
Abstract
Introduction
ADHD is a well-known neurodevelopmental disorder that persists into adulthood (Barkley, Fischer, Smallish, & Fletcher, 2006). Literature has clearly documented neuropsychological deficits in children (Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005) as well as in adults (Alderson, Kasper, Hudec, & Patros, 2013; Schoechlin & Engel, 2005) with ADHD. Although not all individuals with ADHD have neuropsychological deficits (Seidman, 2006), some neuropsychological deficits, especially those subserved by prefrontal brain regions (Sonuga-Barke, 2005), are viewed as endophenotypes (Castellanos & Tannock, 2002) of ADHD and might play a valuable role in validating the psychiatric diagnosis (Hyman, 2007).
Since long ago, there had been criticisms about the arbitrary decision of the age-of-onset criterion for diagnosing ADHD (Barkley & Biederman, 1997; Kieling et al., 2010) and the developmentally inappropriate symptoms as well as symptom threshold in adult populations (Faraone et al., 2000; Tannock, 2013). Longitudinal studies gave conflicting data about the general age range of emerging ADHD symptoms: Some showed that only a small proportion of individuals developed impairing ADHD symptoms after 7 years old (Polanczyk et al., 2010; Todd, Huang, & Henderson, 2008), while others found that more than 10% of individuals with ADHD developed after 7 years old (Applegate et al., 1997; Todd et al., 2008). Diagnosing adult ADHD requires a recall of childhood symptoms (Adler & Chua, 2002) and inevitably suffers from recall bias (Barkley, Fischer, Smallish, & Fletcher, 2002). Individuals with ADHD and their parents frequently reported later ages of onset during the follow-up interviews than their initial reports (Todd et al., 2008). Only half of adults with ADHD recalled their symptom onset before 7 years (Kessler et al., 2005). Therefore, even only a small number of individuals develop ADHD after 7 years old, the possible recalled bias of ADHD onset for adolescents and young adults (Todd et al., 2008) will also result in underrecognition of ADHD in the adult population (Kieling et al., 2010). Adults with unrecognized ADHD often experience various negative life events and have adverse outcomes (Barkley et al., 2006).
Several studies provided evidence to support the revision of ADHD age-of-onset criterion by showing comparable familial transmission, comorbidity pattern (Faraone, Biederman, Spencer, et al., 2006), functional impairment (Rohde et al., 2000; Willoughby, Curran, Costello, & Angold, 2000), impaired neuropsychological functions (Faraone, Biederman, Doyle, et al., 2006), and treatment response (Biederman et al., 2006; Reinhardt et al., 2007) between groups of different ages of onset, naming, by and after 7 years old, of ADHD. Therefore, the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) criteria for ADHD elevate the age-of-onset threshold from 7 to 12 years and lower the symptom threshold from 6 to 5 at each symptom domain for individuals aged 17 years and older (American Psychiatric Association, 2013). After DSM-5 formally published, Chandra, Biederman, and Faraone (2016) reported comparable impairments in quality of life and social adjustment, and similar patterns of psychiatric comorbidity and familial transmission between late-onset ADHD and Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) ADHD. Vande Voort, He, Jameson, and Merikangas (2014) reported that using DSM-5 criteria caused a moderate increase of prevalence (from 7.38% to 10.84%) as compared with DSM-IV criteria despite no significant difference in severity and comorbidity between the earlier and later onset groups. Concerns about overinflating ADHD diagnosis by DSM-5 (Batstra & Frances, 2012; Prosser & Reid, 2013) still call for further studies to validate the new criteria.
Following our previous findings of no difference in functional impairment, quality of life (Lin, Lo, Yang, & Gau, 2015), and psychiatric comorbid conditions (Lin, Yang, & Gau, 2016) between the early- and late-onset adult ADHD groups, this work intended to compare neuropsychological functioning between adults with early- and late-onset ADHD diagnosed by DSM-5. Although such an issue had been investigated by Faraone, Biederman, Doyle, et al. (2006), their work did not address the influence of psychiatric comorbidities on the neuropsychological performance, and most of their neuropsychological tasks were verbally dependent. Visuospatial memory and central executive functions are more closely related to ADHD behavioral symptoms than verbal memory (Alderson et al., 2013). Functional neuroimaging studies also demonstrated that frontoparietal network and visual system subserving visuospatial (working) memory (Klingberg, 2006) and attention (Hart, Radua, Nakao, Mataix-Cols, & Rubia, 2013) have altered activity in adults with ADHD in addition to the frontostriatal network (Cortese et al., 2012; Vaidya, 2012). Therefore, we believe visual tasks are highly correlated to ADHD diagnosis with the level of correlation no less than the verbal ones.
There are several overlapping symptoms between depressive disorders, anxiety disorders, and ADHD, such as inattention, forgetfulness, restlessness, and impulsiveness. Besides, neuropsychological deficits frequently found in ADHD, including deficits in executive functions, working memory, visuospatial memory, psychomotor processing speed, and verbal fluency, are also found in major depressive disorder (Baune, Fuhr, Air, & Hering, 2014) and oppositional defiant disorder (ODD)/conduct disorder (CD; Lin & Gau, 2017; Sergeant, Geurts, & Oosterlaan, 2002). Previous studies either excluded individuals with psychiatric comorbidity (Schoechlin & Engel, 2005) or only adjusted for overall psychiatric comorbidity (Gau & Huang, 2014; Seidman, Biederman, Weber, Hatch, & Faraone, 1998) while investigating neuropsychological functioning in ADHD. Given that adults with ADHD frequently have psychiatric comorbidities (Biederman et al., 1993) which may cloud the diagnosis of adult ADHD (Shaffer, 1994), controlling for a specific comorbidity one at a time is suggested to remove the influences of comorbidities on the neuropsychological deficits found in ADHD (Hervey, Epstein, & Curry, 2004; Schoechlin & Engel, 2005).
The Cambridge Neuropsychological Test Automated Battery (CANTAB) is a widely used measure to assess various nonverbal neuropsychological functioning (Levaux et al., 2007) with good reliability and validity (Luciana, 2003). Combining our previous studies and others’ studies, we found that many tasks in CANTAB could differentiate children (Fried, Hirshfeld-Becker, Petty, Batchelder, & Biederman, 2015; Rhodes, Coghill, & Matthews, 2005) and adolescents (Gau, Chiu, Shang, Cheng, & Soong, 2009) with ADHD from typically developing youths, including high-executive demand tasks, such as Spatial Working Memory (SWM), Stocking of Cambridge (SOC), Intradimensional and Extradimensional Shifting (IED), and low-executive demand tasks, such as Rapid Visual Information Processing (RVP), Reaction Time, and Spatial Span. Besides, previous studies suggested that neuropsychological functions measured by SWM, SOC, IED, Spatial Span (Gau & Shang, 2010), and RVP (Gau & Huang, 2014) in CANTAB might be the endophenotypes of ADHD. Therefore, if adults with late-onset ADHD also have similar neuropsychological deficits measured by the CANTAB as adults with early-onset ADHD and these deficits are independent of any specific psychiatric comorbidity, late-onset ADHD might be within the spectrum of ADHD.
In this study, we selected the neuropsychological tasks assessing visual sustained attention (RVP), short-term spatial memory (Spatial Span), spatial working memory (SWM), set-shifting (IED), and visual planning (SOC), which were sensitive to frontal lobe dysfunction (Owen, Doyon, Petrides, & Evans, 1996), for analysis. To investigate the neuropsychological performance of ADHD regarding age-of-onset, we divided participants into three groups: (a) ADHD with early-onset (onset by 7 years old); (b) ADHD with late-onset (onset between 7 and 12 years old); (c) non-ADHD controls. We expected that adults with ADHD would have significant neuropsychological deficits regardless of the recalled age of onset and the psychiatric comorbidity.
Method
Participants and Procedure
We recruited adults (aged 17 years and older) who met the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) diagnostic criteria for ADHD and subthreshold ADHD (five symptoms out of nine inattention or/and hyperactivity/impulsivity symptoms or age of onset after 7 years) during 2010-2014 at Department of Psychiatry, National Taiwan University Hospital (NTUH), Taipei, Taiwan. There were two sources of the participant recruitment. First, new cases of adult ADHD were recruited by advertisement or referred by psychiatrists or family physicians (new recruitment sample). They first received telephone interview by a trained psychologist using the modified adult ADHD supplement of the Chinese versions of the Kiddie Schedule for Affective Disorder and Schizophrenia–Epidemiological Version (K-SADS-E; Gau & Chang, 2013). After the telephone interview, those who were suspected of having the diagnosis of ADHD and their parents and/or partners were invited. Second, adults with medical documents of childhood ADHD at NTUH who possibly met the DSM-5 criteria for adult ADHD at the time of recruitment were invited (clinical follow-up sample). These adults first came to our clinic when they were 6-10 years old, and they and their parents received clinical evaluation and a formal diagnostic interview. All of them were followed up in the Department of Psychiatry, NTUH with a medical document of their psychopathology, treatment, difficulties, and improvements.
After signing the informed consent, all the participants received formal psychiatric diagnostic interview as well as the Conners’ Adult ADHD Diagnostic Interview (Conners, Erhardt, & Sparrow, 1999) by the corresponding author. Then they received the modified adult version of the ADHD supplement (Gau & Chang, 2013; Lin et al., 2015; Lin et al., 2016) of the K-SADS-E (Gau, 2007) and SADS (Ni, Lin, Gau, Huang, & Yang, 2017) for childhood/current diagnosis of ADHD and other psychiatric disorders, respectively, by the trained interviewers. The interviewers were all blind to the sources of referral. Among adults with ADHD, 93 (43.5%) had been diagnosed with ADHD at childhood with valid medical records at the same hospital, and 121 (56.5%) were recruited by advertisement and referral. Through advertisement on the Internet, newspaper, and posters at the colleges and public places, we recruited adult controls according to the age and sex distributions of the ADHD group. Participants in the control group received the same clinical and psychiatric evaluations as adults with ADHD to ensure that they did not have lifetime or current diagnosis of ADHD.
Participants were excluded if they had any systemic medical illness such as cardiovascular disease, learning disability, autism spectrum disorder, and full-scale IQ < 80. Considering the possibility of cognitive decline, we excluded participants who were older than 40 years. After excluding individuals with incomplete data and those older than 40 years, there were 183 adults with DSM-5 ADHD left in the study. Adults with DSM-5 ADHD were classified into two groups by recalled age-of-onset: early-onset group (onset <7 years old) and late-onset group (onset between 7 and <12 years old). Finally, there were 142, 41, and 148 individuals in the early-onset ADHD, late-onset ADHD, and control groups, respectively. In the late-onset group, six were from the clinical follow-up sample.
All participants, after clinical and diagnostic interviews, were assessed by the Wechsler Adult Intelligence Scale−III for the intelligence, followed by the CANTAB for neuropsychological functioning in a fixed order of the tasks. We asked the participants who currently received medication (n = 77) for ADHD to hold medication at least 48 hr before the neuropsychological assessment. All the psychologists applying the IQ test and CANTAB were blinded for group status. This study was approved by the Research Ethics Committee of NTUH, Taiwan (IRB ID, 2010003087R; ClinicalTrials.gov number, NCT01247610), before the study implementation.
Interviewer Training
The corresponding author was responsible for training interviewers for the psychiatric interview including the Chinese K-SADS-E and SADS interviews (including the modified adult ADHD supplement). The details of interviewer training were described in the supplementary material.
Agreement of Age-of-Onset at Two-Time Points
Only 40 individuals in the clinical follow-up sample had complete data on age-of-onset and ADHD symptoms at both baseline and follow-up. According to the parental reports, all the 40 individuals had the age of onset of ADHD before 7 years at baseline. Of these 40 individuals with ADHD, 34 individuals reported that their age-of-onset of ADHD was before 7 years old at adulthood and six between 7 and 12 years old. All the adults with ADHD retrospectively reported later age-of-onset of ADHD at follow-up—M (SD), 5.51 (1.29) years old in the early-onset group, and 9.17 (1.03) in the late-onset group—than that reported by their parents to the participants with ADHD at baseline—M (SD) 4.19 (1.53) years old in the early-onset group and 4.33 (1.72) in the late-onset group. The result is compatible with the reports of Todd et al. (2008). For the details of age-of-onset and ADHD symptom agreement, please refer to the supplementary material.
Measures
Six CANTAB tasks were selected in this study and classified into low-executive function (low-EF) tasks and executive function (EF) tasks according to the EF demands (Lin, Chen, & Gau, 2013), as described by Rhodes et al. (2005). The descriptions of neuropsychological tasks are summarized in Table 1.
Neuropsychological Tasks and the Corresponding Functions.
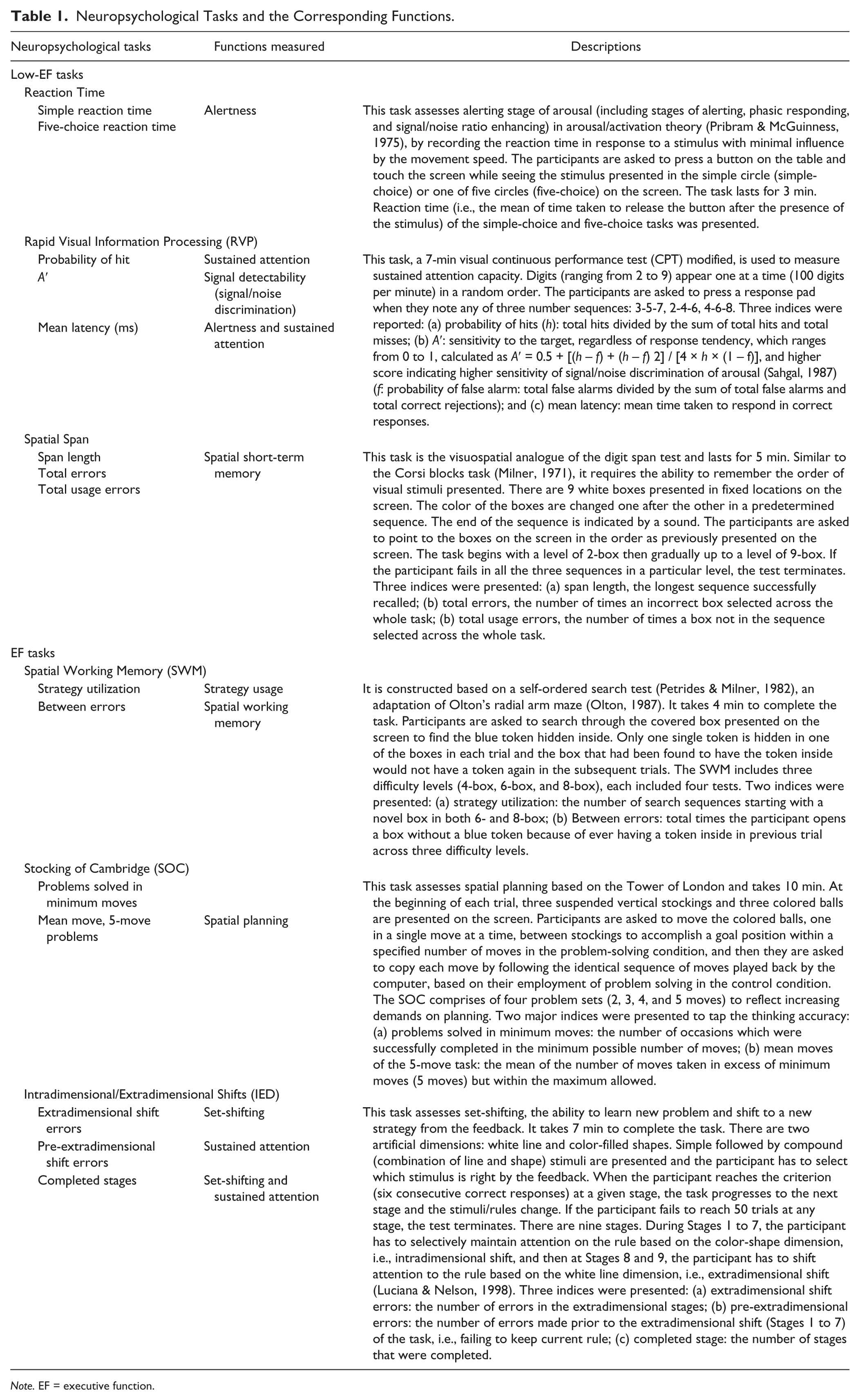
Note. EF = executive function.
Statistical Analyses
We conducted analyses by SAS 9.3 (SAS Institute Inc., Cary, NC). For demographic data, we used chi-square for categorical variables and linear regression for continuous variables. All the results of neuropsychological tasks were calculated and presented with raw scores. For group comparisons of neuropsychological functions, we tested three models using multiple analyses. In the first model (Model 1), we controlled age, sex, and any psychiatric comorbidity (1 for any psychiatric comorbidity and 0 for none). In the second model (Model 2), we added current ADHD medication use (1 for any ADHD medication use and 0 for none), participant’s education, marital status, job, and parental marital status into the first model as the covariates, because these demographic variables were significantly different between groups. The third model was similar to the first model, but the overall “any psychiatric comorbidity” was replaced by the specific psychiatric comorbidity. In the third model (Model 3), a specific psychiatric comorbidity was controlled one at a time, including “depressive disorder,” “anxiety disorder,” “sleep disorder,” “lifetime oppositional defiant disorder (ODD)” and “lifetime conduct disorder (CD),” respectively. We did not control IQ in our analysis because there was no IQ difference between groups (Table 3). Besides, some authors thought factors leading to decreased IQ performance might be the same factors contributing to neuropsychological dysfunction in ADHD. Therefore, controlling for IQ may remove part of the variance of neuropsychological dysfunction associated with ADHD (Nigg, 2001). The Bonferroni correction method was applied to adjust for multiple comparisons in the post hoc analysis. The effect size was calculated for group comparisons of neuropsychological functioning based on Cohen’s definition and was divided into low (0.2-0.5), medium (0.5-0.8), and high (> 0.8) levels. The significant level was preselected as p < .05.
Results
Basic Data and ADHD Symptoms
Table 2 summarizes the demographics of the three groups. Adults with ADHD were significantly older than controls, and there was no group difference in the distributions of sex, and parental occupation and education. More participants in the ADHD groups were married/living with the couple, did not attend college and more parents were divorced or separated as compared to the control group. There were significantly more symptoms of hyperactivity in the early- than in the late-onset ADHD group and no difference in inattention and impulsivity symptoms between two ADHD groups (Table 3). There was no difference in the proportion of ADHD medication use between early-onset and late-onset ADHD groups (Table 3).
Demographic Data.
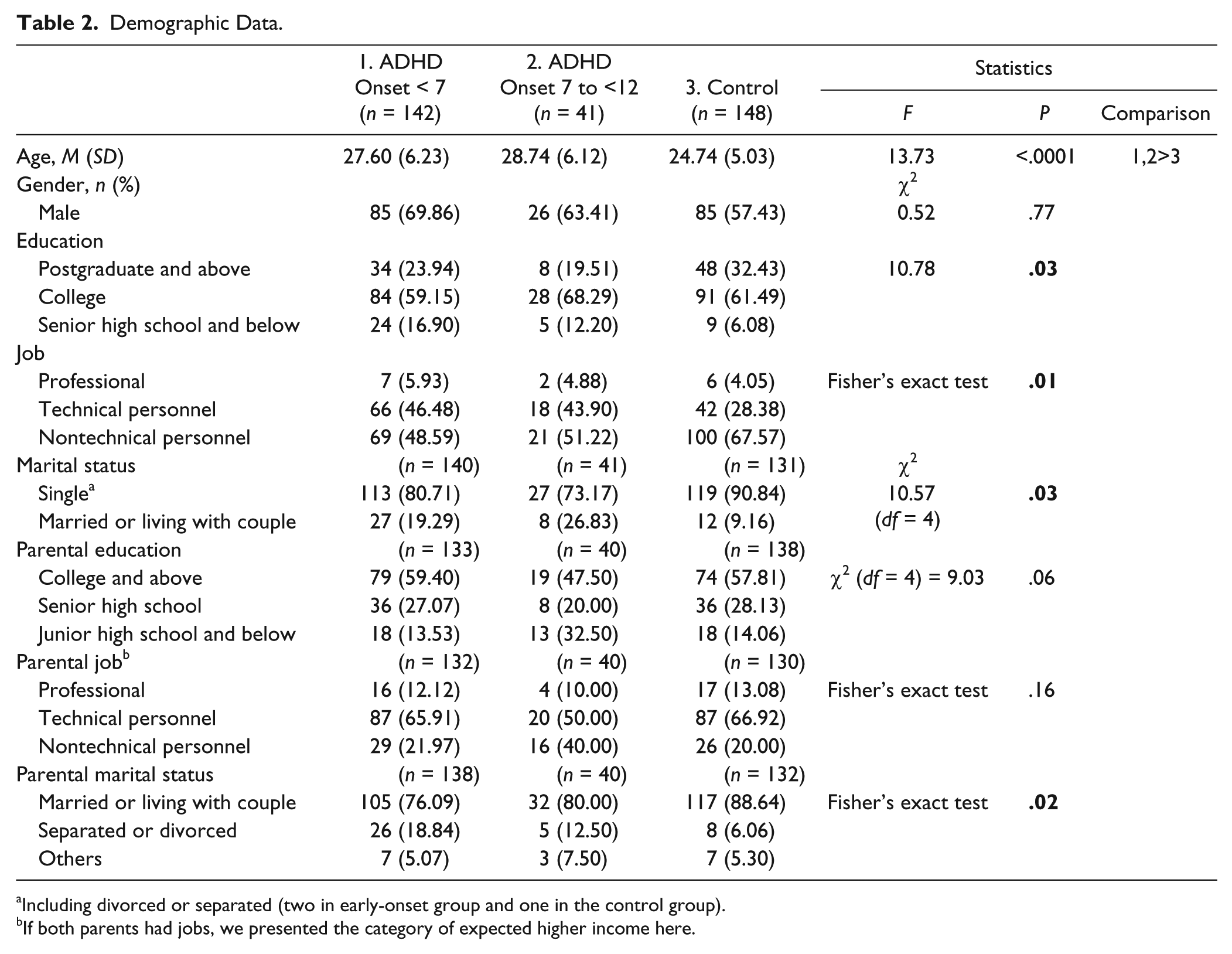
Including divorced or separated (two in early-onset group and one in the control group).
If both parents had jobs, we presented the category of expected higher income here.
ADHD Symptoms, Intelligence, and Psychiatric History Among Groups.
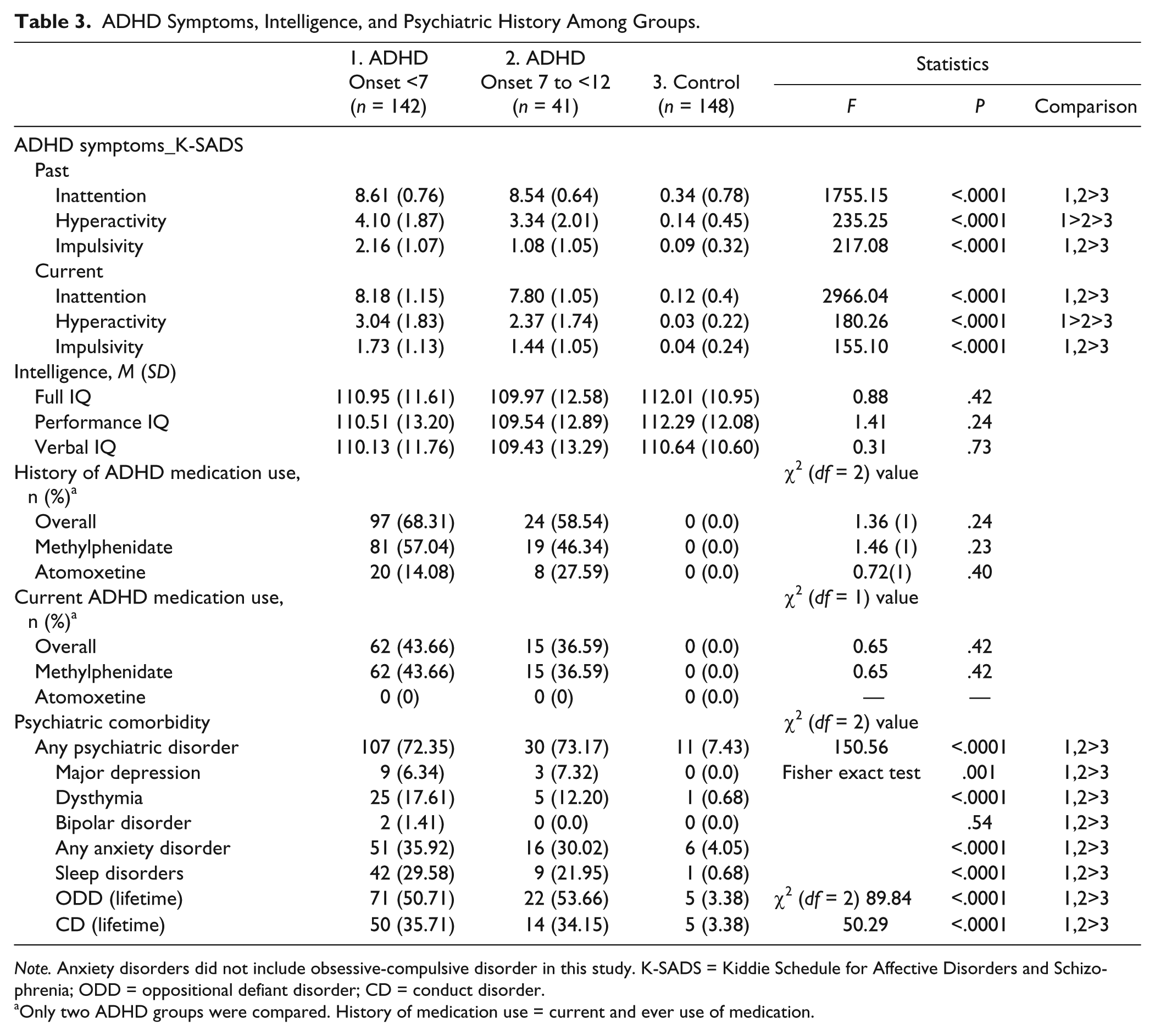
Note. Anxiety disorders did not include obsessive-compulsive disorder in this study. K-SADS = Kiddie Schedule for Affective Disorders and Schizophrenia; ODD = oppositional defiant disorder; CD = conduct disorder.
Only two ADHD groups were compared. History of medication use = current and ever use of medication.
Comparisons of Neuropsychological Functioning Among Groups (Table 4)
Cognitive alertness (Reaction Time)
The early-onset ADHD group had longer reaction time than the control group in the simple analysis. No group difference was noted in the multiple analysis.
Comparison of Neuropsychological Functioning Among Adults With Early-Onset, Late-Onset ADHD, and Controls.
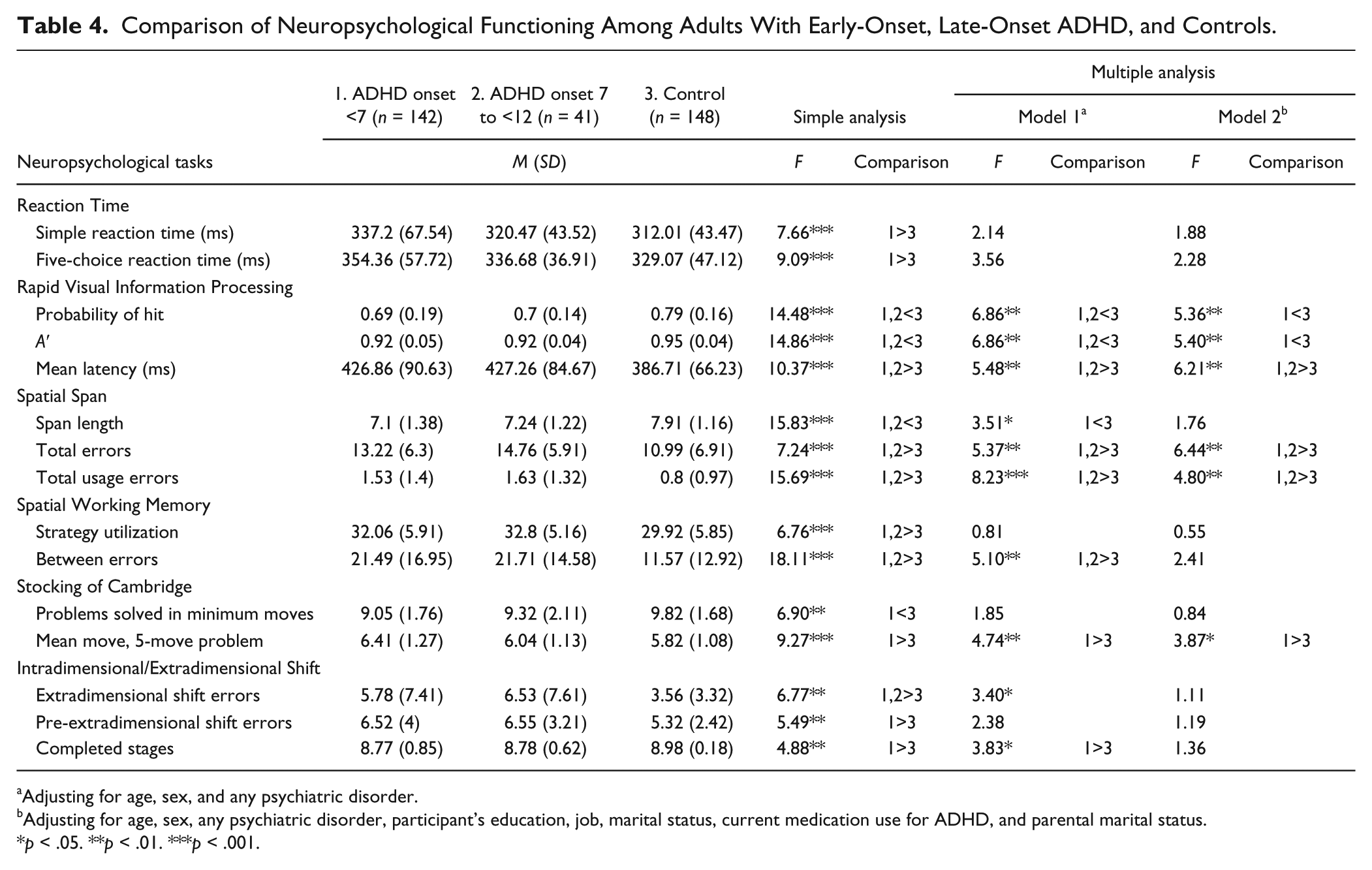
Adjusting for age, sex, and any psychiatric disorder.
Adjusting for age, sex, any psychiatric disorder, participant’s education, job, marital status, current medication use for ADHD, and parental marital status.
p < .05. **p < .01. ***p < .001.
Sustained attention/signal detectability (RVP)
Both the early- and late-onset ADHD groups were impaired in the probability of hit (sustained attention), A′, and mean latency (signal detectability) of RVP in both the simple analysis and the first model of multiple analysis. Only the early-onset ADHD group showed significant impairment in the probability of hit, and A′ and both ADHD groups showed impairment in mean latency in the second model of multiple analysis.
Short-term spatial memory (Spatial Span)
For the span lengths, adults in both ADHD groups had shorter span length than controls in the simple analysis and only adults in the late-onset ADHD group had fewer span lengths than controls in the first model of the multiple analysis. In all analyses, adults in both ADHD groups made more errors than those in the control group.
Spatial working memory (SWM)
Both early- and late-onset groups showed poor strategy utilization and more between errors in the simple analysis. In the multiple analysis, there was no group difference in strategy utilization in both two models and in between errors in the second model of multiple analysis.
Spatial planning (SOC)
Only the early-onset group had fewer problems solved in minimum moves in the simple analysis and more mean moves in the five-move problem in both simple and multiple analyses than the control group.
Set-shifting (IED)
Adults with early- and late-onset ADHD had more extradimensional shift errors than controls in the simple analysis, but not in the multiple analyses. Only the early-onset ADHD group had more pre-extradimensional shift errors in the simple analysis, and fewer completed stages in the simple analysis and the first model of multiple analysis.
For the neuropsychological functions which were impaired in ADHD, the effect size of two ADHD groups over the control group ranged from 0.4 to 0.9, referring a medium to large effect size (Supplementary Table S1). There was no significant difference of neuropsychological functions between the two ADHD groups in the simple and multiple analyses.
Influence of the Specific Psychiatric Comorbidity
When we performed the multiple analysis that controlled for age, sex, and the psychiatric comorbidity one at a time (Model 3), neuropsychological tasks with significant group difference were the same as what was revealed in the simple analyses (Supplementary Table S2).
Influence of ADHD Medication Use
Adding the current medication treatment for ADHD and demographic variables into the multiple analyses models (Model 2), we found that the statistical difference of SWM between errors, IED extradimensional shift errors, and RVP probability of hit and A′ between adults with late-onset ADHD and the controls did not reach the significant level (p > .05; Table 4). Becuase current ADHD medication treatment was reversely correlated with the performance in simple Reaction Time (Pearson correlation, r = .22, p < .001), RVP probability of hit, (r = −.14, p = .01), RVP A′ (r = −.14, p = .01), total usage errors in Spatial Span (r = .21, p < .001), SWM between errors (r = .27, p < .001), IED extradimensional shift errors (r = .17, p = .006), and completed stages (r = −.12, p = 0.03), ADHD medication treatment might share the variance of the correlation between neuropsychological deficits and ADHD. Adults with poorer neuropsychological performance were more likely to receive medication treatment in this naturalistic study, implying a self-selection bias.
Discussion
Main Findings
With the intention to validate the DSM-5 adult ADHD age-of-onset criterion by neuropsychological functioning, this study found that adults with DSM-5 ADHD, regardless of age-of-onset, had significant deficits in sustained attention (RVP probability of hit), signal detectability (RVP A′), spatial working memory (SWM between errors), and set-shifting (IED extradimensional shift errors) after considering the influences of age, sex, and any psychiatric comorbidity, but deficits in alertness (Reaction Time) and planning (SOC five-move task) were only noted in adults with early-onset ADHD. Current medication was correlated with poorer neuropsychological performance, implying a self-selection bias in this study.
Psychiatric Comorbidity and Neuropsychological Functioning in ADHD
Following our previous findings of no difference in functional impairment, quality of life (Lin et al., 2015), and psychiatric comorbidity (Lin et al., 2016) between the early- and late-onset adult ADHD groups, this work further revealed comparable neuropsychological dysfunctions between adults with early- and late-onset ADHD diagnosis according to the DSM-5 criteria. Although this was not the first study to validate the age-of-onset criterion by neuropsychological functioning, this was the first study controlling for each psychiatric comorbidity one at a time. We found no other psychiatric disorder could explain the neuropsychological deficits in adults with ADHD. Under a comprehensive psychiatric interview, adult ADHD diagnosis, even with recalled onset between 7 and 12 years and possible recall bias, would be valid. Late-onset adult ADHD is not a pseudodiagnosis that just coincidentally presents the symptoms of other psychiatric disorders.
Neuropsychological Deficits in Early- and Late-Onset ADHD
In this study, we tested two models of multiple analyses, which revealed similar results. When we looked into the differences of the results between Models 1 and 2, we found that spatial working memory was an important neuropsychological function that made participants decide to use medication, because, in Model 2, current ADHD medication use was associated with worse SWM function (p = .04) independent of group, age, sex, and other demographic variables. Therefore, the loss of group differences of SWM at Model 2 was largely due to the share of the variance of medication use and ADHD. The loss of significant difference between the late-onset and the control groups in RVP might be due to small sample size of the late-onset ADHD group and lack of power to detect the differences when there were many variables in the analysis. The demographic variables had nonsignificant effects on the results. The following discussion is therefore mainly based on the results of the first model of the multiple analyses.
Adults in both early- and late-onset ADHD groups had a longer latency of correct response in RVP, suggesting impaired psychological processes involving sustained attention (van der Meere, Shalev, Borger, & Gross-Tsur, 1995). Meanwhile, our finding that only adults with early-onset ADHD had longer reaction time in both simple and five-choice reaction time tasks suggested that alertness, which was important in the attentional process (Nigg, 2005), was impaired only in early-onset ADHD, or that adults with late-onset ADHD had milder impairment in the attentional network than those with early-onset ADHD. Inattentive symptoms of late-onset ADHD might emerge through neuropsychological mechanisms other than alertness, such as impaired signal detectability of attention, sustained attention, and/or other executive dysfunctions.
We had an intriguing finding that adults with late-onset ADHD had the noninferior performance of SOC as compared with controls despite that they had significant deficits in spatial working memory (SWM) and short-term spatial memory (Spatial Span). During the process of planning, one has to organize response sequences and to monitor execution which places a load on working memory (Owen et al., 1996). The dissociated correlation of late-onset ADHD with spatial (working) memory and spatial planning might be explained by a different load of working memory in CANTAB. SOC in the CANTAB, with the maximum five-move task, required less load of (working) memory than the Spatial Span, with maximum nine digits, and SWM, with maximum eight-box tasks. It was possible that adults with late-onset ADHD had deficits in spatial (working) memory but not planning in the lab setting, and a load of spatial (working) memory in the SOC task did not provoke impaired performance in the late-onset ADHD. Further studies with well-controlled tasks for the divided neuropsychological mechanisms with different loads are needed to verify our hypothesis.
In this study, adults with early-onset ADHD had significantly more previous and current hyperactive symptoms than those with late-onset ADHD, but there was no correlation of hyperactive symptom count and reaction time (simple task, F = 0.01, p = .90, five-choice task, F = 0.58, p = .45) and SOC (five-move tasks, F = 0.02, p = .90) after controlling for the inattentive symptom count. Higher hyperactive symptom count did not explain the differential neuropsychological presentations of early- and late-onset ADHD in this study.
ADHD is a heterogeneous disorder with a various combination of neuropsychological deficits across different affected persons, and the presentations and emergence of symptoms are also correlated to individual adaptation to environmental and developmental constraints (Sonuga-Barke, 2005). Our finding that these late-onset ADHD adults had relatively preserved planning ability implies that they may have fewer dysfunctional brain circuits and thus developed symptoms later or their preserved abilities could compensate for ADHD symptoms during their early childhood. Nevertheless, when ADHD persisted into adulthood, adults with ADHD who recalled onset between 7 and 12 years showed no less functional impairment and had a comparable decrease of life quality as that recalled onset by 7 years (Faraone, Biederman, Spencer, et al., 2006; Lin et al., 2015). More recently, Moffitt et al. (2015) found in their longitudinal study that individuals with adult-onset ADHD, despite subjective complaints of cognitive deficits, had fewer tested cognitive deficits than those with childhood-onset regardless of current ADHD status. Although the symptoms of adult-onset ADHD might be explained by substance dependence and other psychiatric disorders, their findings implied that neuropsychological functions might be correlated to the timing of emergence of ADHD symptoms, that is, late-onset ADHD might be a minor form of ADHD as compared with early-onset ADHD. The author also suggested a possibility that adult-onset ADHD might be an independent disorder etiologically different from childhood-onset ADHD (Moffitt et al., 2015). Further longitudinal and imaging studies are needed to elucidate the role of the Brain Function × Environment interaction in the onset of ADHD in a developmental view.
Limitations
The findings shall be interpreted with some limitations. First, the participants were either clinic-based subjects or recruited via advertisement from the same university hospital. Thus, the generalization of the results is questionable. Second, the intelligence level was relatively high in our sample, and therefore our results could not be generalized to the population of lower intelligence. Third, this study might suffer from recall bias of age-of-onset. Fourth, although we asked the participants who were currently treated with medication to hold it for more than 48 hr before they received CANTAB tests, we could not rule out the possibility of residual or withdrawal effect of medication. Fifth, the sample size of the late-onset ADHD group was relatively small and might lack the statistical power to detect the small group difference, especially between early- and late-onset ADHD. Further longitudinal study with a larger sample size of the late-onset group would be helpful to elucidate the difference between early- and late-onset ADHD and eliminate the recall bias.
Conclusion
Our study showed that adults with late-onset ADHD had comparable neuropsychological deficits, including sustained attention, signal detectability, spatial working memory, short-term spatial memory, and set-shifting as their early-onset counterparts and these deficits could not be explained by the presence of other psychiatric comorbidities. Therefore, extending the age-of-onset criterion for adults did not overdiagnose ADHD in adults, even based on the recalled information. Adults with late-onset ADHD had no deficits in spatial planning and alertness, and the preservation of these neuropsychological abilities might postpone the true or recall of occurrences of ADHD-related difficulties during the development. Further longitudinal studies are warranted to elucidate the role of the interactions between brain functions and the environment in the onset of ADHD at a developmental perspective.
Footnotes
Acknowledgements
We would like to express our thanks to Ms. Yu-Lun Lin for data management and psychiatric interviews, and all participants for their time and efforts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Health Research Institute (NHRI-EX100-10008PI, NHRI-EX101-10008PI, NHRI-EX102-10008PI; NHRI-EX103-10008PI), Taiwan.
Supplementary Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.