
Abstract
Considerable neuropsychological heterogeneity in ADHD has been demonstrated over the past decade and current theoretical models emphasize multiple pathways in self-regulation processes leading to this disorder (Nigg, 2006; Nigg, Goldsmith, & Sachek, 2004). It has been shown that although ADHD has traditionally been conceptualized as a disorder of deficits in top-down cognitive control or executive function (EF; conscious goal-directed behavior), only a portion of children with ADHD is actually suffering from impaired EF (Nigg, Willcutt, Doyle, & Sonuga-Barke, 2005). Such findings beg the question of what other self-regulation processes may be important in the development of ADHD. Recently, emotion regulation has been put forward as key in relation to this disorder in several empirical studies (Forslund, Brocki, Bohlin, Granqvist, & Eninger, 2016; Martel, 2009; Musser, Galloway-Long, Frick, & Nigg, 2013; Shaw, Stringaris, Nigg, & Leibenluft, 2014; Sjowall, Roth, Lindqvist, & Thorell, 2013). However, there is as yet a shortage of longitudinal studies simultaneously examining emotion regulation and cognitive regulation (hot and cool) as potential predictors of developmental change in the two ADHD symptom domains spanning wide developmental periods.
Cognitive Self-Regulation
Top-down processing of information or EF with its multiple and partially independent cognitive functions (e.g., inhibition, working memory/updating and set-shifting, Miyake & Friedman, 2000) are central, but not limited to top-down cognitive self-regulation (Nigg, 2016). In attempts to clarify the ill-defined and broad EF construct, a functional distinction has been established between hot and cool aspects that lies on a continuum (Zelazo & Mueller, 2002). According to Zelazo and Mueller (2002), hot EFs refer to regulation of affective, arousing, and motivationally driven processes associated with ventral parts of the prefrontal cortex (PFC), whereas cool EFs involve abstract, decontextualized, and nonarousing problem solving associated with lateral parts of the PFC. Zelazo and Cunningham (2009) suggest that emotion regulation involves both hot and cool EF, but makes a distinction between when a problem to be solved in itself is that of regulating one’s emotions (i.e., emotion regulation) and when the regulating of emotions occurs as a means of achieving another goal (i.e., hot EF).
Deficits in cool EF make up one important neuropsychological pathway contributing to ADHD symptoms in at least a portion of children with this disorder (Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). Cool inhibition has indeed been shown to be an early predictor of longitudinal ADHD symptoms, and specifically of inattention symptoms, at least across shorter time periods (Berlin, Bohlin, & Rydell, 2003; Brocki, Eninger, Thorell, & Bohlin, 2010; Brocki, Nyberg, Thorell, & Bohlin, 2007; Chhabildas, Pennington, & Willcutt, 2001).
In comparison with the cool aspects of EF, hot EF has not been as widely researched in relation to ADHD symptoms. To date findings are conflicting as to whether hot EF deficits are associated with ADHD independently of antisocial behavior such as ODD/Conduct Disorder (CD), particularly over time. The contrasting results between the existing studies on hot EF and ADHD could be due to variations in tasks (e.g., gambling tasks, delay aversion tasks, and frustration tasks), and level of analyses (i.e., dimensional vs. group differences) with and without control for comorbid symptoms. Furthermore, there are no previous studies on the predictive effect of preschool hot EF on adolescent ADHD symptoms, and whether hot and cool EFs are differentially predictive of change in the two ADHD symptom domains over extended periods of time. It also remains unclear whether hot EF is distinct from top-down regulation of emotion in relation to ADHD (Nigg, 2016). Interestingly, the same brain regions have been theorized as implicated in hot EF and emotion regulation (Martel, 2009) and a recent summary of brain-imaging evidence supports this proposition (Petrovic & Castellanos, 2016).
Emotion regulation
Findings from several recent studies support the long-standing theoretical perspective of poor emotion regulation as an important associated feature of ADHD (Karalunas et al., 2014; Maedgen & Carlson, 2000; Musser et al., 2013; Walcott & Landau, 2004). Importantly, poor emotion regulation skills have been demonstrated to be associated with ADHD symptoms independently of impairments in cool aspects of EF, perhaps constituting a separate self-regulatory pathway to the disorder (Forslund et al., 2016; Nigg et al., 2004; Sjowall et al., 2013). Of late, biological evidence for a role of an emotion regulatory deficit underlying the heterogeneity in ADHD was demonstrated in terms of a deviant parasympathetic mechanism during an emotion regulation task (Musser et al., 2011; Musser et al., 2013), results which were not explained by comorbid conduct problems. Although recent behavioral findings (Sjowall, Backman, & Thorell, 2015) coincide with Musser and colleagues’ (2013) conclusion, there are also studies suggesting the opposite (Maedgen & Carlson, 2000; Melnick & Hinshaw, 2000).
Moreover, there is support for particular emotions and their respective regulation to be differentially important for externalizing behavior problems (Martel et al., 2009; Nigg et al., 2004). Regulation of intense positive emotionality, which is associated with high approach tendencies and impulsivity, has been found important in relation to externalizing behavior problems (Nigg et al., 2004; Rydell, Berlin, & Bohlin, 2003; Rydell, Thorell, & Bohlin, 2007; Stifter, Putnam, & Jahromi, 2008) and as a specific risk factor for ADHD (Martel, 2009; Musser et al., 2013; Nigg et al., 2004). Importantly, this type of positive emotionality/exuberance does not refer to happiness or joy in general, but rather to high temperamental approach tendencies and unrestrained excitement. Rydell et al. (2003) speculate that the distinction between adaptive and problematic positive emotionality rests in the child’s capacity to regulate his or her emotions to achieve social acceptance.
Emotion regulation can be understood as composed of two related and interactive developmental processes: emotional reactivity and regulation. Although there is a discussion about the extent to which emotional reactivity and emotion regulation are separable, research supports considering them as dissociable constructs at the empirical level (Cole, Martin, & Dennis, 2004; Martel et al., 2009). It has been suggested that while high negative emotionality or reactivity may be linked to disruptive disorders in general, possibly accounting for their comorbidity, a deficiency in emotion regulation may be specific for ADHD (Martel, 2009). Thus, studying emotion regulation without accounting for individual differences in emotional reactivity might mask a specific link between the regulation-related process and ADHD.
Developmental Change in ADHD Symptoms
It has been demonstrated, although by relatively few studies, that the manifestations of ADHD symptoms change with age. Typically, levels of hyperactivity and impulsivity decline with development, whereas difficulties with inattention remain more stable over time (Hart, Lahey, Loeber, Applegate, & Frick, 1995; Molina et al., 2009; Willoughby, 2003). Despite this knowledge, very few studies have so far investigated symptom change in relation to early self-regulatory skills, which of course is particularly true for studies simultaneously examining different aspects of self-regulation in relation to ADHD-symptoms across long time periods.
Aim
The aim of this study was to examine individual differences in emotion regulation and hot and cool EF as prospective predictors of developmental change in the two ADHD symptom domains between preschool and adolescence, emphasizing independent and predictive effects. Accordingly, we first examined change in levels of hyperactivity/impulsivity and inattention symptoms from 5 to 13 years. Second, we examined possible independent and interactive effects between the three distinct self-regulatory measures and time on change in each of the ADHD symptom domains. Based on the developmental perspective on ADHD and previous empirical studies (Hart et al., 1995; Molina et al., 2009; Willoughby, 2003), we first hypothesized that levels of hyperactivity/impulsivity symptoms would decrease significantly between preschool and adolescence, whereas symptoms of inattention would remain more stable. Consistent with recent empirical findings (Forslund et al., 2016; Sjowall, Backman, & Thorell, 2015), we further hypothesized that the three self-regulatory processes would form independent contributions to change in ADHD symptoms over time, with poorer self-regulation skills at 5 years contributing to higher levels of ADHD symptoms at 13 years relative to those with good self-regulation in preschool. Due to the scarcity of empirical findings on self-regulatory ability as prospective predictors of developmental change in symptoms, we made no a priori hypotheses in terms of specificity in the relations between the distinct self-regulation measures and each of the two ADHD symptom domains. In terms of regulation deficits in specific emotions, we hypothesized that particularly poor regulation of positive emotionality in preschool would be associated with a change in ADHD symptoms in the negative direction compared with those with good regulation of positive affect in preschool. If true, this would support recent studies showing behavioral evidence for disrupted processing of positive emotions in ADHD (Forslund et al., 2016; Musser et al., 2011; Musser et al., 2013; Sjowall et al., 2013).
Method
The study was approved by the Regional Ethical Review Board, Uppsala. 2013/241, and informed consent was collected from all participating children and their parents according to the declaration of Helsinki.
Participants and Procedures
The sample has previously been described by (Brocki et al., 2007). A total of 72 children (60 boys and 12 girls) entered the longitudinal study. To obtain a sample of children scoring across the full range of ADHD symptom severity, we recruited one third of the children from local Child Health Care Centers. These children had been identified as being at risk for developing a disruptive disorder (i.e., ADHD and/or ODD) based on clinical assessment by trained psychologists specialized in screening children for developmental disorders. The remaining sample consisted of a group of typically developing children chosen to be proportionally matched in terms of sex and age. These children were randomly selected and recruited through the local birth register of Uppsala County, Sweden. No children in the study were at the time of testing receiving psychostimulant medication for ADHD. Parental educational status was high, with 59% of the mothers and 44% of the fathers having a university degree. The majority of parents were Swedish in origin (mothers 94% and fathers 86%), and the majority of children (90%) lived with both parents at T1. Furthermore, 21% of the children were initially rated by parents and teachers as having levels of ADHD symptoms that was considered as being “at-risk.” This means that these children were rated as having at least a score of 2 (i.e., often occurring symptoms) on six symptoms of either hyperactivity/impulsivity or inattention (see Table 2 for descriptive data on ADHD symptoms at T1 and T2). At follow up (T2), 20% of the children remaining in the study were reported by the parents to have received an ADHD diagnosis and 70% out of the diagnosed children had either received or were receiving some sort of behavioral or medical intervention.
At T1 (M = 5 years, 5 months; SD = .68), the children were tested individually at the Department of Psychology, Uppsala University. The tasks being analyzed in the current article were part of a larger battery designed to tap various EFs. To control for possible fatigue effects, the tasks were administered during two sessions over a period of 1 to 2 weeks. The tasks within each session were administered in a randomized order. Each session lasted approximately 1 hr with a break half-way through. At the end of each session, the children received a gift worth approximately €10. At T1, questionnaire data from the children’s parents and teachers were collected for 72 and 68 of the children, respectively. Participant attrition was due to lack of parental consent to contact the teacher (N = 1) and an unwillingness to complete the questionnaire by the teacher (N = 3).
At T2 (M = 13 years, 5 months; SD = .82), 63 children remained in the study (longitudinal gap M = 8 years, 0 months, SD = .73). At T2, the data collection consisted of parents and teachers completing questionnaires for 63 and 47 of the children, respectively. Participant attrition was due to that families no longer wished to participate in the study (N = 9) and lack of parental consent to contact the teacher (N = 5), and an unwillingness to complete the questionnaire by the teacher (N = 11).
Measures
Cool inhibition
At T1, a computerized go/no task was used to test the child’s ability to inhibit a prepotent response. This task consisted of a blue square, a blue triangle, a red square, and a red triangle presented one at a time on a computer screen. During the first part of the task, the children were instructed to press a key (“go”) when a frequent stimulus (a blue figure) appeared on the screen, but to make no response (“no-go”) when an infrequent stimulus (a red figure) appeared. The second part of the task used the same stimuli, but children pressed a key every time they saw a square, and inhibited their response every time they saw a triangle, irrespective of color. Altogether the task included 60 stimuli with a “go-rate” of 77%, and thus prepotency within the task was provided by the majority of the stimuli being “go-targets” (see Berlin & Bohlin, 2002, p. 245, for more detailed information). The score derived from the task was total number of commission errors (pressing the key when a “no-go” target was presented). A test–retest reliability of .62 for this task over a 2-week period has been reported by Thorell (2007).
Hot inhibition
An observational measure based on Kochanska’s cheating paradigm (Kochanska, Murray, Jacques, Koenig, & Vandegeest, 1996) was used to measure hot inhibition at T1. This task consisted of a wooden puzzle containing 11 familiar shapes (e.g., star, oval, square, and circle), and a puzzle frame placed underneath a cardboard box with one side open and a cloth covering the front. The cloth could easily be lifted up so that the child could look at the puzzle. The children were told to try to get as many pieces into the correct places in the puzzle during 3 min, without peeking under the cloth at the puzzle and that the experimenter would count the pieces when the time was up. The experimenter then made an excuse to leave and left the room. The camera was left running during the entire visit so as to make it as inconspicuous as possible. The child’s motivation to cheat was enhanced by the desire to show the experimenter that they were able to complete the puzzle and that they were told that they would receive a reward for doing a good job at the end. Poor rule-governed behavior was assessed from the videotape using a scale from 1 (no instances of cheating, behavior fully rule-governed) to 5 (many instances of cheating/flagrant cheating, very low rule-governed behavior). Interrater reliability was r = .80 using the ratings from all children who had data on this task (N = 66) made by two independent observers.
Emotion regulation
At T1, the children’s parents completed the Emotion Questionnaire (Rydell et al., 2003), in which emotionality and the regulation thereof are rated separately. Thus, this measure relied on the parent’s interpretation of the child’s behavior assuming internal representation of the parent’s experience with the child in relevant situations. The Emotion Questionnaire assesses emotion regulation by asking questions about the child’s capacity to regulate anger, fear, sadness (i.e., negative emotion), and happiness/exuberance (i.e., positive emotion), with and without the assistance of others. One general question is asked for each emotion (e.g., if angry, my child has trouble calming down by him or herself; it is easy for others, for instance a parent, to calm him or her down or if happy and excited, my child has difficulties quieting down on his or her own; it is easy for others, for instance a parent to make him or her quiet down) and two questions regarding self-regulation as well as regulation with the help from others in specific situations (e.g., if my child gets in conflict with a peer, he or she has difficulties calming down on his or her own; it is easy for others, for instance a parent, to make him or her feel better, if my child wins a game or a contest, he or she has difficulties quieting down on his or her own; it is easy for others, for instance a parent to make him or her quiet down). For emotionality, questions are composed to assess the frequency and intensity of reaction for each of the four emotions described above (e.g., my child often becomes sad; he or she reacts strongly and intensely or my child often becomes happy or excited and in an exuberant mood; he or she reacts strongly). Each question is scored on a scale ranging from 1 (doesn’t apply at all) to 5 (applies very well to my/this child), with higher values indicating greater problems with emotion regulation and emotionality. This measure has been reported to have high test–retest reliability and high construct validity (Rydell et al., 2003). Cronbach’s alpha for emotion regulation was .93 and for emotionality .87. In the present study, the emotionality index was used as a control variable to statistically separate regulatory processes from emotionality in relation to ADHD symptoms (see “Statistical Analyses” section).
ADHD and ODD symptoms
At T1 and T2, parents and teachers completed a questionnaire containing items from the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) criteria for ADHD. This measure has been well validated and is frequently used within ADHD research (e.g.,DuPaul, Power, Anastopoulos, & Reid, 1998). Nine items are composed to assess inattention, six items are composed to measure hyperactivity, and three items are composed to assess impulsivity. In addition, at T1, parents and teachers also rated symptoms of ODD, measured using eight items from the DSM-IV criteria (APA, 1994). Each item on the ADHD and ODD scales was scored on a 4-point scale ranging from 0 (never/seldom occurring) to 3 (very frequently occurring). Internal consistency was high with regard to parent and teacher ratings of ADHD with alpha coefficients ranging from .94 to .96. The questions in the ADHD scales were phrased to represent the child’s current behavior. Correlations between parent and teacher ratings for ADHD symptoms at T1 was .87, p < .0001, at T2 .70, p < .0001, and for ODD at T1 .33, p < .01. The mean score across parent and teacher ratings for the separate symptom domains of hyperactivity/impulsivity and inattention were used in the analyses at T1 and T2, as well as for symptoms of ODD at T1. In this study, the ODD index was primarily used as a control variable to statistically control for the overlap between ODD and ADHD at T1.
Statistical Analyses
Data were screened for extreme values, and data points that met criteria for > 3 SD were defined as outliers. We found three outliers for cool inhibition and one for emotion regulation and replaced them with the value next most extreme (Tabachnick & Fidell, 2013). As some of the performance variables and ratings of ADHD and ODD symptoms were skewed (skewness ranging from .03 to 2.89, kurtosis from .20 to 3.21), logarithmic transformations were conducted. Analyses with these more adequately distributed variables did not change the level of significance in any of the analyses. For ease of interpretation, all results presented below are based on raw scores. We calculated a standardized residual for total emotion regulation by partialling out emotional reactivity in line with the proposed importance of isolating the effect of regulation from reactivity (Cole et al., 2004; Rydell et al., 2003). The residuals were calculated in separate regression analyses, with the total emotion regulation measure as outcome variable and the emotionality measure as the predictor. Similarly, for analysis of regulation of the four distinct emotions, a standardized residual was created for each of the separate emotions in separate analyses, with the distinct emotion regulation variables as outcomes and emotionality-matching variables as predictors. To account for comorbidity, symptoms of ODD at T1, which were significantly related to all of the predictors and outcome variables (r = .26 –.80), were controlled for in the analyses specified below.
First, Pearson’s correlations were conducted to examine bivariate relations between T1 and T2. Then, two repeated-measures ANOVAs were performed, with time as independent variable (T1 and T2) and symptoms of inattention and hyperactivity as dependent variables, respectively. To evaluate the independent effects of the three self-regulatory processes on developmental change in in the two symptom domains between T1 and T2, two ANCOVAs were performed with the three self-regulatory processes (cool inhibition, hot inhibition, and emotion regulation) as covariates. Finally, early symptoms of ODD were added as covariate in the analyses. As neither sex nor social background (indexed by a mean value of the mother’s and father’s highest educational level) influenced the patterns of significance for any of the analyses, we did not control for these variables in the final analyses. Independent samples t tests showed that there were no significant differences in any of the study variables at T1 for those children who did not remain in the study at T2 (all ps > .05).
Results
Correlations within and between the self-regulation variables and ADHD symptoms are shown in Table 1. Cool inhibition significantly related to hot inhibition, but no other association was found between the self-regulation variables at T1. Furthermore, cool inhibition, hot inhibition, and emotion regulation were related to at least one of the ADHD symptom domains at T1 and T2. Poorer self-regulation in general was associated with higher levels of ADHD symptoms both concurrently and longitudinally.
Correlations Within and Between the Self-Regulation Measures and ADHD Symptoms at T1 and T2.
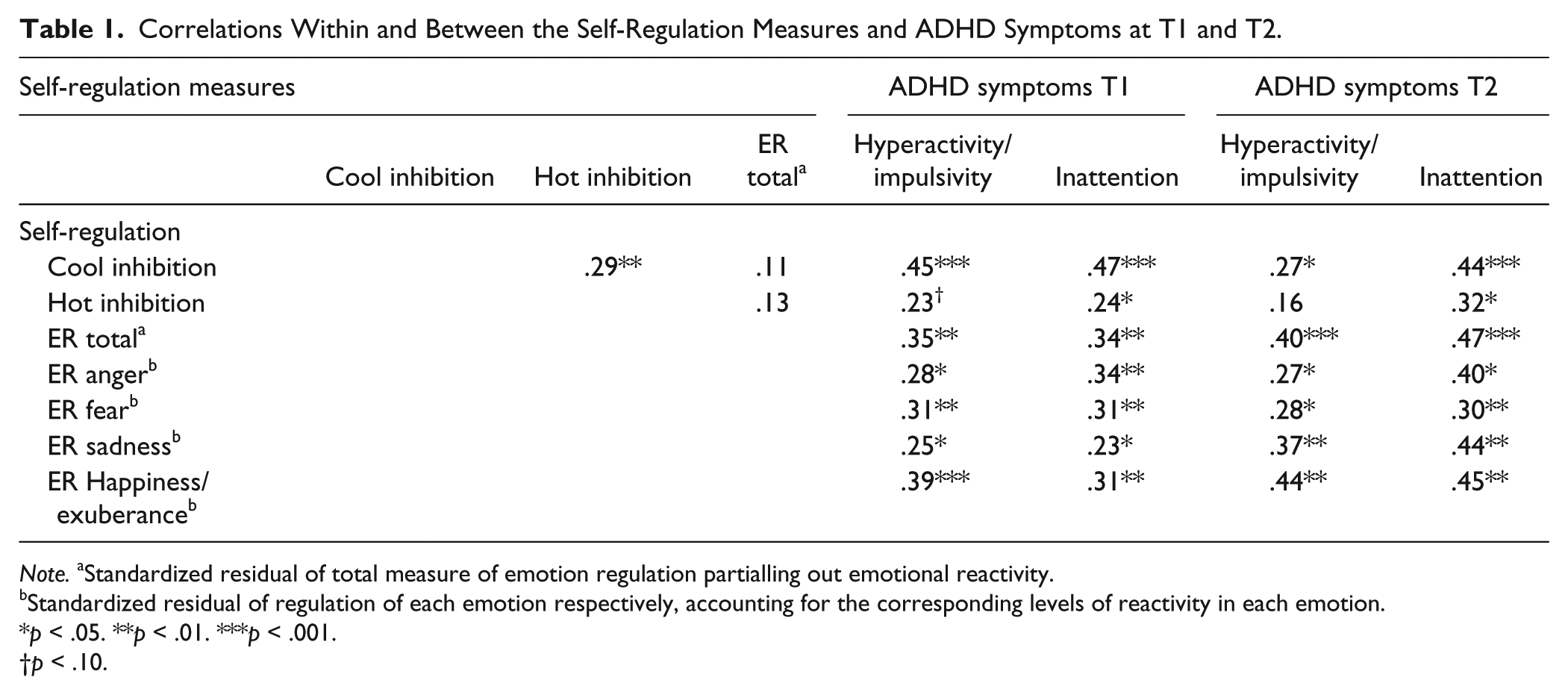
Note. aStandardized residual of total measure of emotion regulation partialling out emotional reactivity.
Standardized residual of regulation of each emotion respectively, accounting for the corresponding levels of reactivity in each emotion.
p < .05. **p < .01. ***p < .001.
p < .10.
Results from the repeated measures ANCOVAs are presented in Table 2. There was a highly significant effect of time on hyperactivity/impulsivity, with symptom levels decreasing between T1 and T2. There was also a significant interaction between time and cool inhibition indicating a steeper decrease of symptoms over time for children who displayed poor as compared to good cool inhibition at preschool age. As seen in Figure 1, the reason for the more pronounced decrease is the higher initial level of hyperactivity/impulsivity for children with poor cool inhibition. This interaction effect remained with control for early symptoms of ODD. No interaction effects were observed for symptoms of hyperactivity/impulsivity and emotion regulation or hot inhibition.
Means, Standard Deviations, and Results From the Repeated-Measures ANCOVAs, Controlling for Early ODD Symptoms.
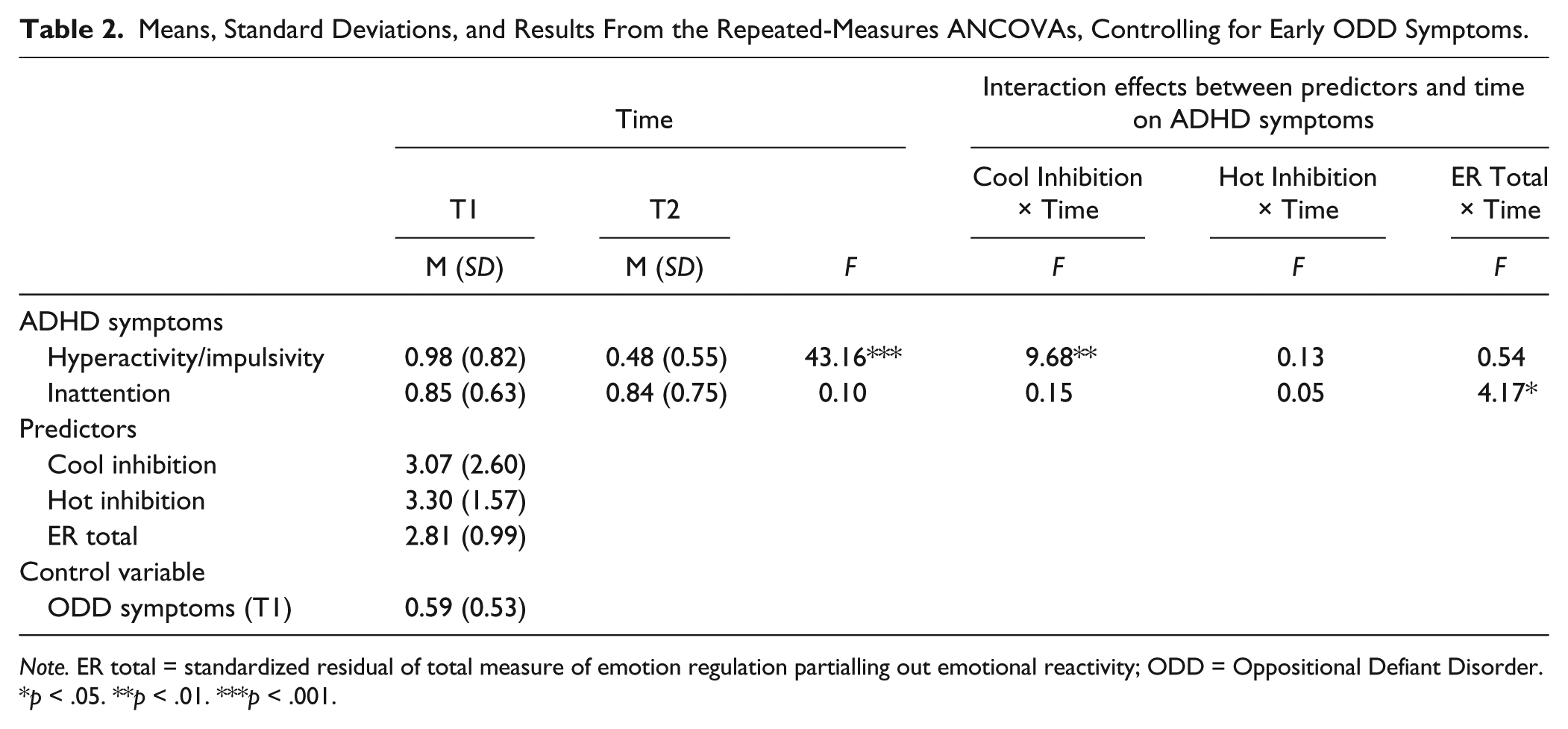
Note. ER total = standardized residual of total measure of emotion regulation partialling out emotional reactivity; ODD = Oppositional Defiant Disorder.
p < .05. **p < .01. ***p < .001.
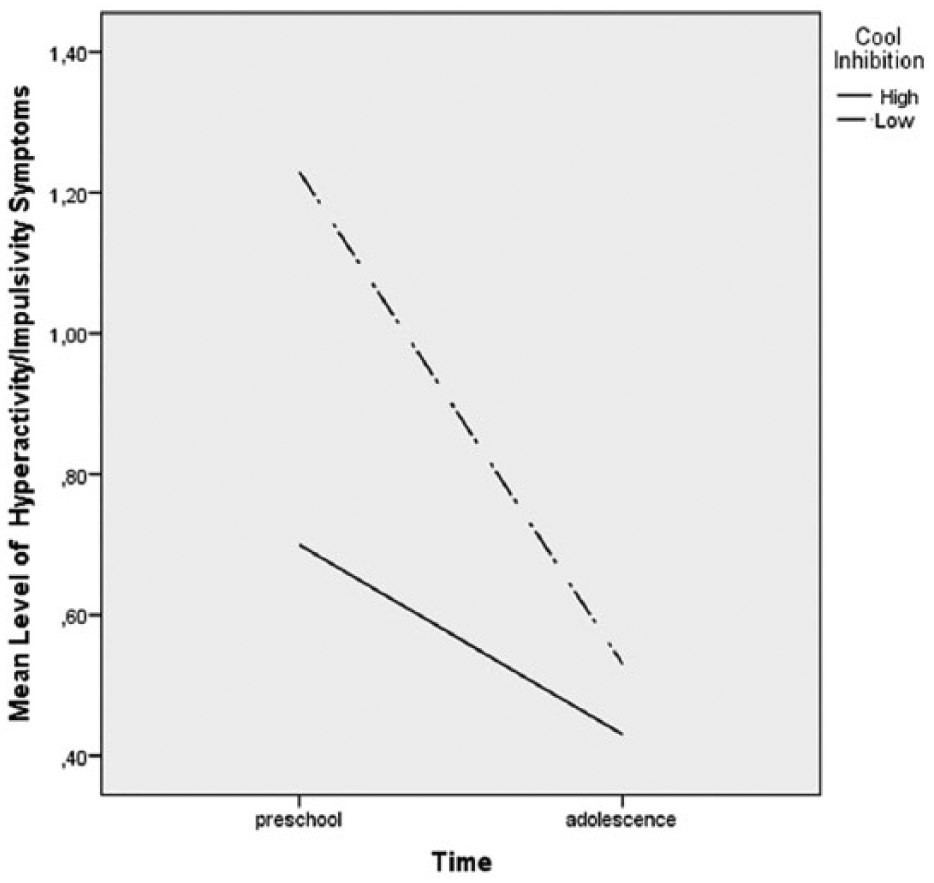
Interaction effect between time and level of cool inhibition on mean level of hyperactivity/impulsivity symptoms across time.
There was no effect of time on inattention symptoms, indicating that levels of inattention remained stable between T1 and T2 for the group as a whole. However, there were individual differences in the development of inattention symptoms as indicated by a significant interaction between time and emotion dysregulation, indicating that the change over time went in the opposite directions for children with good and poor emotion regulation. As seen in Figure 2, children with better emotion regulation at T1 showed a slight decrease in inattention symptoms from T1 to T2, whereas those with poorer emotion regulation at T1 increased slightly between the two time points. This interaction effect remained with control for early symptoms of ODD.
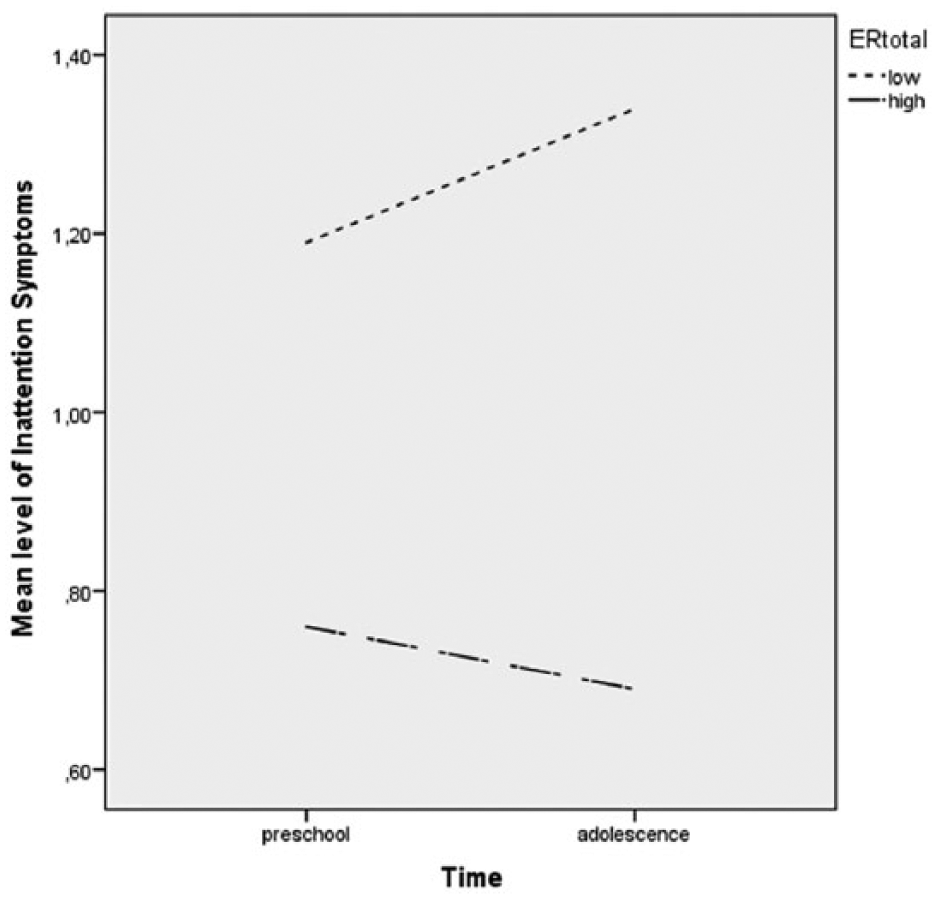
Interaction effect between time and level of emotion regulation on mean level of inattention symptoms across time.
We further examined whether regulation of specific emotions related differently to change in longitudinal symptoms of inattention. Using the standardized residuals for regulation of the specific emotions (anger, fear, sadness, and happiness/exuberance), the ANCOVA was repeated, again with time (T1 and T2) and the regulation of the specific emotions as independent variables and inattention symptoms as dependent variable, controlling for early symptoms of ODD. The results showed an interaction between time and regulation of happiness/exuberance, F = 5.90, p = .018, whereas the interaction terms between the other emotions and time were nonsignificant (aggression, F = 0.24, p = .62; sadness, F = 0.99, p = .32; fear, F = 0.47, p = .50), indicating that the previously obtained effect of total emotion dysregulation on change in symptoms of inattention over time was specific for regulation of positive emotion.
Finally, to confirm that the unique interaction effect between time and dysregulation of positive emotions on symptoms of inattention was not due to shared variance between parent ratings of emotion regulation and ADHD symptoms, a similar repeated-measures ANCOVA was conducted using only the teacher ratings of inattention symptoms as dependent variable and parent ratings of regulation of happiness/exuberance and time as independent variables. The results showed that the previously obtained interaction effect between time and regulation of happiness/exuberance on change in symptoms of inattention remained (F = 10.33, p < .01), indicating that this relation was robust and not due to a reporter effect.
Discussion
Driven by the need to further the knowledge on the contribution of individual differences in distinct aspects of self-regulation as prospective predictors of developmental change in ADHD symptoms, this study examined independent effects of emotion regulation and hot and cool EF in preschool on change in the two ADHD symptom domains from preschool to adolescence. As hypothesized, results showed that levels of hyperactivity/impulsivity symptoms decreased significantly between 5 and 13 years of age, whereas symptoms of inattention remained more stable for the group as a whole. More important, however, were the findings indicating converging developmental paths across time in levels of hyperactivity/impulsivity for those with high versus low inhibitory control, whereas diverging paths in inattention symptoms was observed for those with high versus low emotion regulation.
Effects of Cool and Hot Inhibition on Developmental Change in ADHD Symptoms
We hypothesized that those with poor self-regulation in preschool would show relatively higher levels of ADHD symptoms in adolescence in comparison with those with good self-regulation skills. Although the levels of hyperactivity/impulsivity were higher in adolescence for children with poor cool inhibition as shown in the correlational data, the interactive effect did not support the prediction of a developmental lag in the expected decrease of symptoms. The result appeared somewhat counterintuitive in that the poor inhibitors showed a steeper decline in hyperactivity/impulsivity across time compared with the good inhibitors. Importantly, the reason for this larger symptom decline was that the poor inhibitors started off with significantly higher levels of hyperactivity/impulsivity in preschool. Thus, it appears that poor cool inhibition is primarily important for increased levels of hyperactivity/impulsivity in the preschool age. And although these children continue to show a high symptom level during the school years (Hart et al., 1995; Molina et al., 2009; Willoughby, 2003), they are catching up somewhat with the good inhibitors in hyperactivity/impulsivity in adolescence.
The results for hyperactivity/impulsivity are in line with previous studies demonstrating poor preschool inhibition in the cool domain to be an important associate of later ADHD symptoms (Berlin & Bohlin, 2002; Bohlin, Eninger, Brocki, & Thorell, 2012; Brocki et al., 2010). Importantly, however, this study adds to these findings in significant ways. First, our results indicated that lower levels of cool inhibition in preschool over time become a less important predictor of higher levels of hyperactivity/impulsivity, whereas its relation to levels of inattention symptoms is more stable as demonstrated in the correlational data. Second, the longitudinal relations between hot inhibition and symptoms of inattention (and the marginal significant relation with hyperactivity/impulsivity) disappeared when controlling for cool inhibition. This finding suggests that it was the variance shared with cool inhibition that was captured in the association between hot inhibition and ADHD symptoms. This result is in line with Zelazo and Mueller’s (2002) theoretical proposition that ADHD is viewed primarily as a disorder of cool EF, with hot EF being relatively, but not completely intact. Furthermore, our hot EF task involves compliance and resisting norm breaking behavior. This type of oppositional behavioral problems may well be a part of, although not limited to, the manifestation of ADHD. As there is no clear consensus on the definition of hot EF, variations in operationalizing this process may well have contributed to differences in results. Future longitudinal studies with a focus on hot EF in relation to disruptive behaviors specific for ADHD and ODD/CD, preferably comparing various existing “hot” EF tasks in different age groups, are needed to establish a clear definition of hot EF and its contribution to these disorders.
Effects of Emotion Regulation on Developmental Change in ADHD Symptoms
Early individual differences in emotion regulation predicted ADHD symptoms across time in that those with poor preschool emotion regulation not only had higher levels of inattention at both time points as can be seen in the correlational data, but they also showed a slight increase in inattention symptoms over time, whereas those with good emotion regulation showed a decrease in inattention symptoms. This result adds to recent cross-sectional reports emphasizing emotional functioning as an important associated feature of ADHD (Sjowall, Backman, & Thorell, 2015). Our result also extends recent longitudinal findings (Sjowall, Bohlin, Rydell, & Thorell, 2015) that demonstrated a predictive relation between preschool emotion regulation and symptoms of inattention in adolescence by showing that poor emotion regulation actually may indicate a risk for increased levels of inattention across childhood over time. Our results also corroborate recently reported biological evidence of disrupted emotional processing in relation to ADHD in middle childhood (Karalunas et al., 2014; Musser et al., 2011; Musser et al., 2013).
Interestingly, further analysis on the regulation of separate emotions revealed that, although there were bivariate longitudinal relations between all of the emotions (anger, fear, sadness, and happiness/exuberance) and ADHD symptoms (see Table 1), it was poor regulation of positive emotion (i.e., happiness/exuberance), that independently explained the longitudinal effect of the total measure of emotion regulation on the relative increase in inattention symptoms across time. At a behavioral level, this type of poor regulation of positive emotionality can be observed in situations in which excessive levels of excitement are not appropriate (e.g., happiness over one’s own winning and a friend’s losing in games or in failure to dampen play activities involving high laughter and shouting even when asked to do so by and adult). This finding supports proposals of a temperamental pathway to ADHD symptoms through unrestrained positive approach tendencies and difficulties regulating such emotions (Karalunas et al., 2014), proposed to be independent of deficits in executive functioning (Nigg et al., 2004; Sjowall et al., 2013). This finding is also in line with previous research using the same rating scale for emotion regulation reporting poor regulation of positive emotion in relation to externalizing behavior problems (Rydell et al., 2003) and in relation to ADHD symptoms (Forslund et al., 2016) in nonclinical samples and between regulation of positive emotion and ADHD in a clinical sample.
A key question concerns the actual mechanism involved in the dysregulation of positive emotion that drives the developmental progression of symptoms of inattention. The recent biological evidence published by Musser and colleagues (Musser et al., 2011; Musser et al., 2013) suggests abnormal parasympathetic mechanisms contributing to emotion regulation deficits, and specifically, regulation of positive emotion in childhood ADHD. It is possible that a biologically based difficulty in modulating strong positive affect leads to a series of additive social adversities propelling the child from one step to the next along a specific pathway in the progression of ADHD symptoms. Thus, the importance of emotion dysregulation as an early risk marker for ADHD may allow for new intervention methods with a focus on teaching children with ADHD regulatory skills to manage extreme levels of emotionality and elevated approach tendencies. Indeed, aspects of early family environment and parenting as significant contributing factors in the development of cognitive self-regulation have been emphasized in recent research (Bernier, Carlson, & Whipple, 2010; Bibok, Carpendale, & Muller, 2009).
The finding that dysregulation of negative emotionality, particularly anger, did not contribute to change in ADHD symptoms across time may seem counterintuitive given consistent reports of dysregulation of negative emotion in ADHD (Shaw et al., 2014). However, the aim of the present study was examination of specificity in relation to ADHD symptoms, and we therefore controlled for comorbid ODD symptoms, which are also strongly associated with dysregulation of negative emotionality. Indeed, the present findings give support to theoretical propositions (Martel & Nigg, 2006; Martel et al., 2009), and extend recent empirical findings (Forslund et al., 2016; Sjowall et al., 2013), suggesting that dysregulation of negative emotionality in ADHD may depend on the presence of comorbid ODD symptoms, whereas dysregulation of positive emotionality may constitute a specific risk factor for ADHD symptoms. It is, however, important to remember that ADHD symptoms and ODD symptoms are highly comorbid (Nock, Kazdin, Hiripi, & Kessler, 2007; Waschbusch, 2002), and dysregulation of negative emotion is therefore an important and common associated feature in children and adolescents high in ADHD symptoms.
A possible limitation in the current study was the use of parental ratings of emotion regulation, instead of using objective tasks similarly to the hot and cool EF measures. Using partly the same informants for the predictor and outcome measure involves a possible risk of inflated relations. However, to confirm that the predictive effect of poor regulation of positive emotion on inattention symptoms across time was not due to shared source variance, we conducted an analysis using parental ratings for emotion regulation and teacher ratings only for ADHD symptoms and the conclusion did not change. This means that the unique predictive relation between poor regulation of positive emotion and adolescent ADHD symptoms is robust and not a result of a reporter effect.
Conclusion
This longitudinal study extends the understanding of distinct aspects of self-regulation processes as prospective predictors of ADHD symptoms from preschool to adolescence. Most importantly, our findings demonstrate that poor emotion regulation, and particularly poor regulation of positive emotion is predictive of an increase in symptoms of inattention across time, whereas good emotion regulation is indicative of a decrease of inattention symptoms. Thus, poor emotion regulation may be seen as a risk for increased levels of inattention problems with development. Further, different courses of development for hyperactivity/impulsivity was observed for those with high versus low cool inhibition, with poor inhibitors showing a steep decrease in symptom level over time due to significantly higher levels in preschool compared with the good inhibitors. Our findings indicate that distinct aspects of self-regulation may underlie developmental change in levels of the two ADHD symptom domains from preschool to adolescence. These findings emphasize the importance of distinguishing between cognitive and affective self-regulation in relation to ADHD symptoms over time and point to self-regulation as a potential target for early screening and intervention hindering increased functional impairment in individuals with ADHD over time. It is our hope that the current findings will motivate future longitudinal studies into the specific mechanisms and processes responsible for propelling a child from one step to the next along the self-regulation pathways to ADHD.
Footnotes
Appendix
Descriptive Data for Interaction Effects Between Level of Cool Inhibition × Time (A) and Emotion Regulation Total × Time (B), Respectively Illustrated in Figures 1 and 2.

| A | Hyperactivity/impulsivity | |
|---|---|---|
| Cool inhibition | Preschool |
Adolescence |
| M (SD) | M (SD) | |
| High inhibition | 1.23 (0.94) | 0.43 (0.51) |
| Low inhibition | 0.70 (0.56) | 0.53 (0.59) |
| B | Inattention | |
| Emotion regulation (ER) total | Preschool |
Adolescence |
| M (SD) | M (SD) | |
| High ER | 0.76 (0.59) | 0.69 (0.70) |
| Low ER | 1.19 (0.74) | 1.34 (0.69) |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Jerringfonden (UU PSYK 2013/265) to Karin C. Brocki.