
Abstract
Objective:
This study examined concordance between symptom and performance validity among clinically-referred patients undergoing neuropsychological evaluation for Attention-Deficit/Hyperactivity Disorder (ADHD).
Method:
Data from 203 patients who completed the WAIS-IV Working Memory Index, the Clinical Assessment of Attention Deficit-Adult (CAT-A), and ≥4 criterion performance validity tests (PVTs) were analyzed.
Results:
Symptom and performance validity were concordant in 76% of cases, with the majority being valid performance. Of the remaining 24% of cases with divergent validity findings, patients were more likely to exhibit symptom invalidity (15%) than performance invalidity (9%). Patients demonstrating symptom invalidity endorsed significantly more ADHD symptoms than those with credible symptom reporting (ηp2 = .06–.15), but comparable working memory test performance, whereas patients with performance invalidity had significantly worse working memory performance than those with valid PVT performance (ηp2 = .18).
Conclusion:
Symptom and performance invalidity represent dissociable constructs in patients undergoing neuropsychological evaluation of ADHD and should be evaluated independently.
Introduction
Evaluation of Attention-Deficit/Hyperactivity Disorder (ADHD) represents one of the most common referral questions received by neuropsychologists in North America. A recent survey of neuropsychologists in the United States and Canada reported that ADHD constituted the third most frequently assessed patient/diagnostic group as indicated by 37.5% of respondents, with only dementia (48.6%) and head injury (54.8%) evaluated more often (Rabin et al., 2016). Even so, accurate diagnosis of ADHD can be challenging for several reasons. First and foremost, no simple diagnostic test exists that can reliably and validly differentiate people with ADHD from those without it. Furthermore, ADHD diagnoses made in adulthood often rely on retrospective recollection of childhood experiences, given that the diagnostic criteria for ADHD within the Diagnostic and Statistical Manual of Mental Disorders – 5th Edition (DSM-5; American Psychiatric Association, 2013) require the presence of symptoms during childhood.
Given that establishing a diagnosis of ADHD among adults is reliant upon the patient’s retrospective self-report of symptoms and cognitive sequelae throughout their developmental history, typically without the benefit of academic records or collateral report (e.g., teachers, parents), a semi-structured clinical interview has long considered by many to be the ideal approach to the diagnosis of ADHD (Parker & Corkum, 2016). However, a major limitation of structured interviews is that they do not allow for objective assessment of the validity/credibility of reported symptoms, which is problematic considering that self-report data is often unreliable. Among the reasons for its lack of reliability, key symptoms of ADHD, such as inattention, are commonly found in other disorders and are, therefore, nonspecific from a diagnostic standpoint (Ramsay, 2015; Suhr & Berry, 2017). Moreover, many self-report inventories are vulnerable to magnification and feigning of symptoms and the presence of significant external incentives (e.g., stimulant medications, academic accommodations) in the context of evaluation for ADHD may motivate such behavior (Musso & Gouvier, 2014). Unfortunately, many studies have demonstrated that participants instructed to feign ADHD on self-report inventories are able to do so successfully and often cannot be differentiated from patients with genuine ADHD (e.g., Fischer & Watkins, 2008; Fuermaier et al., 2018; Hirsch & Christiansen, 2018; Musso & Gouvier, 2014; Quinn, 2003; Sollman et al., 2010). Moreover, information on ADHD symptomatology can be easily accessed on the internet, which may help patients who are stimulant-seeking or hoping to obtain academic accommodations learn which symptoms to report during their evaluations. While obtaining behavioral ratings from multiple sources (i.e., self and collateral reports) has been shown to improve the accuracy of diagnosis in ADHD (Nelson & Lovett, 2019), it is not always possible to obtain informant reports. Furthermore, these issues have been shown to extend to feigning of cognitive deficits on neuropsychological testing, such that it can be difficult to accurately discriminate poor attention or a high level of impulsivity from invalid performance on testing (e.g., Hirsch & Christiansen, 2018; Musso & Gouvier, 2014; Sollman et al., 2010).
Given that an accurate ADHD diagnosis is commonly dependent on effortful test performance and credible symptom reporting, proper assessment of both performance and symptom validity is a crucial and necessary standard of practice in a neuropsychological evaluation of ADHD (Suhr & Berry, 2017). In brief, symptom validity refers to the degree to which examinees’ endorsed symptoms on self-report measures can be considered credible, whereas performance validity assesses if obtained neuropsychological test scores reflect examinees’ true cognitive abilities (Larrabee, 2012). Despite promising findings regarding the utility of PVTs (e.g., Jasinski et al., 2011; Marshall et al., 2010; Sollman et al., 2010; Williamson et al., 2014) and SVTs (e.g., Cook et al., 2016; Fuermaier et al., 2016; Harrison & Armstrong, 2016) in ADHD evaluations, a majority of the extant literature has examined these constructs independently. However, in a recent study examining both symptom and performance validity, Shura et al. (2017) found that veterans who met criteria for ADHD were not more likely to overreport symptoms on the MMPI-2-RF than those who did not meet diagnostic criteria nor were they more likely to fail a well-validated PVT. However, the veterans who failed a well-validated PVT reported more ADHD symptomatology than those who passed it.
Collectively, there is a paucity of research examining the convergence of symptom and performance validity in general clinical samples presenting for neuropsychological evaluation of ADHD. In particular, while the consequences of PVT failures on neuropsychological test scores are well-established (e.g., Critchfield et al., 2019), the effect(s) of noncredible symptom reporting on actual neuropsychological test performance remains unclear within the context of ADHD. As such, the purpose of this study was twofold. First, we sought to evaluate the concordance of symptom and performance validity among a large sample of clinical patients referred for neuropsychological evaluation of ADHD. Based on prior literature showing that symptom and performance validity are dissociable constructs in other clinical populations (e.g., Aase et al., 2020), we hypothesized that while there may be some overlap between performance and symptom invalidity, these two constructs would be dissociable such that discrete subgroups of patients with invalid performance (with valid symptom report) or exaggerated symptom report (with valid performance) would emerge. Second, we sought to examine how ADHD symptom report and working memory performance differed based on symptom and performance invalidity. Given the established relationship between PVT failures and neuropsychological test performance, we hypothesized that performance invalidity would have a greater impact on working memory test outcome than symptom invalidity, whereas symptom invalidity would have a more substantial impact of ADHD symptom endorsement relative to performance invalidity.
Method
Participants
Data for this cross-sectional study were obtained from a clinical sample of 221 patients referred for neuropsychological evaluation in order to provide diagnostic clarification of and treatment planning in the context of possible ADHD through the Neuropsychology Service at a large Midwestern academic medical center. All patients were referred for evaluation by their family/general medicine or psychiatric provider and were evaluated by a staff neuropsychologist. Study inclusion criteria were: (1) administration of the Working Memory Index (WMI) from the Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV; Wechsler, 2008); (2) completion of the Clinical Assessment of Attention Deficit-Adult (CAT-A; Bracken & Boatwright, 2005); and (3) completion of at least four independent PVTs from the measures listed in Table 1 (PVTs administered: M = 4.97; SD = 1.02). One participant did not complete the WMI and 17 were administered only three PVTs. These 18 patients were therefore excluded, resulting in a final sample size of 203. The sample was 51% male (N = 103) and 49% female (N = 100) with a mean age of 28.04 years (SD = 7.29) and mean educational attainment of 15.42 years (SD = 2.37). Racial composition was diverse with 47% Caucasian (N = 96), 23% Hispanic (N = 46), 16% African American (N = 32), 9% Asian (N = 19), and 5% other race/ethnicity (N = 10). Of the 203 patients in this final sample, 39 (19%) produced an elevation on at least one CAT-A validity scale (see below) indicating abnormal symptom reporting. In contrast, 164 patients (81%) produced no elevations, indicating valid symptom reporting. Moreover, 27 patients (13%) failed ≥2 PVTs and were classified as having invalid neurocognitive test performance, consistent with current practice standards in clinical neuropsychology that identify failure on at least two independent criterion PVTs as the benchmark for performance invalidity (Boone, 2012; Larrabee, 2008; Meyers et al., 2014).
Criterion Performance Validity Tests and Their Associated Cut-Scores.

Note. BVMT-R = brief visuospatial memory test-revised; CVLT-II = California verbal learning test-second edition; RAVLT = Rey auditory verbal learning test; RBANS = repeatable battery for the assessment of neuropsychological status; WMS-IV = Wechsler memory scale-fourth edition; IR = immediate recognition; DR = delayed recognition.
Measures
Clinical Assessment of Attention-Adult (CAT-A)
The CAT-A is well-validated measure of ADHD symptomatology that includes three primary clinical scales (i.e., inattention, impulsivity, and hyperactivity), as well as multiple cluster scales that measure behaviors and characteristics associated with ADHD (Bracken & Boatwright, 2005). Examinees rate both childhood and current symptoms on a 4-point scale ranging from strongly disagree to strongly agree. Regarding scoring, raw scores are converted to demographically-adjusted T-scores. A unique feature of the CAT-A is that the test includes three embedded symptom validity scales, two of which assess for possible symptom over-reporting/exaggeration (i.e., infrequency [IF] and negative impression [NI]) and one that assesses for underreporting (i.e., positive impression [PI]). Per the CAT-A manual, cut-scores for elevation on the three validity scale elevations were: IF: ≥4; NI: ≥46; PI: ≥63. For this study, an elevation on any one of the two CAT-A over-reporting scales (NI and IF) was operationalized as indicating questionable symptom reporting.
Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV)-Working Memory Index (WMI)
The WMI broadly assess auditory attention, concentration, and working memory abilities (Wechsler, 2008). This index is composed of two core subtests, (i.e., Digit Span and Arithmetic) and includes one supplemental subtest (i.e., Letter-Number Sequencing) that can be substituted for a core subtest, which are used to generate the composite WMI age-adjusted standard score.
Statistical Analyses
To determine the concordance of symptom and performance validity, participants were divided into four groups based on their SVT and PVT results: (1) valid SVT and PVT performance; (2) invalid SVT and PVT performance; (3) invalid SVT performance with valid PVT performance; and (4) invalid PVT performance with valid SVT performance. A series of analyses of variance (ANOVAs) were conducted to assess for significant differences in CAT-A symptom reporting based on SVT pass/failure status and PVT pass/failure status. The false discovery rate (FDR) procedure with a 0.05 maximum FDR was used to mitigate the inflated family-wise error rate associated with multiple comparisons (Benjamini & Hochberg, 1995; Glickman et al., 2014). Finally, two ANOVAs, one with symptom validity groups (i.e., valid/invalid) and one with performance validity groups entered as the fixed factors, with WAIS-IV WMI scores as the dependent variable were conducted to assess for significant differences in objective neuropsychological test performance between valid/invalid SVT versus PVT performance.
Results
See Table 2 for the concordance of SVT and PVT performance. Overall, results indicated that symptom and performance validity were concordant in 76% of cases, with the majority of these being valid SVT/PVT performance, whereas 4% had invalid SVT/PVT performance. In the 24% of cases in which SVT/PVT failure profiles were discrepant, participants were more likely to exhibit invalid SVT performance and valid PVT performance (15%) as opposed to invalid PVT performance with valid SVT performance (9%).
Concordance Between Validity Groups for the Overall Sample.
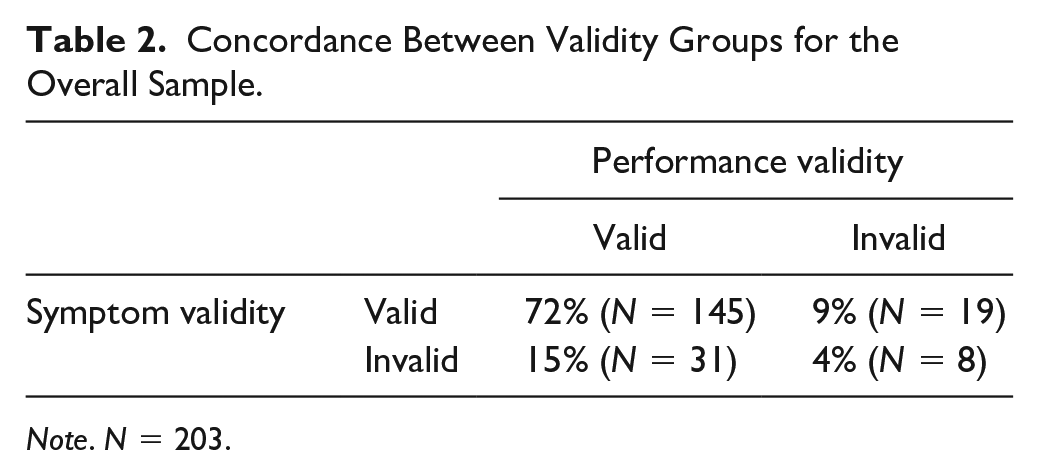
Note. N = 203.
Levene’s test of equality of error variances was nonsignificant for all ANOVAs. As shown in Table 3, patients with invalid symptom reporting endorsed significantly higher levels of both childhood and current ADHD symptoms across all CAT-A clinical scales, with medium to large effect sizes. In contrast, there were nonsignificant differences in symptom reporting between those with valid versus invalid neuropsychological test performance. Finally, as shown in Table 4, ANOVA with performance validity group as the fixed factor revealed significant differences in WMI scores between groups with a large effect size, such that the valid group performed at the population mean, while the mean working memory performance for the invalid group was nearly a full standard deviation lower. By comparison, a parallel analysis of groups divided by symptom validity status revealed nonsignificant differences between valid and invalid groups, with both groups demonstrating intact WMI performance near the population mean.
Attention-Deficit Hyperactivity Disorder Symptom Reporting by Validity Group.
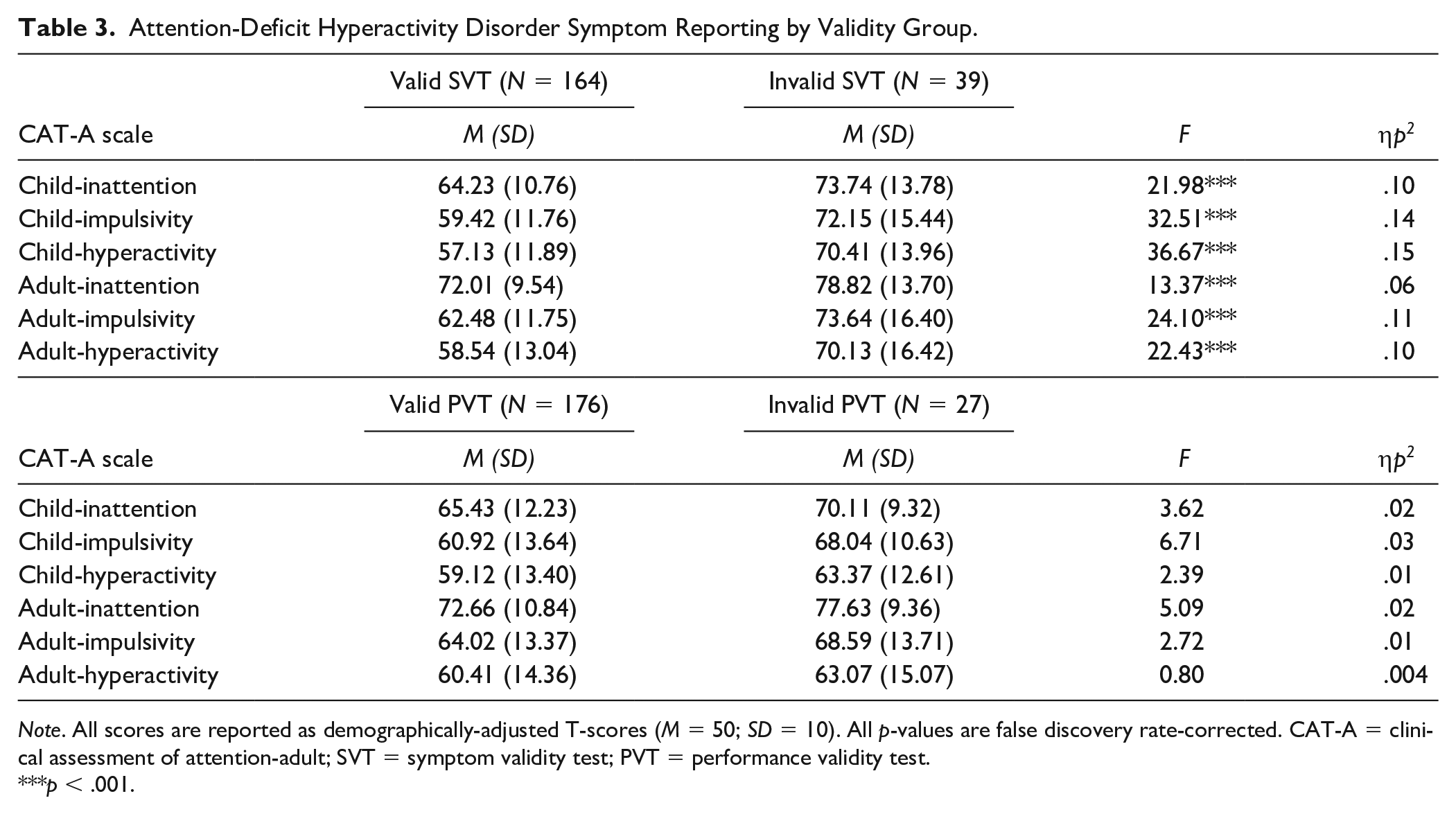
Note. All scores are reported as demographically-adjusted T-scores (M = 50; SD = 10). All p-values are false discovery rate-corrected. CAT-A = clinical assessment of attention-adult; SVT = symptom validity test; PVT = performance validity test.
p < .001.
Working Memory Performance by Validity Group.
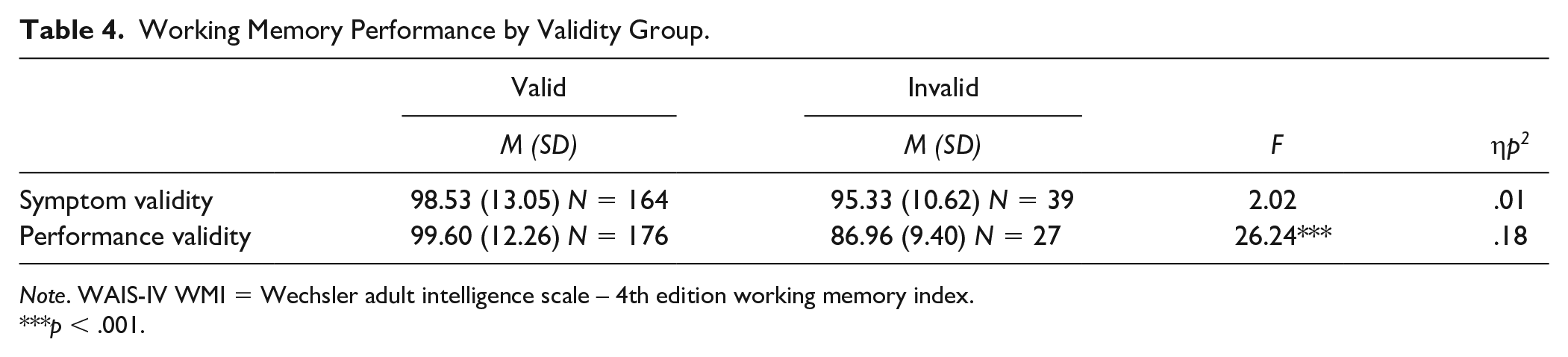
Note. WAIS-IV WMI = Wechsler adult intelligence scale – 4th edition working memory index.
p < .001.
Discussion
This study investigated the concordance of symptom and performance validity among a clinical sample of patients referred for neuropsychological evaluation of ADHD. In addition, we examined how symptom reporting on the CAT-A and performance on a widely-used index of working memory differed based on validity group status. Several findings are of particular interest. First, approximately three quarters of the sample had concordant validity performance (i.e., valid SVT/PVT or invalid SVT/PVT), whereas the remaining one-fourth had divergent validity findings. When validity findings were discordant, patients were more likely to demonstrate symptom invalidity rather than performance invalidity. Second, findings generally support previous literature as well as our hypotheses that symptom and performance validity are dissociable and need to be evaluated independently during ADHD evaluations. Only symptom validity indicators provided meaningful information about possible symptom magnification on the CAT-A, whereas performance validity testing was the lone indicator of differences in working memory performance. As such, symptom and performance validity provide non-redundant information about the credibility of symptom reporting and cognitive test performance, respectively, but cannot be used to infer validity outside of their respective domains.
Results indicated that only 4% of patients had concordant invalid PVT and SVT performance, while 72% displayed concordant valid performance across both forms of validity assessment. Among those with discordant PVT and SVT performance, more exhibited valid PVT performance and invalid SVT performance (15% of the total sample), with the remaining 9% of the overall sample exhibiting invalid PVT performance and valid SVT performance. These findings reflect a significantly lower rate of performance invalidity than previous studies using only one PVT failure to classify performance invalidity (e.g., 19%–48%; Shura et al., 2017; Suhr et al., 2008; Sullivan et al., 2007). However, they are fairly consistent with a study by Van Dyke et al. (2013), which used more conservative validity classification criteria of ≥2 failures on PVTs or SVTs as indicative of invalidity in their respective categories. In their study, 24% of the mixed neuropsychiatric sample was classified as having symptom invalidity, whereas 8% demonstrated performance invalidity and 4% had both invalid SVT and PVT performance. Moreover, the Van Dyke et al. (2013) study included a confirmatory factor analysis examining the relationship between cognitive test performance, symptom self-report, performance validity, and symptom validity, which supported a 3-factor model. Specifically, performance validity and cognitive test performance represented two distinct factors, while symptom validity and symptom self-report loaded together on a third factor. This convergence further cautions against the use of SVTs as a proxy for assessment of performance validity, and highlights the need for evaluation of each construct independently.
Providing further support for this notion, the current study also showed that patients with invalid SVT performance endorsed significantly more ADHD symptoms in childhood and adulthood than those with valid SVT performance. However, there were no differences in symptom reporting between the PVT validity groups. Not surprisingly, a different pattern emerged when examining differences in working memory performance by validity groups. In particular, those with invalid PVT performance performed nearly a full standard deviation worse on the WMI than those with valid PVT performance. Working memory performance did not differ significantly by SVT validity groups. Taken together, these results confirm that symptom invalidity provides useful information about potential exaggeration of ADHD symptoms but cannot be used to infer validity of cognitive test performance. The opposite pattern emerged regarding the implications of performance invalidity, which provided information about suppressed test performance, but should not be used to make inferences about the validity of an examinee’s symptom reporting.
This study benefitted from several methodological strengths, including a demographically diverse clinical sample and the use of several well-validated criterion PVTs to identify invalid neuropsychological test performance (i.e., employing current practice standards of ≥2 PVT failures as indicative of invalid performance; Larrabee, 2008, 2014; Webber et al., 2020). However, some limitations are noteworthy. First, due to the use of retrospective clinical data, the PVTs used to determine performance invalidity were not standardized across patients. Future prospective studies may benefit from implementation of a standardized PVT battery to increase the consistency and reliability of validity group classification. Second, symptom validity classification was determined based solely on the CAT-A validity scales in the present investigation. Future studies may benefit from exploring the use of other methods for symptom validity classification, such as validity scales contained within the Minnesota Multiphasic Personality Inventory-2-Restructured Form (MMPI-2-RF; Ben-Porath & Tellegen, 2008/2011), in addition to other ADHD symptom inventories with validity indices. Additionally, in examining the effect of symptom and performance validity on cognitive test performance, we limited the analysis to performance on a single index of working memory. As such, it remains unclear how well these findings may generalize to performance on tests within other cognitive domains.
In sum, the results of this study align with current literature suggesting that SVT performance is not highly correlated with PVT performance. Specifically, symptom overreporting and performance invalidity appear to represent dissociable constructs in patients undergoing neuropsychological evaluation for ADHD, further substantiating prior claims that independent assessment of both constructs is warranted. Furthermore, differential impacts on neurocognitive test performance were observed for those with valid and invalid cognitive performance within this population. Continued efforts to clarify the relationship between symptom validity and performance validity in patients with ADHD are necessary to further classify the association between these constructs, as well as their relationship with neurocognitive performance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.