
Abstract
Introduction
ADHD is a debilitating neurodevelopmental disorder that effects approximately 5.5% of children/adolescents worldwide (Erskine et al., 2017). The negative life consequences associated with ADHD can be substantial and result in significant social and economic burden, with more than 65% of children with ADHD developing additional disorders over their lifetime (Harpin, 2005; Shaw et al., 2012). Other associated negative long-term outcomes of ADHD include low self-esteem, poor interpersonal relationships, obesity, poor academic outcomes, low employment prospects, delinquent behavior/substance abuse, and driving violations/accidents (Harpin, 2005; Shaw et al., 2012). Effective treatment for ADHD is available and recommended by the National Institute for Health and Care Excellence (NICE; 2008) in the United Kingdom in the form of psychosocial parent training for young children (below 6 years of age), and psychopharmacological, or multimodal treatment for older children. Many of the associated risks are significantly greater for individuals with untreated versus treated ADHD (Shaw et al., 2012). Early signs of ADHD can be detected in preschool children aged 3 years or younger (Arnett, Macdonald, & Pennington, 2013; Harpin, 2005), and early and accurate identification of those in need of help can minimize the long-term negative effects (Halperin, Bedard, & Curchack-Lichtin, 2012; Sonuga-Barke, Koerting, Smith, McCann, & Thompson, 2011).
Yet, not all children who may benefit from treatment receive the help they need. Although there are ongoing debates about over- or underrecognition and/or misdiagnosis of ADHD (Sciutto & Eisenberg, 2007; Timimi & Taylor, 2004), in many countries, administrative prevalence rates (the numbers with a clinical diagnosis) are far below figures found in epidemiological studies suggesting an overall trend for underidentification. In the United Kingdom, for instance, actual prevalence of ADHD in the community is approximately 2% (Ford, Goodman, & Meltzer, 2003), whereas administrative prevalence is less than 1% (Holden et al., 2013). The disparity between actual rates of ADHD in the community and the numbers diagnosed and treated in clinics is substantially larger for females than males, particularly in those below 18 years of age (Holden et al., 2013). Male to female prevalence rates of ADHD are approximately 2:1 in community samples (Willcutt, 2012). In the United Kingdom, the prescribing pattern for male versus female patients with ADHD is estimated at 5.5:1 (for those aged between 6 and 12 years of age; McCarthy et al., 2012). This suggests a substantial shortfall in the referral of young females with ADHD. Yet, the functional long-term impact of ADHD is equally debilitating for females as it is for males (Quinn & Madhoo, 2014; Rucklidge, 2010) and treatments are equally effective (Sharp et al., 1999).
Because parents and teachers play an essential role in the referral process (Ford et al., 2003; NICE, 2008; Sayal, Taylor, Beecham, & Byrne, 2002), research into why females appear to be disproportionately underrepresented in clinical populations has focused on the way that adults react to female and male ADHD symptoms differently. One explanation of this is that parents and teachers see ADHD in males as more clinically serious than ADHD in females because the male presentation of ADHD is typically more overt and disruptive in nature than the female presentation of ADHD (Gaub & Carlson, 1997; Sciutto, Nolfi, & Bluhm, 2004). This in turn might lead to males being more readily referred than females. Indeed, it has been reported that ADHD in males is more likely than in females to present as hyperactivity/impulsivity and be accompanied by externalizing disorders (oppositional defiant disorder and conduct disorder); whereas ADHD in females is likely to take an inattentive form and be accompanied by internalizing disorders (anxiety and depression; Gaub & Carlson, 1997; Gershon, 2002; Quinn & Madhoo, 2014). Consistent with this, several studies have provided evidence of sex differences in ADHD behavior. For example, Abikoff and colleagues (2002) demonstrated sex-specific differences in observed classroom behavior in females and males who met parent-reported ADHD Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria (Abikoff et al., 2002).
A second explanation of such differences, that does not necessarily contradict the first, is that even if male and female presentation is the same, parents and teachers may respond to it differently because of gender-specific expectations for, and stereotypes of, behavior (Biederman et al., 2005). The media representation of ADHD as predominantly male (Horton-Salway, 2013) may contribute to a cultural expectation bias that leads to an underidentification of ADHD symptoms in females (Biederman et al., 2005; Williamson & Johnston, 2015). This could be because adult referrers are simply less sensitive to ADHD behaviors in females compared with males. Alternatively, they may unknowingly adopt a different threshold for assessing male and female ADHD, which may lead to an underestimation of female symptom severity.
Attempts to compare adult responses to the same ADHD behaviors in males and females have typically used standardized vignettes describing symptoms of the DSM presentation categories (inattentive, hyperactive/impulsive, combined) ascribed to either a male or female name. Such studies have reported mixed findings. One study found that teachers rated females as more highly impaired and in need of intervention than males, at least in response to descriptions of hyperactive and impulsive behavior (Coles, Slavec, Bernstein, & Baroni, 2012), whereas another study reported no evidence of sex differences (Moldavsky, Groenewald, Owen, & Sayal, 2013). Using the vignette methodology, teachers (Ohan & Visser, 2009; Sciutto et al., 2004) and parents (Ohan & Visser, 2009) have indicated a greater likelihood to seek further evaluation/intervention for males with ADHD symptoms than females with ADHD symptoms, even though symptomology and impairment descriptions were exactly the same (Ohan & Visser, 2009; Sciutto et al., 2004).
However studies relying on teacher/parent responses to vignette-based descriptions lack ecological validity as they may not adequately reflect, or capture ADHD behaviors in a natural setting. In the study reported in the current article, we adopted an alternative approach that directly compared adult ratings of ADHD against actual ADHD behaviors directly observed in the classroom. This involved a secondary analysis of historical data drawn from a study originally conducted to assess the effects of food additives on 3- to 4-year-old and 8- to 9-year-old children within the community (McCann, et al., 2007). For the purposes of the analysis reported here, the sample was divided into three groups based on directly observed ADHD behaviors reported by blinded assessors in the classroom using a validated ADHD observation measure—the Classroom Observation Code (COC; Abikoff & Gittelman, 1985), creating low, moderate, and high COC groups. The expectation being that within these groups, males and females would be roughly matched for levels of actual observed ADHD behaviors. Low, moderate, and high groups were then compared on parent and teacher ADHD reports using clinical rating scales.
We tested two hypotheses:
We expected this to be reflected in a significant interaction between COC group and sex on parent/teacher ratings.
We expected this to be reflected in a main effect of sex with higher adult ratings in males than in females irrespective of COC group.
Two design features make this data set especially valuable. First, the study was not restricted to clinical cases: Data came from a population-based sample representing the full range of classroom ADHD behaviors and was therefore free of the biases and constraints created by the referral process of a clinical population.
Second, it contained two distinct age groups covering the preschool and school-aged periods. This is important because it has been argued that differences in the biological/maturational processes between the sexes mean that the presentation of ADHD symptoms may be different for boys and girls during different developmental periods (Mahone & Wodka, 2008; Nussbaum, 2012). A delay in the expression of ADHD symptoms in females might explain evidence of a trend for later referral and diagnosis in females versus males by which time symptoms are more pronounced (Quinn & Madhoo, 2014; Rucklidge, 2010). In addition to an examination of the sex-based relationship between ratings and observed behavior, we were also able to compare the numbers of males versus females displaying different levels of observed ADHD behavior (i.e., in terms of the proportion of male vs. female membership of the low/moderate/high COC groups), examine whether females displayed lower levels of ADHD behaviors in the classroom within these groups in comparison with males, and also examine whether these patterns varied as a function of age.
Method
The data reported here were obtained from a study of the effect of food additives on children’s behavior (McCann et al, 2007). The variables analyzed came from the baseline measures obtained from observers, teachers, and parents of children who participated in the food-additive trial before any food intervention had taken place. They are therefore representative of the full range of behavior normally seen in these age groups.
Participants
The sample of preschool children from the original food-additive trial was drawn from a community population of children aged between 3 years and 4 years 2 months registered in early years settings (nurseries, day nurseries, preschools, playgroups) within the Southampton City Council area. The older sample from the food-additive trial was drawn from children aged between 8 and 9 years attending schools within the city of Southampton. The samples were representative of the full range of socioeconomic background of the community, as the number of participants receiving free school meals (an index of social disadvantage) was proportional to the city as a whole. Historical data from a total of 153 children aged 3 to 4 years and 144 children aged 8 to 9 years were included in the current analyses. The younger males had a mean age = 43.5 months (SD = 4.6) and the younger females’ mean age = 43.4 months (SD = 4.4). The older males had a mean age = 106.4 months (SD = 6.1) and the older females’ mean age = 106.1 months (SD = 5.8). There were no significant differences by sex according to age of the children in these groups.
Measures
Direct measures of ADHD behaviors
In both age groups, actual ADHD behavior was directly observed using the COC (Abikoff & Gittelman, 1985), recommended for ADHD screening and diagnosis (Volpe, DiPerna, Hintze, & Shapiro, 2005). The occurrence of 12 mutually exclusive behaviors (noncompliance, physical aggression, verbal aggression to other children, verbal aggression to teacher, interference with other children, out of chair, off-task, minor motor movement, gross motor standing, gross motor, solicitation of teacher, absence of behavior) was evaluated and scored by trained independent researchers. Observations occurred during a range of on- and off-task (switching) activities as part of the data collection for the original food-additive trial. The interrater reliability of scores, using the standardized procedures of the COC, was tested prior to the start of the study and then in mid-study, and exceeded .87. For the purposes of this study, the baseline score of each child prior to food-additive treatment was used. The observed ADHD behavior score for the COC was obtained by summing the number of times each of the 12 behaviors were observed in the 24 mins of observation for the week, that is, the total summed across the three observation periods.
Parent and teacher ratings of ADHD behaviors
For the 3- to 4-year-old children, the Abbreviated ADHD Rating Scale–IV (Teacher version; DuPaul, Power, Anastopoulos, & Reid, 1998; DuPaul et al., 1997) was completed by the early year setting practitioner who described the frequency of the specific behaviors displayed over the past week. A total score (max of 30) was obtained for 10 (inattentive five items, hyperactive five items) of the 18 items in this questionnaire. Examples of questions included in the abbreviated teacher version were “fails to give attention to details or makes careless mistakes in schoolwork”, “does not follow through on instructions and fails to finish work”, “has difficulty organizing tasks and activities”, “is on the go or often acts as if “driven by a motor””, “talks excessively”, and “blurts out answer before questions have been completed”. Parents were asked to complete the Abbreviated Weiss–Werry–Peters (WWP) Activity Scale (Routh, 1978) to assess ADHD symptoms in preschool children. Items on this scale include “switching activities”, “poor concentration”, “always on the go”, and “interrupting or talking too much”. Interparent agreement of the WWP is good (r = .82; Mash & Johnston, 1983). Parents rated their child’s behavior over the previous week on seven items and a total score was obtained.
For the 8- to 9-year-old children, teachers completed the 10-item (max score of 30) Abbreviated ADHD Rating Scale–IV (teacher version) described above and parents completed a parent version of the same Abbreviated ADHD Rating Scale–IV (DuPaul et al., 1998; DuPaul et al., 1997). Examples of questions included in the abbreviated parent version include - “fails to give attention to details” or “makes careless mistakes in schoolwork”, “runs about or climbs excessively in situations in which it is inappropriate”, “does not follow through on instructions” and “fails to finish work”, “has difficulty organizing tasks and activities”, “is “on the go” or often acts as if “driven by a motor””, “avoids tasks (e.g., schoolwork, homework) that require sustained mental effort”, and “talks excessively”.
Each parent/teacher rating was collected for each week of the study, but only the baseline scores were used in the current data analysis.
Statistical Analysis
To test our two hypotheses, we conducted secondary analyses of the historical data described above. The overall sample population of each age-group was divided into three groups corresponding to tertiles of directly observed ADHD behaviors derived from the COC (low, moderate, and high COC groups). First, we tested whether there were different proportions of males and females in the COC groups. Second, we tested whether the sexes differed in their levels of observed ADHD behavior once they had been allocated to their COC group membership—that is, were low, moderate, and high COC group females observed to have similar levels of observed ADHD to their male counterparts? Third, sex and COC group were entered as independent variables in four two-way ANOVAs with parent and teacher ratings as the dependent variable. Each ANOVA addressed a different age and rating source combination (i.e., parent, 3- to 4-year-olds; teacher, 3- to 4-year-olds; parent, 8- to 9-year-olds; teacher, 8- to 9-year-olds). In each case, we predicted that if parents or teachers were better able to rate ADHD in males than females (Hypothesis 1), there would be a significant interaction between COC group and sex. We expected that/adult ratings for males would show consistency with the increased severity of COC group; whereas group differences in adult ratings for females would be less marked - or inconsistent with the direction of severity of COC group. In addition, if males’ behavior was rated as more serious/severe than that of females (Hypothesis 2), we would expect a main effect of sex, with males rated as having significantly more ADHD behaviors than females within COC groups of equivalent severity.
Results
The social–economic status (SES) of the families included in the study were assessed according to categories used by U.K. National Statistics (Hall, 2006): high (managerial role/professional), intermediate (self-employed), and low (routine work). There were no statistically significant associations with sex of child and maternal or paternal SES in either 3 to 4-year-old (χ2 = 1.07 df = 3, p = .78) or 8- to 9-year-old populations (χ2 = 4.31, df = 3, p = .37).
The COC scores for children aged 3 to 4 years ranged from 3 to 91, with an overall mean of 25.87 (SD = 13.86). For children aged 8 to 9 years, observed COC scores ranged from 3 to 197 with an overall mean of 37.24 (SD = 21.84). There were significant sex differences in the distributions across COC groups, with significantly more males in both age bands in the high group (see Table 1).
Sex Differences in the Proportion of Individuals Within the Observed COC Groups.

Note. COC = Classroom Observation Code.
The COC group means of directly observed ADHD behaviors for males and females are presented in Figure 1. There was a highly significant effect of group for both 3- to 4-year-olds and for 8- to 9-year-olds. There were no significant effects of sex (or any interactions with sex). As can be seen, males and females were well matched for levels of observed ADHD ratings within each group (Figure 1).
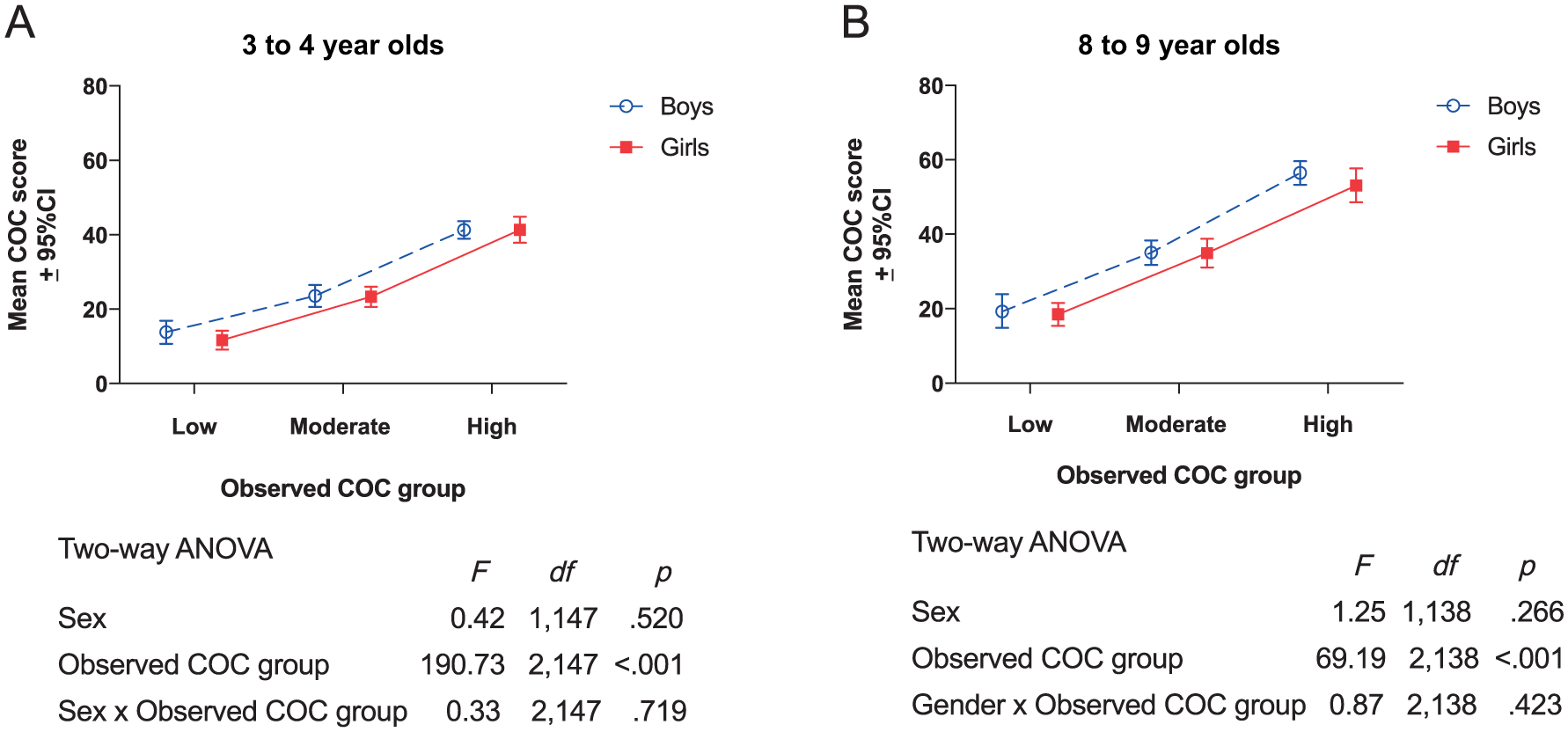
Mean (± 95% CI) COC scores for males and females by observed COC group for 3- to 4-year-olds and 8- to 9-year-olds.
Figure 2 illustrates outcomes and analysis of parent and teacher ratings of ADHD behaviors according to sex and COC group status for 3- to 4-year-olds and 8- to 9-year-olds.
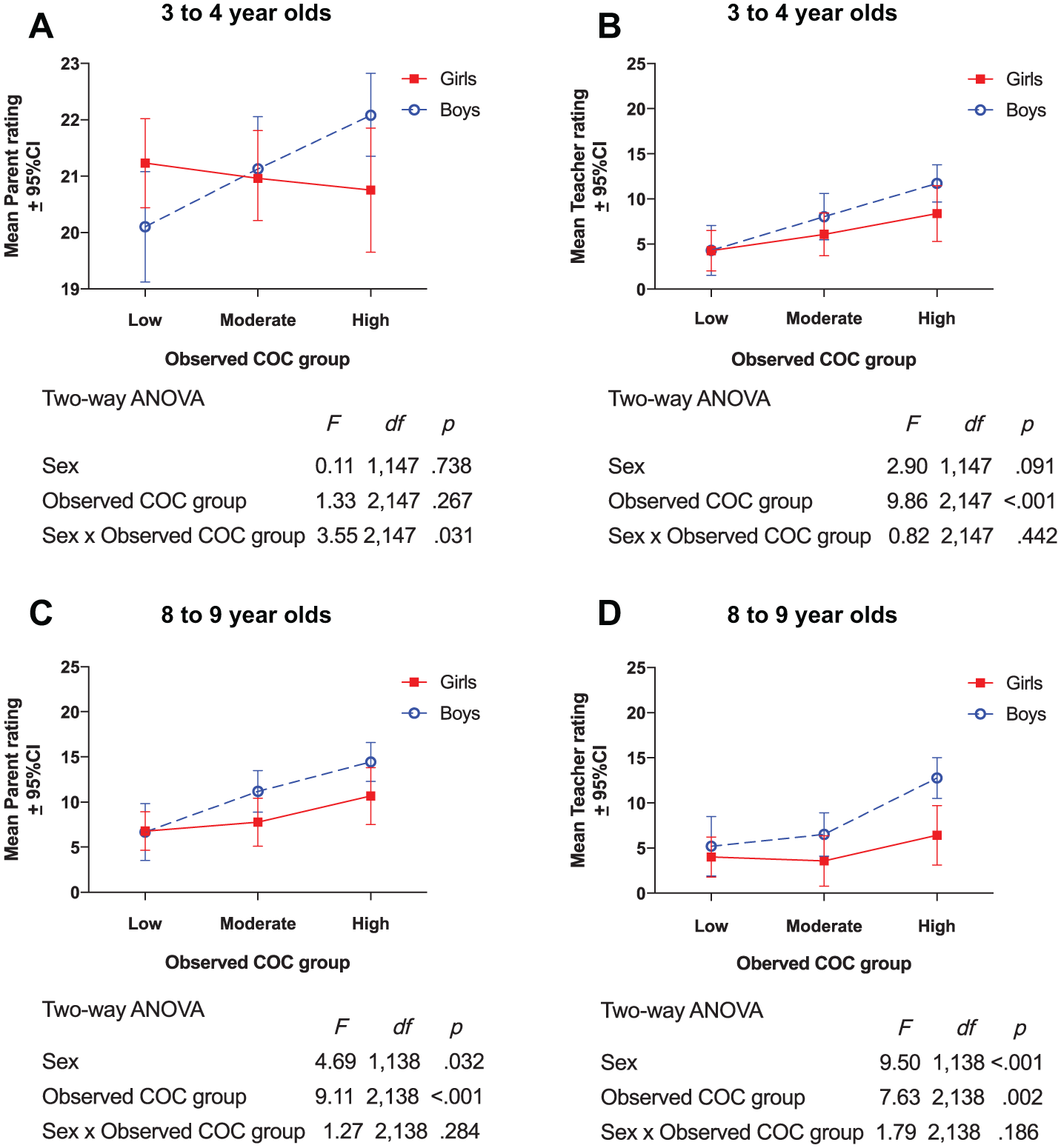
Mean (± 95% CI) parent and teacher ratings for males and females by observed COC group for 3- to 4-year-olds and 8- to 9-year-olds.
Parent WWP scores for 3- to 4-year-olds ranged from 6 to 28, with a mean score of 21.17 (SD = 2.27). For this outcome measure, there was no main effect of COC group, or sex. There was a significant sex × group interaction (p = .031). Parent ratings of males increased significantly across the low, moderate, and high COC groups (one-way ANOVA, F = 5.98, df = 2, 76, p = .004); whereas there was no COC group effect in parent ratings of females in this age group (one-way ANOVA, F = 0.23, df = 2, 71, p = .798; Figure 2a). Parent ADHD rating scores in the 8- to 9-year group ranged from 0 to 28 with a mean score of 9.88 (SD = 6.78). Teacher ADHD rating scores ranged from 0 to 27, with a mean score of 7.34 (SD = 6.78) for 3- to 4-year-olds and 0 to 29 with a mean score of 6.74 (SD = 7.18) for the 8- to 9-year-olds. There was no COC Group × Sex interaction effect for these three outcome measures. However, there was a main effect of sex for them all (Figure 2b, 2c, and 2d). This was clearest in the older children where the effect was significant for both teacher and parent ratings, with ratings for males being significantly higher than for females on both parent (F = 4.69, df = 1, 138, p = .032) and teacher (F = 9.5, df = 1, 138, p < .001) ratings (Figure 2c and 2d). The effect of sex for teacher ratings in the 3- to 4-year-olds was in the same direction but failed to reach significance (Figure 2b; p = .091).
Discussion
In the current article, we tested two hypotheses about the nature of systematic sex-related biases in adult ratings of ADHD—by comparing those ratings across groups defined in terms of directly observed ADHD classroom behaviors in a secondary analysis of existing population-based samples. The first hypothesis was that adults are less able to rate female compared with male ADHD. The second was that females are systematically rated as less severe than males—even when they have the same level of directly observed behavior. There were a number of findings of interest.
First, as expected, there were more males categorized in the high COC groups (i.e., those with high levels of directly observed ADHD classroom behaviors). More than 40% of males compared with 22% of females were in the high COC group. This pattern is consistent with prevalence data from epidemiology studies that indicate a greater proportion of males than females typically display elevated symptoms of ADHD in community samples within these age groups (Willcutt, 2012). However, because inattentive/internalizing behaviors predominate among the female ADHD presentation (Gaub & Carlson, 1997; Gershon, 2002; Quinn & Madhoo, 2014), it has been argued that standardized screening measures/rating scales may inadvertently be biased toward the typical male presentation—adding to the female underreferral problem (Soffer, Mautone, & Power, 2008). This is reflected in the greater focus on hyperactive/aggressive behaviors versus inattentive behaviors in COC coding, which may have contributed to an overrepresentation of males in the high COC groups here.
Second, there was no evidence of age-related changes in sex differences in prevalence. The proportions of males and females within each COC group in this study were similar for 3- to 4-year-olds and 8- to 9-year-olds alike (Table 1). Consequently, these data do not provide evidence of gendered maturational differences in the trajectory of ADHD behaviors (Mahone & Wodka, 2008; Nussbaum, 2012)—at least not within the age groups studied here.
Third, and crucially for our interpretation of potential adult rating sex differences, there were no sex differences in directly observed behaviors within the COC groups. Males and females showed comparable levels of ADHD behaviors within their respective groups (low/moderate/high; Figure 1).
Fourth, as we predicted in relation to Hypothesis 1, there was some evidence that adults’ ratings reflected observed ADHD status less well in females than males—at least for parents of the younger children. Figure 2a shows that parent ratings for males but not females increased across COC groups in line with increases in directly observed behaviors. This effect was not present for ratings of older children (2c). One explanation is that the WWP (the parental rating scale used for the 3- to 4-year-olds) mainly includes items relating to hyperactivity/impulsivity and only one relates to inattention—and therefore was less reflective of the predominant feature of female ADHD. However, as noted above, the COC measure also focused predominantly on hyperactive/externalizing behaviors, so the female observed COC ratings were unlikely to be elevated by predominantly inattentive behaviors. In previous studies, the WWP has been shown to reliably identify children at risk of later ADHD (Sonuga-Barke, Thompson, Stevenson, & Viney, 1997), and a prospective longitudinal study of preschoolers in a community setting found similarly elevated symptoms of hyperactivity in males and females based on WWP scores (Smith et al., 2016). However, the Smith et al. (2016) study also showed that preschool hyperactivity in males was more strongly associated with mental health risks in late adolescence/adulthood, which suggests that preschool hyperactivity (as reported by parents) is not a reliable precursor to later ADHD symptoms in females (Smith et al., 2016). Our study suggests that this finding may be due to reduced parental sensitivity to hyperactivity in females versus males. Indeed, it has been previously argued that an oversight of hyperactive symptoms in females may contribute to the reported predominance of inattentive versus hyperactive behaviors in females (Weiss, Worling, & Wasdell, 2003). A further consideration is that the parent ratings of the child will largely be based on the behavior within the home setting, whereas the observed ratings were based on behavior within the school setting.
Consequently, the Sex × Group interaction which was specific to parent (not teacher) ratings in the younger population alone may indicate that preschool female behavior differs to a greater extent than males within the home versus school environment. Home versus school behavior is therefore an area for future exploration in relation to the potential contribution to the underidentification and underreferral of young girls with ADHD (Nussbaum, 2012; Soffer et al., 2008), particularly in light of the significant role of parents and teachers (Ford et al., 2003; NICE, 2008; Sayal, Ford, & Goodman, 2010).
Fifth, our results suggest a striking tendency in the older group of children for both parents and teachers to consistently “under-rate” ADHD in females compared with males—at least in contrast to directly observed classroom behavior. This was consistent with our second hypothesis that parents and teachers systematically underestimate the levels of ADHD behaviors for females in comparison with males, which was particularly evident for the 8- to 9-year-old children in the high COC group. There are a number of possible explanations for this effect. Adult ratings may have been influenced by the type of predominant ADHD symptoms or differences in non-ADHD behaviors that have previously been argued to contribute to the underreferral and undertreatment of school-aged females (Quinn & Madhoo, 2014; Rucklidge, 2010). As males with ADHD typically display more overtly aggressive behavior than females with ADHD (Rucklidge, 2010), there is a possibility that the observed COC scores were influenced by greater levels of aggressive behavior in males than in females in this study. Thus, the lower adult ratings for females versus males may reflect an oversight of less obtrusive ADHD behaviors in females, or a bias in the raters’ perception of the severity of male versus female ADHD behaviors, or even a combination of these factors. Regardless of the reason, these findings highlight an important area of concern, not least because those children in the high COC group are more likely than those in the moderate or low groups to include children reaching clinical levels of ADHD (although clinical status was not assessed in the original collection of the data).
There are some limitations to the reported analysis. First, it involved a secondary analysis of existing data—Therefore, the data were not collected with this analysis in mind. Consequently, the abbreviated version of the measures used in the original study prior to intervention did not include all the items. This limits the possibility to conduct further exploratory data analyses of the observed sex differences, particularly in relation to predominant symptoms of inattentiveness versus hyperactivity/impulsivity or aggressive behaviors. However, recent studies using structural equation modeling to evaluate factor loadings of the specific DSM features of ADHD have concluded that ADHD is best conceived on the same general continuum rather than as distinctive subtypes in preschool children (Arias, Ponce, Martinez-Molina, Arias, & Nunez, 2016). Furthermore, structural equation models that have evaluated the role of sex have established invariance between the sexes in relation to factor loadings in preschool populations (Arias et al., 2016) in older children (Caci, Morin, & Tran, 2016; Dumenci, McConaughy, & Achenbach, 2004) and in adults (Gibbins, Toplak, Flora, Weiss, & Tannock, 2012), suggesting that items relating to ADHD in males and females are measuring the same thing.
Second, all ratings—including observational scales—are subject to bias, such as halo effects (i.e., influenced by prior beliefs about the condition/treatment; Gualtieri & Johnson, 2005), so it cannot be assumed that the observed data were immune to gender bias. However, the COC scores were collected by objective observers in the original food-additive trial, extensively trained in the use of the instrument with an interrater reliability of >.87 (McCann et al., 2007). Furthermore, any impact of bias based on socially stigmatized predominantly male representations of ADHD (Horton-Salway, 2013) does not fit with increased observational scores of females and not males (which would explain the pattern of observed vs. rating results), so if there was an impact of bias, it seems more likely to be reflected in the adult ratings of higher male versus female scores.
Potential rater bias resulting either from family SES or sex of rater was not controlled for in the analyses. However, there was no association between the SES of the families (based on employment classification; Hall, 2006) in either younger or older children according to sex of child. Although the population samples included in this study represented SES slightly below the national average of the general population (according to comparable figures from the Office for National Statistics), one would expect young parents early in their working lives to be slightly below the national average. Together with evidence that the number of participants receiving free school meals (an index of social disadvantage) were also representative of the city as a whole, we believe our population was representative of the social spectrum and did not differ between male and female samples. Likewise, the sex of the rater did not differ between male and female samples. The trained observers were all female. Teachers were also predominantly female (above 80%) and nearly all of the parent ratings were completed by mothers. There is a possibility that male and female raters may reflect differential biases according to the sex of the child, but this consideration was beyond the scope of this analysis. Certainly, there is evidence that the interpersonal relationship between the child and the rater does influence ADHD rating scores (Mikami, Chi, & Hinshaw, 2004), so the impact of gendered social skill abilities and coping mechanisms (Novik et al., 2006; Quinn & Madhoo, 2014) in relation to adult ratings also warrants investigation in future studies.
Third, the observations were conducted within a preschool or school setting, so did not take account of behavior that may be susceptible to change in different environments/settings. Ratings by parents/teachers are likely to be influenced by their knowledge of the child, either at home or in the playground, so their rating scores may have reflected behaviors outside of a classroom setting, which the observational scores would not. Because evidence of behavior across settings is a requirement of a clinical diagnosis of ADHD (NICE, 2008), this study identifies a potential link to the underrecognition or underdiagnosis of ADHD in females versus males.
Given that unrecognized and undersupported ADHD is equally debilitating for females as males (Quinn & Madhoo, 2014; Rucklidge, 2010) and females with ADHD are at higher risk of self-harm and suicide than their non-ADHD peers (Hinshaw et al., 2012), these findings highlight potential directions for future investigation. Further research is required to establish whether females presenting with ADHD behaviors within a classroom setting demonstrate greater social skills/coping strategies, or present less obvious ADHD behaviors outside of the classroom than their male counterparts—contributing to a systematic oversight of ADHD in females. As indicated above, it is unknown how many of the population included in this study had a confirmed diagnosis of ADHD. However, using a nonclinical community sample is a strength of the study as it allowed direct comparison of the full spectrum of ADHD behavior in males and females alike.
Summary/Concluding Remarks
Despite the limitations posed by this secondary analysis (discussed above) that preclude the opportunity to explore specific reasons for the reported sex differences, our findings highlight two potential reasons why ADHD in females may be underestimated in ratings of teachers and parents. First, for the young age group, parent ratings of girls were not consistent with levels of directly observed behaviors—suggesting that parents may be less sensitive to the ADHD behaviors of females. Second, that in the older group, parents and teachers rated high levels of ADHD behaviors in females lower than males who demonstrated comparable ADHD levels within the classroom setting. These results are consistent with explanations of a gender bias in the recognition of symptoms of ADHD that have been argued to contribute to the underreferral and undertreatment of females (Biederman et al., 2005), rather than theories of maturational processes that differentially affect the developmental course of the symptoms of ADHD between the sexes (Arnett et al., 2013; Mahone & Wodka, 2008). Given the need for early identification to optimize treatment outcomes and limit the long-term negative effects of ADHD, regardless of sex, our results indicate that a potential systematic underestimation of ADHD symptoms by parents and teachers for females within a classroom setting in comparison with males warrants further exploration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.J.M. and J.S. have no conflict of conflicts of interest. E.J.S.S.-B. has received speaker fees, consultancy, research funding, and conference support from Shire Pharma and speaker fees from Janssen Cilag. He has received consultancy fees from Neurotech Solutions, Aarhus University, Copenhagen University and Berhanderling, Skolerne, Copenhagen, KU Leuven, and book royalties from Oxford Univeirsty Press and Jessica Kingsley. He is the editor-in-chief of the Journal of Child Psychology and Psychiatry for which his University receives financial support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data in this article were obtained in a study funded by the Food Standards Agency (Grant T07040).