
Abstract
Introduction
An estimated 2% to 12% of college students have attention-deficit/hyperactivity disorder (ADHD; Nugent & Smart, 2014). Although college students with ADHD tend to have higher cognitive abilities and more effective compensatory skills than their peers diagnosed with ADHD who do not attend college or higher education (Frazier, Youngstrom, Glutting, & Watkins, 2007), they have struggles dealing with a college or university environment. Studies focusing on college students with ADHD show that compared with their college peers without the disorder, they have difficulty with global academic functioning (for review: Emmers, Janssen, Petry, Van der Oord, & Baeyens, 2017). More particularly, they have problems with planning their daily academic life; they have difficulty completing academic assignments in time, take longer to complete assignments, and have difficulty planning their studies and going to lectures (Advokat, Martino, Hill, & Gouvier, 2007; DuPaul, Weyandt, O’Dell, & Varejao, 2009; Gudjonsson, Sigurdsson, Smari, & Young, 2009; Johnson & Reid, 2011; Lewandowski, Lovett, Codding, & Gordon, 2008; Prevatt, Proctor, Baker, Garrett, & Yelland, 2011; Weyandt et al., 2013). Also, they show problems with academic study skills, such as difficulty with appropriate test-taking strategies and delineating main and side issues (Johnson & Reid, 2011; Reaser, Prevatt, Petscher, & Proctor, 2007). All these academic difficulties may result in a less successful academic career and a higher risk of college dropout (Barkley, Fischer, Smallish, & Fletcher, 2006). Several studies show that during their whole academic career, college students with ADHD have lower grade point averages than their peers (Blase et al., 2009; Frazier et al., 2007; Heiligenstein, Guenther, Levy, Savino, & Fulwiler, 1999) and are less likely to graduate from college (Heiligenstein et al., 1999). By adulthood, individuals with ADHD have completed fewer years of education than individuals without ADHD, with relatively few individuals with ADHD graduating from higher education (DuPaul et al., 2009; Fleming & McMahon, 2012).
Next to academic problems, in students with ADHD, higher rates of comorbidity have been reported than their college student peers in both the internalizing (depressive and anxiety) as well as the externalizing (substance use, oppositional behavior) symptom domains (Fleming & McMahon, 2012). Within ADHD samples, depressive and anxiety symptoms increase throughout the transition from adolescence to adulthood as a result of the expansion of the failures in among others school, work, and relationships (Safren, Sprich, Cooper-Vince, Knouse, & Lerner, 2010).
Two important life changes can be put forward to explain these difficulties they experience in daily life and in their (academic) functioning. First, students attending college mostly are in their late adolescent years (19-22 years), which is an important transition phase to adulthood. Compared with mid-adolescence (15-18 years), late adolescence is characterized by an increasing responsibility for themselves and others, an increased capacity of self-reflection. However, self-regulation is not yet fully developed (Arnett, 2000; Casey, Jones, & Hare, 2008), especially not in individuals with ADHD (Alderson, Kasper, Hudec, & Patros, 2013; Marx et al., 2010; Shaw et al., 2007). Second, evidence shows that within transition phases (e.g., from high school to college or university), individuals with ADHD have significant increases in planning and organizational problems (Langberg et al., 2011). Especially in college students with ADHD, increasing academic demands coincide with a loss of a structured environment (i.e., home, high school), which potentially exceeds their planning and organizational capacities (DuPaul et al., 2009) and self-regulation capacities.
A longitudinal study among college students with ADHD showed the importance of these planning skills for the functioning of college students (Dvorsky & Langberg, 2019). Planning-related deficits in the beginning of the year were the most important predictor (more than ADHD symptoms) of the grades at the end of the academic year (Dvorsky & Langberg, 2019). Moreover, motivational deficits at the beginning of the academic year predicted academic functioning at the end of the academic year (Dvorsky & Langberg, 2019). Next to executive deficits such as planning problems, deficits in reward processing and motivation (e.g., a preference for immediate reward and an aversion for delay-related situations) play an important role in the functional impairments individuals with ADHD display (Dovis, Van der Oord, Huizenga, Wiers, & Prins, 2015; Dovis, Van der Oord, Wiers, & Prins, 2012; Van Dessel et al., 2018). In college life, reinforcers are often delayed (e.g., studying for an exam before having the reward of passing the exam), and immediate reinforcers (e.g., social activities with friends, social media) are omnipresent. These results suggest that planning skills and motivation are important impairment domains that need to be targeted in treatment for college students for ADHD (He & Antshel, 2017).
Studies in adults with ADHD show the effectiveness of treatments targeting the core executive function problems of planning and organization (Safren, Sprich, Cooper-Vince, et al., 2010; Safren, Sprich, Mimiaga, et al., 2010) and motivational deficits (Solanto et al., 2010). An individual cognitive behavioral planning and organization intervention was more effective on the reduction of ADHD symptoms and internalizing comorbidity, compared with an active control condition (Safren, Sprich, Mimiaga, et al., 2010). Another group-based intervention, focused on increasing planning and organization skills and reducing motivational deficits, found significant reductions in ADHD symptoms, but not comorbidity (Solanto et al., 2010). It should be noted, however, that both these interventions were not specifically tailored for the demands that college students encounter with planning and organization in their academic life in this specific developmental transition phase.
Until recently, there was a lack of randomized controlled studies on the effectiveness of specific cognitive behavioral therapy (CBT) interventions focusing on enhancement of their planning capacities, specifically, for college students with ADHD (He & Antshel, 2017; Knouse, 2015). A recent review (Knouse, 2015) reports four planning-focused CBT treatment studies for this specific group, with the treatments showing potential to improve both symptomatology and functioning. However, of these four studies, only two are randomized clinical trials (RCT). The first RCT (N = 17) showed promising evidence of a short (three session) group-based organizational skills training in students with elevated ADHD symptom scores (however, no clinical diagnosis of ADHD); after following the course, they showed less ADHD symptoms and academic impairment than a comparison group (LaCount, Hartung, Shelton, & Stevens, 2018). The other RCT (N = 33) that was conducted in diagnosed students with ADHD showed that as compared with students who received handouts covering ADHD self-management skills, a dialectical behavior therapy group skills training (with among others organization and planning skills emphasized) was effective in improving inattentive symptoms, executive functioning, and quality of life. However, the power of the study was quite low (Fleming, McMahon, Moran, Peterson, & Dreessen, 2015). Also a recent study shows promising and long-term effects of a CBT in students with ADHD, which uses mentoring sessions alongside treatment not only on reduction of ADHD symptoms and executive functioning but also on comorbid symptoms and educational functioning (Anastopoulos et al., 2018). In sum, there are indications that planning-focused CBT is effective for college students with ADHD to improve in various domains (e.g., quality of life, inattentive symptoms), but randomized controlled studies are called for in larger samples (He & Antshel, 2017; Knouse, 2015).
In the current study, we developed a cognitive-behavioral planning and organization intervention, specifically focused and adapted to the specific problems college students with ADHD encounter (i.e., studying and academic problems). The planning and organization program for college students is based on a planning and organization intervention program that was developed and tested for adolescents with ADHD (Boyer, Geurts, Prins, & Van der Oord, 2015; Kuin, Boyer, & Van der Oord, 2013) in which also motivational interviewing is integrated to target their motivational deficits, often encountered in this period of their life, and to enhance their motivation for change. An RCT in adolescents with ADHD (N = 159) showed preliminary evidence for effectiveness of this program on reduction of planning deficits and adolescents’ satisfaction with the intervention (Boyer et al., 2015), as compared with another nonplanning focused active treatment. Moreover, treatment attrition was low (5%), and improvement of ADHD symptoms and other related problems were maintained over time (Boyer et al., 2015). For the current study, we adapted this treatment manual for use with college students (see “Method” section).
The current study compares the immediate effectiveness of this planning-focused CBT in college students with ADHD as compared with a waitlist control condition. Our primary outcomes were academic functioning (learning and study strategies) and ADHD symptoms, whereas our secondary outcomes were comorbid symptoms (e.g., depression, oppositional defiant disorder/conduct disorder) and planning-related difficulties (objectively measured by a neuropsychological measure of planning). Outcomes were measured pre- and posttreatment. Further stability of effects was assessed 4 months after completion of the intervention in the active condition. We expected the intervention to be more effective than the waitlist control condition on reduction of ADHD symptoms, comorbidity, objectively measured planning, and improvement of learning and study strategies. Also, we expected the treatment effects to be stable to 4 months follow-up.
Method
Participants and Procedure
Participants were recruited through three different student counseling services, two university college services (Hasselt, Antwerp), and one university service (Leuven). Inclusion criteria were (a) age between 17 and 25 years, (b) being enrolled in a Belgian university college or university, (c) having a prior diagnosis of ADHD that was confirmed using the Diagnostic Interview for Adults with ADHD (DIVA; Kooij & Francken, 2010), (d) if taking medication for their ADHD, being stabilized on medication at least for 4 weeks, (e) no comorbid diagnosis of borderline personality disorder (as we deemed a short-term intervention not suitable for those with a personality disorder) on the McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD; Verschuere & Tibboel, 2011). For those scoring above cutoff on this screener (a score of “yes” on 7 out of 10 items), the Borderline Personality Disorder section of the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994; SCID-II; First, Gibbon, Spitzer, Williams, & Benjamin, 1997) was assessed to confirm exclusion, (f) no comorbid substance abuse disorder or suicidal ideation and no severe depression on the Mini International Neuropsychiatric Interview (MINI) Plus (Sheehan & Lecrubier, 2004; Van Vliet, Leroy, & Van Megen, 2000): those meeting DSM criteria for substance abuse and those indicating suicidal ideation (as objectified by a moderate to high risk on the “suicidality index” of the MINI) were excluded. None of the students who applied for the intervention were excluded based on these criteria.
After enrollment, college students were invited for a short session, during which participants were given information on the study and the nature of the treatment (a six-session treatment focused on enhancing planning and organization of their daily academic life), and written informed consent was obtained. Then, a pretest of approximately 2.5 h was planned in which several measures and semistructured interviews were administered, as well as the assessment of current medication use. During posttest (immediately after the last session) and follow-up (approximately 4 months after the last session), the same measures, with the exception of the selection measures, were re-administered. Posttest and follow-up were conducted by research assistants as much as possible, blind to intervention condition.
After pretest, participants were randomized to either active or waitlist control condition. Randomization was conducted such that random numbers were generated (www.randomizer.org), using blocked randomization (by 2). To assure complete blindness, randomization was conducted after two participants had given informed consent. Randomization was stratified by gender, using covariate adaptive randomization (Kang, Ragan, & Park, 2008). During active intervention or during waitlist, participants were instructed not to change medication dose or regimen or to receive other psychological intervention. After posttest, those randomized to the waitlist could follow the training, however, we did not follow up the participants in this condition anymore. For clinical trial registration, see http: with ADHD.” http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=3265,
Selection measures
The Diagnostic Interview for Adult ADHD, second edition (DIVA 2.0; Kooij & Francken, 2010) is a structured diagnostic instrument for ADHD in adulthood. The DIVA 2.0 investigates the presence (yes/no) of the DSM-IV criteria of ADHD in childhood and adulthood, as well as five areas of functioning in both life periods (education, work, social relationships, social activities/leisure time, and partner/family relationships and self-esteem). A criterion of six symptoms of either inattention or hyperactivity/impulsivity was used to confirm the diagnostic criteria. The interview is preferably administered in the presence of the ADHD patient and his or her family. For the current study, we assessed the interview with the student only. The DIVA 2.0 has good concurrent validity (Ramos-Quiroga et al., 2019).
The MINI Plus (Sheehan & Lecrubier, 2004) is a short diagnostic structured clinical interview for 17 Axis I Psychiatric Disorders of DSM-IV and International Classification of Diseases–10th edition (ICD-10). In this study, we administered the clinician rated format: The presence or absence of symptoms (yes/no) is rated by the clinician. If initial scores on starting questions are too high, follow-up questions are administered to cover the full DSM-IV criteria of a psychiatric disorder. The MINI shows adequate reliability and validity (Sheehan & Lecrubier, 2004).
The MSI-BPD (Zanarini et al., 2003) is a 10-item based self-report screening instrument for borderline personality disorder, based on a subset of questions that comprise the borderline module of the Diagnostic Interview for DSM-IV Personality Disorder (DIPD-IV; Zanarini, Frankenburg, Sickel, & Yong, 1996). Adults indicate the presence or absence of 10 problem behaviors. A score of ≥7 has been suggested as a clinical score. Sensitivity and specificity are reported to be good (Zanarini et al., 2003).
The Borderline Personality Disorder section of the Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II; First et al., 1997) was administered in this study if a subject’s score is in the clinical range of the MSI-BPD (Zanarini et al., 2003). The SCID-II is a structured clinical interview that assesses the full range of traits found in DSM-IV Axis II. The SCID-II contains 140 questions, which are scored on a 3-point scale (absent/doubtful/present). Acceptable reliability and validity have been established (First et al., 1997).
Outcome Measures
Primary outcomes
The ADHD Rating Scale (ADHD-RS; DuPaul, Power, Anastopoulos, & Reid, 1998) consists of the 18 DSM-IV items for ADHD. However, in the Dutch version, five DSM-IV items containing double statements were reformulated in two separate statements (Kooij et al., 2008). When scoring the ADHD-RS, these 23 item scores were recalculated to the original 18 DSM-IV items. The items were rated twice on a 4-point scale: once based on behavior in the past 6 months and a second time based on behavior during childhood. The ADHD-RS can be completed either as a self-report scale for adults or by someone who knows the person well, the current study used the self-report scale. The Dutch questionnaire consists of two subscales (inattention and hyperactivity/impulsivity). Higher scores indicate more problems. In a Flemish population of 16 to 25 year olds, acceptable reliability and validity are established (Baeyens, Van Dyck, Broothaerts, Danckaerts, & Kooij, 2012).
The Learning and Study Strategies Inventory (LASSI, Weinstein, Palmer, & Schulte, 1987, 2002; Dutch translation, Lacante & Lens, 2005) is a self-report measure assessing students’ awareness about and use of learning and study strategies related to skill, will, and self-regulation components of strategic learning. It consists of 77 items and 10 subscales, each related to either strategic learning skills (i.e., information processing, selecting main ideas, and test strategies), strategic learning (i.e., test anxiety, motivation, attitude), or self-regulation (time management, concentration, self-testing, study techniques). Higher scores indicate better learning and study strategies. The reliability and validity of the LASSI are adequate (Weinstein & Palmer, 2002), with reports of LASSI scores predicting students’ Grade Point Average (GPA; Carson, 2011; Marrs, Sigler, & Hayes, 2009).
Secondary outcomes
The Beck Depression Inventory II (BDI-II; Beck, Steer, & Brown, 1996) is a 21-item self-report scale assessing cognitive, affective, and somatic symptoms of depression. Higher scores indicate a greater severity. Reliability and validity are reported to be good (Beck et al., 1996).
A subtest of the Delis-Kaplan Executive Function System (D-KEFS; Delis, Kaplan, & Kramer, 2001) was used to assess planning. The Tower Test assesses several key executive functions (EF), including planning. The objective of this subtest is to move disks, varying in size from small to large, across three pegs to build a designated tower in the fewest number of moves possible. In constructing the target towers, the examinee must follow two rules: (a) move only one disk at a time and (b) never place a larger disk over a smaller disk. The “total achievement score” was used as outcome. The total achievement score gives an overall planning score and is based on the number of moves to build the tower, rule violations, completion time, and final tower correctness (Delis et al., 2001). Scores range from 0 to 30, with higher scores indicating better planning skills.
The Adult Self-Report (ASR; Achenbach & Rescorla, 2003) is a 126-item standardized, empirically validated measure of problem behavior intended for completion by adults aged 18 to 59 years. Problem items are rated as “not true,” “somewhat or sometimes true,” or “very true or often true” in the past 6 months. Co-occurring problems are clustered into the syndrome scales anxious/depressed, withdrawn, somatic complaints, thought problems, attention problems, aggressive behavior, rule-breaking behavior, and intrusive behavior. The composite scale of the first three syndrome scales is “Internalizing Problems” and of the last five syndrome scales is “Externalizing problems”. Higher scores indicate more problems. Acceptable reliability and validity have been established (Achenbach & Rescorla, 2003).
Intervention
The planning and organization intervention (Boyer, Van Dyck, Kuin, & Van der Oord, 2012), is a manualized 6-week individual intervention focused on enhancement of planning and organization skills related to the college and university context. Sessions (approximately 1 h) took place at university or college psychological services in one of the three locations. For the college students in two locations, the sessions were free. Due to university regulations of one of the sites (students must pay for psychological service of the university), those students paid €15 per session. 2
The intervention was provided by eight clinical psychologists (in Flanders, clinical psychologists have followed a 3-year bachelor in psychology and a 2-year master in clinical psychology), who were trained for 8 h by the first author (certified behavior therapist, supervisor of the Flemish Behavior Therapy Association); all had experience with cognitive behavior therapy and were either licensed cognitive behavior therapists or were in the clinical training program for cognitive behavior therapy. In Flanders, the cognitive behavioral therapy program is a selective 4-year clinical psychology postmasters course, as such therapists were highly qualified to provide the treatment. As the aim of this study was exploring efficacy under regular circumstances in natural university/college settings and no additional funding was available, there was no follow-up supervision or quality control on implementation of the protocol throughout the whole trial, although for the first patient(s) of every therapist, a supervision session was planned.
The first session of the manual was dedicated to providing information about the training, exploring individual difficulties with studying and medication (if applicable), psycho-education about ADHD, exploring pros and cons of behavior change, and determining five individual treatment goals. Together with the therapist, each student formulated five personal goals they wanted to work on during the course (e.g., being on time for classes). The second session involved creating a planning scheme for the semester using a daily planner. The third session involved making a weekly plan and a to-do list. The fourth session was on strategies for efficient studying, such as handling distraction during studying. In the fifth session the student could bring a friend or family member, and it was evaluated if and how this friend/family member could support the student with ADHD. The final session was an evaluation and repetition of all the learned skills. During every session, the cognitions about their functioning and goals were evaluated, and if needed, they were restructured.
Furthermore, following each session, students completed a questionnaire to evaluate the intervention session they received. To monitor intervention and therapist’s acceptability four questions were rated on a 5-point Likert-type scale, with higher scores indicating positive evaluation (Boyer et al., 2015). Therapist and students discussed the scores of this scale, if indicated. Also, each week the student rated how implementation of treatment in their daily life had gone the previous week, by evaluating their five personal goals using the 5-point scale. 4 months after the intervention, there was a booster session in which a relapse prevention plan was made: There was a repetition of all the learned skills, and together with the student, it was evaluated whether the skills had been helpful or needed to be adapted.
This student manual was adapted from the Dutch manual for adolescents with ADHD “Plan my Life” (Boyer et al., 2015; Kuin, Boyer, & Van der Oord, 2013), in close cooperation with an experienced student counselor from a Belgian university college, who had ample experience working with students with ADHD. To suit the student population, it was adapted in the following ways. First, it was shortened from eight (as in Plan my Life) to six sessions. This was necessary because university counseling services only are allowed to provide short-term treatment (i.e., six sessions), and within the Belgian 13-week semester system, six sessions could easily be given in one semester (with also time for referral, intake, and posttest without interfering with exam periods at the end of the semester). Second, as students are often away from their home town and have a need for independence, we did not provide the two parental sessions from “Plan my life,” although they could bring their parents in the session in which we focus on how significant others could help them with their planning and organization. Third, an additional focus was making a semester planning. Finally, we added optimal modules on enhancing study strategies (e.g., how can I learn a large amount of text?).
Statistical Analyses
First, using t tests for continuous variables and Fisher’s exact tests for categorical variables, it was checked whether the intervention condition and waitlist condition differed on demographics and pretest outcome measures. Intent-to-treat analyses were conducted on the primary and secondary outcomes in which missing data were estimated using stochastic regression analyses (Baraldi & Enders, 2010), additionally completer analyses were conducted. These missing data were not related to any subject characteristics and therefore were missing completely at random, χ 2 (55, N = 58) = 62.49, p = .23. The range of missing data for the pre- and posttest scores ranged from 2% (ADHD-RS pretest, LASSI pretest, planning pretest) to 36% (LASSI posttest), with no significant differences in missing data among treatment conditions, χ 2 (1) = 0.60, p = .44. There are also no significant differences in missing data between the three locations, χ 2 (2) = 2.11, p = .35. The follow-up data had at a minimum of 47.6% missing data (range 47.6%-50%; for explanation, see flowchart in Figure 1) and were therefore not imputed nor included in the analysis as imputing data with these percentages are not reliable (Sheffer, 2002). As these low amounts of data for the follow-up are potentially not representative for the whole group that participated in the study, only the immediate effects (pre-post data) are reported from now onwards.
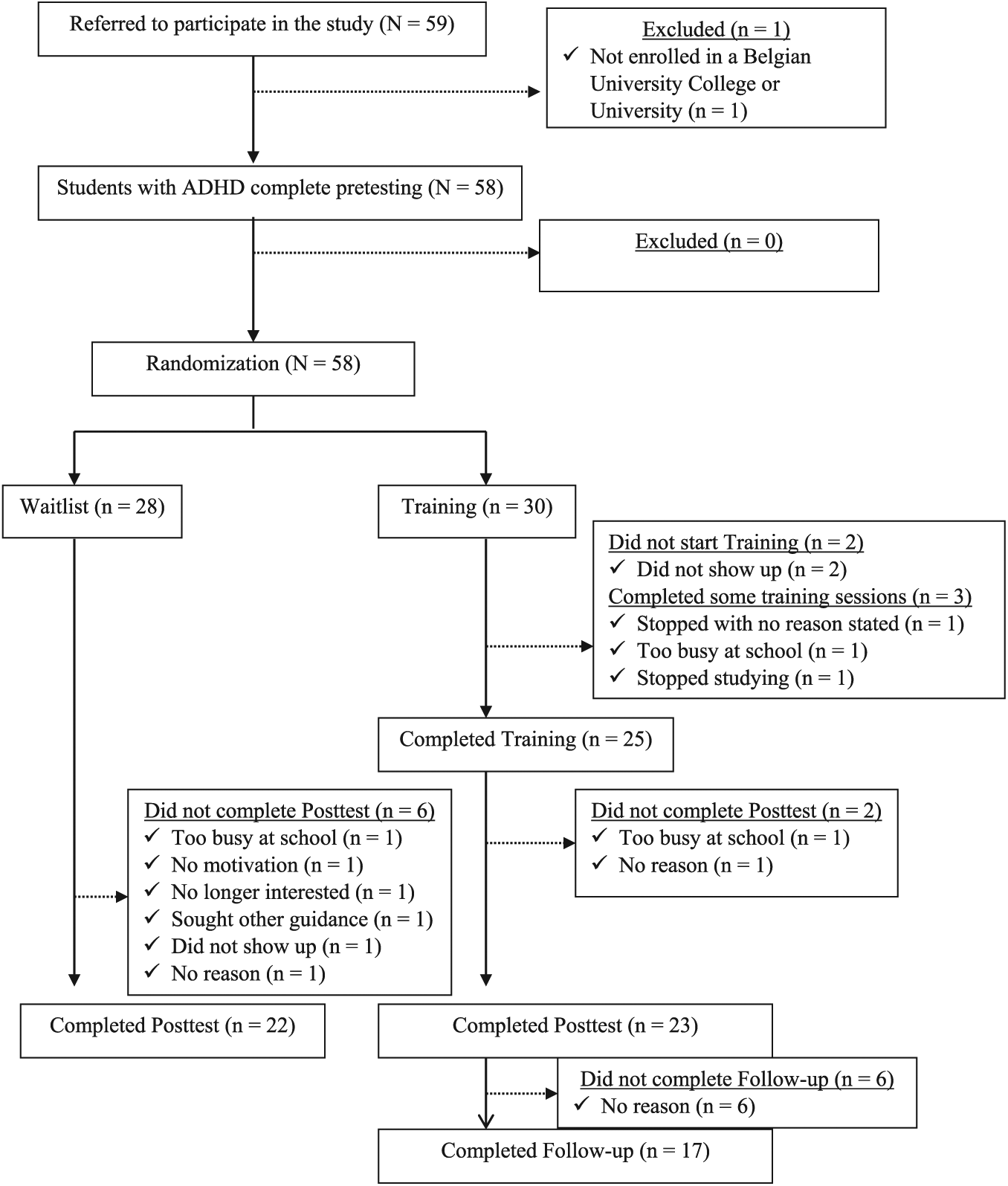
Flowchart of participants in the current study.
To test for treatment effects, three separate MANOVAs were conducted, one with the two subscales of the ADHD measure, one with the LASSI subscale scores, and one with the secondary outcomes (ASR, Tower Test, and BDI scores). In these MANOVAs, pre- and posttest scores were used as the within-subjects factor and treatment condition as the between-subjects factor. These MANOVAs were followed up by univariate analyses on the subscale scores. Partial eta-squared effect sizes (
Results
Descriptive Statistics
In total, 59 students were enrolled in the study (18 females, 41 males), one was excluded because of not being enrolled in a university or university college at the time of the study (for flowchart see Figure 1). The remaining 58 were randomized to immediate intervention (n = 30) or waitlist (n = 28). The groups did not differ in baseline demographics, type of ADHD diagnosis, pretest scores, or comorbidity (Tables 1 and 2). Of the students randomized to the treatment condition, 17% did not start or complete the six treatment sessions due to various reasons (stopping study, not interested, no reason stated), 23% of the students (both waitlist and treatment condition) did not complete posttest. Within the intervention group, there were no significant differences between those who completed treatment or posttest and those who did not complete treatment or posttest at baseline (see Supplementary Table 2).
Frequencies of Baseline Demographics and Results of the Fisher’s Exact Tests Between Intervention and Waitlist.
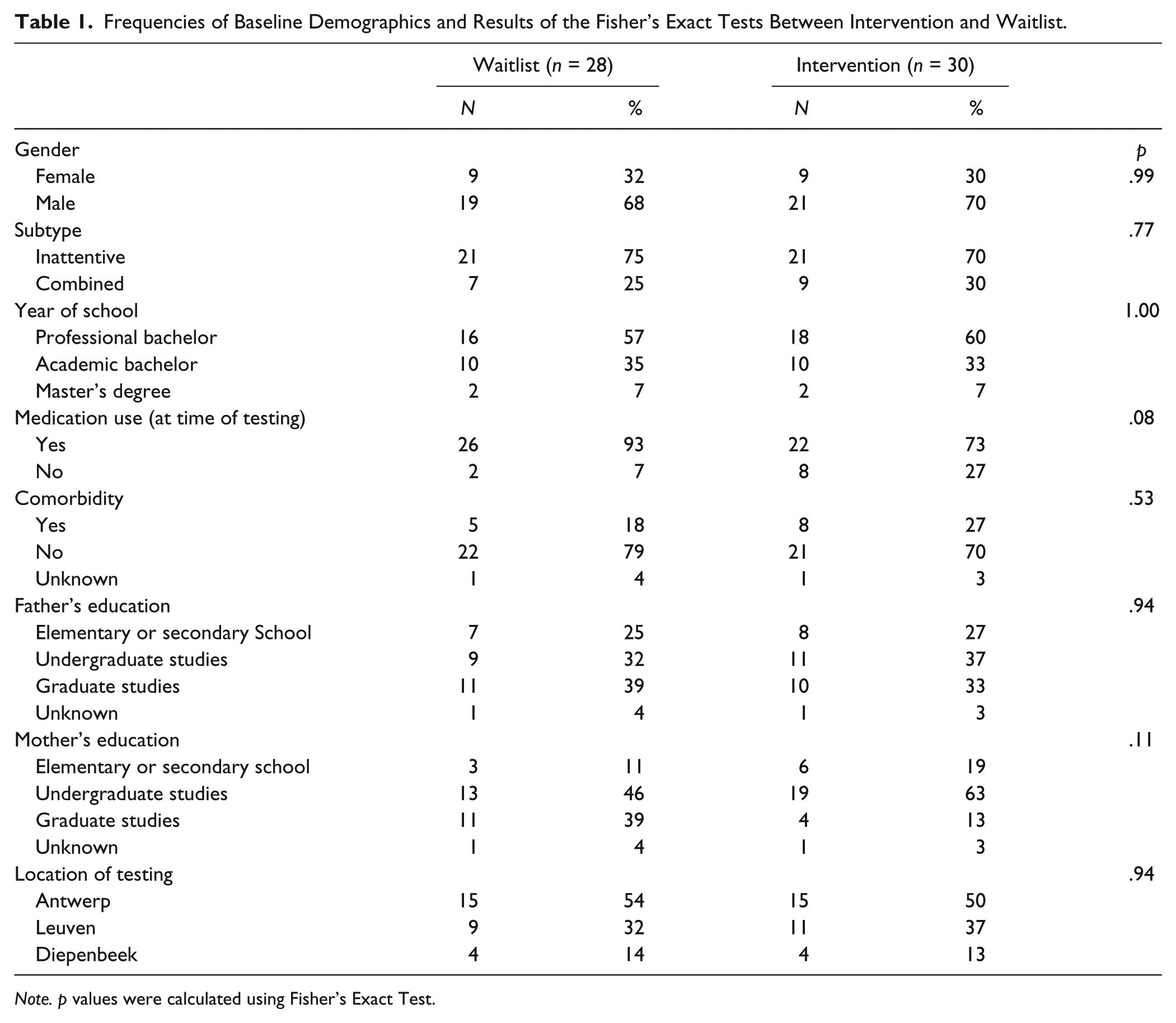
Note. p values were calculated using Fisher’s Exact Test.
Results of the t Tests Between Conditions (Intervention vs. Waitlist) on Descriptive Statistics and Baseline Measures.
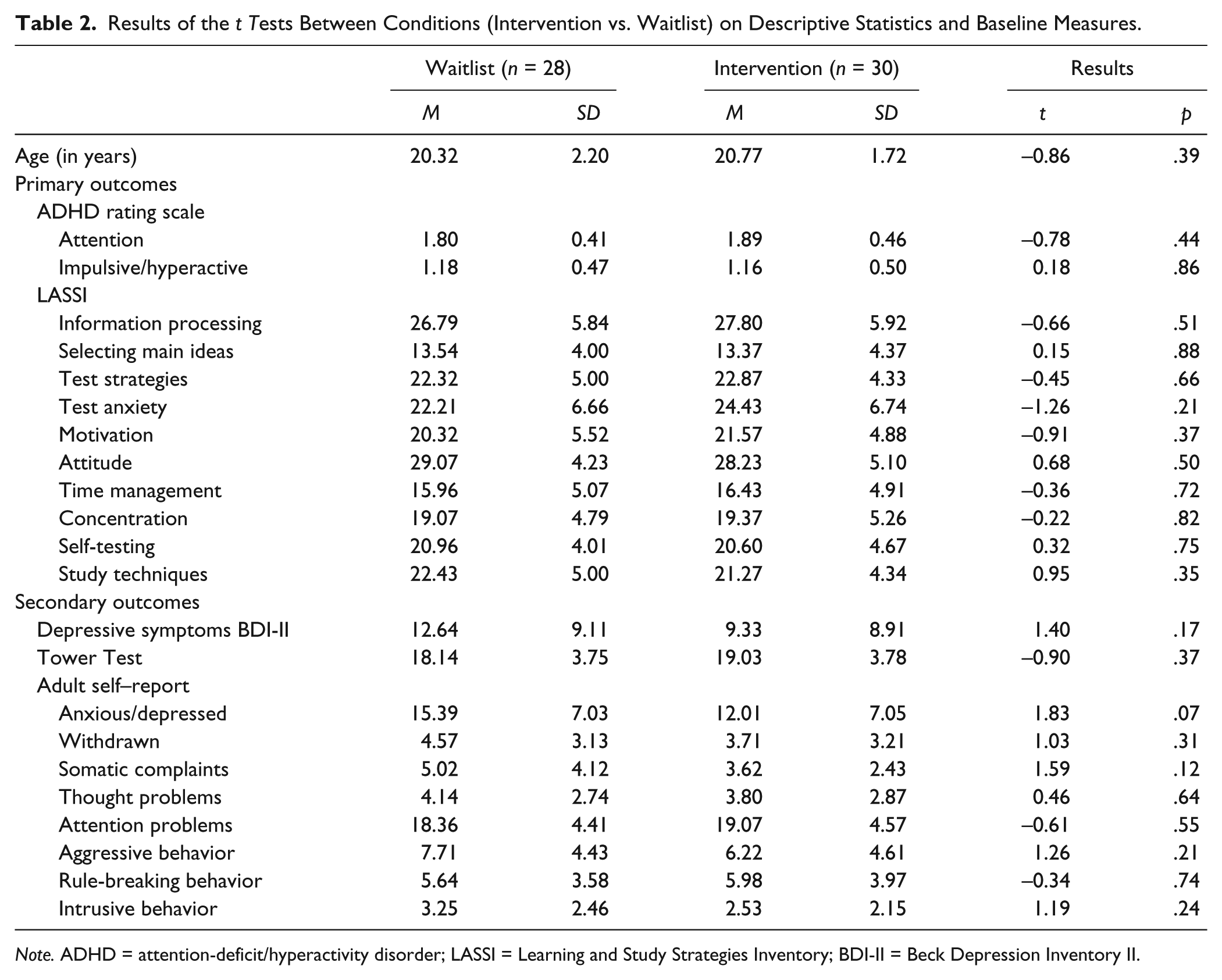
Note. ADHD = attention-deficit/hyperactivity disorder; LASSI = Learning and Study Strategies Inventory; BDI-II = Beck Depression Inventory II.
Inferential Statistics
As for the primary outcomes of the intent-to-treat sample, multivariate analyses showed a main effect of time (pretest to posttest) on ADHD symptoms and a trend (.09) for the time by condition interaction (Tables 3 and 4). Follow-up univariate analysis of this trend showed a significant time (large effect size) and time by condition interaction for the inattention subscale (medium effect size) but not for the hyperactivity subscale. The training condition showed a larger reduction of their inattention symptoms from pre- to posttest than the waitlist control condition.
Pretest and Posttest Means and Standard Deviations of Primary and Secondary Outcomes in Waitlist and Intervention Conditions.
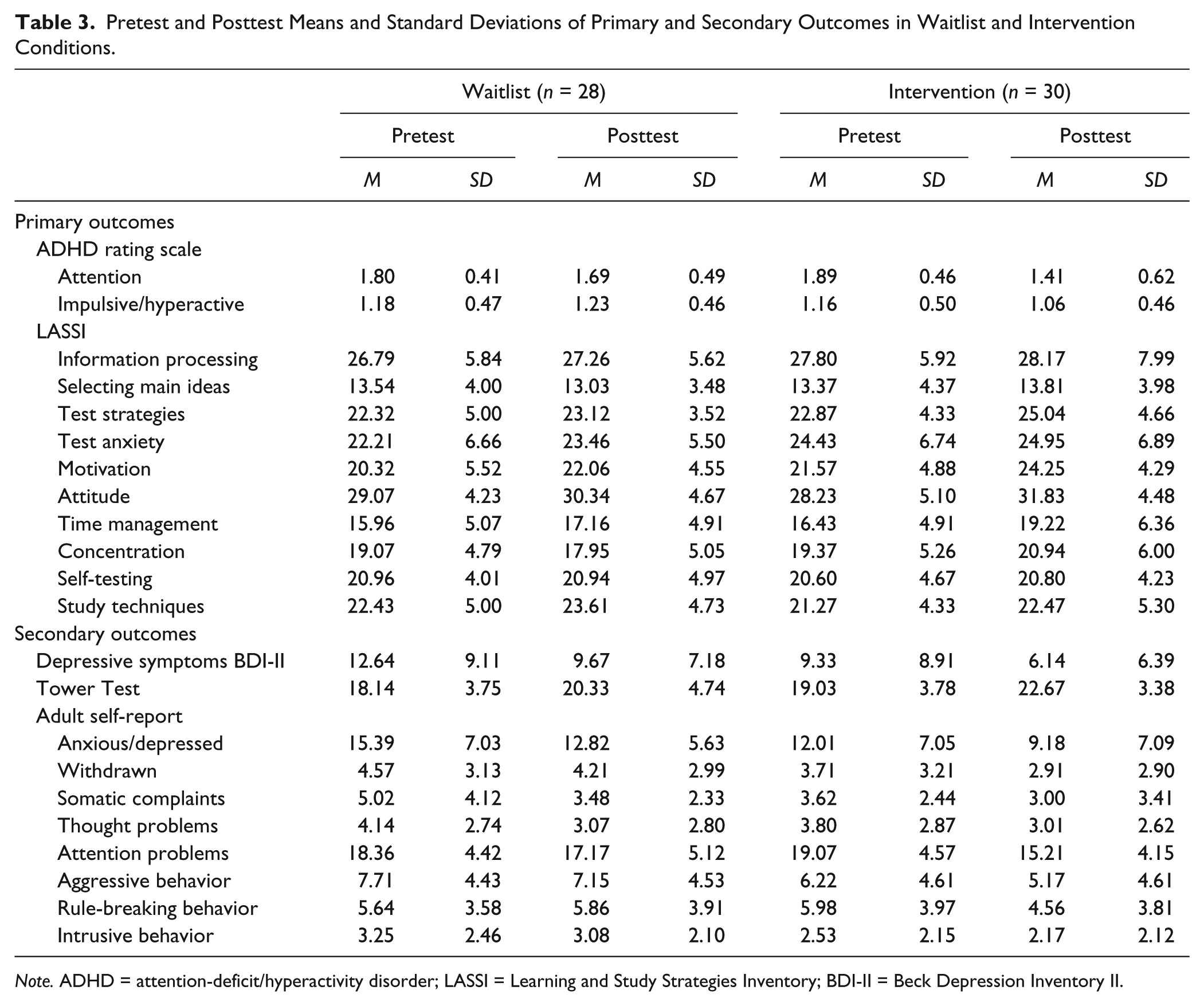
Note. ADHD = attention-deficit/hyperactivity disorder; LASSI = Learning and Study Strategies Inventory; BDI-II = Beck Depression Inventory II.
MANOVA Results for the Imputed Data in the Study (Intent-to-Treat Analyses).
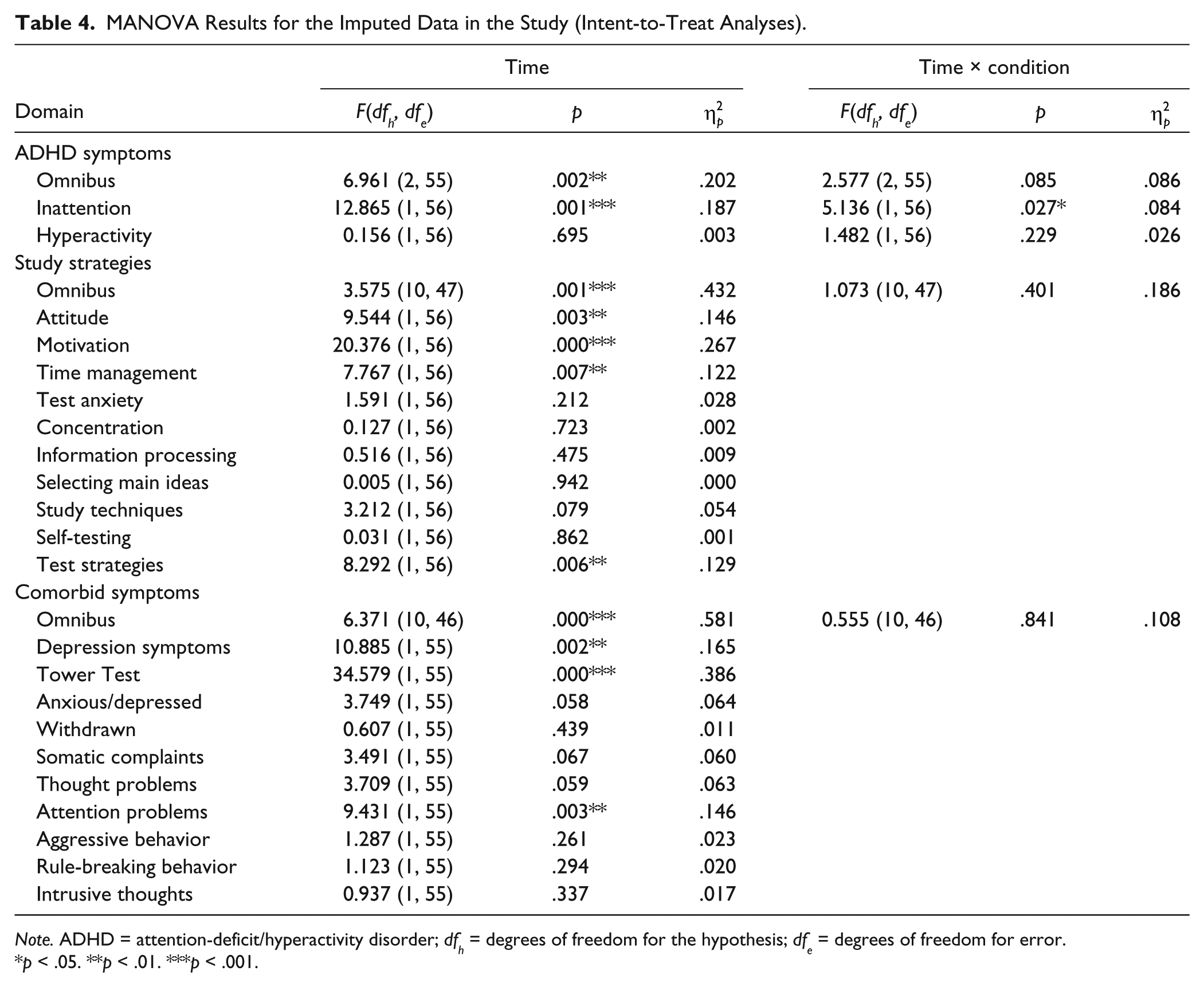
Note. ADHD = attention-deficit/hyperactivity disorder; dfh = degrees of freedom for the hypothesis; dfe = degrees of freedom for error.
p < .05. **p < .01. ***p < .001.
For the other primary outcome, LASSI multivariate analyses showed a significant main effect of time, but no time by treatment interaction. The follow-up univariate analysis showed significant time effects for the subscales attitude, motivation, time management, and test strategies (medium to large effect sizes). As there was no significant interaction effect, follow-up univariate analysis are not justified.
As for the secondary outcomes, the MANOVA showed a main effect of time (pre- to posttest), but no time by treatment interaction. Follow-up univariate tests showed significant time effects for depressive symptoms (BDI), the Tower Test (D-KEFS), and the attention problems subscale of the ASR (medium to large effect sizes).
Completer analyses showed largely similar results (Supplement Table 3), with that difference that the LASSI subscale attitude did not show a significant time effect.
Discussion
For the present study, we developed a six-session cognitive behavioral planning and organization intervention specifically focused and adapted to the specific problems college students with ADHD encounter (i.e., studying and academic problems). We expected this intervention to be effective on reduction of self-rated ADHD symptoms to increase learning and study strategies and planning skills and to reduce comorbidity. Our study showed mixed findings; over time, large improvements were seen in the treatment condition but only attention (ADHD-RS) improved more in the intervention condition than in the waitlist condition. Unexpectedly, the students who followed the intervention did not show significant additional benefits on other study skills as compared with the waitlist, nor did the comorbidity reduce more in the intervention group.
The significant time by treatment interaction on the inattention subscale indicate at least some positive results from only six sessions of planning-focused treatment for college students with ADHD. The finding of a significant interaction in the inattention subscale and not the hyperactivity/impulsivity subscale is not surprising, given that adults with ADHD are predominantly of the inattentive subtype (Willcutt, 2012). Moreover, planning and organization treatments tend to affect and focus more on the inattention than the hyperactivity/impulsivity domains (Langberg, Epstein, Becker, Girio-Herrera, & Vaughn, 2012).
An unexpected finding was the large pre-post time effects observed in both the intervention and the waitlist control conditions, on the improvement of study skills and objectively measured planning skills and the reduction of internalizing symptoms. With regard to the study skills, the students in both groups indicated to use more test strategies, to have better time-management and more motivation for academic tasks, and to have a better attitude at posttest. Also, in both groups, levels of internalizing comorbidity (in particular, depressive symptoms) decreased. Although these findings are positive, they are surprising as the waitlist students did not receive any intervention focusing on these learning and study skills or internalizing problems.
Several explanations can be put forward for these results. College students with ADHD are higher functioning and may have more learning and skill capacities than those individuals with ADHD who do not make it to college. In the informed consent, all students were given information about the nature of the treatment, as such also those who were after pretest randomized to the waitlist condition knew that the focus would be on enhancing planning and organization of their academic life and work. It may be that merely the fact of enrollment in a study focusing on enhancing these capacities prompts and motivates them toward actually using these skills and capacities, which in turn positively influenced their depressive thoughts. Pointing toward this hypothesis are the large time effects seen in both groups in the subscales reflecting the strategic learning or “will” component of the LASSI (motivation, attitude). These subscales assess the motivation and attitude of students toward studying and learning. Also, with our current design without a placebo or control condition controlling for nonspecific effects and objective measures of the behavior, the large time effects in both groups and our intervention effects may be related to placebo, expectancy effects, rater biases, or nonspecific effects (e.g., attention effects of the test sessions or rater biases; with a more pronounced effect in the intervention group on one of the outcomes).
With regard to the large and significant time effects of both groups on the neuropsychological measure of planning, this effect could be due to practice or learning effects. Other studies also find that repeated assessment with this planning task may enhance performance on this planning task (Boyer et al., 2015), pointing toward learning or practice effects. Although at the start of the study, we anticipated that teaching planning skills in daily life may also influence the performance on a neuropsychological task, in hindsight, one could wonder whether a treatment that focuses on planning skills at a behavioral level (making to do lists, using a daily planner) can alter these neuropsychological functions. The treatment focuses on usage of compensatory strategies for these deficits and may not ameliorate the deficits themselves (Boyer, Geurts, & Van der Oord, 2018). Moreover, performance-based planning measures such as the Tower Test have low ecological validity and do not correlate with questionnaires rated daily life planning deficits (Boyer et al., 2018; Toplak, West, & Stanovich, 2013).
Our study should be interpreted in light of several limitations. First is the amount of missing data primarily due to study dropout, making it impossible to analyze the stability of the effects of our intervention. In a previous study in adolescents with ADHD (Boyer et al., 2015), such high rates of study dropout or intervention dropout were not reported (only 5%). There may be several reasons for this. First of all, in a student’s life, parents play a lesser role in structuring their appointments and daily life than in adolescence, which may explain the difference in dropout between the current study and the study in adolescence. Furthermore, the current study was run in regular student services and without funding; there was no financial compensation for completing assessments or no dedicated research assistant permanently available at the sites to monitor the students and motivate students to come to assessments. As such, the higher study dropout rates may reflect the characteristics of the group but also may reflect the nature and design of our study, or both. The other two RCT’s that have been conducted with an intervention with college students have lower dropout rates (Fleming et al., 2015; LaCount et al., 2018). However, in contrast to our study, one study (LaCount et al., 2018) provided a reward for participation in the intervention (psychology course credit), which indicates that compliance and dropout may have been an issue in their sample as well.
Second, our sample size was lower than we expected (N = 84) by the start of the study (38 per condition; to reach sufficient power [.80] for a large effect size difference with an alpha .01, oversampling for an anticipated 10% dropout; Cohen, 1992). Time restraints and change in policy and cuts in the resources and personnel of the student services forced us to stop the study before the designated N. Nevertheless, our final sample size was adequately using an alpha of .05 (26 per condition; Cohen, 1992) and is higher than most RCTs conducted to date in college students with ADHD (Knouse, 2015), although the final power of our current significant finding was below acceptable norms (.61).
Furthermore, our study was more an effectiveness study than an efficacy study. It was run in regular clinical services without regular supervision for the therapists or intermediate quality control of the interventions given. Although all of them were trained by the first author and trained in providing CBT, and followed supervision sessions for their first college students with ADHD, we cannot ascertain that all therapists were as well equipped and as good in providing the treatment, which may have caused a lack of procedural integrity and reduced intervention effects. However, this makes the results of our study more generalizable to regular student mental health services. Notwithstanding, we did find significant effects on the reduction of inattention (our primary outcome).
Also, a limitation is that due to constraints in time and funding, we did not systematically follow up how many students of the waitlist control condition followed treatment afterward a period of waiting. A further limitation is that although most of the students had a diagnosis of ADHD since childhood and we checked current diagnostic criteria (using the criterion of six symptoms of inattention or hyperactivity/impulsivity) with a semistructured interview that assessed impairment and childhood onset, this information was provided by a single informant (the student) and not systematically cross-checked with another informant.
Finally, it should be noted that with the current nonblinded and subjective assessments it cannot be ruled out that the additional reduction in inattention symptoms for the intervention group may also be due to nonspecific effects of treatment, expectancy, or rater effects. A possibility is also that these scales were significant because of chance effects due to multiple testing, although the specificity of this finding does not point toward these explanations.
Another issue is the length of the intervention, it was quite short (six sessions) compared with other adult-focused (12 sessions; Safren, Sprich, Mimiaga, et al., 2010), college student–focused (eight sessions; Fleming et al., 2015), and adolescent-focused (eight student and two parental sessions; Boyer et al., 2015) planning and intervention programs, whereas length of planning and organization treatment may be related to outcome effectiveness (Schultz, Evans, Langberg, & Schoemann, 2017). However, as the focus of student services is to provide short-term treatment, our results are generalizable to the regular student services offered to many college students with ADHD, and despite the limited length of treatment, we did find significant effects on our primary outcome for the intervention group.
In sum, this short six-session planning and organization intervention that was implemented and tested in regular student services, and thus is highly generalizable to regular practice, had moderate short-term effects on reduction of inattention symptoms for college students with ADHD. Furthermore, both the waitlist and intervention group reported significant short-term gains in their learning and study skills as well as their planning skills, and reductions in their comorbidity, pointing toward the hypothesis of the potential of this higher functioning group of individuals with ADHD to be positively affected by merely enrolling in a study. It should be noted that as compared to the waitlist condition, effects of our intervention were only modest and on one outcome (inattention symptoms), as such further implementing our treatment in its current form does not seem indicated. It also shows the importance of including control conditions in intervention research as when one would analyze the intervention condition on its own, without a comparison, far more positive effects would be reported. To improve effectiveness of our intervention, potentially longer treatment or more practice in daily life (e.g., mentoring sessions alongside the current CBT; for example, as in Anastopoulos & King, 2015; Anastopoulos et al., 2018) is needed.
Supplemental Material
Supplementary_Tables_June4SVDO – Supplemental material for A Randomized Controlled Study of a Cognitive Behavioral Planning Intervention for College Students With ADHD: An Effectiveness Study in Student Counseling Services in Flanders
Supplemental material, Supplementary_Tables_June4SVDO for A Randomized Controlled Study of a Cognitive Behavioral Planning Intervention for College Students With ADHD: An Effectiveness Study in Student Counseling Services in Flanders by S. Van der Oord, B. E. Boyer, Lotte Van dyck, K. J. Mackay, H. De Meyer and D. Baeyens in Journal of Attention Disorders
Footnotes
Acknowledgements
The authors would like to thank the participating students as well as the therapists and participating student services in Belgium (Thomas More University College, KHLIM/UCLL, KU Leuven student services).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Van der Oord was a codeveloper of two cognitive behavioral treatments “Plan my Life” and “Solution Focused Treatment” (no financial interest). Bianca Boyer was also a codeveloper of two cognitive behavioral treatments “Plan my Life” and “Solution Focused Treatment” (financial interest). Other authors declare no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly supported by the research foundation Flanders (FWO) grant (G.0738.14N; only partly for reporting of results/writing paper).
Notes
Supplementary Material
Supplementary material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.