
Abstract
ADHD is a neurobiological developmental disorder characterized by a persistent inattention and/or hyperactivity/impulsivity severe enough to interfere with a child’s normal psychological development. This disorder negatively influences the quality of performance in common daily activities, making the children affected unable to adjust their behavior to the demands of a given situation (Capodieci, Rivetti, & Cornoldi, 2016). The reported prevalence rates of ADHD among schoolchildren of all ages in Europe and elsewhere in the world are typically high (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007; Wittchen et al., 2011), meaning that nearly every classroom may include at least one child with symptoms of ADHD. The classroom is a very important place for all children because it is where they learn how to interact with their peers, as well as gaining academic skills. This is one of the reasons why peer-reported social preferences are such a strongly informative measure (Hoza, 2007). The symptoms of ADHD tend to prevent the children affected from interacting successfully with their peers (Hodgens, Cole, & Boldizar, 2000; Hoza et al., 2005; Mrug, Hoza, Pelham, Gnagy, & Greiner, 2007). Research (Rich, Loo, Yang, Dang, & Smalley, 2009) has shown that children with symptoms of ADHD are often rejected because of their inclination to be forceful, indelicate, inflexible, disturbing, impatient, and heedless of the rules in organized games. The type of classroom behavior associated with their rejection by their peers includes being off-task, troublesome, rude, and incapable of self-control. Peer-reported social preferences have also been found more accurate than parents’ reports in predicting psychiatric problems later on (Cowen, Pederson, Babigian, Isso, & Trost, 1973; Mikami, Chong, Saporito, & Na, 2015). In particular, the difficult social relations of children with ADHD are associated with negative longitudinal outcomes, including serious conduct problems (Bagwell, Molina, Pelham, & Hoza, 2001). This is confirmed when class nominations are used as the main measure of students’ relations with peers in social behavior studies (Barkley, 2002; Hoza et al., 2005). The solidity of social preference is usually perceived as resulting from children’s steady behavior over time, and especially from consistency in the troublesome conduct of unpopular children.
The mechanisms underlying social and relational difficulties remain poorly understood, however. It had been suggested, as previously mentioned, that ADHD children’s difficulties with their peers relate to their negative behavior and weak social skills, but recent research has pointed to other potential contributors too. For example, children with ADHD seem to be extremely poor at judging their own social behavior using self-report tools, which revealed discrepancies vis-à-vis their actual performance. During a laboratory interaction task (Hoza, Waschbusch, Pelham, Molina, & Milich, 2000), when compared with a control group, boys with ADHD reported having done better in their interaction with an unfamiliar boy, whereas objective coders rated their performance significantly worse.
This underestimation of their problems in various areas on the part of children with ADHD has been amply studied and called positive illusory bias (PIB; Hoza, Pelham, Dobbs, Owens, & Pillow, 2002). In other words, ADHD children’s self-perceptions are frequently inconsistent with objective measures of their performance, or with parents’ or teachers’ ratings of their competence. There have been reports of children with ADHD exhibiting illusions of a greater self-competence than that of their peers without the condition (Hoza et al., 2002; Owens & Hoza, 2003). In typically developing (TD) children, a moderately positive illusion of self-competence is an adaptive mechanism that enhances motivation, performance, and persistence in completing a task (Taylor & Brown, 1988). This does not seem to be true of the positive illusions held by children with ADHD, however, who tend more frequently—despite their positive illusory self-perception—to give up on a task, and to perform less well than their non-ADHD peers (Hoza, Waschbusch, Owens, Pelham, & Kipp, 2001; Owens, Goldfine, Evangelista, Hoza, & Kaiser, 2007). Positive illusory self-perceptions may make children with ADHD more susceptible to failure because they are likely to prevent such children from recognizing the need to improve, acknowledge negative feedback, and change their approach to the completion of a task (Milich & Okazaki, 1991). On the contrary, their lack of awareness may spare their self-confidence, and protect their self-concept (Owens et al., 2007). Be that as it may, the potential adaptive or maladaptive consequences of positive illusory self-perception remain uncertain.
However, the literature regarding PIB is still controversial; Jiang and Johnston’s (2017) findings suggested the need to further test the extent to which it is the lower impairment levels of children with ADHD, rather than the PIB, that are associated with their overestimation. Consistent with the results of Swanson, Owens, and Hinshaw (2012) and Watabe, Owens, Serrano, and Evans (2017), this study’s findings question the incremental validity of the PIB construct above and beyond impairment. However, results are not consistent with those of Jia, Jiang, and Mikami (2016) and Ohan and Johnston (2011), which demonstrate that the PIB is related to functioning independent from impairment. So, it is possible that differences across studies in methodology or measures used to account for impairment may explain these divergent results.
Explanations that have been advanced for PIB include cognitive immaturity (Milich, 1994), neuropsychological deficits (Owens & Hoza, 2003), ignorance of incompetence (Hoza et al., 2002), and self-protection (Ohan & Johnston, 2002). This last hypothesis has garnered more empirical support than any other proposed reason for PIB in children with ADHD, although further evidence is needed to confirm or reject it, and to elucidate the role of PIB in children with ADHD. The self-protection hypothesis posits that, when children with ADHD are threatened by a challenging task, they attempt to hide their incompetence and avoid feelings of inadequacy by inflating their sense of self-competence (Diener & Milich, 1997). This would mean that children with ADHD overestimate their competence as a coping mechanism, thereby presenting a confident front to others and protecting their self-concept (Evangelista, Owens, Golden, & Pelham, 2008). Many studies found a lower than normal self-concept in children and adolescents with ADHD, however (Wehmeier, Schacht, & Barkley, 2010). Self-concept can be defined as an individual’s positive or negative attitude to himself or herself. Several factors relating to self-concept have been identified and studied in children with ADHD, such as academic and social self-concept (Edbom, Lichtenstein, Granlund, & Larsson, 2006). Genetic and environmental determinants of self-concept have been investigated, but no specific determinants of low self-concept have emerged. Children with ADHD and associated impairments, such as learning disabilities, or social and emotional difficulties, nearly always have a low self-concept (Brook & Boaz, 2005), challenging the hypothesis that PIB might have a self-protective function in such children.
Another important aspect investigated in these children’s social difficulties concerns the perception of loneliness. Various researchers found that, despite symptoms of ADHD being related to more peer dislike and rejection, children with ADHD did not report feeling more lonely than control children (Diamantopoulou, Henricsson, & Rydell, 2005; Heiman, 2005; Houghton, Roost, Carroll, & Brandtman, 2015). Here again, PIB seems to have a self-protective function: Even though they are more often rejected by their peers, children with symptoms of ADHD report having good self-perceived social and interpersonal skills. This prevents them from feeling lonely, but is not strong enough to protect them against a low self-concept, which is a broader construct about the self, with self-competence and self-liking as constitutive dimensions (Tafarodi & Swann, 2001).
On this basis, the aim of our study was to examine PIB, social difficulties, self-concept, and loneliness in children with symptoms of ADHD. Unlike previous research, the present study tried to answer some open questions about the social difficulties and PIB experienced by children with ADHD. Specifically, the PIB phenomenon was studied by comparing children who had ADHD with children who had similar social difficulties, but no ADHD, in an effort to better understand the influence of PIB on other, secondary problems, as suggested by Owens and colleagues (2007). In other words, the present study aimed to ascertain whether PIB had an adaptive or maladaptive influence on self-concept and loneliness. Our first objective was therefore to see whether children with ADHD were more likely to be rejected and less popular in class and how this situation changed across primary school age groups. A second objective was to compare children’s self-perception with their teachers’ perception of any social difficulties, considering children with ADHD and a control group of children matched for age and gender with weak social abilities, but no ADHD. Finally, self-concept and loneliness were compared between these two groups and vis-à-vis a third group of TD children. Based on the previous literature, our study hypothesis was that children of all ages with symptoms of ADHD were less likely to be preferred and more likely to be rejected by their peers and that the children with ADHD would show PIB regarding their social abilities by comparison with the children with social difficulties (but no ADHD). The former children (those with symptoms of ADHD) were also expected to show less self-concept, but not more loneliness, than the TD children, and a higher self-concept than the controls with weak social abilities—based on the assumption that PIB has a self-protective function.
Method
Participants
The study involved 196 children (aged between 7.4 and 11.4 years) attending 12 primary school classes (in Grades 2, 4, and 5) at two different schools in the same area of north-eastern Italy. Specifically, there were 74 second-graders (33 M, 40 F), 80 fourth-graders (46 M, 34 F), and 42 fifth-graders (23 M, 19 F) involved in the study.
From this sample, we selected a group of children with symptoms of ADHD judging from a screening process that included informal interviews with teachers and parents, and a score of 14 or higher (the cutoff proposed by the authors, see Marzocchi, Re, & Cornoldi, 2010) on at least one of the two subscales (i.e., inattention, hyperactivity) of the Scala per i Disturbi di Attenzione/Iperattività per Insegnanti (SDAI) teacher’s report, an ADHD scale for teachers (Marzocchi & Cornoldi, 2000). A score of 14 in the SDAI scale means the presence of a 1.5 mean/item in the nine items regarding inattentive and/or hyperactive/impulsive symptoms, with a number of symptoms between five to nine (see Capodieci, 2017, for further details) It should be noted that these children had not been specifically diagnosed with ADHD—a condition still rarely diagnosed in Italy at any age (Skounti, Philalithis, & Galanakis, 2007). Children with symptoms of ADHD were 21 (13 M, 8 F). Between children selected as having symptoms of ADHD, eight have prevalent inattentive symptoms, five hyperactive/impulsive symptoms, and eight combined symptoms. Children were not receiving any kind of treatment, including medication. A control group was selected that was matched with the children with ADHD symptoms group in terms of age, gender, rated intellectual ability, and socioeconomic level, but with weak social abilities (see Table 1). In both groups, the children had an average cognitive level, and no other serious psychological issues (oppositional behavior or internalizing problems). None of the children had a history of neurological or psychiatric problems. Children with other neurodevelopmental disorders (i.e., autism spectrum disorders, intellectual disabilities, or sensory disorders) were excluded from the sample. Written consent was obtained from children’s parents before they took part in the study. This study was conducted in accordance with the recommendations of the Padua University ethics committee and was approved by our institutional board.
Characteristics (Mean and SD) of Children With Symptoms of ADHD and a Control Group of Children With Weak Social Abilities.

Note. Control items = rated intellectual ability and socioeconomic level; SDAI = Scala per i Disturbi di Attenzione/Iperattività per Insegnanti [ADHD scale for teachers]; COM = Comorbidity.
Materials
Sociometric questionnaire
To analyze their social preferences, the children were asked to name three classmates they most liked to play with (Elledge, Elledge, Newgent, & Cavell, 2016). As suggested by Asher and Dodge (1986), “liked least” nominations were avoided. Instead, children rated how much they liked to play with each classmate on a 5-point scale, where 1 counted as liked least nominations. Children were asked to write the names of their three favorite classmates, and then to answer three questions on each classmate, on a scale from 1 = not at all to 5 = very much: “How much do you like to play with him/her?” “How much would you like him/her as a deskmate?” and “How much would you like him/her as a teammate?” As the number of classmates providing nominations varied between classrooms, scores were converted into z scores for each class—as is normal practice in sociometric research (e.g., Coie & Dodge, 1983)—to enable comparisons between scores for students in classes of different sizes. Social preference scores were computed by subtracting “liked-least” from “liked-most” nominations, then dividing the resulting number by the number of student raters minus 1 (as students could not rate or nominate themselves). Children were classified as “rejected” on the grounds of the following three criteria (Coie, Dodge, & Coppotelli, 1982):
a. standardized social preference scores < −1.0,
b. standardized liked-least scores >0, and
c. standardized liked-most scores <0.
Social preference scores and rejected sociometric status were considered as separate indicators of children’s social risk and were used to analyze changes. Sociometric questionnaires are important because they are more predictive of children’s future psychological functioning than measures provided by teachers or parents (Capodieci et al., 2016; Cowen et al., 1973).
SDAI teacher’s report scale
This scale is widely used in Italy and has been validated for the Italian population, revealing high interjudge and test–retest reliabilities (r > .8 in both cases), a strong discriminatory power, and a concurrent validity obtained by correlating this scale with others (r > .95; Marzocchi et al., 2010). The scale exactly reflects the 18 symptoms listed in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) for the purpose of diagnosing ADHD and therefore includes two subscales, one for inattention (nine items), and one for hyperactivity/impulsivity (nine items). Teachers were asked to closely monitor a child’s behavior for about 2 weeks and then report the frequency of the types of symptomatic behavior described in each item. Scores for the items on the SDAI scale range from 0 (problematic behavior never present) to 3 (very often present).
Comorbidity (COM) teacher’s report scale
Teachers were also asked to answer the COM questionnaire to identify any minor symptoms of other psychological and psychopathological problems, and to collect relevant information on the children (Marzocchi et al., 2010). The COM teacher’s report scale was proposed in its updated form, comprising 35 items, to analyze social and relational aspects too (Capodieci, in press). Teachers and parents were interviewed informally to collect further evidence of a child’s ADHD symptoms, not only at school but also in other settings, to rule out children with other difficulties.
To examine the specific behavior of interest in this study, we administered various tests to both the teachers and the children. The reason for administering a questionnaire to the teachers was to obtain a more objective measure of the children’s interpersonal skills, as recommended in literature (Hoza et al., 2002). The same questionnaire (Interpersonal Competence Scale [ICS]) was proposed to the teachers and the children, to identify any discrepancies between what the children reported and their teachers’ impressions. The ICS (Cairns, Leung, Gest, & Cairns, 1995) consists of 18 items, divided into three main factors: aggressiveness (AGG), popularity (POP), and academic abilities (ACA); and three secondary factors: social affiliation (AFF), Olympian quantities (OLY: sporting prowess, attractiveness, and tendency to win at games, sports, etc.), and internalizing difficulty (INT). The sum of the interpersonal competence scores (the summed competence, SC score) was also considered: This is obtained from the unweighted mean of the five subscale scores (POP, AFF, OLY, ACA, AGG), with the AGG reversed in sign. Each item referring to a given type of behavior was scored on a continuum between positive and negative poles (e.g., never aggressive–always aggressive), to indicate the child’s habitual behavior on a scale from 1 to 7. To avoid bias in the responses, different polarities were inverted in different items. The assessment is given by the sum of the scores, the higher the score, the better the aspect considered describes the child’s behavior.
Multidimensional Self-Concept Scale (MSC)
The MSC is based on a hierarchical model of self-concept comprising six self-concept dimensions (Social, Competence, Affect, Academic, Family, and Physical) that partly overlap and partly assess general self-concept (Bracken, 2003). For the present study, we used three subscales—concerning the Social, Competence, and Academic dimensions—because they are intuitively more related to interpersonal relationships with peers. The children were asked to score each item using a 4-point scale from 4 (absolutely true) to 1 (absolutely not true). The reliabilities of the subscales are Social Self-Concept (SC-S), Cronbach’s α = .86; Competence Self-Concept (SC-C), Cronbach’s α = .82; and Academic Self-Concept (SC-A), Cronbach’s α = .86 (Bracken, 2003).
Children’s loneliness and social dissatisfaction self-report
Children were asked to score statements regarding themselves (e.g., “I have nobody to talk to”; “I am lonely”; “I don’t have anybody to play with at school”) on a 5-point scale, and higher total scores indicated a greater sense of loneliness (Loneliness, adapted from Asher, Hymel, & Renshaw, 1984). This measure has been used in previous studies and validated for different cultures (e.g., Asendorpf & Van Aken, 1993; Casiglia, LoCoco, & Zappulla, 1998; Chen, Liu, & Li, 2000). Its internal consistency was reportedly .84, .90, .95, and .84, in Brazilian, Canadian, Chinese, and Italian samples, respectively (Chen et al., 2004). The Loneliness Questionnaire (Asher et al., 1984), adapted for use in Italian by Casiglia et al. (1998), is a self-report measure of the degree of a child’s satisfaction with their relationships with their peers. As reported by the authors, this questionnaire correlates with the child’s status in the class as a group, a lower status correlating with higher scores for loneliness and dissatisfaction (Asher et al., 1984). The Italian form of the questionnaire consists of 18 items on a 5-point scale, from 5 (always true) to 1 (never true).
Procedure
The self-report scales were administered collectively to the children at school, in a counterbalanced order, during two sessions lasting a mean 30 min in the first part of the morning. Before administering the questionnaires, the children were told that it was important to answer truthfully, that they could ask questions if anything was not clear, and that their answers would be used anonymously (an aspect especially important to children in fourth and fifth grade, who are more likely to provide socially desirable).
Results
The distribution of the residuals was found to be normal for all measures of interest in the whole sample and in the measures considered for the different grades sample, without relevant outlier data (Shapiro–Wilk between .76 and .98 with p < .05). The statistical analyses were run in two separate stages. The first involved an analysis of the social preferences expressed by the children in the three areas of inquiry, using the sociometric questionnaire and the three questions on how much they would like a given classmate as a playmate, deskmate, and teammate). This analysis was run on the whole sample (196 children, 21 of them with symptoms of ADHD) to obtain a clear sociometric picture of all the children about their classmates. We expected to ascertain whether children with symptoms of ADHD were actually less likely to be preferred and more likely to be rejected by their peers. In the second stage, our group of children with symptoms of ADHD was compared with the control group of children matched for social abilities, but no symptoms of ADHD. Both the teacher-report and the self-report scales were compared between these two groups, also including an analysis of the children’s social preferences.
Analysis of Social Preferences in the Group of Children as a Whole
Table 2 shows the two groups’ mean scores and standard deviations for the three different questions answered by the children—Q1: “How much do you like to play with him/her?” Q2: “How much would you like him/her as a deskmate?” Q3: “How much would you like him/her as a teammate?” First, the comparison was drawn on the whole sample. Then, given the interesting results that emerged, each school grade was considered separately.
Mean Scores and SDs in the Two Groups of Children (Control and Symptoms of ADHD) for Nominations by Classmates.
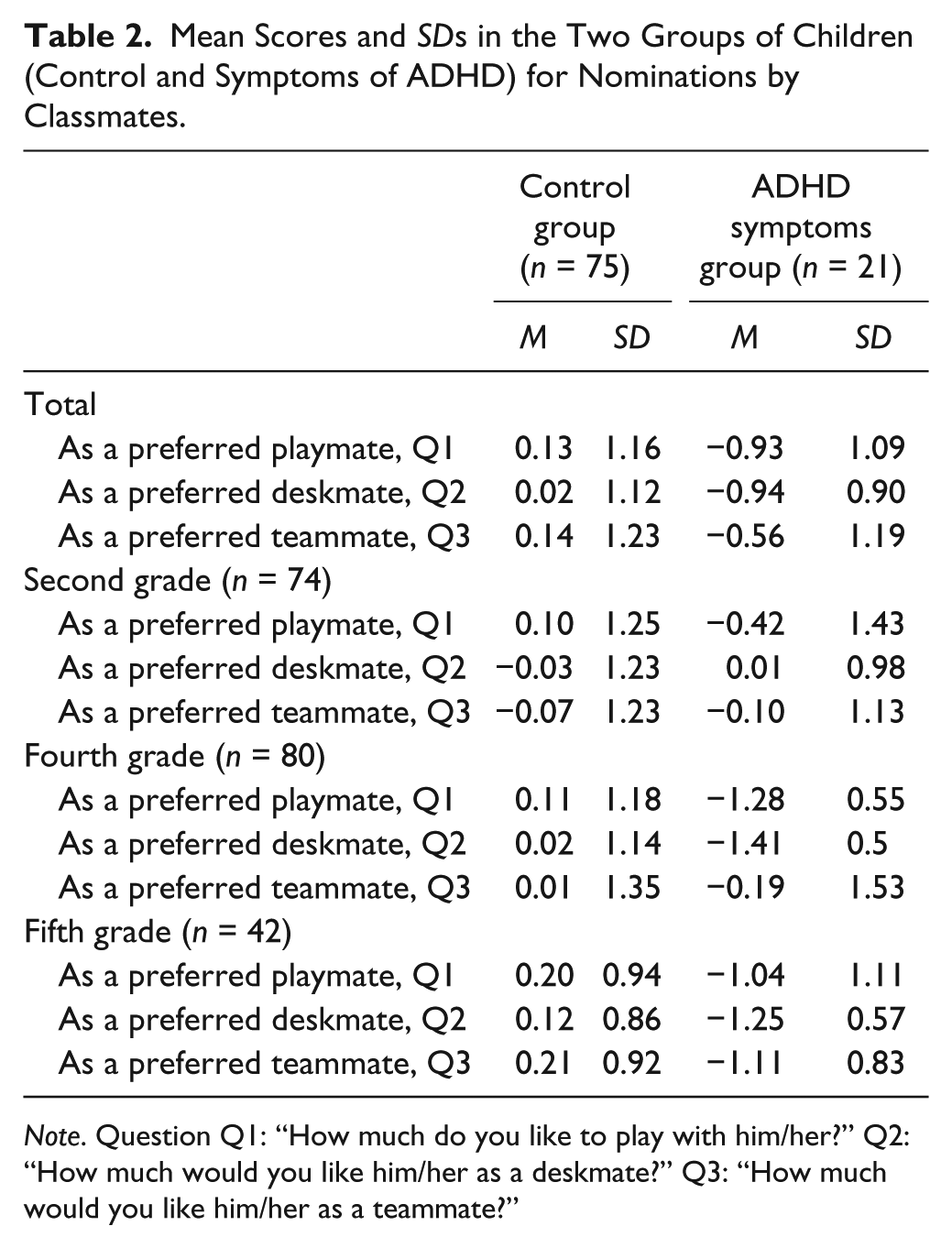
Note. Question Q1: “How much do you like to play with him/her?” Q2: “How much would you like him/her as a deskmate?” Q3: “How much would you like him/her as a teammate?”
One-way ANOVAs comparing the group of children with ADHD symptoms with the whole sample of children showed that children with symptoms of ADHD group were more often rejected by peers in all three areas: as playmates, F(1, 194) = 15.80, p < .001,
Table 3 shows the percentage of rejected children in the two groups (control and ADHD) when the sample was divided by school grade, analyzed using a chi-squared (χ2) test. Clearly, the proportion of children rejected followed an opposite trend in the two groups over time: It declined in the control group for all three conditions (playmate, deskmate, teammate), but was already higher in second grade in children with symptoms of ADHD, and continued to rise for all three conditions.
Percentage of Children Rejected in the Two Groups (Control and Symptoms of ADHD) by School Grade.
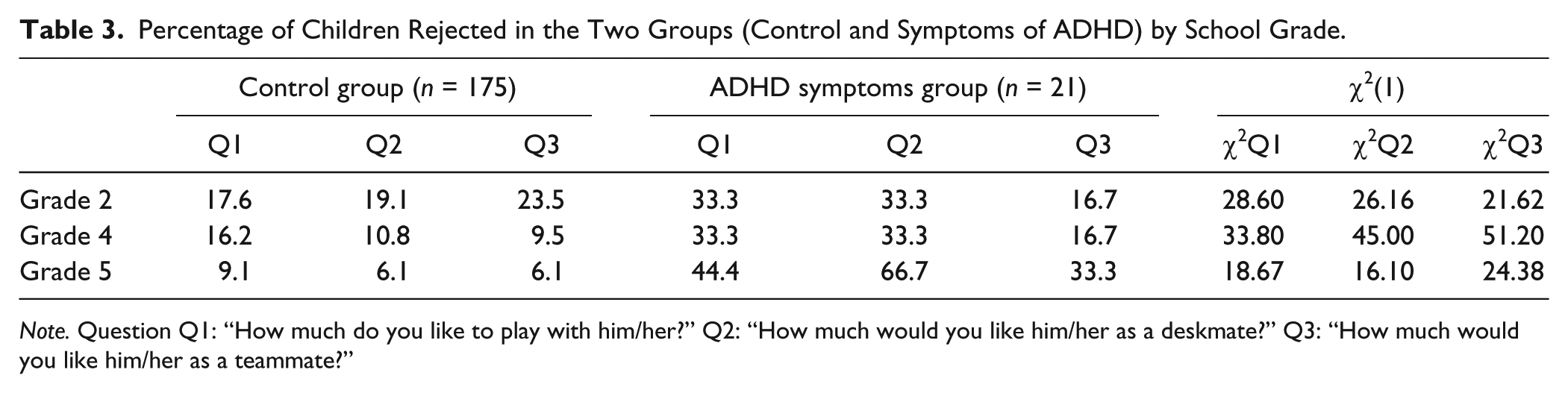
Note. Question Q1: “How much do you like to play with him/her?” Q2: “How much would you like him/her as a deskmate?” Q3: “How much would you like him/her as a teammate?”
Comparison Between Children With Symptoms of ADHD and Controls With Weak Social Abilities
The second part of the analysis was performed on the two groups—children with symptoms of ADHD and controls with low social abilities but no ADHD symptoms—which both consisted of 21 children (13 M and 8 F), matched for age, gender, socioeconomic status, control items on the SDAI scale, and sociability on the COM scale. In the ICS, the teachers’ and the children’s answers were compared using a repeated-measures ANOVA (Table 4). The two groups of children (i.e., symptoms of ADHD and controls) were analyzed separately, and the effect sizes were recorded for the various different factors (AGG, POP, ACA, AFF, OLY, interpersonal competence scores).
Means (SD in Brackets) and Cohen’s d Measuring Effect Size in the Comparison Between the Teacher and Child Versions of the ICS in the Two Groups (Controls With Weak Social Abilities and Symptoms of ADHD).
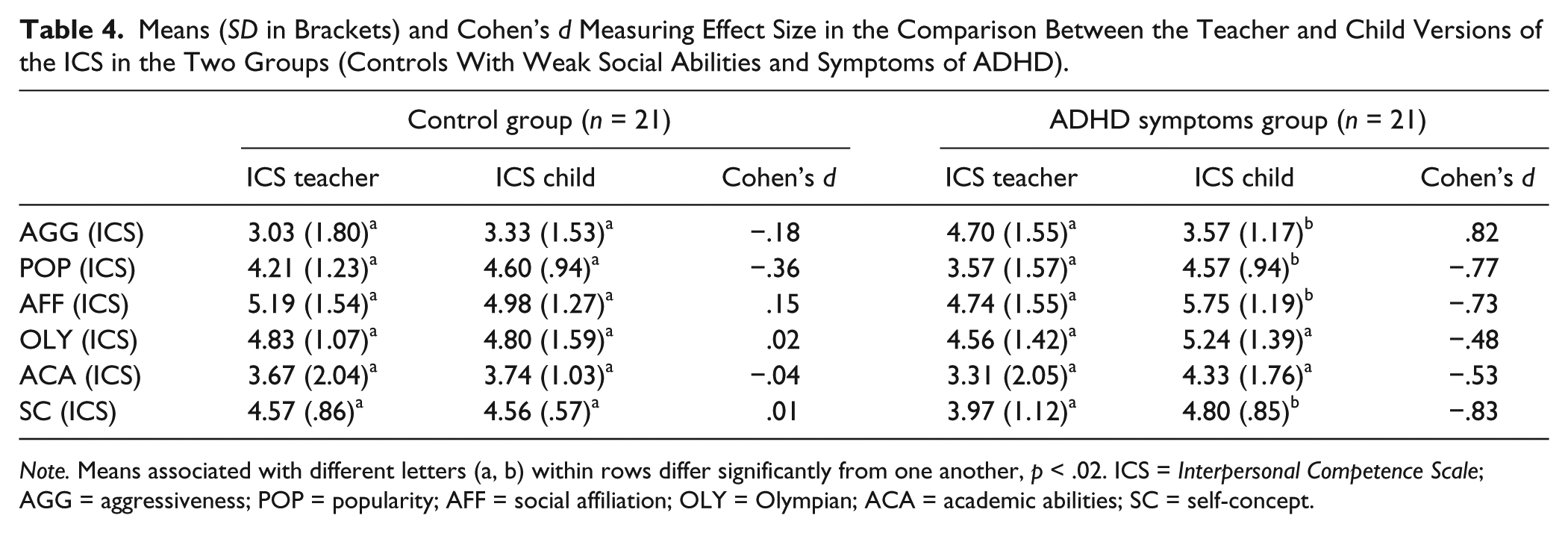
Note. Means associated with different letters (a, b) within rows differ significantly from one another, p < .02. ICS = Interpersonal Competence Scale; AGG = aggressiveness; POP = popularity; AFF = social affiliation; OLY = Olympian; ACA = academic abilities; SC = self-concept.
Table 4 shows that both groups revealed poor social skills. The teachers and control children produced similar answers in the areas investigated by the ICS (with no significant differences between them), but the children with symptoms of ADHD tended to judge themselves less aggressive, AGG: F(1, 19) = 8.04, p = .010,
Using one-way ANOVAs, the two groups were also compared (Table 5) in terms of the three subscales in the MSC, and of the children’s loneliness and social dissatisfaction self-report. These analyses revealed no statistically significant differences between the two groups on any of the three subscales in the MSC or in the children’s loneliness and social dissatisfaction self-report.
T Scores in the Two Groups (Controls With Weak Social Abilities and Symptoms of ADHD) in the MSC and Loneliness Questionnaires.
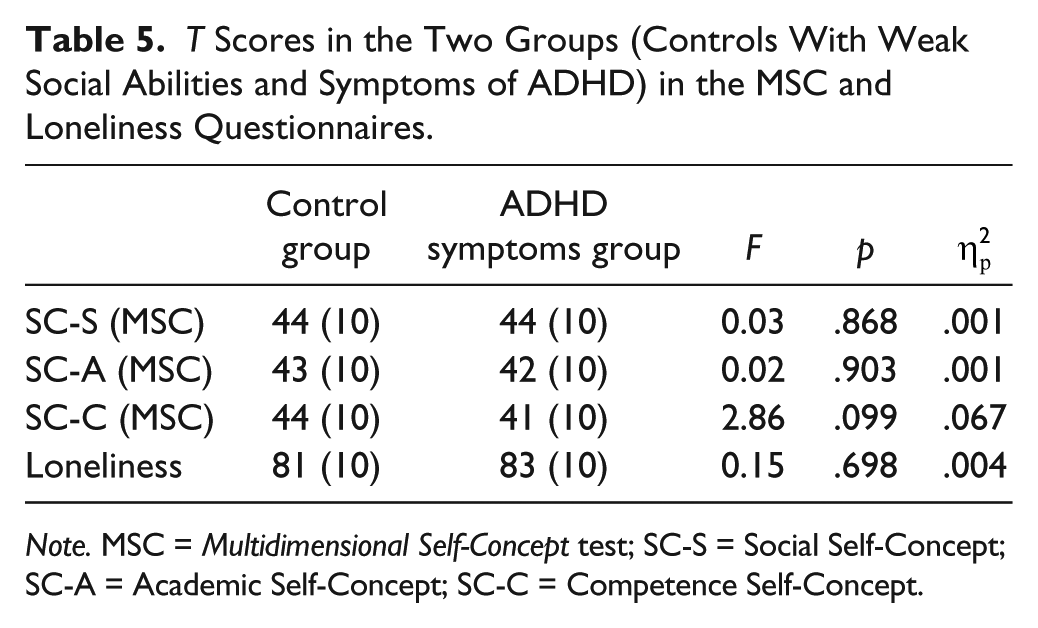
Note. MSC = Multidimensional Self-Concept test; SC-S = Social Self-Concept; SC-A = Academic Self-Concept; SC-C = Competence Self-Concept.
As these two groups of children had weak social abilities (with or without symptoms of ADHD), they were compared with the rest of our sample, that is TD children with moderate to strong social skills (n = 154; social ability COM: M = .42, SD = .91), to identify any differences in self-assessed self-concept and loneliness. Differences were found on all three subscales in the MSC between the two groups with weak social abilities (controls and group of children with ADHD symptoms) and the TD children, with this latter group exhibiting a higher self-concept in all the three areas—SC-S: F(1, 194) = 5.23, p = .006,
Discussion
The main goal of our study was to examine PIB, peer relations, self-concept, and loneliness in children with symptoms of ADHD. For this purpose, we asked primary schoolchildren attending second, fourth, and fifth grades to complete several questionnaires about their preferences in peer relations (sociometric questionnaire), their perception of self-competence in social and relational abilities (ICS), their self-concept (MSC), and their sense of loneliness (Loneliness). We also asked their teachers to complete three questionnaires, one on any behavior suggestive of ADHD, another on related problems (SDAI and COM), and one on children’s social and relational abilities (ICS).
A first objective was to see whether children with symptoms of ADHD were more likely to be rejected and less often preferred as classmates, and how this situation changed with age during primary school. A second objective was to compare children’s self-perception with their teachers’ perception of their social and relational difficulties, both in children with symptoms of ADHD and in a control group with weak social abilities matched for age and gender. Then these two groups’ self-concept and loneliness were also compared with a group of TD children.
Regarding our first aim, our results suggest that children with symptoms of ADHD are less likely to be preferred and more likely to be rejected than their peers. The percentage of children rejected followed an opposite trend over time when the children with symptoms of ADHD were compared with the TD children: The latter showing a declining rejection index over time in all three dimensions (playmate, deskmate, and teammate), whereas the symptoms of ADHD group’s likelihood of being rejected was already high in second grade, and continued to increase in all three areas.
As for the second aim, we compared the group of children with symptoms of ADHD and control children’s self-perception and their teachers’ perception of any social and relational difficulties, using the ICS. Although both groups of children had weak social skills, the teachers and control children gave similar answers in the areas investigated by the ICS, whereas the children with symptoms of ADHD tended to see themselves as less aggressive, more popular, and faring better on AFF and interpersonal competence than was reported by their teachers. These findings would support the hypothesis that PIB is associated with ADHD symptoms rather than with social difficulties, given that both groups of children were similarly weak in social skills (Owens et al., 2007).
As for the results concerning self-concept and loneliness, we found that children with social difficulties—with and without symptoms of ADHD—revealed a lower self-concept than TD children, but the sense of loneliness was similar in the children in all three groups. Comparing the results of children with social difficulties—with and without symptoms of ADHD—with normative data from the Italian adaptation of the MSC (Bracken, 2003), we found that their T scores ranged between 40 and 45, indicating a medium self-concept, even if lower than TD peers. These findings are consistent with reports in the literature of children with ADHD showing a lower self-concept than TD children (Wehmeier et al., 2010), but experiencing much the same sense of loneliness (Diamantopoulou et al., 2005; Heiman, 2005; Houghton et al., 2015). These findings are not in contrast with the hypothesis that PIB could be a coping mechanism that protects children’s self-concept (Hoza et al., 2004; Hoza et al., 2002). In fact, we found that children with ADHD symptoms of estimated themselves as having good social abilities and average self-concept, and the same was true for children with weak social abilities without ADHD symptoms. The sense of loneliness, moreover, seemed to be uninfluenced by the social difficulties experienced by the children in both groups (with and without symptom of ADHD), in fact no differences was found with children of the control group but all children reported a high level of perceived loneliness. The reason for this might relate to the characteristics of the questionnaires adopted. The MSC poses practical questions about the children’s school marks and their friends (e.g., “I’m satisfied with my reading literacy marks”), whereas the questions on loneliness are more theoretical (e.g., “I often get lonely”), and might be more difficult for primary schoolchildren to understand.
In our view, this study has some important clinical and educational implications. For a start, it demonstrates that, children with symptoms of ADHD showed signs of PIB, and this phenomenon give them a medium self-concept, even if lower than TD children. Furthermore, as previously found in the literature (Ohan & Johnston, 2011), even in our sample seems that PIB protects children with symptoms of ADHD from anxiety and depression. In fact, our children did not show psychiatric symptoms, and previous findings (Lee, Falk, & Aguirre, 2012; McQuade et al., 2014) suggested that PIB is associated with lower levels of depressive symptoms in children with ADHD, and in particular in those less preferred by their peers.
It is worth noting that being aware of their deficiencies could also help to motivate people to take action on their behavior (Hoza & Pelham, 1995), whereas inaccurate estimations of their capabilities could interfere with any treatment they receive. Either way, our study may contribute to our understanding of the PIB phenomenon, and its consequences on self-concept in children with ADHD, although this issue warrants further research.
The present study has some limitations to bear in mind, including the small number of children involved of different grades, the modest involvement of their parents, and the absence of any measures of other problems (learning difficulties, internalizing symptoms). Further research should thus examine the construct of loneliness, and why children with ADHD generally do not appear to feel lonely despite tending to be rejected by their peers. Even with the abovementioned limitations, our findings may have important implications for training implemented to develop ADHD children’s social abilities in class (such as cooperative learning, for example, Capodieci et al., 2016) from the first years of primary school to prevent any worsening social relations and rejection by peers. Future studies should also analyze certain aspects of PIB and how it relates to self-concept and loneliness in more depth to ascertain whether our findings can be generalized to other samples.
In conclusion, our study supports the hypothesis that children with symptoms of ADHD tend to be rejected and that the approval of their peers decreases over the years. Our findings also support the hypothesis of PIB in children with symptoms of ADHD, regardless of their social skills: Compared with a control group of children with weak social abilities (but no symptoms of ADHD), the children with ADHD tended to judge themselves as being less aggressive, more popular, and better in terms of AFF and interpersonal competence than their teachers reported. Whether and to what degree children with ADHD may experience a sense of loneliness remains to be investigate more in depth.
Footnotes
Acknowledgements
The authors are grateful to Professor Cornoldi who supported in this study and to Frances Coburn for her valuable suggestions and English revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.