
Abstract
Introduction
ADHD is characterized by symptoms of listlessness, disorganization, and/or hyperactivity/impulsiveness (American Psychiatry Association, 2013; Thapar & Cooper, 2016). The prevalence in adult individuals is 2.5% to 4.4% (Kessler et al., 2006; Simon, Czobor, Bálint, Mészáros, & Bitter, 2009), with the combined subtype of the disorder being the most commonly diagnosed (56%-62%), followed by the predominantly inattentive subtype (31%-37%) and hyperactive/impulsive (2%-7%) (Millstein, Wilens, Biederman, & Spencer, 1997; Wilens et al., 2009).
The currently worldwide available pharmacological treatments are psychostimulants (methylphenidate, dexmethylphenidate, lisdexamfetamine, amphetamine salts, dexamphetamine), noncerebral stimulants (atomoxetine), and antidepressants (bavisant, modafinil, armodafinil, metadoxine, dasotroline, desipramine, and mecamylamine) (Adler et al., 2013; Amiri, Farhang, Ghoreishizadeh, Malek, & Mohammadzadeh, 2012; Arnold, Feifel, Earl, Yang, & Adler, 2014; Butterfield, Saal, Young, & Young, 2016; Hamedi et al., 2014; Koblan et al., 2015; Loland et al., 2012; Manor et al., 2012; Palumbo et al., 2008; Paterson, Douglas, Hallmayer, Hagan, & Krupenia, 1999; Potter, Ryan, & Newhouse, 2009; Riahi, Tehrani-Doost, Shahrivar, & Alaghband-Rad, 2010; Spencer et al., 2007; Spencer, Adler, Weisler, & Youcha, 2008; Takahashi et al., 2014; Weisler, Pandina, Daly, Cooper, & Gassmann-Mayer, 2012; Wilens et al., 1996; Young, Sarkis, Qiao, & Wietecha, 2011). A review of guidelines based on evidence for the pharmacological treatment of ADHD in children, adolescents, and adults considers psychostimulants such as methylphenidate and amphetamines to be the first-choice strategies, followed by atomoxetine as a second-line treatment. The other drugs are reported only as off-label usage. However, some adverse effects such as loss of appetite, abdominal pain, headaches, and sleep disorders are strongly related to cerebral stimulants. Other symptoms such as sleepiness, gastrointestinal disorders, diminished appetite, increase of suicidal thoughts, and hepatitis are associated with the use of atomoxetine (Canadian Agency for Drugs and Technologies in Health, 2016; Canadian Attention Deficit Hyperactivitiy Disorder Resource Alliance, 2011; Gibson, Bettinger, Patel, & Crismon, 2006). In this context, considering that ADHD is a chronic disease that tends to remain in 65% of adult patients after being diagnosed in childhood (Dulcan & Benson, 1997), the increased consumption and exposition to drugs may reflect safety issues and patient’s tolerability and should be carefully analyzed.
To select adequate treatments, health professional’s decisions should be based on strong and quality evidences of interventions. Systematic reviews and statistical elements (meta-analyses) of randomized controlled trials (RCTs) represent the top of the evidence-based practice and may be helpful when collecting information about a participant (Evans, 2003; Sampaio & Mancini, 2007). Meta-analyses may be performed in a conventional way (pairwise comparison between two treatments), or through the combination of direct and indirect evidence of all treatment arms of studies in a multiple treatment comparisons path; this is also called mixed treatment comparison (MTC) or network meta-analyses (Jansen, Crawford, Bergman, & Stam, 2008; Jansen & Naci, 2013). MTC allows the comparison of more than two interventions, even when these are not directly compared in the literature, providing an overview of all available information over a topic in the same model.
A single meta-analysis about ADHD treatment in adults has been published so far. However, the authors evaluated some outcomes of efficacy and tolerability for only two drugs, atomoxetine and methylphenidate extended release (OROS MPH) (Bushe et al., 2016), which does not allow the safety profiles for the available treatments to be adequately summarized. Besides that, there are just a few direct comparisons (head-to-head) of ADHD drugs in RCTs with adult patients which may prevent further conclusions from being drawn. Thus, the objective of this study was to synthesize evidence comparing the safety profile of any available drug used to treat ADHD in adult patients with no associated comorbidities.
Method
The systematic review was designed according to the recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Cochrane Handbook for Systematic Reviews of Interventions (Higgins & Green, 2011). All steps were followed by two independent reviewers with a third author to resolve discrepancies during the consensus.
Strategic Searches, Studies Selection, and Data Extraction
The systematic searches were done on the electronic databases, such as PubMed/Medline, Scopus, Science Direct, The Cochrane Library, Web of Science, SciELO, PsycINFO, and International Pharmaceutical Abstracts, using the following descriptors: clinical trials, random*, random allocation, attention deficit hyperactivity disorder, attention deficit-hyperactivity disorder, attention deficit disorder, adhd, adult*, adult, and adults. The descriptors were combined with the Boolean operators AND and OR, and updated in June 2016 (see Supplemental Material Appendix 1 for full search strategy). Language and time were not used as limits for the searches. We also searched for eligible articles through the references of the papers included during the manual search.
Randomized, double-blind, and parallel controlled trials that compared any drug used for treating adults with ADHD (>18 years, without any comorbidities), head-to-head or against placebo, and evaluated outcomes of safety (e.g., adverse events) were included. Drugs at any dosage and regimen were considered. The following data were independently extracted: baseline characteristics (authors’ names; year of publication; country; sample size; patients’ gender; age; and condition; and trial duration); safety outcomes were assessed based on the incidence of adverse events, namely, anorexia, diminished appetite, insomnia, sleepiness, and diminished libido. Other types of studies (e.g., reviews; editorials; nonrandomized trials), other types of interventions, inclusion of individuals under age 18 years, and trials reported in nonroman characters were excluded.
Quality Assessment of the Included Studies
The included articles were evaluated considering their methodological quality, according to the Jadad Scale (Moore et al., 1996) (see Supplemental Material Appendix 2), and risk of bias by the tool available from the Cochrane Collaboration (Higgins & Green, 2011) (see Supplemental Material Appendix 3). The results were not used as exclusion criteria, but they were considered for interpreting results.
Statistical Analyses
The statistical analyses were performed with the software Review Manager Version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Sweden) (Higgins & Green, 2011), and ADDIS (Aggregate Data Drug Information System) Version 1.16.5 (Valkenhoef, Tervonen, Zwinkels, Brock, & Hillege, 2013).
For pairwise meta-analyses, comparisons of active-drug versus placebo were considered. Calculations were based on measurements of effects such as odds ratio (OR), with confidence intervals (CIs) of 95%, using the statistical method of Mantel–Haenszel and fixed- and random-effects models. The heterogeneity was estimated through I2 statistics, being considered low (I2 < 25%), moderate (25% < I2 <50%), or high (I2 > 50%) (Huedo-Medina, Sánchez-Meca, Marín-Martínez, & Botella, 2006). For the sensibility analyses, the hypothetical exclusion of studies to investigate the influence of each trial on the global effect estimate was performed.
For the network meta-analysis (MTC), we used the Bayesian statistical model, adjusted with Monte Carlo Markov chain (MCMC), and performed multiple comparisons involving both direct and indirect comparisons of all interventions and placebo. We built networks of comparisons for each of the studied outcomes. Consistency analyses were performed to evaluate the relative effect of each drug in networks where credibility interval (CrI) of 95% and OR values were considered as measures. The p value < .05 was considered statistically significant. The network robustness was evaluated through node-splitting analysis (Dias, Welton, Caldwell, & Ades, 2010), in which we considered differences between the direct and indirect comparisons of a determined node (p < .05 represents inconsistency of data, which must be evaluated). Besides that, a probability ranking was elaborated for each outcome, considering the probability of each drug to be classified as best, second best, and so on (Caldwell, Welton, & Ades, 2010; Jansen et al., 2008; Jansen & Naci, 2013).
Ethical Requirements
The current study had no need for approval by the Research Ethics Committee, as the referred Committee in their respective institutions has previously approved the primary studies. The Informed Consent Form was also not required.
Results
A total of 7,487 studies were initially identified, of which 1,138 were duplicates. After reading the titles and abstracts, 86 studies were selected for full-text appraisal. Finally, 10 RCTs (Adler, Spencer, et al., 2009; Adler, Zimmerman, et al., 2009; Goto et al., 2017; Hamedi et al., 2014; Spencer et al., 2008; Sutherland, Adler, Chen, Smith, & Feltner, 2012; Michelson et al., 2003; Weisler et al., 2006; Weisler et al., 2012; Young et al., 2011) were eligible for the proposed analyses, with five of them referring to atomoxetine, two reporting extended-release mixed amphetamine salts, one describing methylphenidate OROS, one on bupropion, and one about bavisant. Figure 1 shows the systematic review process. No study was added by the manual search.
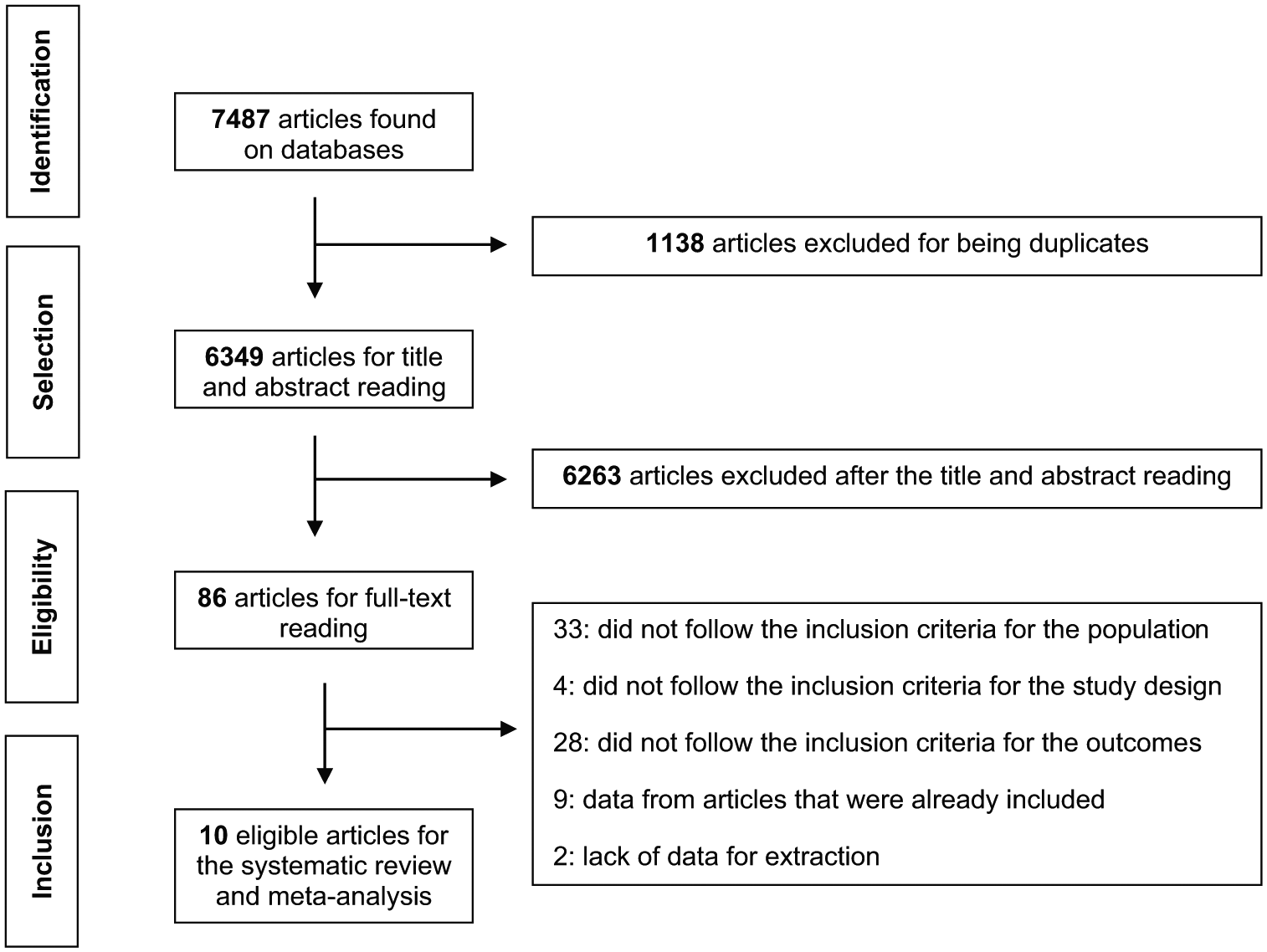
Flowchart of systematic review process.
The main characteristics of each study are summarized in Table 1. The papers were published from 2003 to 2014. The average period of treatment was of 10.5 weeks, with 4 and 24 weeks being the shortest and longest periods, respectively. The drugs varied according to their formulation, with atomoxetine, bupropion and bavisant being immediate release drugs, and mixed amphetamine salts and methylphenidate OROS having extended release. The total number of randomized patients was 3,006 individuals, with an average age of 37.1 years. Considering studies’ methodological quality, the average score obtained from the Jadad Scale was 4.0, whereas seven articles presented higher quality, and three were moderate. The risk of bias showed that most studies did not properly describe the allocation concealment. The domain with the highest risk of bias was from other sources, where most of the authors informed the financial support of the pharmaceutical industries and the presence of conflicts of interest.
Main Characteristics of the Studies Included in the Systematic Review.
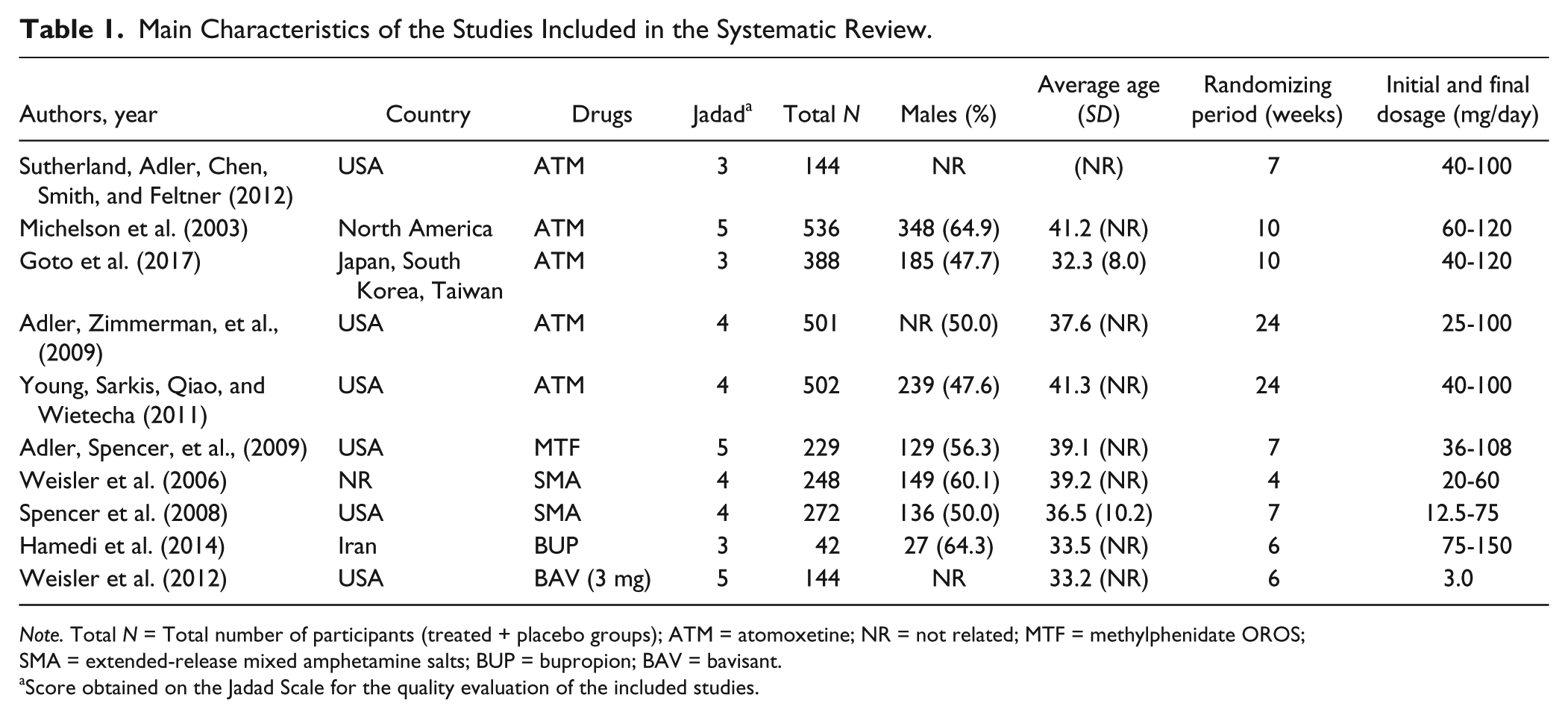
Note. Total N = Total number of participants (treated + placebo groups); ATM = atomoxetine; NR = not related; MTF = methylphenidate OROS; SMA = extended-release mixed amphetamine salts; BUP = bupropion; BAV = bavisant.
Score obtained on the Jadad Scale for the quality evaluation of the included studies.
With the included studies, pairwise meta-analyses and MTC were conducted, and the evaluated outcomes were anorexia, decreased appetite, insomnia, sleepiness, and diminished libido. Except for anorexia, the remaining outcomes showed at least one statistical difference between drugs and/or placebo. We could perform pairwise meta-analyses with atomoxetine versus placebo and extended-release mixed amphetamine salts versus placebo. In both comparisons and for all outcomes, placebo was considered safer, leading to fewer adverse events (see Supplemental Material Appendix 4). Similar results were obtained with the MTC analyses. For clarity, a main network was built accounting for all drugs and regimens (methylphenidate OROS, atomoxetine, bupropion, bavisant, extended-release mixed amphetamine salts and its doses of 20, 40 and 60 mg) and placebo as common comparator (Figure 2). For each outcome, smaller networks were built and analyzed. The components of each network’s outcome are showed in Table 2.

Network with all comparisons of the treatments.
Composition of the Analyses of the Networks Formed for Each Outcome.

In MTC, we also found statistically significant differences when comparing drugs versus placebo for the outcomes of diminished appetite, insomnia, sleepiness, and diminished libido. Table 3 summarizes the main results of pairwise and MTC analyses for comparisons. As we did not find clinical trials that directly compared atomoxetine and methylphenidate OROS for sleepiness, the result was obtained only from MTC and revealed that atomoxetine was more related to this outcome (OR = 0.24, 95% CrI = [0.06, 0.97]). The remaining drugs (bupropion and bavisant) also integrated the MTC analyses, but no significant differences between placebo or other drugs were confirmed. The complete analyses of network consistency are reported in Supplemental Material Appendices 5 and 6.
Final Results of the Statistically Significant Comparisons by Traditional Pairwise and Network Meta-Analyses.

Note. MTC = mixed treatment comparison; OR = odds ratio; CI = confidence interval; CrI = credibility interval; NE = not evaluated.
Due to the simplified geometry of networks formed (star-shaped), only one node-split was visualized on the analyses for the outcome of sleepiness, and results showed robustness of the network (OR = −1.38, 95% CrI = [−4.59, 0.72]) for the direct comparison; OR = −1.50, 95% CrI = [−3.50, 0.15] for indirect comparison; and OR = −1.41, 95% CrI = [−2.90, −0.03] for mixed ones) with p = .93 (>.05).
Rankings probabilities for drugs were also obtained for each outcome. Drugs have probabilities of occupying each position in the ranking, whereas the first carries a higher incidence for the respective outcome (less safe) and the last one was shown to be safer (Figure 3). The psychostimulants mixed amphetamine salts have the highest probabilities of provoking the events of decreased appetite (81% of probability), insomnia (79%), and anorexia (41%), and the safest suggested option was atomoxetine (81%) for cases of loss of appetite, and bupropion for anorexia (48%) and insomnia (32%). However, with regard to insomnia, bupropion (75%) showed the highest probability of causing this event, while methylphenidate OROS (91%) was considered the best choice. Atomoxetine presented the highest chance of causing decreased libido (77%) and bavisant 3 mg (44%) was considered the best choice for this outcome.
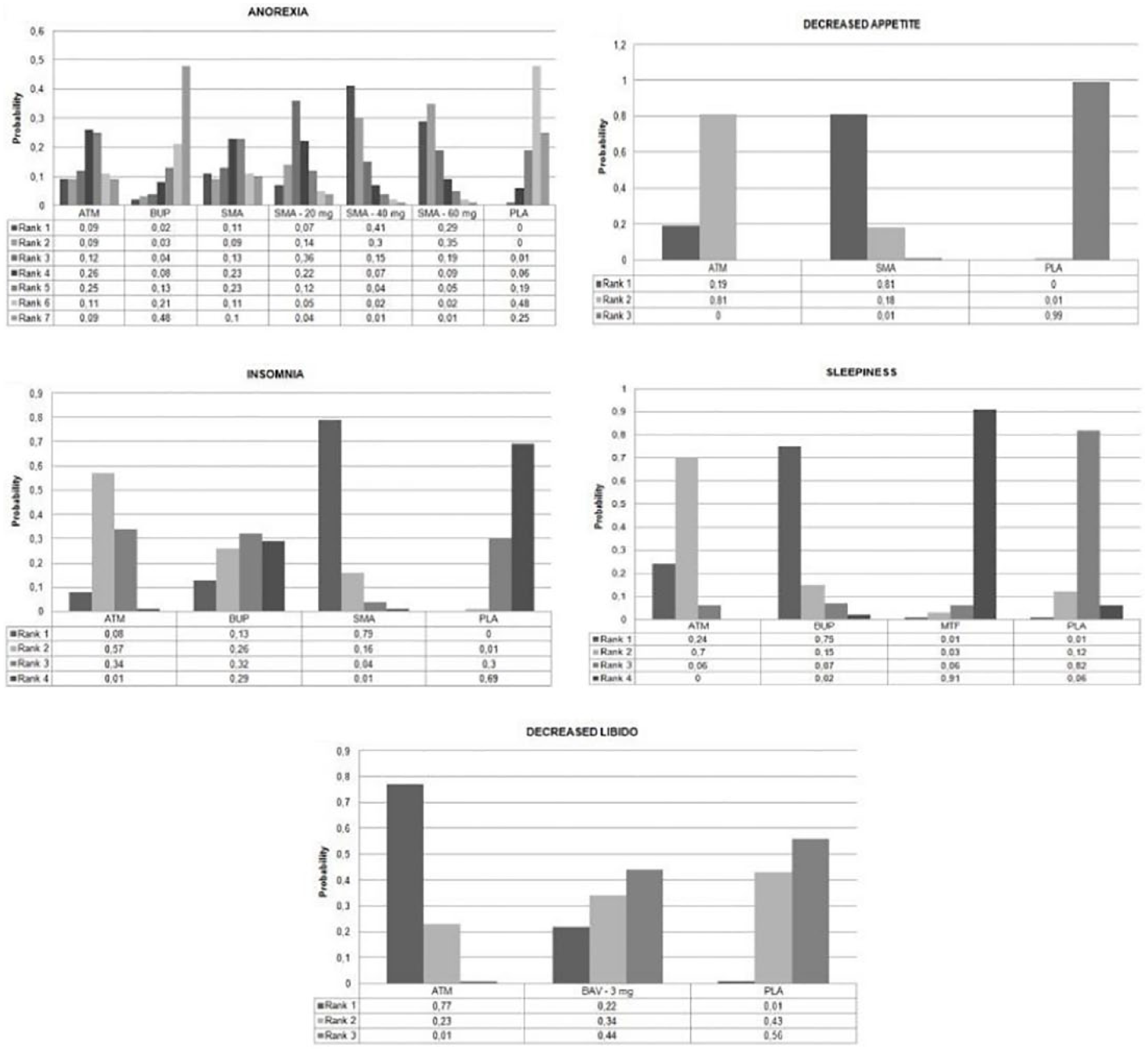
Probability ranks for each drug of occupying a determined position for each considered outcome.
Discussion
This is the first network meta-analysis of safety for the five main drugs used for treating ADHD in adults without any other comorbidity. Apart from drug’s efficacy, safety is equally a relevant topic in medical practice, particularly with regard to approving new medication or questioning the possibility of withdrawing a drug from the market (Alshammari, 2016). We considered double-blind RCTs since they represent the most robust evidence with a higher quality for conducting systematic reviews of interventions. Apart from the pairwise meta-analyses, the MTC technique allowed not only a direct comparison between drugs and placebo but also an indirect comparison between head-to-head trials and different dosages of treatments. Bushe et al. (2016) studied adults with ADHD using a similar methodology, but they evaluated atomoxetine and methylphenidate OROS in different outcomes, without considering the safety profile; they concluded that those drugs are effective for their purpose. Other drugs with potential use which are employed off-label have been poorly studied.
In general, slightly significant statistical differences of safety events among treatments were observed. Most comparisons in the literature are against placebo (atomoxetine versus placebo; mixed amphetamine salts versus placebo), and confirmed that active-drugs have the potential to cause more adverse events, as expected. The head-to-head comparisons showed that methylphenidate OROS was safer than atomoxetine, leading to fewer sleep disorders. This is probably due the mechanism of action of the psychostimulants, which causes alertness due to the increase of extracellular dopamine and norepinephrine in the prefrontal cortex, and dopamine in the striate cortex, with an excitatory effect in the central nervous system (Bolea-Alamañac et al., 2014). Another point to be considered is the type of delivery system technology, because prolonged formulations were developed aiming to decrease the frequency of doses and adverse events (Sugrue, Bogner, & Ehret, 2014). Takahashi et al. (2014), conducted a RCT with 143 adults with ADHD treated with methylphenidate OROS. Patients did not report sleepiness, but 15 of them (10.5%) presented insomnia. Another double-blind, randomized trial compared a group treated with methylphenidate OROS (n = 110) to the placebo group (n = 116) for 7 weeks and highlighted that three patients from the active group (2.7%) reported sleepiness and with insomnia in 10 of them (9.1%) (Adler, Zimmerman, et al., 2009). The psychostimulants are considered the first choice of treatment for ADHD (Chan, Fogler, & Hammerness, 2016; Thapar & Cooper, 2016). However, as observed in our study and previously cited in the literature, there are some adverse events involved with the use of this class of drugs, such as insomnia, diminished appetite, anorexia, weight loss, and agitation. The incidence of these events are quite common and physicians should be aware of the potential effect of each drug to adapt the choices for patients (Adler, Zimmerman, et al., 2009; Spencer et al., 2008; Takahashi et al., 2014).
Atomoxetine is a noncerebral stimulant, selective norepinephrine reuptake inhibitor (Bymaster et al., 2002; Chiara et al., 2004). An integrated analysis of 15 clinical trials showed its adverse events resulting from a comparison against placebo such as decreased appetite, insomnia, and sleepiness in 14.9%, 11.3%, and 6.0% of the cases, respectively (Camporeale et al., 2015). With regard to the adverse effects related to the sexual system, a study showed their frequency during the treatment with atomoxetine versus placebo, and decreased libido occurred in 4.6% of the patients (Camporeale et al., 2013). The increase of these adverse effects is related to the possible nonselective peripheral effect on the adrenergic nervous terminations in the sphincter smooth muscle cells and urethral arteries (Sumner, Schuh, Sutton, Lipetz, & Kelsey, 2006; Viktrup, Pangallo, Detke, & Zinner, 2004), which supports the result that was found for this outcome.
Our networks were found to be robust and, despite few differences, were highlighted among drugs; the results may be used as the basis of decision making in practice. The extended-release mixed amphetamine salts and atomoxetine present relevant adverse effects for their classes, which should be taken into consideration when deciding the therapeutic choice for each patient. Drugs such as bupropion and bavisant seem to be promising alternatives, as shown in the rank probabilities, but as only a few trials could be gathered, results from MTC carries a wide CrI. Thus, these effects should be better investigated in further studies or comparisons. The possibility to incorporate these therapies in clinical guidelines should also be considered, based on clinical evidence, thereby providing further tolerable alternatives. Besides the efficacy and safety profile, it is important to conduct pharmacoeconomic studies to evaluate the cost–benefit of each therapy in health-care settings of the countries.
This study has some limitations. We included only 10 clinical trials in the meta-analyses, which may have underestimated the statistical differences between the comparisons. However, the strategies on the databases and manual search did not reveal any additional studies, demonstrating that all of the information available in the literature were collected. We were not able to perform subgroup analyses with the technology of delivery system or medication doses due the small number of studies. However, it was possible to show some differences that should be better investigated in future studies. It was not possible to analyze the efficacy outcomes of the referred drugs since there is a remarkable lack of standardization on the report of data in clinical trials (e.g., different psychometric scales are used, measures of effect are divergent, and authors did not provide complete raw data). Besides that, the MTC methodology confirmed the results obtained from the conventional meta-analyses and allowed new evidence to be generated to date by the head-to-head comparisons.
Conclusion
This study, through the combination of statistical techniques, generated evidence on the extended-release mixed amphetamine salts and atomoxetine potentials to cause more adverse events. Methylphenidate remains as an important treatment with regard to some side-effects that should be considered during therapy selection. Bupropion and bavisant seem to be potential alternatives for ADHD treatment. These results may help to guide clinical decisions and base future studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.