
Abstract
Introduction
Elevated placebo effects have been repeatedly reported in clinical trials of adults with ADHD, generating interest in the characterization of its occurrence. A strong placebo response has been noted in several psychiatric disorders, including depression, insomnia, and anxiety (Weimer, Colloca, & Enck, 2015a). Placebo effects have been described as genuine psychological or physiological effects, which are attributable to receiving a substance but are not due to the pharmacological properties of that substance (Stewart-Williams & Podd, 2004). Koshi and Short (2007) described several psychological explanations of the placebo response. They suggested two major mechanisms: conditioning, which is a learning mechanism that occurs at the unconscious level, and the patient’s expectations from the administered “medication,” which occur at the conscious level as they are based on former knowledge and beliefs about the medications (Koshi & Short, 2007). As many participants involved in clinical trials have had numerous previous exposures to medications and their effects, the act of taking a “medication” can itself serve as a conditioned stimulus, triggering the expectancy of a reward (i.e., desired outcome). A participant’s positive expectations may also reduce anxiety and/or activate reward mechanisms in the brain (Benedetti, 2014). This may have important implications for the placebo response in ADHD, as an association between reward pathway dysregulation and ADHD has been demonstrated (Volkow et al., 2009). Neuroimaging studies have shown that expectations of symptom improvement involved in the placebo response are driven by frontal cortical areas, particularly the dorsolateral prefrontal, orbitofrontal, and anterior cingulate cortices, as well as other areas involved in the expectancy of receiving a reward, such as the ventral striatum (Lidstone & Stoessl, 2007). These areas are among some of the same brain regions that have been implicated in the pathophysiology of ADHD (Castellanos & Proal, 2012). Considering the role of the neurotransmitter dopamine (DA) in both the pathophysiology and pharmacotherapy of ADHD, it is plausible that alterations in DA may mediate the placebo effects in this disorder. Accordingly, the DAergic system has been found to be involved in the placebo response in several neurological conditions, suggesting that there could be common placebo mechanisms involved in different disorders (Benedetti, 2014).
Beyond understanding the nature of the placebo effect, predicting which individuals will develop a placebo response could be of great benefit for both research and clinical practice. A comprehensive review of more than 500 randomized placebo-controlled trials in psychiatry attempted to predict the factors associated with increased placebo response (Weimer, Colloca, & Enck, 2015b). The study revealed that only three of the 20 factors analyzed were associated with greater placebo effects: low baseline severity of symptoms, more recent trials, and unbalanced randomization (trial designs with more patients assigned to the drug arm than the placebo; Weimer et al., 2015b). Interestingly, demographic factors did not reveal any consistent results. The review did not find any additional predicting factors when taking into account different types of studies, such as randomized controlled trials of nondrug interventions or laboratory studies (Weimer et al., 2015b).
There are little data available comparing the placebo effect sizes between different primary measures in ADHD. The rate of the placebo response in adults with ADHD ranges between 17% and 40% depending on the criteria of response used, and was often measured using self-report scales (Waxmonsky, Waschbusch, Glatt, & Faraone, 2011). It is plausible that the choice of measurement tool and criteria for response play a central role in the detection of placebo effects. One study that did look at several efficacy measures showed that response and remission rates on both the placebo and drug arms were typically lower on the Clinical Global Impressions–Improvement scale (CGI-I)-based definition as compared with the ADHD Rating Scale–IV (ADHD-RS-IV; Waxmonsky et al., 2011). Moreover, there was an association between lower symptom severity and higher levels of placebo response in both adult and pediatric patients with ADHD (Waxmonsky et al., 2011). In contrast, a retrospective study of two randomized trials in adults with ADHD, using Conners’ Adult ADHD Rating Scale (CAARS)-Observer-Rated, demonstrated that higher symptom severity predicted higher placebo response rates (Buitelaar et al., 2012). The same study also found other possible predictors of placebo response in adults with ADHD: younger age, shorter time since diagnosis, and lower educational level. Although younger age has been associated with a lower placebo response in other ADHD studies, causality has not been established (Manor et al., 2008; Newcorn et al., 2009). A study that compared pediatric with adult populations found higher placebo effects on the pediatric population (Khan, Fahl Mar, & Brown, 2017), though in ADHD placebo response is thought to be higher in adults (possible due to the relative absence of hyperactivity).
In summary, there are no consistently reported predictive factors mediating the placebo response in patients with ADHD, as there are only a few studies that have attempted to draw conclusions about the placebo effects in ADHD. Thus, the present study aimed to characterize the placebo response in adults with ADHD. To this end, we analyzed data from a double-blind, randomized placebo-controlled trial of a nonstimulant drug candidate (metadoxine) using gold-standard measures in registration clinical trials, namely the CAARS and the Adult ADHD Self-Report Scale (ASRS). Unfortunately, due to lack of data we were unable to suggest a reasonable, evidence-based, hypothesis.
Method
This is a retrospective cohort analysis of the placebo arm of a 6-week randomized, multicenter, double-blind study of metadoxine 1,400 mg/day in adults with ADHD (Weisler et al., 2014). It was done in 20 research centers: 18 centers in the United States and two in Israel. Included were 140 adults (aged 18-55 years) with ADHD who completed the entire 6-week study and were treated with placebo.
The mean age was 35.8 ± 10.5 years. About 75 (53.6%) participants were female. The study was approved by the Institutional Review Board (IRB) of all the centers involved, and all participants provided informed consent to participate. The main inclusion criterion was either Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) or Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) diagnosis of ADHD, with at least moderate clinical severity, as determined by the Adult ADHD Clinician Diagnostic Scale (ACDS version 1.2) modified for DSM-IV-TR and DSM-5, Clinical Global Impression-Severity score ≥4 and CAARS–Investigator-rated total score ≥22. Main exclusion criteria were treatment resistance to ≥2 previous trials of either stimulant or atomoxetine treatment of ADHD, pregnancy or lactation, a major non-ADHD psychiatric diagnosis, alcohol or substance use disorders, clinically significant or unstable general medical condition (as determined by medical history, physical examination, and laboratory and electrocardiogram [ECG] tests), and recent or concomitant use of psychotropic medications or supplements for ADHD. Following baseline assessment and randomization, participants were monitored weekly. After a 2-week run-in period, the study lasted 6 weeks under treatment, with a clinical visit once weekly. The CAARS was completed every week except Week 5. One follow-up visit was conducted at Week 8.
Measures
CAARS–Investigator rated
The CAARS has a validated investigator-rated version, the CAARS-Inv (Conners, 1999), which was used in this study for baseline assessment and as the primary endpoint. The CAARS was collected weekly throughout, except Week 5, when there was not an office visit. The CAARS includes the inattentive (Subscale A or CAARS-A), hyperactive-impulsive (Subscale B or CAARS-B), and total ADHD (Subscale C or CAARS-C) scores, and the ADHD index (Subscale D or CAARS-D). CAARS-A and -B are based on the DSM criteria, and CAARS-C is the summary of both. CAARS-D includes 12 additional questions which do not reflect the DSM criteria but address other aspects of ADHD—such as emotional dysregulation, self-esteem, and to a lesser extent, impairment in executive function. The CAARS internal consistency measures vary considerably (αCronbach = .49-.97), whereas test–retest reliability is reasonably high (.77-.91; Smyth & Meier, 2019). Estimates of discriminant validity for CAARS and anxiety measures (e.g., Hamilton Anxiety Scale, State-Trait Anxiety Inventory, etc.) indicate that this is overall low (.40-.65; that is, the constructs are reasonably but not perfectly discordant; Smyth & Meier, 2019).
ASRS
The ASRS is the World Health Organization’s (WHO) rating scale for adult ADHD, which aims to assess current symptoms (Fredriksen et al., 2014). The ASRS contains 18 items regarding the frequency of recent DSM-IV (4th ed.; DSM-IV; APA, 1994) Criterion A symptoms adapted for adults and measured on a 5-point Likert-type scale (Adler et al., 2006; Fredriksen et al., 2014). The ASRS has internal consistency with the rater-administered ADHD Rating Scale (ADHD-RS; Adler et al., 2006). Normative data and information on several populations are available for the ASRS, which has been translated into many languages (Fredriksen et al., 2014).
Additional measures
A variety of physiologic measures were obtained, including heart rate and blood pressure, body mass index (BMI) and the monitoring of specific adverse events that might qualify as nocebo responses (e.g., nausea, headache, fatigue, and nasopharyngitis-like symptoms).
Placebo Profile Definition
To define the placebo response, we used two terms: intensity—that is, what was the size of the effect—and frequency—that is, what was the percentage of weeks in which there was a placebo response. As no clear definition of the intensity or the size of the placebo response in ADHD was found in our literature review, an arbitrary definition was suggested, ranging from mild (25% improvement) to moderate (33% improvement) to large (>40% improvement). This procedure was used for both the CAARS-Inv and the ASRS. For the ASRS, according to the literature, improvement is defined by the total scores (Kessler et al., 2007): Mild improvement was defined as an achievement of a score <24 and large as <17. It should be noted that the methods of measuring the placebo response for CAARS and ASRS are different, using the rate of change and the total score, accordingly. This difference might, in itself, influence the determination of the placebo response. Also, to investigate the existence of possible profiles of placebo response in ADHD, we defined several different profiles: An early-only placebo response was defined as achieving a significant response of at least mild intensity by Week 1, followed by a nonresponse in every visit between Weeks 3 and 6. A late-only placebo response was defined as achieving a response at Week 6, with a nonresponse in every visit between Weeks 1 and 4. A consistent placebo response was defined as achieving a response by Week 1 or 2, followed by significant responses in all of the following visits until the end of the study. Participants who exhibited a placebo response at any point during the study but did not meet any of the above profiles were defined as having a variable placebo response.
Statistical Analysis
We used SPSS for Windows ver. 22 (IBM Inc., Chicago, IL) for statistical analysis. Descriptive statistics are expressed as number or mean accompanied by standard deviation (SD) or rate (%) as appropriate. One-way ANOVA with repeated measures (ANOVA-RM) was used to assess changes in the CAARS and ASRS scores during the study. A value of p < .05 was considered significant, p < .01 highly significant, and p > .05 nonsignificant. Binary logistic regression was used to predict significant placebo responses with demographic and clinical data.
Results
The study included 140 adults (aged 18-55 years) with ADHD who completed the entire 6-week study and were treated with placebo. The mean age was 35.8 ± 10.5 years. The M:F rate was 46.4%:53.6% accordingly. The ADHD presentations were as follows: Inattentive type = 37.7%, Hyperactive = 1.4%, Combined = 61%.
CAARS
The mean baseline CAARS value was 38.0 ± 8.0. For the one-way ANOVA-RM for the CAARS, the assumption of sphericity was violated (Mauchly’s test p < .01), and epsilon correction according to the Greenhouse-Geisser test was used (ε = .53). Placebo treatment elicited a significant improvement in the CAARS over time, F(2, 404) = 61.2, p < .00001, partial η2 = .31, η2 = .11. Mean CAARS scores improved from 38.0 ± 8.0 at baseline to 27.5 ± 11.7 at Week 6, which is a 27.6% improvement. CAARS placebo response proportions for each week of the study are shown in Table 1, and placebo response profiles for CAARS are shown in Table 2.
CAARS Placebo Response by Weeks (N = 140, Only 6-Week Completers).

Note. See Method for definitions of placebo profiles. CAARS = Conners’ Adult ADHD Rating Scale.
Placebo Response Profiles in Various Placebo CAARS Reduction Cutoff Criteria.
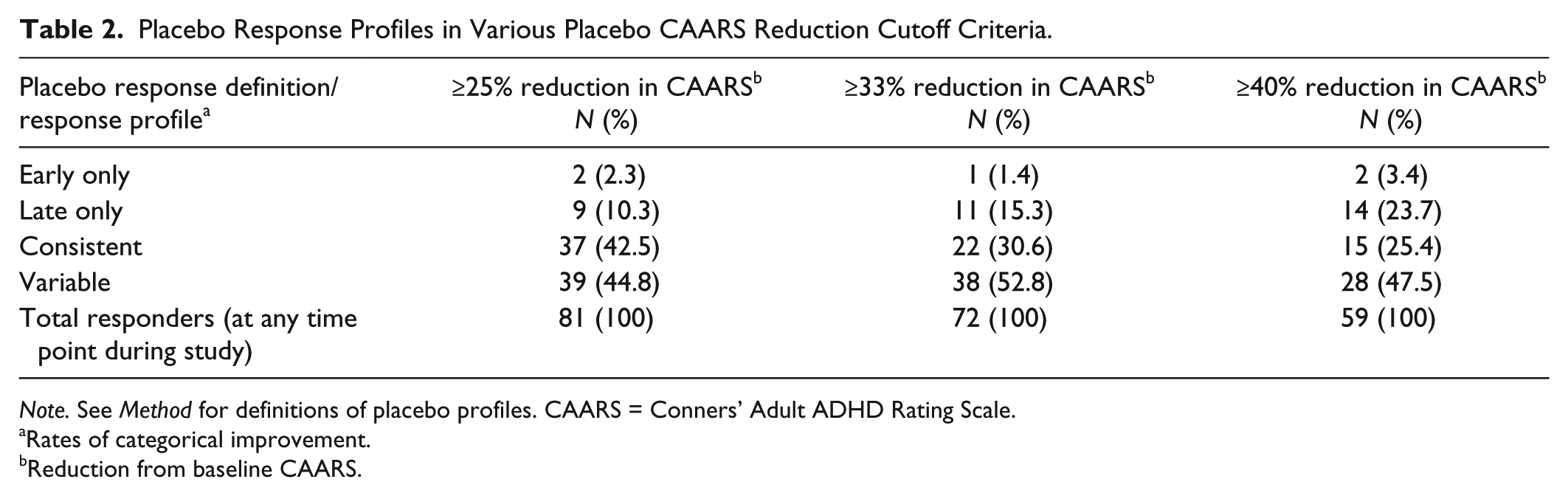
Note. See Method for definitions of placebo profiles. CAARS = Conners’ Adult ADHD Rating Scale.
Rates of categorical improvement.
Reduction from baseline CAARS.
A separate logistic regression analysis was conducted to predict a placebo response at Week 6 by determining placebo responses at specific earlier weeks of the study (Table 3). The results show that an early placebo response on the CAARS predicts an end-of-study placebo response on the CAARS (Week 1 and onward; Figure 1).
Placebo Response Prediction at End of Study (Week 6).
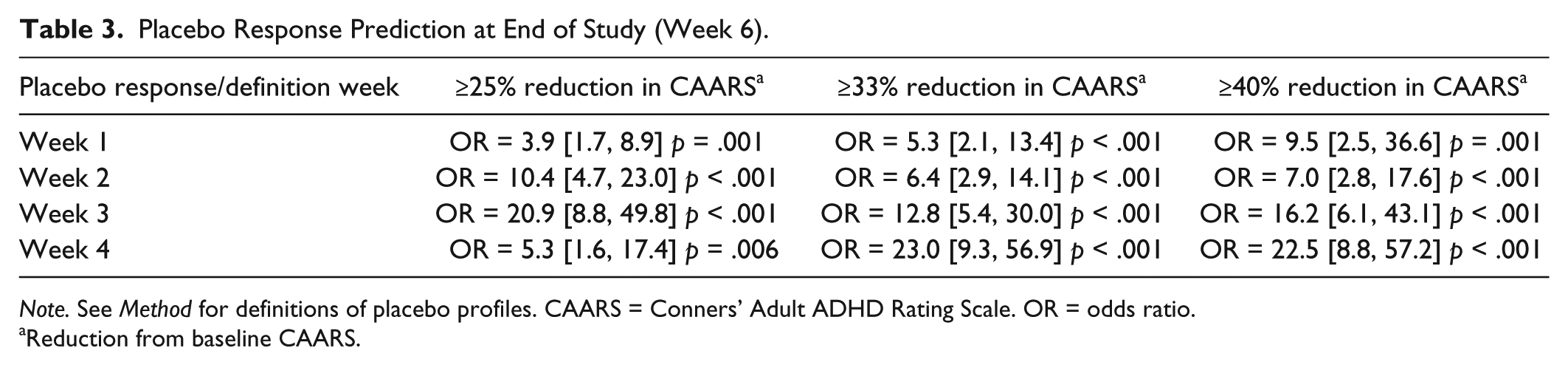
Note. See Method for definitions of placebo profiles. CAARS = Conners’ Adult ADHD Rating Scale. OR = odds ratio.
Reduction from baseline CAARS.
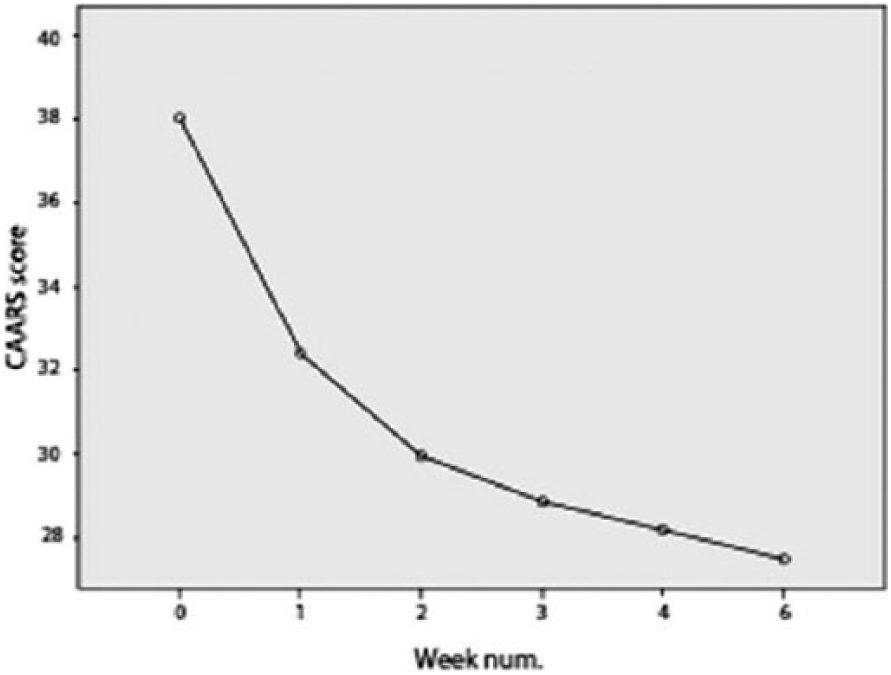
Time of course of alterations in CAARS score during the study.
ASRS
The mean baseline ASRS value was 47.4 ± 11.0. For the one-way ANOVA-RM for the ASRS, the assumption of sphericity was violated (Mauchly’s test p < .01), and epsilon correction according to the Greenhouse-Geisser test was used (ε = .46). Placebo treatment elicited a significant improvement in ASRS scores over time, F(2, 383) = 43.1, p < .00001, partial η2 = .24, η2 = .07. Mean ASRS scores improved from 47.4 ± 11.0 at baseline to 36.8 ± 13.5 at Week 6, which is a 22.3% improvement. ASRS placebo response proportions for each week of the study are shown in Table 4, and placebo response profiles for ASRS are shown in Table 5. It should be noted that although the response pattern is quite similar to what was seen with the CAARS, the intensity of the response is smaller. This could either be due to the measures themselves, the different raters (self vs. investigator), or the definition of placebo response used for the different scales (as these were not the same).
ASRS Response by Weeks (N = 140, Only 6-Week Completers).

Note. ASRS < 24: Less likely to have ADHD; ASRS < 17: Unlikely to have ADHD. ASRS = Adult ADHD Rating Scale.
Placebo Response Profiles in Different Placebo ASRS Reduction Cutoff Criteria.
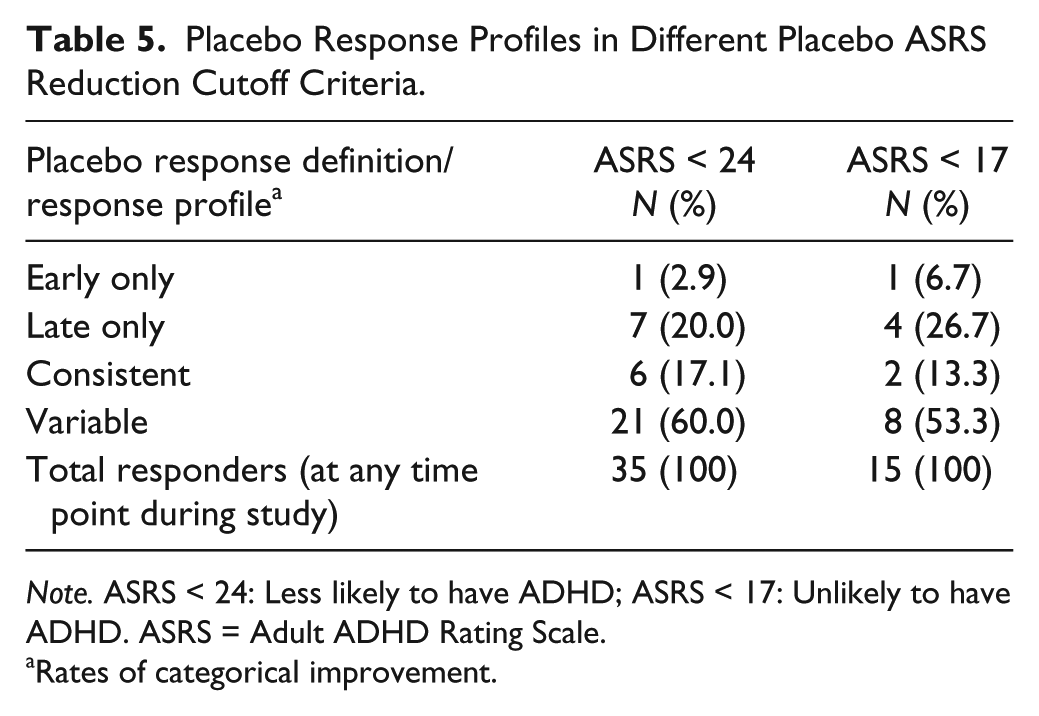
Note. ASRS < 24: Less likely to have ADHD; ASRS < 17: Unlikely to have ADHD. ASRS = Adult ADHD Rating Scale.
Rates of categorical improvement.
A separate logistic regression analysis was conducted to predict a placebo response at Week 6 by determining ASRS placebo responses at specific earlier weeks of the study (see Table 6). The results show that an early placebo response predicts an end-of-study placebo response on ASRS (Week 2 and onward; Figure 2).
Placebo Response Profiles in Different Placebo ASRS Reduction Cutoff Criteria.
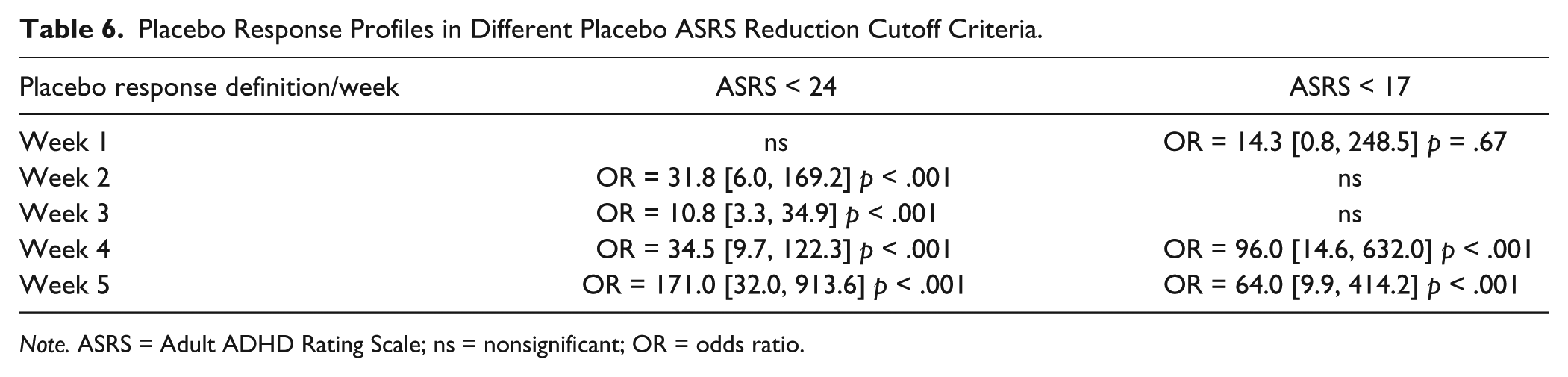
Note. ASRS = Adult ADHD Rating Scale; ns = nonsignificant; OR = odds ratio.
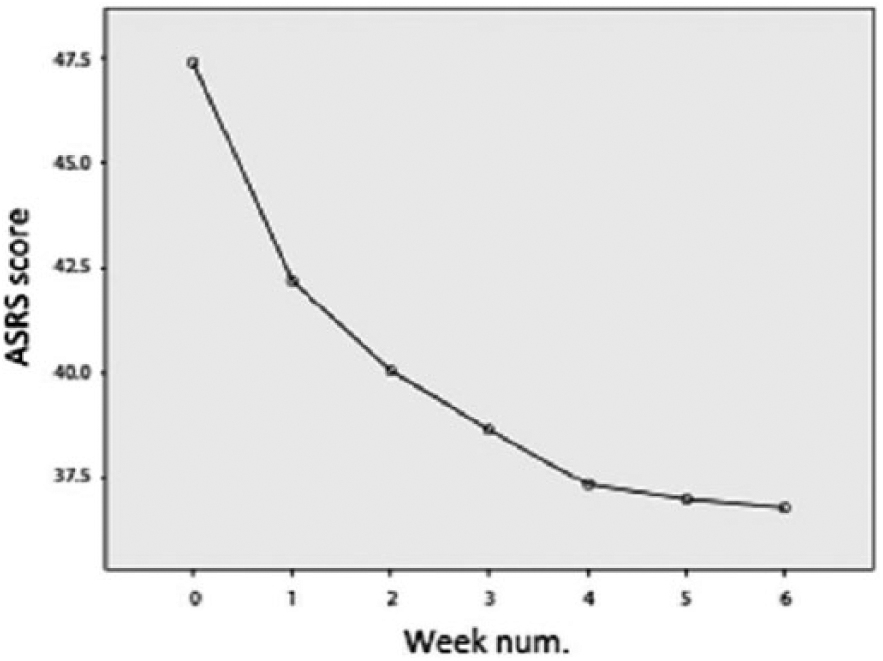
Time course of alterations in ASRS during the study.
Baseline ASRS severity did not predict end-of-study placebo response (p > .15 for both response cutoff definitions). Baseline CAARS severity did not predict an end-of-study placebo response (p > .05 for all cutoffs).
To predict the likelihood of a significant placebo response (defined as ASRS < 17) at the end of the study (Week 6), we conducted a binary logistic regression with the following independent variables: age, gender, systolic blood pressure, BMI, and specific nocebo responses (nausea, headache, fatigue, and nasopharyngitis). A significant model was retrieved, χ2(9) = 22.7, p = .007, Nagelkerke R2 = .37, correctly classifying 94.3% of cases. Nausea significantly predicted an end-of-study placebo response, odds ratio (OR) = 13.9, p = .03, 95% confidence interval (CI) = [1.3, 145.9]. None of the other variables were predictive of an ASRS placebo response at Week 6.
Discussion
The Placebo Response in Self- vs. Clinician-Rated Measures
This study assessed the placebo response in adults with ADHD using the placebo arm of a randomized double-blind study of a nonstimulant investigational medication (metadoxine). Administering the placebo as an arm in a nonstimulant study may enhance our ability to draw conclusions regarding the placebo response compared with other studies of stimulants, in which drug-treated participants are less blinded due to the obvious sympathomimetic adverse effects. Here, the participants are really unaware of the nature of the compound, have no clue of their possible response, and sometimes might be even misguided by expected typical side effects such as nausea. Hence, nonstimulant placebo responses may better reflect the true nature of the placebo response in ADHD due to this lack of obvious side effects. This is a relative advantage of this study.
Both the self-report (ASRS) and clinician-rated (CAARS-Inv) measures showed a significant improvement in scores with time. Surprisingly, placebo response rates were generally higher for clinician-rated (CAARS) than for self-rated (ASRS) measures. Although these are different scales, this finding may indicate a possible additive effect in placebo responses, in which the participant’s responses may be amplified by clinician expectations and/or interpretations, leading to higher “improvement” in the clinician rating. Alternatively, the difference in placebo response estimation between CAARS and ASRS may reflect the different calculations of the placebo response by the two measures. The contribution of rater to placebo response is not entirely a new idea; for example, placebo responses in children seem to stem primarily from their parents’ perception of improvement (the so-called “placebo response by proxy”; Waschbusch, Pelham, Waxmonsky, & Johnston, 2009). In addition, although a previous review concluded that the CAARS has overall good psychometric properties (αCronbach = .74-.92, 82% sensitivity, 87% specificity; Taylor, Deb, & Unwin, 2011), a large (n = 756) recent study on postsecondary students with and without ADHD (Mage = 21.2 and 22.2 years, respectively) found a low negative predictive value (68%-71%), casting doubt on the utility of the CAARS as a single screening measure for adult ADHD (Harrison, Nay, & Armstrong, 2019). This finding supports the notion that clinical trials should beware of the difficulties of both self-report and investigator-rated measures in determining response, the one not better than the other. It is suggested that comparable methods of estimating the placebo response should be developed for direct comparison.
Time Course of the Placebo Response
Placebo response rates were found to increase toward the end of the study for both the CAARS-Inv and ASRS, regardless of the response cutoffs. This finding is consistent with the results of Waxmonsky et al. (2011), who found slower times to response in participants receiving placebo compared with active treatment. It could be that the placebo response takes time to reach its peak, perhaps similar to the subacute and chronic therapeutic effects seen with numerous psychotropic medications. Or, it could be that the expectations of the participants change over time when there is not a response. It remains to be tested what mechanisms are involved in such evolving responses. One possibility is that unintended therapeutic interactions with the clinicians who collect data for the study may enhance the placebo response with time. It could also be that participants are expecting a response and believe that the investigators expect it too, and thus, in the final assessment they overestimate the benefit of the treatment.
One possible implication is that relatively short (e.g., ≥4-week) trials may be more adequate for managing placebo-controlled comparisons, with a longer duration of exposure carrying increased risk for placebo response and less adequate drug–placebo discrimination. It should be noted that the assumption that the nature of response will be similar in participants treated with placebo and active medication may not be the same (i.e., participants treated with active drug may report improvement earlier in treatment, whereas those on placebo may preferentially report it later on). In addition, in longer trials (>4 weeks) the placebo response might be amplified by the investigator–participant relationship or other factors related to expectancy.
Given the high placebo response in adult ADHD trials, it is reasonable to wonder whether concomitant use of rating and objective measures could help constrain the placebo response. This approach remains to be tested. The difficulties encountered with clinician ratings and self-report measures in this study suggest that reliable and valid objective measures may be helpful enhancing drug–placebo discrimination. Of course, this is only a speculation, and requires more systematic study.
There is much to be learned from the time course to response in placebo-treated adults in this study. As early as Week 1 for the CAARS-Inv and as early as Week 2 for the ASRS, the occurrence of placebo response significantly increased the likelihood of an end-of-study placebo response. This finding would be consistent with the practice of using placebo lead-in to minimize placebo response (as early responders would be thrown out). However, the most frequent placebo response profile was variable for both CAARS-Inv and ASRS, followed by either a consistent response profile (for CAARS-Inv) or a late-only response profile (for ASRS). This suggests an inconsistency in placebo responsivity within the same individual, and therefore attempting to manage placebo response by excluding placebo responders after an initial exposure to treatment may not be adequate. It should be noted that using stricter placebo cutoff criteria seems to lead to a shift to the late-only profile, with some decrease in the high variable profile. Therefore, defining a stricter response threshold is not adequate to estimate placebo response. It is suggested that the variability of the placebo response in ADHD may be akin to the variability in the presentation of the ADHD symptoms, which is typical to the disorder (Klein, Wendling, Huettner, Ruder, & Peper, 2006). Hence, it is suggested that a novel standardized calculation based on a composite score of several visits’ assessments may be needed for a reliable evaluation of medications’ efficacy in ADHD.
Clinical Predictors of an End-of-Study Placebo Response
Consistent with previous studies, demographic variables (e.g., age, gender) did not predict an end-of-study placebo response. However, one clinical variable showed a tendency to predict a placebo response: the nausea. It is likely that nausea can be a predictor of placebo response. Nausea is a well-known side effect of many medications; and it is reasonable that participants experiencing nausea may believe that they are receiving a medication rather than placebo. This may partially explain why placebo response which occurred in the context of nausea had a tendency to predict an end-of-study placebo response for both CAARS and ASRS in this study.
Limitations and Conclusion
The current investigation is limited by its being based on a single study and being about a specific drug. It is also constrained by the lack of objective measures to assess attentional performance. However, objective measures of ADHD symptoms (e.g., continuous performance tests or other related measures of attention or inhibitory control) are generally considered as secondary outcome measures, and the aim of this study was the evaluation of primary rating measures in relation to placebo response.
In addition to the above limitations, several demographic and clinical variables were not investigated in the current study, and should be considered in future studies, such as socioeconomic status, cigarette smoking, and analysis by previous treatment status.
In conclusion, this study aimed to characterize the magnitude, the time course, and the predictors of placebo response in an adult ADHD clinical trial. It shows a substantial rate of placebo response, including what was defined as large placebo response (>40% symptom change). It shows a specific pattern of placebo response, in which variable pattern is the most common. This observation, if replicated, indicates a need to develop new methods to calculate efficacy and to attenuate the placebo response. Options include the use of a composite score based on both rating instruments and objective measures, and a composite score based on assessments conducted at several visits. Further studies are warranted to identify the mechanisms involved in placebo response in ADHD, in an attempt to develop more accurate assessments of medications’ efficacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The data presented in this study were collected from the placebo arm of a study funded by Alcobra Ltd., however, there was no involvement of Alcobra Ltd. in the content and/or the interpretation of the results of the present study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drs. Ben-Sheetrit, Newcorn, Danieli, Weizman, Peskin and Manor participated in a series of studies funded by Alcobra Ltd.