score of 2) for 2 to 4 times/week, to rarely (score of 1) for 0 to 1 time/week. Positively phrased items were reverse scored so that higher scores always indicate more sleep problems. The CSHQ yields a total score in addition to subscale scores which reflect specific sleep domains (Bedtime Resistance, Sleep Onset Delay, Sleep Duration, Sleep Anxiety, Night Wakings, Parasomnias, Sleep Disordered Breathing, and Daytime Sleepiness).
Of note, the CSHQ total score is calculated using all 33 items from the eight subscales. In addition, the current study used the Owens, Spirito, and McGuinn (2000) cutoff total score of 41, which was established using an intersect point of sensitivity and specificity. This cutoff score corresponded with the upper 23.3% of their control group’s total scores and correctly identified 80% of their clinical sleep group. In addition, consistent with prior prevalence research in adolescent samples (Fisher et al., 2014), the presence of a problem at the subscale level was defined as an item mean score of ≥2, indicating that the items/behavior(s) in that domain occurred at least “sometimes: 2 to 4 times in a typical week.” Owens, Spirito, and McGuinn found adequate internal consistency of the CSHQ total score in a community sample (α = .68); internal consistency was similar in the present sample (α = .63).
Sleep Self-Report (SSR)
The SSR (Owens, Maxim, Nobile, McGuinn, & Msall, 2000) is an 18-item self-report questionnaire assessing sleep problems that correspond to items found on the CSHQ. Reviews of evidence-based sleep measures indicate that the SSR is valid for use with children 7 to 12 years old (Lewandowski, Toliver-Sokol, & Palermo, 2011), with the Mage of the current sample being 11.95, and the SSR has also been used in multiple studies that included younger and older adolescents (Becker, 2014; Pirinen, Kolho, Simola, Ashorn, & Aronen, 2010). In reflecting on a recent “typical” week, adolescents are prompted to report whether a particular sleep behavior occurred on a 3-point scale ranging from usually (score of 3) if the sleep behavior happened 5 to 7 times/week, sometimes (score of 2) for 2 to 4 times/week, and rarely (score of 1) for 0 to 1 time/week. A total SSR score is derived from 13 items relating directly to the sleep domains found in the CSHQ (i.e., sleep duration, daytime sleepiness, difficulty falling asleep, and night wakings). Some items were reverse scored so that higher total scores consistently correspond with sleep problems. As with the CSHQ, the presence of a clinically significant problem at the subscale level was defined as an item mean score of ≥2, indicating that the behavior(s) occur at least “2 to 4 times in a typical week.” In the present study, the internal consistency of the items contributing to the total score was adequate (α = .67).
Pediatric Daytime Sleepiness Scale (PDSS)
The PDSS (Drake et al., 2003) is an eight-item questionnaire designed to measure sleepiness in children with self- and parent-report versions. The PDSS is one of the six sleep measures to meet criteria as “well established” according to the American Psychological Association Division 54 evidence-based assessment criteria (Lewandowski et al., 2011). Informants rate on a 5-point scale how often they/their child feel(s) sleepy during a usual week (4 = always, 3 = frequently, 2 = sometimes, 1 = rarely, 0 = never). These items are summed to produce a total sleepiness score that can range from 0 to 32. One item is reverse scored so that higher scores on all items reflect greater sleepiness. Consistent with prior work (Drake et al., 2003; Langberg et al., 2013; Maganti et al., 2006), a clinically significant problem with daytime sleepiness was defined as four or more items/problems rated as occurring frequently or always. Additional items were included at the bottom of the scale that asked parents and adolescents about bedtimes and wake times on weekdays and weekends. In the current study, the internal consistency was adequate for both parent (α = .76) and self-report (α = .79) total scores.
SCT Scale
The SCT Scale (Penny, Waschbusch, Klein, Corkum, & Eskes, 2009) was completed by adolescents and contains 14 items rated on a 4-point scale from 0 = never to 3 = very often. The Penny et al. scale is frequently used to measure SCT (Becker, Luebbe, & Joyce, 2015; Jacobson et al., 2012) and demonstrates adequate test–retest reliability between .70 and .87. Validity of the self-report version of this scale has demonstrated using bifactor modeling and confirmatory factor analysis (Smith et al., 2018). In the current study, the 14-item SCT total score was a predictor in the regression analyses and demonstrated good internal consistency (α = .86).
Services Use in Children and Adolescents–Parent Interview (SCA-PI)
The SCA-PI (Jensen et al., 2004) was administered to participants’ parents/caregivers to capture ADHD medication and other service use across mental health, primary care, school, and community settings. Test–retest reliability for reporting service use on the SCA-PI is excellent, overall kappa = .97 (Hoagwood et al., 2004). Parents were asked whether their child was currently taking medication for ADHD and this variable was included in the analyses.
Analytic Plan
To evaluate the prevalence of specific sleep problems, descriptive statistics were calculated based on parent and self-report of sleep problems on the CSHQ, SSR, and PDSS. Means, standard deviations, and ranges were calculated for each measure’s total score, subscale scores (i.e., within the CSHQ and SSR), and at the item level. In addition, the proportion of the sample whose subscale or total scores were above clinical thresholds was calculated (see “Measures” section for a description of clinical thresholds). Means, standard deviations, and ranges were also calculated for total time spent in bed, separated by parent and adolescent report, and by school nights and weekend nights.
Total scores on the PDSS, CSHQ, and SSR and time in bed were compared across ADHD presentation and ADHD medication status. Subgroup comparisons were conducted using independent samples t tests, and the significance value was set a priori to p < .01 to correct for conducting multiple tests. Cohen’s d values were also calculated to examine the magnitude of differences between the subgroup means.
To evaluate predictors of daytime sleepiness, the mean of the parent and self-report PDSS total scores was calculated and used as the dependent variable for the regression models. This allowed information from both raters to contribute to the overall report of daytime sleepiness, and it reduced the likelihood that the results would be confounded by within-rater bias. For additional preparation before conducting the regression models, a correlation matrix was calculated to check for possible multicollinearity among variables.
The first regression model included the subscale scores from the CSHQ and SSR and the amount of time spent in bed (average of parent and adolescent report) on school nights and weekend nights simultaneously entered into the model as predictors. The total variance in PDSS scores accounted for by these variables was examined, and each variable was also examined individually to determine whether it was significantly associated with the PDSS. Variables that were significant predictors were carried forward into the second regression model. Given the number of predictors entered into the model, the p-value threshold was set to be less than .01, rather than the traditional .05, to reduce the likelihood that a variable was found to be statistically significant by chance.
The second regression model evaluated whether symptoms of ADHD, ODD, SCT, anxiety, and depression and medication status accounted for significant variance in PDSS above and beyond sleep variables identified in the first model. This regression was hierarchical: The first step included all the significant sleep variables identified in the first regression, and the remaining variables were added on the second step to allow for evaluation of ΔR2. In the final model, the predictor variables were again individually examined for statistically significant associations with the PDSS using a p-value threshold of less than .01.
Results
Prevalence of Sleep Problems
Descriptive statistics are presented in Table 1. Using the CSHQ total score, nearly three quarters of the sample (72.8%) was above the clinical threshold for total sleep problems. However, less than 8% of the sample met the clinical threshold on any of the individual CSHQ subscales, with the exception of the Daytime Sleepiness subscale (27.8%). The individual subscales on the SSR followed the same pattern. Specifically, 21.6% of the sample was above the threshold on the Daytime Sleepiness subscale but only 7.6% for Bedtime Behavior and 6.5% for Sleep Behavior. When examining the PDSS, a higher portion of the sample (37% based on parent report and 43% self-report) scored higher than the established clinical threshold in comparison with the CSHQ and SSR Daytime Sleepiness subscales.
Total Score Descriptive Statistics, Item-Level Descriptive Statistics, and Percentage Above Clinical Cutoffs for Sleep Problems on PDSS, CSHQ, and SSR.
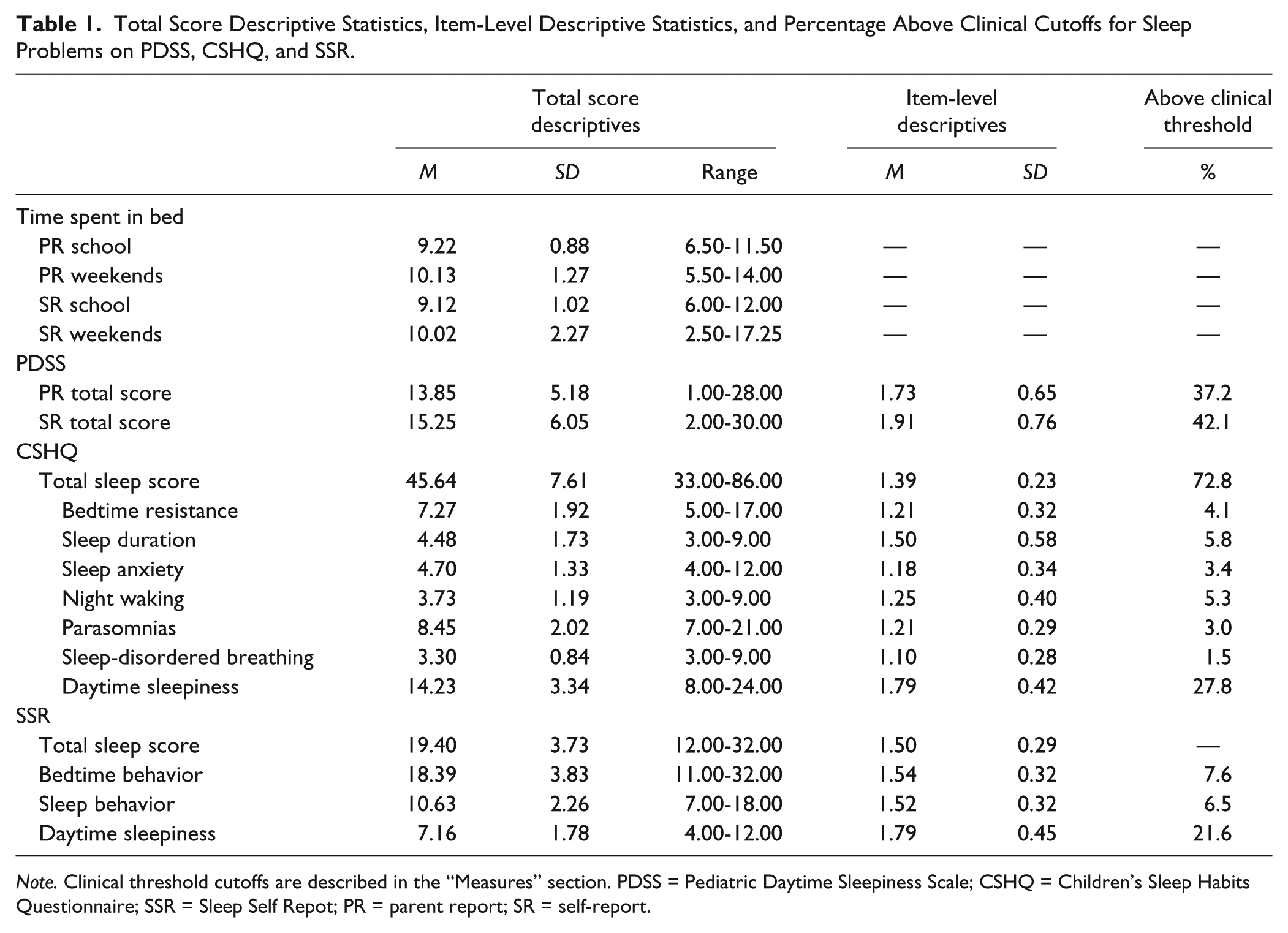
Note. Clinical threshold cutoffs are described in the “Measures” section. PDSS = Pediatric Daytime Sleepiness Scale; CSHQ = Children’s Sleep Habits Questionnaire; SSR = Sleep Self Repot; PR = parent report; SR = self-report.
Independent-samples t tests revealed no significant differences between adolescents with ADHD-IA or ADHD-C Presentation in their total scores for the CSHQ, SSR, and PDSS, or parent or adolescent report of time in bed on school nights or weekend nights (all ps > .01). Similarly, no significant differences were observed based on whether or not the adolescent was taking medication (all ps > .01). Furthermore, Cohen’s d values comparing group means revealed a small or negligible difference between ADHD presentation and medication subgroups for all measures (see Table 2).
Paired Comparisons of Time in Bed, Daytime Sleepiness, and Sleep Problems by ADHD Subtype and Medication Use.
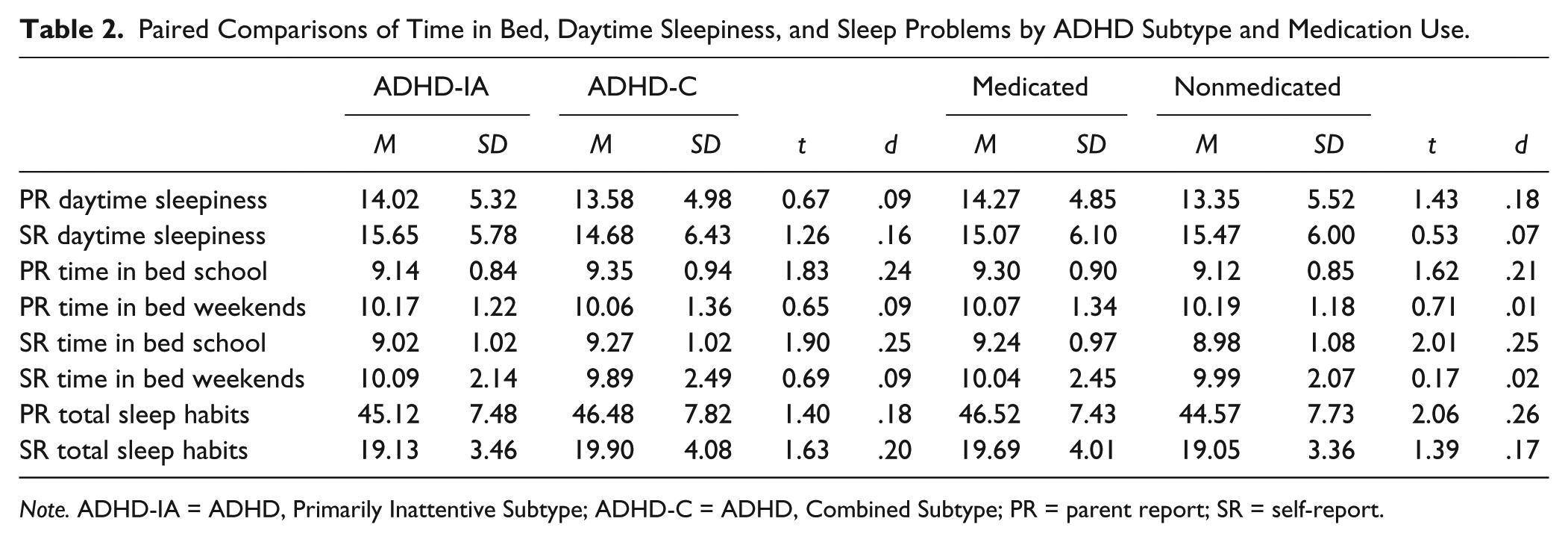
Note. ADHD-IA = ADHD, Primarily Inattentive Subtype; ADHD-C = ADHD, Combined Subtype; PR = parent report; SR = self-report.
Predicting Daytime Sleepiness
The correlation matrix including all predictor variables is presented in Table 3. The majority of correlations were small to moderate and no correlations exceed .6, suggesting that multicollinearity was not a problem. The first regression, including all CSHQ and SSR subscales (with the exception of the Daytime Sleepiness subscales) in a single model predicting the mean PDSS score, accounted for a statistically significant portion of the variance, F(10, 248) = 8.23, p < .001, R2 = .27. The Bedtime Resistance subscale of the CSHQ (β = .20, p = .008), the average number of hours spent in bed on school nights (β = −.18, p = .002), and on weekend nights (β = .21, p < .001) were the only individually significant predictors. All three of these variables were subsequently carried into the second regression model.
Means, Standard Deviations, and Intercorrelations of Study Variables.
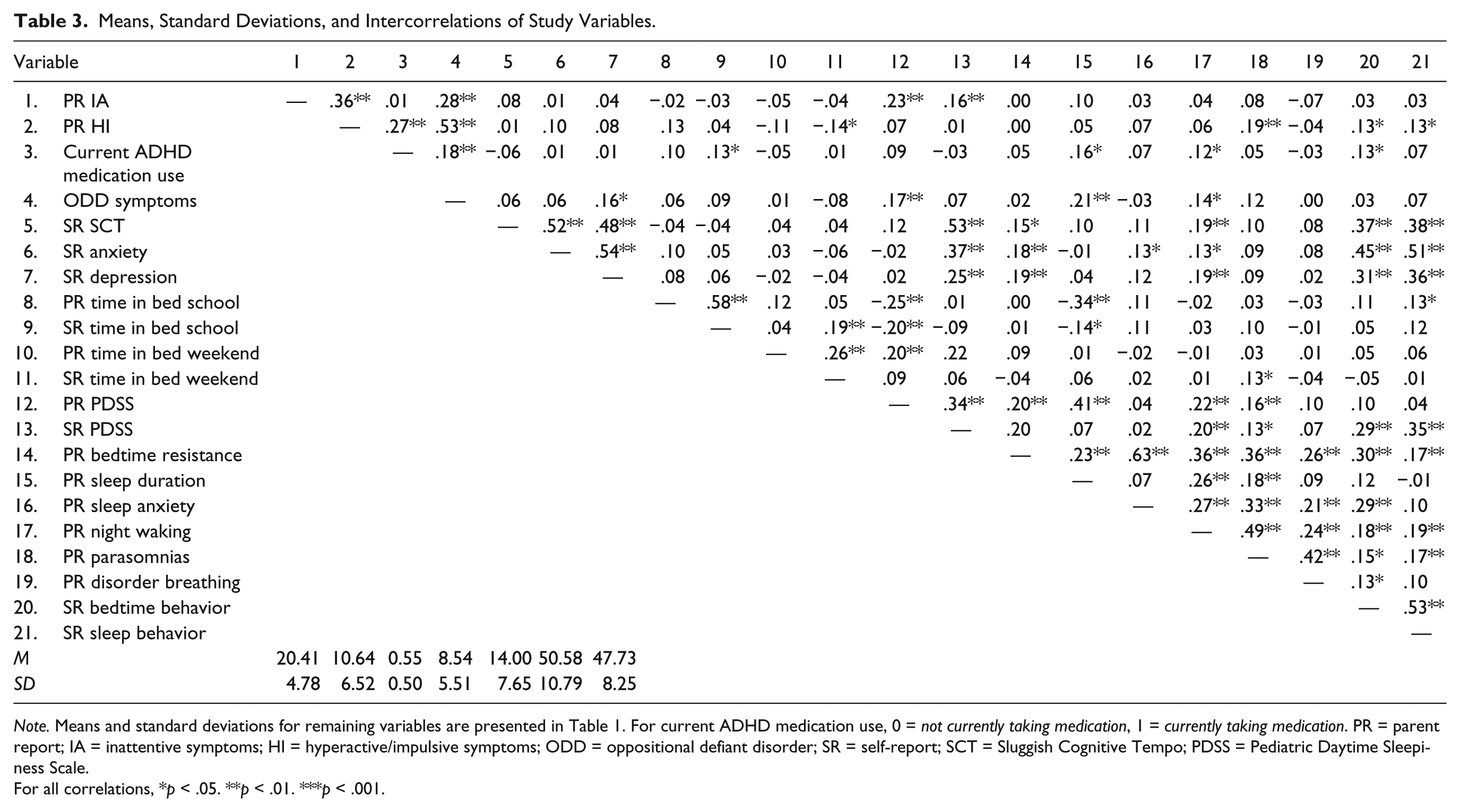
Note. Means and standard deviations for remaining variables are presented in Table 1. For current ADHD medication use, 0 = not currently taking medication, 1 = currently taking medication. PR = parent report; IA = inattentive symptoms; HI = hyperactive/impulsive symptoms; ODD = oppositional defiant disorder; SR = self-report; SCT = Sluggish Cognitive Tempo; PDSS = Pediatric Daytime Sleepiness Scale.
For all correlations, *p < .05. **p < .01. ***p < .001.
Step 1 of the second regression, including bedtime resistance and time in bed on school and weekend nights, was significant, F(3, 255) = 13.97, p < .001, R2 = .14. Step 2 was also significant, F(10, 248) = 8.66, p < .001, R2 = .33, and accounted for significantly more variance in the mean PDSS score as compared with the base model, ΔF(7, 248) = 10.26, p < .001, ΔR2 = .19. In the final model, bedtime resistance (β = .19, p < .001), average time in bed on school nights (β = −.20, p < .001), and average time in bed on weekend nights (β = .21, p < .001) remained significantly associated with daytime sleepiness. From the variables entered on the second step, parent report of ADHD inattentive symptoms (β = .20, p < .001) and self-report of SCT symptoms (β = .35, p < .001) were the only variables that were significantly associated with PDSS ratings. The results of the full regression model are presented in Table 4.
Regression Model for Significant Sleep Factors and Relevant ADHD Factors Predicting PDSS Scores.
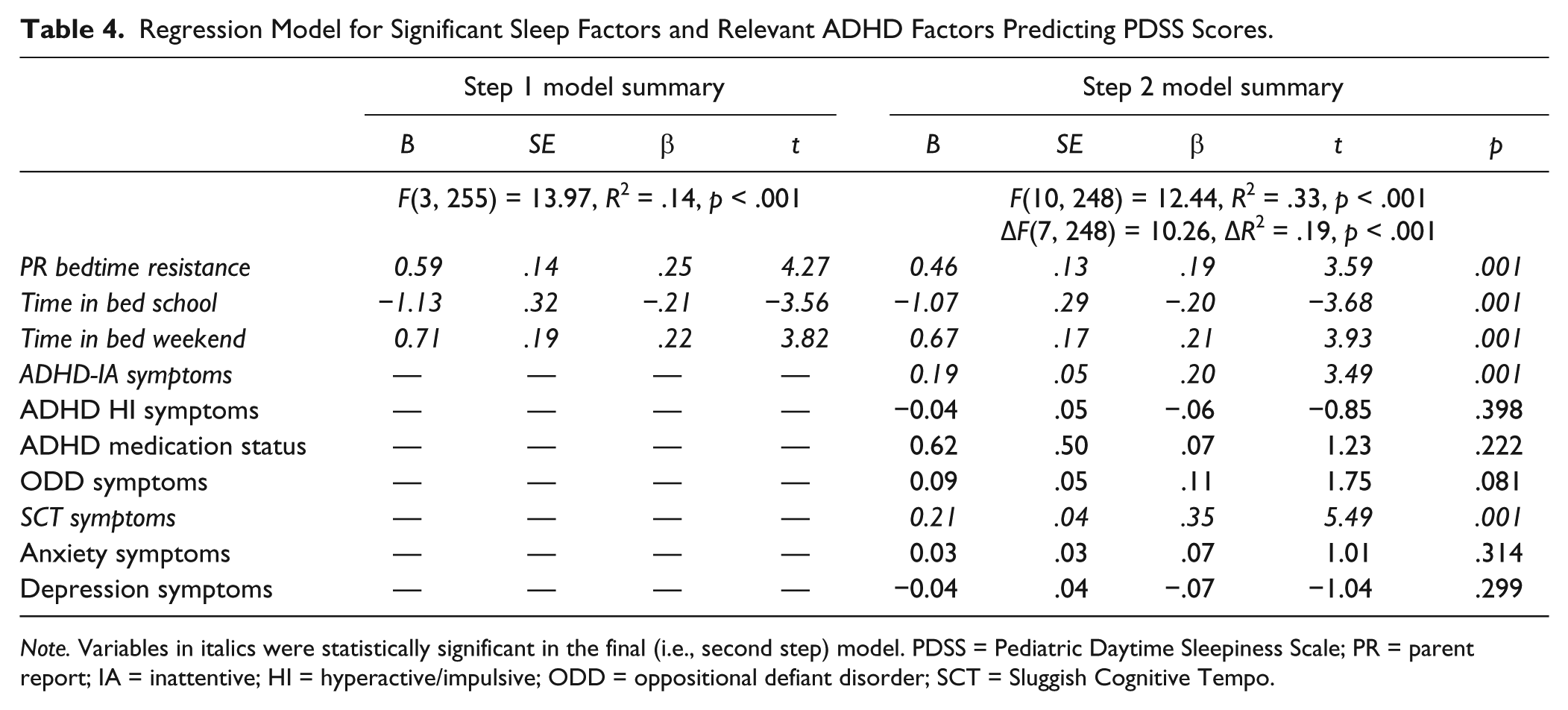
Note. Variables in italics were statistically significant in the final (i.e., second step) model. PDSS = Pediatric Daytime Sleepiness Scale; PR = parent report; IA = inattentive; HI = hyperactive/impulsive; ODD = oppositional defiant disorder; SCT = Sluggish Cognitive Tempo.
Discussion
This study evaluated the prevalence of sleep problems and predictors of daytime sleepiness in a large sample of young adolescents comprehensively diagnosed with ADHD. A remarkable 72% of the sample met the threshold for clinically significant overall sleep problems based on parent report (i.e., CSHQ total score). However, when separately considering the specific sleep domains assessed on the CSHQ and SSR, rates of specific sleep problems in the sample were relatively low (1.5%-7.6%). The exception to this pattern— across raters, measures, ADHD presentation, and medication use—was the high prevalence of clinically significant daytime sleepiness (21.6%-42.1%). Based on these findings, it appears evident that the “sleep problems” often cited in youth with ADHD are largely driven by high rates of daytime sleepiness (see Table 1). In seeking to identify predictors of daytime sleepiness, time in bed and bedtime resistance were the most important sleep variables, and inattention and SCT symptoms predicted daytime sleepiness above and beyond these sleep variables. Implications of these findings and directions for future research are discussed in the subsequent sections.
The high prevalence of daytime sleepiness found in this study is consistent with one of the only other studies to evaluate prevalence specifically in an adolescent with ADHD sample. Fisher et al. (2014) reported that 43% of adolescents with ADHD endorsed significant problems with fatigue, almost identical to the rates found in the present study that assessed daytime sleepiness specifically using the PDSS. Notably, the Fisher et al. study demonstrated the importance of evaluating sleep and ADHD from a developmental perspective, as children in their sample endorsed relatively low rates of fatigue, and it was not until adolescence that high rates were present. The low prevalence of specific sleep problems found in this study is consistent with an emerging body of research using objective measures (i.e., actigraphic studies), showing that children with and without ADHD do not significantly differ in sleep quality or quantity (Bergwerff et al., 2016; De Crescenzo et al., 2016). It is worth noting that the threshold set for a domain specific sleep problem in this study was relatively low. On the specific CSHQ and SSR scales, participants with an item mean score ≥2 (i.e., “sometimes”) were considered to have a clinically significant problem in that area. Despite this low threshold, only the Daytime Sleepiness subscale on the CSHQ and SSR had a prevalence of higher than 8% in the sample (see Table 1). Overall, these findings call into question the clinical utility of the CSHQ total cut-score of 41 for use with adolescents with ADHD and suggest a more conservative cutoff may be needed. There is uneven item representation across the CSHQ subscales, with the Daytime Sleepiness scale having the largest number of items (n = 8) relative to the other scales. Accordingly, the 72% of the sample that met the total score threshold was largely a function of the high rates of daytime sleepiness. Given the unequal influence of particular sleep domains, it is recommended that clinicians using the CSHQ to screen for sleep problems in youth with ADHD focus on the specific domain scores rather than the total cut-score.
Given the high rates of daytime sleepiness in the sample, the analyses evaluating which variables were most strongly associated with the parent and adolescent PDSS scores are important. In contrast to our hypothesis, in the initial model, with only sleep variables as predictors, the only CSHQ or SSR subscale that significantly predicted daytime sleepiness was the Bedtime Resistance subscale from the CSHQ. It is important to note that the items on the Bedtime Resistance subscale do not assess active resistance to bedtime through child oppositionality, defiance, or delaying tactics. Rather, the Bedtime Resistance subscale items focus on poor sleep habits (e.g., “goes to bed at same time,” “falls asleep in own bed”), separation anxiety related to sleep (e.g., “afraid of sleeping alone,” “needs parent in room to sleep”), and general difficulties around bedtime (e.g., “struggles at bedtime”). Thus, our findings indicate that poor sleep habits and separation anxiety around bedtime are associated with greater daytime sleepiness, perhaps due to an inconsistent sleep schedule/structure and/or poor quality sleep. It is also noteworthy that two of the three variables most strongly associated with daytime sleepiness were the total time spent in bed on school nights and weekends. This finding is intriguing in the context that both parents and adolescents reported that adolescents spent greater than 9 hr in bed per night on weekdays on average and around 10 hr per night on weekends on average. The term time in bed is used here because these figures are based on participants and their parents reporting “what time did you go to bed” and “what time did you wake up.” Accordingly, these data might not accurately reflect sleep duration if adolescents are experiencing difficulties with transitioning from the bedtime routine to a sleep state (e.g., delayed sleep onset). Furthermore, it is important to recognize that reporting average time in bed may mask intraindividual variability in sleep patterns and problems (Becker, Sidol, Van Dyk, Epstein, & Beebe, 2017).
There is some evidence that youth with ADHD have significantly higher intraindividual variability of sleep (e.g., a larger standard deviation of hours slept over a 1-week period) in comparison with their peers (Gruber & Sadeh, 2004) and greater day-to-day variation in sleep onset latency in comparison with both typically developing peers and peers with other psychiatric disorders (Hvolby, Jorgensen, & Bilenberg, 2008). It has been hypothesized that this variability is due to “problematic nights” resulting from a combination of factors, including high rates of comorbid mental health conditions, family factors, and homework problems such as procrastination and homework completion difficulties that negatively affect bedtime, sleep latency, and sleep quality (Moreau, Rouleau, & Morin, 2014). The measures used in this study are not designed to capture this variability. For example, even with the occurrence of one poor night’s sleep, average time in bed across a week’s time could still be more than 9 hr. Similarly, a significant problem with sleep onset latency that occurred once per week would be rated as never or sometimes on the CSHQ or SSR but could still have a significant impact on functioning. Accordingly, additional research is needed that evaluates the sleep of adolescents with ADHD on a more micro day-to-day level. However, it remains the case that in the present study, time in bed and all the CSHQ and SSR subscales together only accounted for 27% of the variance in daytime sleepiness. This finding begs the question, what other factors are leading approximately 40% of the sample to endorse clinically significant problems with sleepiness?
The second regression model, including time in bed, bedtime resistance, ADHD symptoms, ODD symptoms, medication status, and symptoms of SCT, anxiety, and depression, accounted for 33% of the variance in daytime sleepiness. Adolescent-reported symptoms of SCT and parent-reported inattention were the strongest predictors in the model, predicting daytime sleepiness above and beyond time in bed and bedtime resistance. Previous research demonstrates that although empirically distinct, there is considerable overlap between the constructs of SCT, inattention, and daytime sleepiness (Becker, Luebbe, & Langberg, 2014; Langberg, Becker, et al., 2014). SCT includes symptoms of slowness, mental confusion or “fogginess,” excessive daydreaming, low motivation, and drowsiness (Becker, Leopold, et al., 2016). Similarly, inattentive symptoms can look functionally similar to daytime sleepiness in the form of high distractibility or difficulty focusing for long periods of time. This finding raises the possibility that high rates of daytime sleepiness in ADHD samples at least partially represent a subjective feeling of underarousal, rather than solely being a problem with nighttime sleep functioning. It is likewise possible that a systemic, chronic underarousal contributes to a range of inattentive, underactive, and sleepy behaviors which are captured across the various rating scales assessing SCT, inattentive, and daytime sleepiness behaviors (Lecendreux et al., 2000; Miano et al., 2006). These possibilities have important theoretical and clinical implications. Indeed, daytime sleepiness has been found to predict academic impairment in ADHD samples above and beyond the influence of ADHD symptoms (Langberg, Dvorsky, Becker, & Molitor, 2014; Langberg et al., 2013). It is also important to acknowledge that the final regression model still only accounted for 33% of the variance in daytime sleepiness. As discussed in the “Future Research” section, this suggests that there are additional important predictors of daytime sleepiness yet to be identified. Overall, these findings suggest that the picture is complex, and that clinicians treating problems with daytime sleepiness will need to consider a wide variety of contributing factors including, but not limited to, specific sleep problems.
Limitations
The main limitation associated with this study is that the predictor analyses were cross-sectional. As such, it cannot be assumed that inattention and SCT cause daytime sleepiness or predict increases in daytime sleepiness over time, and similar to studies of sleep in general population samples (Kelly & El-Sheikh, 2014), these associations may be reciprocal. Indeed, the lack of longitudinal sleep research has been repeatedly noted as a limitation of the sleep literature as a whole (Cortese et al., 2009; Kelly & El-Sheikh, 2014; Shochat et al., 2014). In addition, although the prevalence cutoffs used for the PDSS and daytime sleepiness are well established, the cutoffs used for the CSHQ and SSR are less well established and were created to mirror prior sleep prevalence research (Fisher et al., 2014). As such, the prevalence rates for specific sleep problems found in this study need to be replicated with additional sleep measures to ensure that these rates generalize across measures and clinical cutoffs. Finally, this study relied solely on subjective, questionnaire measures to assess sleep. A stronger measurement approach would include multimethod assessment and objective measures of sleep.
Future Research
After considering a wide range of potential contributing factors, our regression models still only explained 33% of the variance in daytime sleepiness. Other potentially important factors to be considered in future research include technology (e.g., use of social media and gaming) and caffeine use and aspects of functional impairment such as homework problems. For instance, technology use at night—and technology multitasking in particular—is associated with adolescents reporting falling asleep in school (Calamaro, Mason, & Ratcliffe, 2009). In terms of functional impairment, Langberg, Dvorsky, Becker, and Molitor (2016) demonstrated that school maladjustment predicted daytime sleepiness in 62 university students with ADHD and found that locus of control mediated this association. This finding appears to be consistent with the hypothesis that adolescents with ADHD who regularly struggle in school (DuPaul & Langberg, 2014) may feel cognitively overwhelmed and mentally taxed, and that these feelings may lead adolescents with ADHD to report that they are fatigued and tired. To date, this possibility has not been explored. It would be interesting to investigate whether adolescents with ADHD report feeling sleepy and fatigued at all points during the day (e.g., morning, afternoon, and night), or if they only report these feelings when they are being cognitively taxed (e.g., in school).
An alternative possibility is that high rates of daytime sleepiness are driven by poor sleep, but that this will only be captured through daily measurement looking for “problematic nights” or intraindividual variability in sleep/wake patterns (Becker, Sidol, et al., 2017). A significantly higher percentage of youth with ADHD experience homework difficulties in comparison with typically developing youth (74% and 28%, respectively; Coghill et al., 2008). Importantly, parents report that most of these difficulties are concentrated during the late afternoon and evening hours leading up to bedtime (Coghill et al., 2008). Homework difficulties and conflict surrounding homework and studying may contribute to night-to-night variability in sleep functioning (e.g., bedtime, sleep onset delay) observed in youth with ADHD (Gruber & Sadeh, 2004; Gruber, Sadeh, & Raviv, 2000; Hvolby et al., 2008; Moreau et al., 2014). Research in community samples has demonstrated that a single instance of staying up late to study during the week can have a negative impact on functioning in school the next day (Gillen-O’Neel, Huynh, & Fuligni, 2013). Additional research is needed to determine whether factors such as homework problems and/or parent–adolescent conflict surrounding homework lead to problematic nights of sleep and daytime sleepiness in adolescents with ADHD.
Conclusion
This study included a large number of adolescents carefully diagnosed with ADHD and found that daytime sleepiness was far and away more prevalent than nighttime sleep problems, as rated by both parents and adolescents themselves. Of note, the only nighttime sleep variables associated with greater daytime sleepiness were time spent in bed and bedtime resistance behaviors (e.g., poor sleep habits, separation anxiety surrounding sleep). In considering various co-occurring symptoms as predictors of daytime sleepiness, problems with attention—including both ADHD inattentive and SCT symptoms—were most strongly associated daytime sleepiness. These findings point to complex interrelations between attention and daytime sleepiness and the need for more research investigating the contributors to daytime sleepiness in adolescents with and without attention problems.
Footnotes
Authors’ Note
The contents of this article do not necessarily represent the views of Institute of Education Sciences (IES) and do not imply endorsement by the federal government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant to the first author from the Institute of Education Sciences (IES; R305A130011).