
Abstract
Children with ADHD experience more sleep problems than their typically developing peers (Cortese et al., 2013). These sleep problems contribute to poorer behavioral functioning and quality of life (Cortese, Faraone, Konofal, & Lecendreux, 2009). Poor sleep hygiene is a strong contributor to sleep problems in typically developing children (LeBourgeois, Giannotti, Cortesi, Wolfson, & Harsh, 2005; Mindell, Meltzer, Carskadon, & Chervin, 2009). However, few studies have examined the contribution of sleep hygiene to sleep problems in young children with ADHD and no studies have examined the contribution in adolescents with ADHD. Examining contributors to sleep problems which are modifiable, such as sleep hygiene, is important given the impact sleep problems have on both child and family functioning (Sung, Hiscock, Sciberras, & Efron, 2008). Investigating the contribution of sleep hygiene to sleep problems in adolescents with ADHD may assist in the adaptation of existing behavioral sleep interventions for young children with ADHD, which include sleep hygiene strategies, so they are suitable for adolescents with ADHD (Corkum et al., 2016; Hiscock et al., 2015; Keshavarzi et al., 2014).
Sleep problems are experienced by up to 70% of children with ADHD (Sung et al., 2008). The types of sleep problems reported at higher rates than for typically developing peers, when using self- and parent-report, include bedtime resistance, sleep onset latency, sleep maintenance issues, difficulties with morning waking, sleep breathing problems, and daytime sleepiness (Cortese et al., 2009). Using objective measures of sleep, children with ADHD have higher sleep onset latency, a higher apnea–hypopnea index (an indicator of obstructive sleep apnea), poorer sleep efficiency, and shorter sleep durations (Cortese et al., 2009) compared with same-aged peers. In addition, adolescents with ADHD are more likely than their typically developing peers to experience sleep disorders such as insomnia, circadian rhythm disorder, sleep disordered breathing, and sleep movement disorders (Cortese et al., 2013). A number of factors increase the risk of sleep problems in this population, most notably internalizing disorders, for example, depression and anxiety, and externalizing disorders, for example, oppositional defiant disorder and conduct disorder (Lycett, Sciberras, Mensah, & Hiscock, 2015), ADHD medication use (Stein, Weiss, & Hlavaty, 2012), and a delay in dim light melatonin onset, which is a marker of circadian rhythm delay (van der Heijden, Smits, Van Someren, & Gunning, 2005). However, limited studies have investigated modifiable risk factors which may impact on the sleep problems of adolescents with ADHD, such as sleep hygiene.
The associations evident between sleep hygiene and sleep problems in young children with ADHD may potentially be different in adolescence given the general increase in sleep problems observed during this developmental period. That is, typically developing individuals experience negative changes in sleep throughout adolescence (Baker, Richdale, Short, & Gradisar, 2013), with increased sleep onset latency, later bedtimes, reduced weekday sleep duration, reduced total sleep time, increased daytime sleepiness, and insomnia (Gradisar, Gardner, & Dohnt, 2011; Hysing, Pallesen, Stormark, Lundervold, & Sivertsen, 2013). Research has shown the reduced sleep duration of adolescents is partly due to environmental factors (e.g., academic pressures, part-time work, social expectations) rather than due to a reduced need for sleep (Carskadon et al., 1980). The reduced sleep duration and sleep onset latency is also partly due to biological factors, with the circadian rhythm of sleep undergoing a phase delay in adolescence, that is, the internal biological sleep clock moves sleep onset to a later time, and the slowing of the sleep–wake pressure system during puberty, that is, post pubertal individuals find it easier to stay awake than prepubertal/early pubertal individuals (Carskadon, 2011). In addition, daytime sleepiness has been shown to occur at different times for children and adolescents, with children being tired in the mornings and evenings and adolescents experiencing sleepiness in the early and mid-afternoon (Carskadon et al., 1980; Carskadon, Wolfson, Acebo, Tzischinsky, & Seifer, 1998).
Sleep hygiene refers to modifiable environmental (e.g., conducive sleeping environment), scheduling (e.g., consistent sleep–wake schedule), sleep practices (e.g., predictable bedtime routine), and physiological (e.g., reduced caffeine consumption) factors that promote sleep (Jan et al., 2008; Mindell et al., 2009). A number of poor sleep hygiene practices have been identified as increasing the risk of sleep problems in adolescents. These include increased technology use (i.e., computer, cell phone, MP3 player) and increased caffeine consumption in the evenings, which lead to increased sleep onset latency, later bedtimes, and decreased sleep duration, which in turn result in increased daytime sleepiness (Calamaro, Mason, & Ratcliff, 2009; Pieters et al., 2014). In addition, the lack of parental regulation, particularly around setting bedtimes and limit-setting regarding the frequency and intensity of technology use, has also been identified (Carskadon, 2011; Pieters et al., 2014).
Research into the relationship between sleep hygiene and sleep problems has primarily focused on typically developing adolescents. In particular, good sleep hygiene has been moderately to strongly related to sleep quality (LeBourgeois et al., 2005) and sleep hygiene interventions have been shown to improve sleep quality and reduce daytime sleepiness (Dewald-Kaufmann, Oort, & Meijer, 2014; Tan, Healey, Gray, & Galland, 2012). However, no studies have examined the association between sleep hygiene and sleep problems in adolescents with ADHD. Nevertheless, the association between sleep hygiene and sleep problems has been investigated in children with ADHD, with inconsistent results.
Weiss, Wasdell, Bomben, Rea, and Freeman (2006) examined a sleep hygiene intervention in children with ADHD (n = 27; age range = 6-14 years; Mage = 10.29 years) and increased sleep onset latency (i.e., sleep onset > 60 mins) and found a medium-to-large reduction in average sleep onset latency following the sleep hygiene intervention. The finding that sleep hygiene interventions improve sleep in children with ADHD (n = 20; age range = 8-13 years; Mage = 10.10 years) has since been replicated by Keshavarzi et al. (2014), with improvement evident in sleep duration, sleep onset latency, night waking, bedtime resistance, and morning waking. In addition, Sciberras, Song, Mulraney, Schuster, and Hiscock (2017) reported poorer sleep hygiene was associated with the following sleep problems in children with ADHD (n = 361; age range = 5-12 years; Mage = 9.50 years): delayed sleep onset, with small effect; increased bedtime resistance, with medium effect; and increased daytime sleepiness and increased sleep duration problems, both with small to medium effect. The association, however, was not evident for parasomnias, sleep anxiety, and night waking.
In contrast, van der Heijden, Smits, and Gunning (2006) grouped children with ADHD (age range = 6-12 years; Mage = 8.82 years) into those who did not experience chronic sleep onset latency problems (n = 23) and those who did (n = 74), that is, sleep onset > 30 mins at least 4 times a week for over a year, as measured by actigraphy. The results revealed no differences in overall parent-reported sleep hygiene scores between the two groups. These results were supported by van der Heijden, Stoffelsen, Popma, and Swaab (2018) with children aged 6 to 12 years grouped into those with ADHD (n = 44; Mage = 9.80 years), autism spectrum disorder (ASD; n = 68; Mage = 9.60 years), and typically developing (n = 243; Mage = 8.70 years). The results indicated parent-reported sleep problems in children with ADHD were not related to poor sleep hygiene.
The inconsistent findings from these studies may be explained in several ways. First, van der Heijden et al. (2006) used an objective measure of sleep, while the remaining four studies used parent-reported measures. In addition, generalizability to all individuals with ADHD was limited in the Weiss et al. (2006), van der Heijden et al. (2006), and Keshavarzi et al. (2014) studies as individuals with comorbid conditions which may affect sleep were excluded. Also, while Weiss et al. (2006) and van der Heijden et al. (2006) both looked specifically at sleep onset latency, the definition used in each study was different. Finally, it should be noted that Weiss et al. (2006) and Keshavarzi et al. (2014) included young adolescents in their sample, however, the average age of participants was still comparable with the other studies conducted.
Behavioral sleep interventions have been demonstrated to be effective in children with ADHD and sleep problems (Corkum et al., 2016; Hiscock et al., 2015). However, no such interventions have been developed specifically for adolescents. Understanding the role of modifiable factors, such as sleep hygiene, impacting on the sleep experienced by adolescents with ADHD, is integral to informing intervention development in this area. Therefore, this study aimed to examine whether sleep hygiene practices are an additional contributing factor to sleep problems in ADHD, particularly for adolescents. We measured a broad range of sleep problems including sleep onset difficulties, sleep maintenance issues, problems returning to sleep, difficulties with morning waking, and daytime sleepiness. Both self- and parent-report measures were adopted to provide a rigorous account of sleep in adolescents with ADHD. Although no studies have investigated the association between sleep problems in adolescents with ADHD and sleep hygiene, based on the studies involving typically developing adolescents and children with ADHD, we expected that poor sleep hygiene would be associated with non-biologically based sleep problems. To ensure the generalizability of our findings to the broader ADHD population, we included participants with comorbid conditions (e.g., depression, anxiety, and conduct disorder), as well as adolescents who were and were not taking ADHD medication.
Method
Participants
Participants were 79 adolescents with ADHD aged 13 to 17 years (M = 14.24; SD = 1.32; 13 years, n = 42; 14 years, n = 18; 15 years, n = 6; 16 years, n = 7; 17 years, n = 6). Families were recruited from April to December 2016 from an existing database of families who had expressed interest in participating in ADHD research (Lycett, Sciberras, Mensah, Gulenc, & Hiscock, 2014). All adolescents had been diagnosed with ADHD by their pediatrician. Families were contacted via phone by project research assistants to ascertain whether their adolescents met the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) ADHD criteria. This was assessed by parent-report using the ADHD Rating Scale-IV (DuPaul, Power, Anastopoulos, & Reid, 1998) and study designed questions to assess age of onset, cross-situational impairment, and symptom duration of at least 6 months. Families were excluded if they were non-English speaking or if the adolescent had an intellectual disability or a serious medical condition.
Measures
Eligibility criteria
ADHD symptom severity was measured using the parent-reported ADHD Rating Scale-IV (DuPaul et al., 1998). The total was used as were both subscales, inattention and hyperactivity/impulsivity (total: 18 items, α = .92; subscales: α = .85-.93). Symptoms were rated off ADHD medication on a 4-point rating scale from 0 = never or rarely to 3 = very often, indicating the frequency of symptoms over the past 6 months. Higher scores indicate more frequent ADHD symptoms. The adolescent was eligible if they experienced at least six symptoms on either the inattention or hyperactivity/impulsivity subscale often or very often and two study designed questions confirmed symptom duration of at least 6 months (Did your child have these symptoms for 6 months or longer before he or she was diagnosed with ADHD?), and cross-situational impairment (Are these symptoms present at home, school, or when out socially [e.g., in the park, visiting friends]?), as per the DSM-5 criteria (American Psychiatric Association, 2013). The scale has adequate test–retest reliability over a 4-week period and adequate internal consistency (overall: r = .85, α = .92; subscales: r = .78-.86, α = .86-.88; DuPaul et al., 1998). The adolescent was ineligible if they had a serious medical condition (parent-reported yes/no to Does your child have a serious medical condition?) or an intellectual disability (parent-reported yes/no to Does your child have an intellectual disability?).
Sleep hygiene was measured by adolescent self-report using the revised Adolescent Sleep Hygiene Scale (Storfer-Isser, LeBourgeois, Harsh, Tompsett, & Redline, 2013). The total score was used (24 items, α = .83), with the following six sleep hygiene domains being assessed by the scale: physiological (e.g., After 6:00 p.m. in the evening I have drinks with caffeine [e.g., cola, tea, coffee, Red Bull]), behavioral arousal (e.g., I go to bed and do things in bed that keep me awake [e.g., watching TV, reading]), cognitive/emotional (e.g., I go to bed and think about things I need to do), sleep environment (e.g., I fall asleep while watching TV), sleep stability (e.g., During the weekends, I “sleep in” more than 1 hr past my usual wake time), and daytime sleep (e.g., After 6:00 p.m. in the evening I take a nap). Each item was rated using a 6-point rating scale from 1 = always to 6 = never, indicating the frequency of sleep hygiene practices over the past month. All items were reverse coded, with higher scores indicating better sleep hygiene. A validated measure of sleep hygiene for adolescents with ADHD or other neurodevelopmental disorders is not available, therefore, a validated measure of sleep hygiene for typically developing adolescents was used. The scale has satisfactory internal consistency (overall: α = .84), concurrent validity with objective sleep measures, and convergent validity with behavioral outcomes (Storfer-Isser et al., 2013).
Self-reported sleep problems were assessed by adolescent self-report using the Adolescent Sleep Wake Scale (LeBourgeois et al., 2005). The total score and each of the five subscales were used (total: 28 items, α = .93; subscales: α = .84-.87). The five subscales include going to bed (e.g., I have trouble making myself go to bed at bedtime), falling asleep (e.g., When it’s time to go to sleep [lights-out] I have trouble settling down), maintaining sleep (e.g., During the night I wake up more than once), reinitiating sleep (e.g., After waking during the night, I have trouble getting back to sleep), and returning to wakefulness (e.g., In the morning, I wake up and just can’t get going). Each item was rated using a 6-point rating scale from 1 = always to 6 = never, indicating the frequency of the sleep problem over the past month, with higher scores indicating better sleep quality. The scale has good reliability and subscale internal consistency (overall: α = .80; subscales: α = .60-.81; LeBourgeois et al., 2005).
Parent-reported adolescent sleep problems were collected using the Sleep Disturbance Scale for Children (Bruni et al., 1996). The total score and two of the six subscales were used (total: 27 items, α = .89; subscales: α = .76-.82). The two sleep problem subscales included in this study were disorders of initiating and maintaining sleep (e.g., The child has difficulty getting to sleep at night) and disorders of excessive somnolence (e.g., The child awakes in the morning feeling tired) and were selected on the basis that sleep hygiene practices would have more of an impact on these aspects of sleep as opposed to those more biological in nature (i.e., sleep breathing disorders, disorders of arousal/nightmares, sleep wake transition disorders, and sleep hyperhidrosis). Each item was rated using a 5-point rating scale from 1 = never to 5 = always (daily), indicating the frequency of the sleep problem over the past 6 months, with higher scores indicating poorer sleep quality. The scale has satisfactory internal consistency and adequate test–retest reliability (overall: α = .71, r = .71; Bruni et al., 1996).
Sample characteristics included adolescent age; adolescent gender; ADHD symptom severity (parent-reported ADHD Rating Scale-IV total score; DuPaul et al., 1998); ADHD medication use (parent-reported yes/no to Is your child currently taking medication to assist with learning, behavior, emotional or sleep difficulties?); professionally diagnosed externalizing comorbidities, that is, oppositional defiant disorder and conduct disorder, and internalizing comorbidities, that is, depression/dysthymia, anxiety, and obsessive-compulsive disorder (parent-reported yes/no to Has your child ever been DIAGNOSED with or TREATED for any of the following by a health professional?); sleep disordered breathing (parent-reported Sleep Disturbance Scale for Children–Sleep Breathing Disorders subscale score; Bruni et al., 1996); parent high school completion (parent-reported); parent age (parent-reported); parent gender (parent-reported); parent in paid employment (parent-reported yes/no to Are you currently in paid employment?); and parent mental health (parent-reported yes/no to Have you ever been diagnosed with any mental health condition by a health professional [e.g., ADHD, depression, anxiety, or psychosis]?)
Procedure
Information statements, consent forms, and surveys were mailed and/or emailed to eligible parents and adolescents using REDCap, a secure web-based data capture application (Harris et al., 2009). Adolescents received a AU$20 voucher upon completion of their survey as compensation for the time involved. Ethics approval (2016-024) was obtained from the Deakin University Human Research Ethics Committee.
Statistical Analyses
Sample characteristics were described using percentages for categorical variables and mean and SD for continuous variables. The mean and SD of all sleep problem and sleep hygiene variables are also reported. Pair-wise correlation coefficients are reported for all study variables. Socio-demographic characteristics which were associated with sleep problems at p < .10 were included as confounding variables in multiple linear regression analyses investigating the association between sleep hygiene (predictor) and sleep problems (outcome). Power analysis was conducted to evaluate the minimum effect size detectable for a predictor in a multiple regression with seven covariates included. Setting alpha at .05, power at .80, and sample size as 79, G*Power (Faul, Erdfelder, Lang, & Buchner, 2007) indicated effect sizes greater than f2 = .10 could be detected. All analyses were conducted using Stata 15.0 (StataCorp, 2017).
Results
Sample Characteristics
Of the 124 adolescents eligible for this study, 79 (64%) had parent and adolescent data available. There were no differences in adolescent age, adolescent gender, or ADHD symptom severity between those who did and did not complete the survey.
Sample characteristics are presented in Table 1. The majority of adolescents were male (89%) and the majority of all adolescents were taking ADHD medication (65%). Approximately half had either an internalizing (41%) or externalizing (18%) disorder diagnosis. Responding parents were mostly mothers (99%), with an average age of 46.3 years (SD = 5.2) and most were in paid employment (77%). More than half of the parents reported experiencing a mental health condition (51%). Total sleep duration was a variable in this sample with 16% (n = 13) having 9 to 11 hrs of sleep, 32% (n = 25) 8 to 9 hrs, 27% (n = 21) 7 to 8 hrs, 23% (n = 18) 5 to 7 hrs, and 3% (n = 2) less than 5 hrs. Table 2 reports the mean, SD, and range of all sleep hygiene and sleep problem variables.
Sample Characteristics of Adolescents With ADHD.
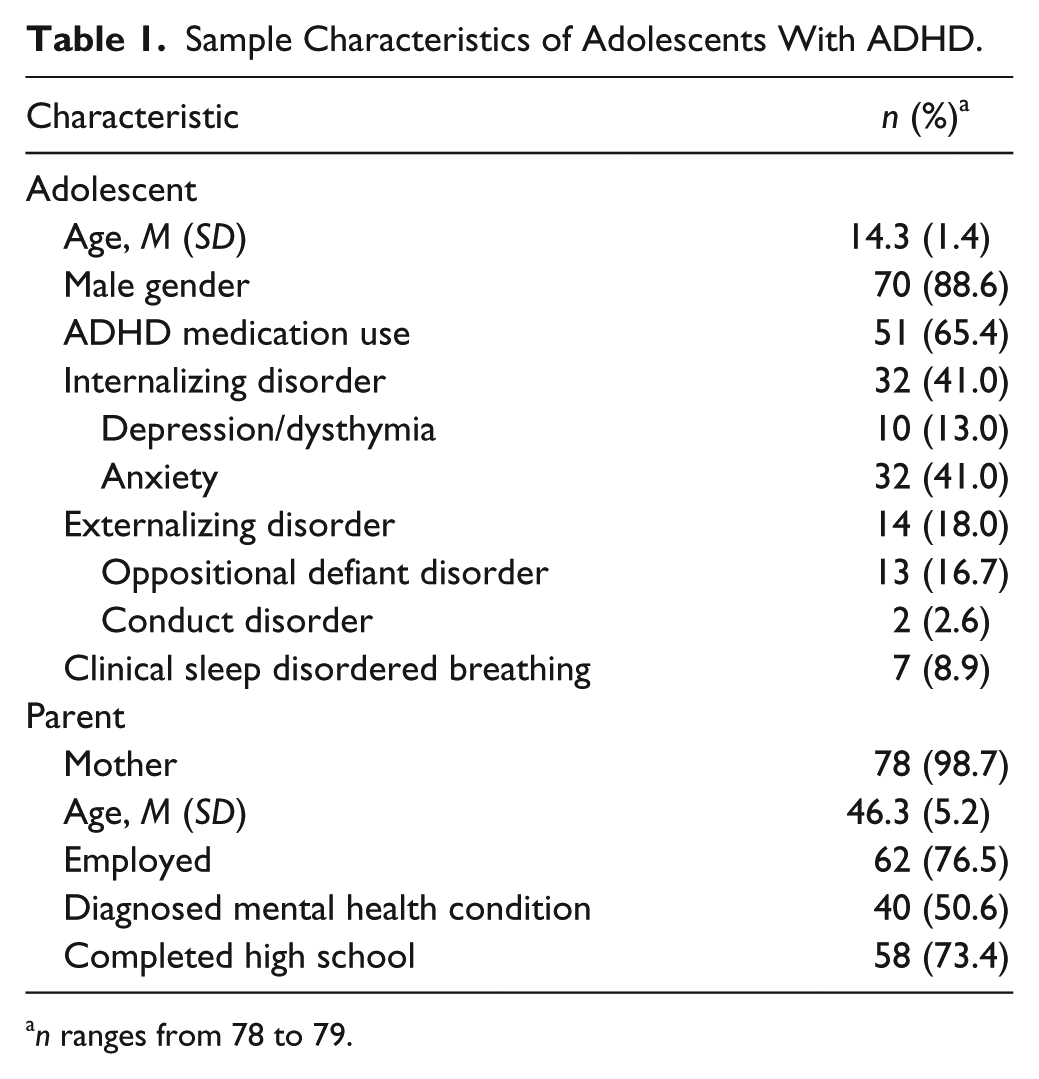
n ranges from 78 to 79.
Mean (SD) of Parent and Adolescent Reported Sleep Problem and Sleep Hygiene Variables.

n ranges from 77 to 79.
Correlation Between Study Variables
Table 3 includes the pair-wise correlations between all study variables. Adolescent age, parent age, parent employment, and parent high school completion were not associated with any self- or parent-reported sleep problem variables at p < .10. Adolescent gender (self-reported reinitiating sleep: r = .3, p = .01), ADHD medication use (self-reported maintaining sleep: r = .2, p = .07; self-reported returning to wakefulness: r = .2, p = .06), externalizing disorders (self-reported maintaining sleep: r = −.2, p = .04; self-reported returning to wakefulness: r = .2, p = .08), internalizing disorders (self-reported reinitiating sleep: r = −.3, p = .01; self-reported returning to wakefulness: r = .2, p = .08; parent-reported total sleep problems: r = .4, p < .001; parent-reported disorders of initiating and maintaining sleep: r = .4, p < .001), clinical sleep disordered breathing (parent-reported total sleep problems: r = .2, p = .08), ADHD symptom severity (self-reported going to bed: r = −.2, p = .04; parent-reported total sleep problems: r = .5, p < .001; parent-reported disorders of initiating and maintaining sleep: r = .4, p < .001; parent-reported disorders of excessive somnolence: r = .4, p < .001), and parent mental health (self-reported reinitiating sleep: r = −.2, p = .04; self-reported returning to wakefulness: r = .2, p = .04; parent-reported total sleep problems: r = .2, p = .03; parent-reported disorders of initiating and maintaining sleep: r = .3, p = .02; parent-reported disorders of excessive somnolence: r = .3, p = .01) were associated with some domains of self- or parent-reported sleep problems at p < .10 and were, therefore, included as covariates in multiple regression analyses, as reported below.
Correlation Between Study Variables.
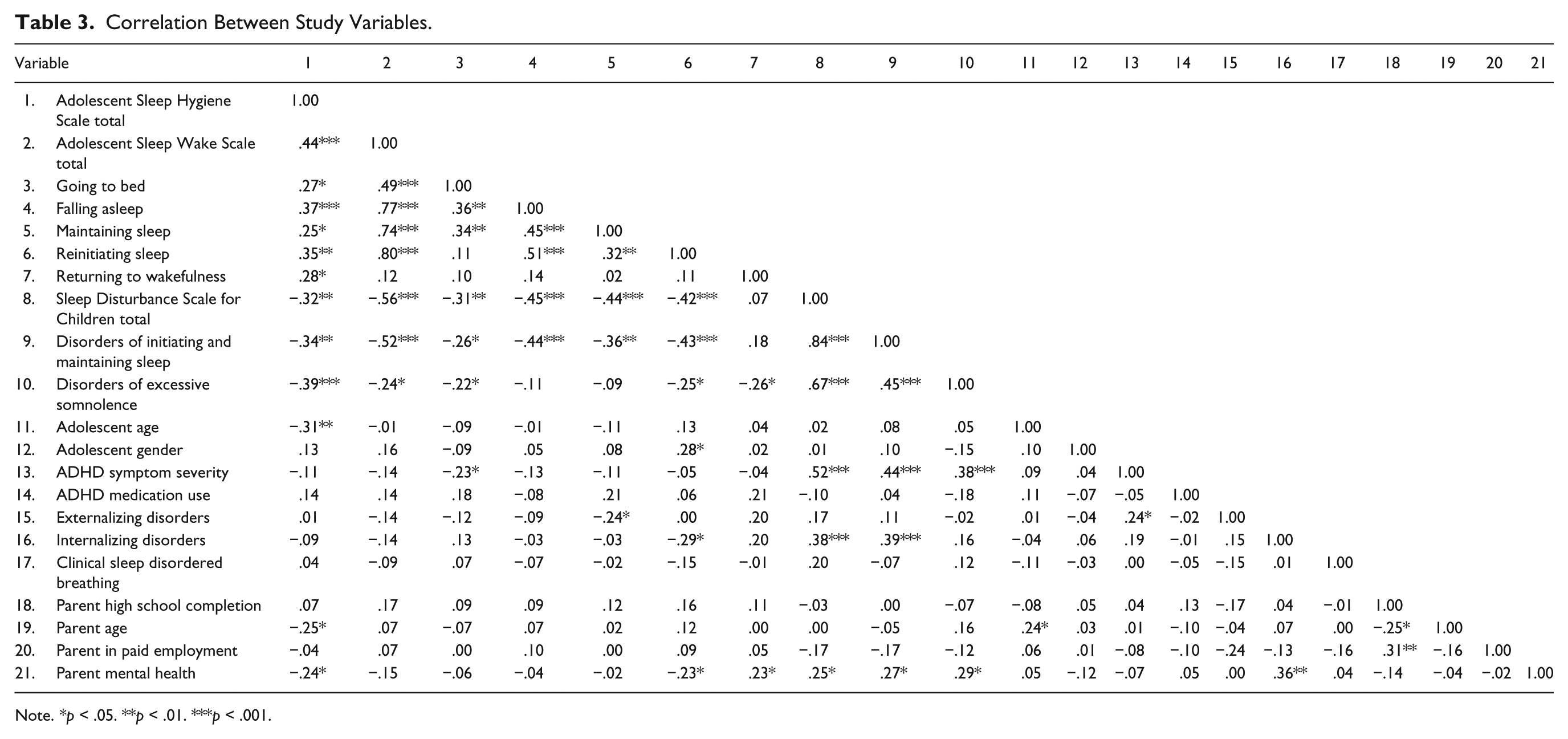
Note. *p < .05. **p < .01. ***p < .001.
Relationship Between Sleep Hygiene and Self- and Parent-Reported Sleep Problems
As per Table 4, adolescent reported sleep hygiene was associated with most aspects of sleep as measured by both self- and parent-report. Sleep hygiene was associated with self-reported total sleep problems (β = .39, p = .001), falling asleep (β = .36, p = .003), reinitiating sleep (β = .37, p = .01), and returning to wakefulness (β = .33, p = .004). There was some evidence of a relationship between sleep hygiene and going to bed (β = .19, p = .06) and maintaining sleep (β = .22, p = .08), however, these findings fell short of statistical significance. Similarly, sleep hygiene was associated with parent-reported total sleep problems (β = −.23, p = .02), initiating and maintaining sleep (β = −.26, p = .01), and excessive somnolence (β = −.30, p = .003).
Association Between Sleep Hygiene and Sleep Problems in Adolescents With ADHD.
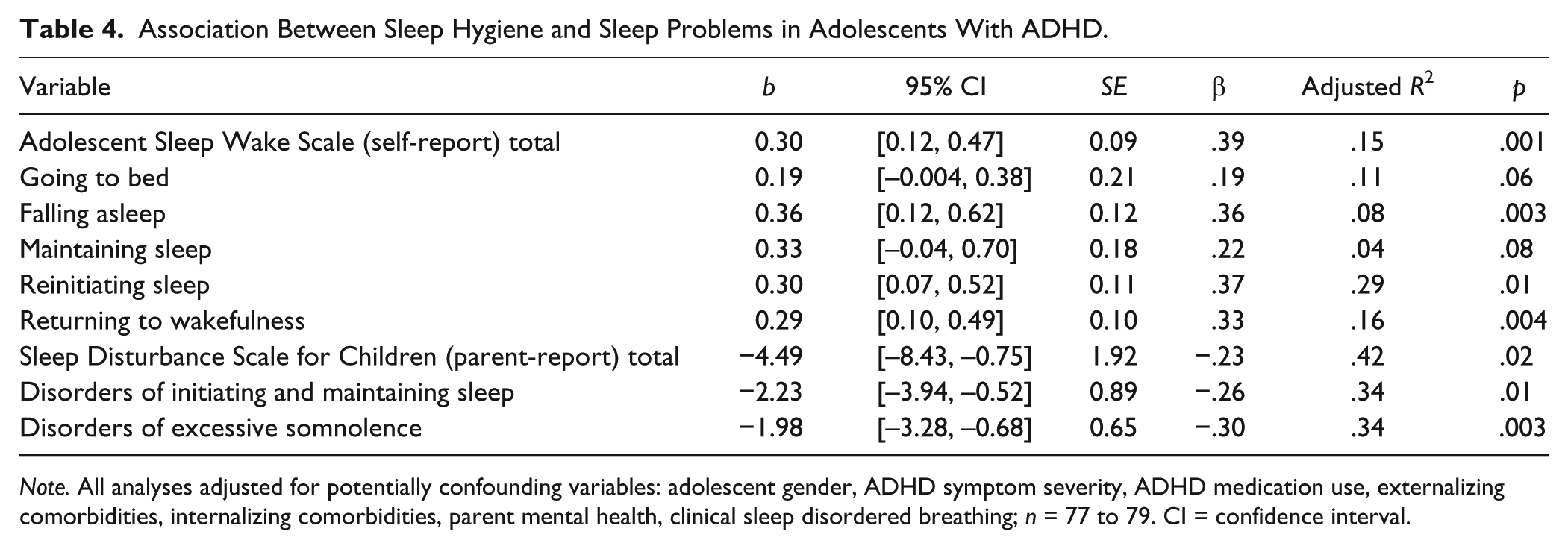
Note. All analyses adjusted for potentially confounding variables: adolescent gender, ADHD symptom severity, ADHD medication use, externalizing comorbidities, internalizing comorbidities, parent mental health, clinical sleep disordered breathing; n = 77 to 79. CI = confidence interval.
A number of variables were independently associated with the following self- and parent-reported sleep problems in our adjusted models. For self-report, going to bed was independently associated with internalizing disorders (β = .27, p = .03) and ADHD symptom severity (β = .24, p = .04); reinitiating sleep with adolescent gender (β = −.22, p = .04) and internalizing disorders (β = −.27, p = .02); and returning to wakefulness with parent mental health (β = −.24, p = .05). For parent-report, total sleep problems were associated with internalizing disorders (β = .21, p = .03), ADHD symptom severity (β = .44, p < .001) and clinical sleep disordered breathing (β = .22, p = .02); initiating and maintaining sleep with internalizing disorders (β = .24, p = .02) and ADHD symptom severity (β = .39, p = .01); and excessive somnolence with ADHD symptom severity (β = .39, p < .001) and parent mental health (β = .27, p = .01).
Discussion
Although there is considerable evidence speaking to the nature of sleep problems in children with ADHD (Cortese et al., 2009), comparatively little is known about sleep in adolescents with ADHD. To the best of our knowledge, this is the first study to examine the relationship between sleep hygiene and sleep problems in adolescents with ADHD. The results from this study suggest a relationship between self-reported sleep hygiene and total self-reported and parent-reported sleep in adolescents with ADHD, with small and moderate effect sizes, respectively. These findings held when accounting for key potential confounding variables such as medication use and comorbidities. Sleep hygiene was associated with most domains of self- and parent-reported sleep problems including self-reported problems falling asleep, reinitiating sleep and returning to wakefulness, and parent-reported disorders of initiating and maintaining sleep and disorders of excessive somnolence.
These findings are consistent with some studies that have examined the relationship between sleep hygiene and sleep problems in children with ADHD (Sciberras et al., 2017). Our results are also consistent with studies which have found that sleep hygiene interventions improve the sleep of children with ADHD (Keshavarzi et al., 2014; Weiss et al., 2006). Our results are also consistent with typically developing adolescents where good sleep hygiene has been moderately to strongly related to sleep quality (LeBourgeois et al., 2005) and sleep hygiene interventions have been shown to improve sleep quality and reduce daytime sleepiness (Dewald-Kaufmann et al., 2014; Tan et al., 2012).
The findings of this study are somewhat in contrast to both van der Heijden et al. (2006) and van der Heijden et al. (2018). The differences in findings from this study may reflect that we assessed sleep problems by self- and parent-report, rather than by actigraphy (van der Heijden et al., 2006). Our study also included adolescents with comorbid disorders (e.g., depression and anxiety) which were excluded in van der Heijden et al. (2006). In van der Heijden et al. (2018), sleep hygiene was associated with sleep problems only for typically developing children and children with ASD but not ADHD. However, van der Heijden et al. (2018) differed in a number of ways from the current study, that is, the sample was younger (age range = 6-12 years), the ADHD group was smaller (n = 44), and sleep problems and sleep hygiene were assessed via parent-report only.
Sleep hygiene was not significantly associated with self-reported problems with going to bed and maintaining sleep. It is important to note there was indeed evidence that these variables had small associations with sleep hygiene, however, these relationships fell short of statistical significance. Both the presence of an internalizing disorder and ADHD symptom severity were independently associated with problems going to bed, suggesting the management of internalizing disorders and ADHD symptoms may be more important targets when considering how to improve problems for adolescents with ADHD getting to bed at night. In contrast, we identified no independent predictors of maintaining sleep problems (e.g., legs kick or jerk during the night) in this sample, which could suggest this aspect of sleep is more biologically driven.
Our study also shed light on how other characteristics of adolescents with ADHD were associated with sleep problems. Internalizing disorders and parent mental health were independently associated with multiple aspects of sleep problems. Our findings fit with previous research demonstrating links between internalizing disorders and sleep problems in children and adolescents with ADHD (Becker, Langberg, & Byars, 2015; Lycett, Mensah, Hiscock, & Sciberras, 2014). Our findings also fit with recent research demonstrating that comorbid internalizing symptoms are differentially associated with particular domains of sleep problems (Becker, Cusick, Sidol, Epstein, & Tamm, 2018). There is likely a bi-directional relationship between internalizing problems and sleep problems. For example, it has been shown that internalizing difficulties increase the risk for sleep problems and vice-versa (Quach, Nguyen, Williams, & Sciberras, 2017). Although the family environment is likely an important contributor to sleep problems, this has yet to be examined in adolescents with ADHD. We found that parent mental health was associated with some aspects of sleep indicating that examining the influence of family factors on sleep problems in adolescents with ADHD may be a fruitful area for future research. It is unsurprising that ADHD symptom severity was associated with multiple domains of sleep problems given the overlap in the symptoms of ADHD and the consequences of sleep deprivation. Clinical sleep disordered breathing was associated with total parent-reported sleep problems, which is consistent with prior research (Beebe, 2006). ADHD medication use and externalizing disorders were not independently associated with any domains of sleep problems. Males with ADHD had more reinitiating sleep problems than females with ADHD, which is in contrast to recent research demonstrating that 7- to 13-year-old females with ADHD had poorer sleep across most domains compared with males with ADHD (Becker et al., 2018). However, our sample of females was very small.
This study had a number of strengths including the collection of sleep data from both adolescents and their parents and our measurement of sleep including detailed and widely used measures of sleep and sleep hygiene. Our sample was also inclusive of a broad range of adolescents with ADHD irrespective of comorbidities and medication use. However, we did have a modest sample size (n = 79), which may have reduced the ability to detect statistically significant effects. Our study also focused on subjective reports of sleep difficulties, as opposed to an objective measure of sleep, such as actigraphy, which would permit measurement of day-to-day variations in sleep problems (Cortese et al., 2009). Also, the pubertal status of our participants was not obtained, limiting our ability to investigate possible biological factors impacting on sleep problems. In addition, there is some item overlap between the Adolescent Sleep Hygiene Scale (Storfer-Isser et al., 2013) and both the Adolescent Sleep Wake Scale (LeBourgeois et al., 2005) and the Sleep Disturbance Scale for Children (Bruni et al., 1996) which may reduce the ability to draw conclusions about associations between sleep problems and sleep hygiene. Finally, the association between sleep problems and the individual sleep hygiene domains was not analyzed. As such, it is not possible to determine which modifiable sleep hygiene practices (e.g., caffeine consumption, media usage, consistent sleep–wake schedule) had an association with sleep problems and whether particular sleep hygiene practices affect specific sleep problems.
Given the high prevalence of sleep problems in adolescents with ADHD, obtaining a sleep history, including an assessment of both sleep hygiene and sleep problems, should be an essential component of clinical assessment. Clinicians should consider the benefits of modifying sleep hygiene practices when assessing and treating the sleep problems of adolescents with ADHD. Research is needed to evaluate the efficacy of improving sleep problems in adolescents with ADHD and, in particular, whether improving sleep problems in this population leads to improvements in daily functioning. Our findings also suggest that the presence of internalizing comorbidities and parent mental health difficulties may be a red flag for sleep problems in adolescents with ADHD.
The findings of this study point to an association between poorer sleep hygiene and increased sleep problems in adolescents with ADHD. Given this observed association, interventions incorporating some focus on sleep hygiene, in addition to other targeted strategies, may prove to be effective in improving sleep in this population. Sleep hygiene strategies have been included in behavioral interventions that have been designed to improve sleep in children with ADHD (Corkum et al., 2016; Hiscock et al., 2015; Keshavarzi et al., 2014). We are now working on adapting such programs to be suitable for adolescents with ADHD.
Footnotes
Authors’ Note
Data were collected and managed using the Research Electronic Data Capture (REDCap) tools hosted at the Murdoch Children’s Research Institute (MCRI). REDCap is a secure, web-based application designed to support data capture for research studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Central Research Grant Scheme at Deakin University. E.S. is supported by an NHMRC Early Career Fellowship (1037159) and NHMRC Career Development Award (1110688). C.M. is supported by an Australian Government Research Training Program Scholarship. MCRI is supported by the Victorian Government’s Operational Infrastructure Support Program.