
Abstract
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a childhood-onset neurodevelopmental disorder characterized by pervasive and impairing symptoms of inattention, hyperactivity, and impulsivity, with a prevalence in adults estimated between 2.1% and 2.5% (Simon, Czobor, Balint, Meszaros, & Bitter, 2009; Vitola et al., 2017). ADHD in adults is associated with high rates of psychiatric comorbidity, with an odds ratio of having one, two and three comorbid Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) disorders of 3.0, 6.2, and 9.6, respectively (Fayyad et al., 2016). Internalizing symptoms are one of the most prevalent ADHD comorbid conditions in adulthood (Kessler et al., 2006; Piñeiro-Dieguez et al., 2016), especially in women (Edvinsson, Lindström, Bingefors, Lewander, & Ekselius, 2013; Müller et al., 2017; Piñeiro-Dieguez et al., 2016; Solberg et al., 2018). Having a higher education and a job is related to a lower probability of comorbidity (Anker, Bendiksen, & Heir, 2018), whereas a higher risk of co-occurring internalizing disorders is related to ADHD symptom severity (Michielsen et al., 2013; Simon, Czobor, & Bitter, 2013) and persistence (Agnew-Blais et al., 2018; Cadman et al., 2016; Yoshimasu et al., 2018). The presence of comorbid internalizing disorders complicates the treatment (Biederman et al., 2008; Wilens, Nieremberg, Rostain, & Spencer, 2008), resulting in more severe impairment (Biederman, 2004; McIntyre et al., 2010).
Among internalizing problems, depression and anxiety symptoms have been consistently associated with adult ADHD (Biederman, Petty, Clarke, Lomedico, & Faraone, 2011; Grogan & Bramham, 2016; Kessler et al., 2006; Michielsen et al., 2013; Simon et al., 2013). In addition, these comorbid symptoms increase in severity with age (Bramham et al., 2012). Persistent ADHD is related to higher rates of comorbid depression and anxiety disorders compared with remittent ADHD and healthy controls (Biederman et al., 2011), and vice versa; ADHD symptom rates are increased among individuals with severe and chronic depression and comorbid anxiety disorders (Bron et al., 2016). Recent evidence suggests that this relationship might be partially explained by shared genetic factors (Chen et al., 2016; den Berg & Marcoen, 2004; Rydell, Taylor, & Larsson, 2017; Segenreich et al., 2015) and mutual neurobiological deficits, as, for example, poor prefrontal activity and impairments in the limbic–cortical–striatal–pallidal–thalamic circuits (Katzman, Bilkey, Chokka, Fallu, & Klassen, 2017; Marwood, Wise, Perkins, & Cleare, 2018). But, nevertheless, environmental factors also play a crucial role, because growing up with ADHD usually leads to experiencing more adversity throughout life because of the impairment (e.g., social rejection, poor school/work performance, poor family relationships) caused by the symptoms of the disorder (Bernardi et al., 2012; Brown, Flood, Sarocco, Atkins, & Khachatryan, 2017; Garcia et al., 2012), which also contributes to a low mood and feelings of anxiety (Bramham et al., 2012).
These difficulties, in addition to the negative social feedback received since childhood (S. Young et al., 2008), have also been associated with the development of another major internalizing symptom that is often linked with adult ADHD: problems with self-esteem (Cook, Knight, Hume, & Qureshi, 2014; Newark, Elsässer, & Stieglitz, 2016). In adults, self-esteem is negatively correlated to current ADHD symptomatology (Dan & Raz, 2015). As expected, the negative impact of ADHD and its internalizing comorbidities is also related to a lower perceived quality of life (QoL; Bernardi et al., 2012; Gudjonsson, Sigurdsson, Eyjolfsdottir, Smari, & Young, 2009; Quintero, Morales, Vera, Zuluaga, & Fernández, 2017).
Emotional dysregulation (ED) has been defined as a multidimensional construct that involves the lack of inhibition of behavior associated with strong negative or positive emotion and subsequent failure to engage in self-regulatory actions (Mitchell, Robertson, Anastopolous, Nelson-Gray, & Kollins, 2012). ED constitutes another key internalizing problem related to ADHD throughout the lifespan (Shaw, Stringaris, Nigg, & Leibenluft, 2014) and is a major cause of impairment (Corbisiero, Mörstedt, Bitto, & Stieglitz, 2017), independently of other comorbid conditions (Vidal et al., 2014). At the same time, research suggests that ED is a key risk factor for internalizing psychopathologies, such as anxiety and depressive disorders (Bertocci et al., 2016), and that adults with ADHD with a current comorbidity present significantly more severity of ED (Corbisiero et al., 2017). Three models have been proposed to explain the overlap between ED and ADHD symptoms (Shaw et al., 2014): (a) ED is a core diagnostic feature within ADHD; (b) both conditions are correlated, but constitute different dimensions; and (c) the combination of both of them forms part of a nosological entity by itself. The accumulated evidence up to now mainly supports the first model (Hirsch, Chavanon, Riechmann, & Christiansen, 2018; Retz, Stieglitz, Corbisiero, Retz-Junginger, & Rösler, 2012).
Pharmacotherapy remains the first line of treatment for adults with ADHD (National Institute for Health and Care Excellence, 2008), but mixed results have been found on comorbid internalizing symptoms (Adler et al., 2013; Epstein, Patsopoulos, & Weiser, 2014; Lenzi, Cortese, Harris, & Masi, 2018; Moukhtarian, Cooper, Vassos, Moran, & Asherson, 2017). In addition, different nonpharmacological interventions have been tested in treating adult ADHD core symptoms (e.g., DSM-5 symptoms: inattention, hyperactivity, and impulsivity) and also internalizing comorbidity outcomes have been reported.
Cognitive-behavioral therapy (CBT) has been adapted for treating ADHD in adults and is aimed at developing behavioral strategies to compensate for core neuropsychiatric deficits and change dysfunctional thinking styles (Safren, Sprich, Chulvick, & Otto, 2004). A number of randomized controlled trials (RCTs) using CBT approaches have found a positive effect on self-rated comorbid depression and anxiety symptoms (Dittner, Hodsoll, Rimes, Russell, & Chalder, 2018; Emilsson et al., 2011; Safren et al., 2005) and self-esteem (Stevenson, Whitmont, Bornholt, Livesey, & Stevenson, 2002), particularly at the follow-up (S. Young et al., 2015), whereas others have reported no change (Pettersson, Söderström, Edlund-Söderström, & Nilsson, 2014; Solanto et al., 2010; Virta et al., 2010b). In addition, all CBT trials measuring the effect on self-reported ED showed an improvement (Emilsson et al., 2011; S. Young et al., 2015). A better perceived QoL has been reported when comparing CBT with a treatment as usual (TAU) control group (S. Young et al., 2015), but others found no change, in comparison with active control groups or waiting lists (Pettersson et al., 2014; Vidal-Estrada et al., 2013; Virta et al., 2010b).
Another of the most studied interventions is dialectical behavioral therapy (DBT) that was initially developed for treating borderline personality disorder (Linehan, 1993) and afterward adapted for adult ADHD (Hesslinger et al., 2002), as there are several similarities between both disorders (e.g., deficits in affect regulation, impulse control, substance abuse, low self-esteem). DBT aims at promoting the acceptance and validation of ADHD-related symptoms, on one hand, and, on the other hand, teaching the skills required for change and self-management (Hesslinger et al., 2002). Improvements in QoL and in comorbid depression have been reported by some DBT trials (Fleming, McMahon, Moran, Peterson, & Dreessen, 2015; Hesslinger et al., 2002; Morgensterns, Alfredsson, & Hirvikoski, 2016; Philipsen et al., 2007), but not when compared with active control groups (Fleming et al., 2015; Philipsen et al., 2015).
Likewise, mindfulness-based therapies (MBTs) have also been adapted to this population. MBTs are a type of meditative techniques that emphasize an observant and nonreactive stance toward one’s thoughts, emotions, and body states (Zylowska et al., 2008). MBTs have also been tested in adult ADHD with positive results in ED, both clinician (Mitchell et al., 2013) and self-reported (Hepark et al., 2015), mixed findings in anxiety symptoms (Gu, Xu, & Zhu, 2017; Hepark et al., 2015), and no improvements in depression (Hepark et al., 2015; Mitchell et al., 2013).
Neurofeedback (NFB) efficacy has been examined in ADHD adults as well, with mixed results in comorbid depression and anxiety (Arns, Drinkenburg, & Leon Kenemans, 2012; Mayer, Blume, Wyckoff, Brokmeier, & Strehl, 2016; Mayer, Wyckoff, Schulz, & Strehl, 2012; Salomone et al., 2015; Schönenberg et al., 2017) and self-reported improvement in self-esteem (Salomone et al., 2015). NFB is based on the fact that normalization of the altered brain activity through modulation by operant learning procedures can lead to improvements in cognitive and behavioral functioning in individuals with ADHD (Arns, Heinrich, & Strehl, 2014).
Cognitive training (CT) efficacy has also been studied in adult ADHD, and no improvements could be found in depression and QoL (Stern, Malik, Pollak, Bonne, & Maeir, 2016; Virta et al., 2010b). The purpose of CT is to remediate deficits in cognitive processes through the repetition of a specific activity that aims at improving a cognitive skill or a general cognitive ability (i.e., working memory, inhibition, attention; Rabipour & Raz, 2012).
Psychoeducation (PsyEd) programs which are focused on providing education and information about ADHD without practicing any skills have also been used in adults with ADHD. With these interventions, no improvements have been obtained in comorbid self-reported self-esteem, depression, or anxiety symptoms (Vidal-Estrada et al., 2013; Wiggins, Singh, Getz, & Hutchins, 1999). Finally, cognitive hypnotherapy has also been specially adapted for adult ADHD, and no changes have been observed in comorbid internalizing symptoms (Virta et al., 2010a).
Previous meta-analytic reviews have found that CBT (Knouse, Teller, & Brooks, 2017; Lopez et al., 2018; Z. Young, Moghaddam, & Tickle, 2016) and MBT (Cairncross & Miller, 2016) are effective in treating core ADHD symptoms, even in the long term (López-Pinar, Martínez-Sanchís, Carbonell-Vayá, Fenollar-Cortés, & Sánchez-Meca, 2018). Some of them have also found that self-reported anxiety depression and self-esteem were significantly improved with CBT, with no changes in QoL and when compared with active control groups (Jensen, Amdisen, Jørgensen, & Arnfred, 2016; Lopez et al., 2018). However, the effect of other interventions such as DBT, MBT, NFB, CT, PsyEd, or hypnotherapy on internalizing comorbid symptoms or the long-term efficacy has not been examined by these reviews. In addition, some significant studies published recently have not been included (Dittner et al., 2018; Hoxhaj et al., 2018; Schönenberg et al., 2017; Stern et al., 2016).
Furthermore, with regard to their methodologic quality, studies evaluating nonpharmacological interventions presented a different risk of bias and used different outcome measure sources or comparison group type, which could significantly change the treatment effect estimates (Cuijpers, Li, Hofmann, & Andersson, 2010; Higgins & Green, 2011; Karlsson & Bergmark, 2015). Previous meta-analyses found no difference between self-reported and clinician-reported comorbid anxiety and depression symptoms reduction (Jensen et al., 2016), but the improvements were not significant when compared with active control groups (Lopez et al., 2018). The importance of using placebo or active control groups has become a major issue in psychosocial clinical research (Wampold, Frost, & Yulish, 2016), although in this field it entails facing important methodological and theoretical challenges (Locher, Gaab, & Blease, 2018). These groups allow the control of nonspecific factors (e.g., expectation of improvement, therapeutic relationship, social contact, among others), and thereby the evaluation of the specificity of treatment ingredients included in the active intervention. This variable could have a crucial role in the effect estimates; since when placebo therapies are designed in an equivalent way (in terms of number and duration of sessions, training of therapist, format of therapy, and restriction of topics), differences with active treatments decrease (Baskin, Tierney, Minami, & Wampold, 2003).
Individual studies assessing nonpharmacological treatments also differed in terms of other clinically relevant variables, such as the setting of the intervention (i.e., individual or group therapy), percentage of participants under pharmacotherapy, treatment length, or participants’ age or sex, and this might moderate the effect of the intervention on internalizing symptoms (Bramham et al., 2012; Cunill, Castells, Tobias, & Capellà, 2016; Pozza & Dèttore, 2017; Solberg et al., 2018). The impact of these clinically relevant variables on the effect size has not been assessed by previous meta-analyses (Jensen et al., 2016; Lopez et al., 2018).
Likewise, the mechanism for the improvement of internalizing comorbid symptoms is still unknown. A possibility could be that the therapy directly improves these associated symptoms as the main CBT (Safren et al., 2004; Solanto et al., 2010; S. Young & Ross, 2007) and DBT (Hesslinger et al., 2002) programs include one or more sessions aimed at dealing with them. In the same way, some evidence has been found about the improvement of self-regulation of attention and emotion after mindfulness training (Teasdale, Segal, & Williams, 1995), which would support this first therapeutic pathway model. On the contrary, an alternative therapeutic pathway might be that internalizing comorbid symptomatology improves as a secondary gain from the reduction of ADHD core symptoms.
Thus, the main aim of this meta-analytic review was to evaluate the efficacy of different nonpharmacological interventions (CBT, DBT, MBT, NFB, CT, PsyEd, and hypnotherapy), specifically adapted or developed to address the core symptoms of adults with a primary diagnosis of ADHD, in their comorbid internalizing symptoms (depression and anxiety symptoms, low self-esteem, impaired perceived QoL and ED), both after treatment and at follow-up. In addition, two secondary objectives were included: (a) the investigation of whether the effect of treatment on ADHD core symptoms could predict improvements on the comorbid internalizing symptomatology and (b) the examination of how different variables (outcome measure source, within-study risk of bias, therapy type and setting, control group type, medication status, participants’ age and sex, and follow-up length) moderate effect size (ES) estimates for each outcome.
Method
This review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Liberati et al., 2009; see Supplementary Table 1).
Participants, Interventions, Comparators, Outcomes, and Studies Included
Participants
Studies in which all participants were at least 18 years old, with a primary diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000), DSM-5 (American Psychiatric Association, 2013), or International Classification of Diseases (10th rev.; ICD-10; World Health Organization, 1992) criteria for ADHD in adults, diagnosed by a mental health professional on the basis of a full clinical interview and validated ADHD rating scales, were included. As long as these criteria were fulfilled, both community and diagnoses made by the research team were permitted. Because this review is focused on comorbid internalizing symptoms, studies that included participants with severe active addictions or bipolar, psychotic, or personality disorders were excluded.
Intervention
Studies with one experimental group or more receiving a nonpharmacological intervention specifically designed or modified for treating adult ADHD, either supported by pharmacotherapy or not, were included.
Comparisons
For between-group outcomes, studies with one group or more not receiving an ADHD-specific nonpharmacological treatment (control group) were included. The following comparison groups were considered: (a) an active control group, in which participants received support from a therapist, in a group or individual nondirective sessions where no specific strategy was discussed, or even nonspecific interventions for ADHD such as relaxation training or sham NFB; (b) a TAU group, in which all participants received ADHD medication, and even some kind of counseling or clinical management, provided that nonspecific strategy for ADHD was discussed; or (c) a waiting list group, in which participants were waiting without receiving a nonpharmacological intervention, even though some, but not all, participants might receive pharmacotherapy.
Outcomes
Studies including self-reported or clinician-reported measures of comorbid depression or anxiety symptoms, self-esteem, QoL or ED were included. These measures must be obtained with instruments with adequate psychometric properties.
Study design
Both uncontrolled single-group pretest-posttest studies and RCTs were included. Although it could raise issues of internal validity, the inclusion of uncontrolled single-group pretest–posttest studies in a meta-analysis is supported by some authors when few RCTs are available, or there are ethical or other reasons that hinder or prevent using control groups (Hunter & Schmidt, 2004; Petticrew & Roberts, 2005).
Systematic Review Protocol
In accomplishing this systematic review, no previous protocol was carried out.
Search Strategy
A systematic literature search was carried out in Scopus, PsycINFO and MEDLINE (via PubMed) without a date limit. The following terms were used in the title and abstract: adult*; ADHD OR attention deficit hyperactivity OR attention deficit disorder; psychosocial t* OR skills train* OR CBT OR cognitive behavio* OR DBT OR dialectical behavio* OR neurofeedback OR MBCT OR mindful*. In addition, reference lists of relevant articles found were screened. The last search was performed on October 20, 2018.
Study Selection and Data Extraction
First, duplicates were removed, and a screening search on the basis of title and abstract was performed by the first author. Then, the masked articles were selected independently by two researchers, with an excellent agreement (κ = 0.81), and solving inconsistencies by consensus.
Data were extracted independently and coded in a pilot-tested spreadsheet by two researchers, with an excellent agreement (κ = 0.88 for RCTs; κ = 0.98 for pretest–posttest studies). A consensus was reached in cases where there were disagreements. Coding covered all items of study characteristics described in the Cochrane Handbook (Higgins & Green, 2011). The codebook can be requested from the corresponding author.
Data Analysis
Comprehensive Meta Analysis (Version 3.3.070) and Review Manager (Version 5.3) software were used for data analysis. Raw data can be accessed in the following link: https://www.dropbox.com/sh/0la6u15y9jnq3c5/AAByTErq7aqsnGknXpgrEphsa?dl=0. Posttreatment and long-term reduction of comorbid anxiety and depression symptoms, problems with self-esteem and ED and improvement of QoL were considered the primary outcomes. The ES for within-subject (pretest to posttest and follow-up) single-group studies was defined as the average pretest-follow-up change, divided by the pretest standard deviation, and with a correction factor for small sample sizes (Morris, 2000). The ES index for between-group (nonpharmacological treatments vs. control groups) outcomes was computed as the difference between the average pretest–posttest and follow-up change of the experimental and control groups, divided by a pooled estimate of the pretest standard deviations of the two groups, also with a correction factor for small sample sizes (Morris, 2008). Sampling variances of the ESs were estimated following Morris’s proposal (Morris, 2000, 2008). In these calculations, the Pearson correlation coefficient between the pretest and posttest/follow-up scores must be known. As studies did not report the Pearson correlation coefficients, these were imputed following Rosenthal’s recommendation (Rosenthal, 1991) by using r = 0.7. ES values of 0.2, 0.5, and 0.8 were considered small, moderate, and large, respectively (Cohen, 1988).
ES estimates of the individual studies, weighted by their inverse variance, were synthesized for each outcome. A random-effect model was selected because of the expectation of a high heterogeneity between studies and it was assumed that the true effect size may vary from study to study (Borenstein, Hedges, Higgins, & Rothstein, 2010). A 95% confidence interval (CI) was computed. Interpreting the values of 25%, 50%, and 75% as reflecting low, moderate, and high heterogeneity, respectively; the I2 index was used for the assessment of the ES consistency (Higgins, Thompson, Deeks, & Altman, 2003). This index describes the percentage of total variation across studies that is due to heterogeneity, rather than chance.
The first author, supervised by the second, assessed the internal validity of each study using The Cochrane Collaboration’s tool for assessing risk of bias (Higgins et al., 2011). Discrepancies were decided by consensus. Blinding of the therapists could not be assessed, as the studies used nonpharmacological treatments. To ascertain the influence of this variable on ES estimates, sensitivity analyses were performed, but studies were not excluded for presenting a high risk of bias evaluation.
We conducted several analyses to assess the publication bias. First, the funnel plots were examined visually. Second, the trim-and-fill method was performed (Duval & Tweedie, 2000), which trims the asymmetric results on the right side and fills the plot with their imputed counterparts on the left, estimating a new corrected ES. Third, the Egger test was carried out to test the asymmetry of the funnel plots (Egger, Smith, Schneider, & Minder, 1997). This test evaluates bias predicting the standardized effect (ES divided by the standard error) with the precision of each ES (the inverse of the standard error). Finally, the fail-safe N (Rosenthal, 1979), which is the number of additional studies with a null effect needed to make the meta-analysis nonsignificant (raising the p value above .05), was also calculated.
The impact on ES estimates of some clinically and demographically relevant variables, such as therapy type, therapy setting, percentage of participants under medication, mean age of participants, and percentage of male participants, was assessed. These variables were selected because some of them were assessed in previous meta-analytic reviews and because of their clinical significance. In addition, because of the suspected heterogeneity in the methodological quality of the included studies, some relevant variables for this issue, such as the risk of bias assessment, outcome measure source, control group type, and follow-up length, were included in the moderator analyses as well. These analyses were performed with chi-square tests for categorical variables and with meta-regressions for continuous variables. To increase the statistical power of these analyses, all therapies were merged for each outcome, following the procedures of previous meta-analytic reviews in the field (Knouse et al., 2017). Due to the importance of an adequate comparison group, additional sensitivity analyses were made within each nonpharmacological intervention, isolating the effect of those studies that compared the treatment with an active control group, where positive results were found.
Results
Study Selection
From 1,054 records, 20 RCTs, three controlled pretest–posttest, and 12 uncontrolled single-group pretest–posttest studies were identified and included in the analyses (see Figure 1 and Tables 1 and 2). All studies included were published in peer review journals. A total of 587 studies were excluded after a screening on the basis of the title and abstract. Four controlled studies were excluded from between-group but included in within-subject meta-analyses, because they were not randomized (Bramham et al., 2009; Bueno et al., 2015; Wiggins et al., 1999), and because all groups received a specific therapy for ADHD (Cherkasova et al., 2016). Thus, finally, up to 18 comparisons were available for between-group outcomes, and up to 33 treatment groups were included in the within-subject meta-analyses. For the studies by Philipsen et al. (2015) and Schönenberg et al. (2017), each treatment group was compared with the equivalent control group, based on medication status and comparing NFB versus sham NFB, respectively. A total of 18 studies were excluded because they did not measure any of the outcomes considered in our review (Bachmann et al., 2018; Barth, Mayer, Strehl, Fallgatter, & Ehlis, 2017; Cowley, Holmström, Juurmaa, Kovarskis, & Krause, 2016; Hirvikoski, Waaler, Lindström, Bölte, & Jokinen, 2015; Janssen, de Vries, Hepark, & Speckens, 2017; Janssen et al., 2018; Kaiser, 1997; LaCount, Hartung, Shelton, Clapp, & Clapp, 2015; Schoenberg et al., 2014; Solanto, Marks, Mitchell, Wasserstein, & Kofman, 2008; Thompson & Thompson, 1998; Van der Oord et al., 2018; Virta, Hiltunen, Mattsson, & Kallio, 2015; Wang et al., 2016; Weiss et al., 2012; White & Shah, 2006; Zilverstand et al., 2017; Zwart & Kallemeyn, 2001); four because there were insufficient data in the article (Cole et al., 2016; Hirvikoski et al., 2011; Huang et al., 2019; Weiss & Hechtman, 2006); two for not including all participants who were at least 18 years old (Vidal-Estrada et al., 2015; Zylowska et al., 2008); two for including participants with severe substance abuse (Bihlar Muld, Jokinen, Bölte, & Hirvikoski, 2016) and personality disorders (Prada et al., 2015); and one because the treatment was self-applied (Moëll, Kollberg, Nasri, Lindefors, & Kaldo, 2015) or a formal diagnostic assessment for ADHD was not made (Wymbs & Molina, 2015).
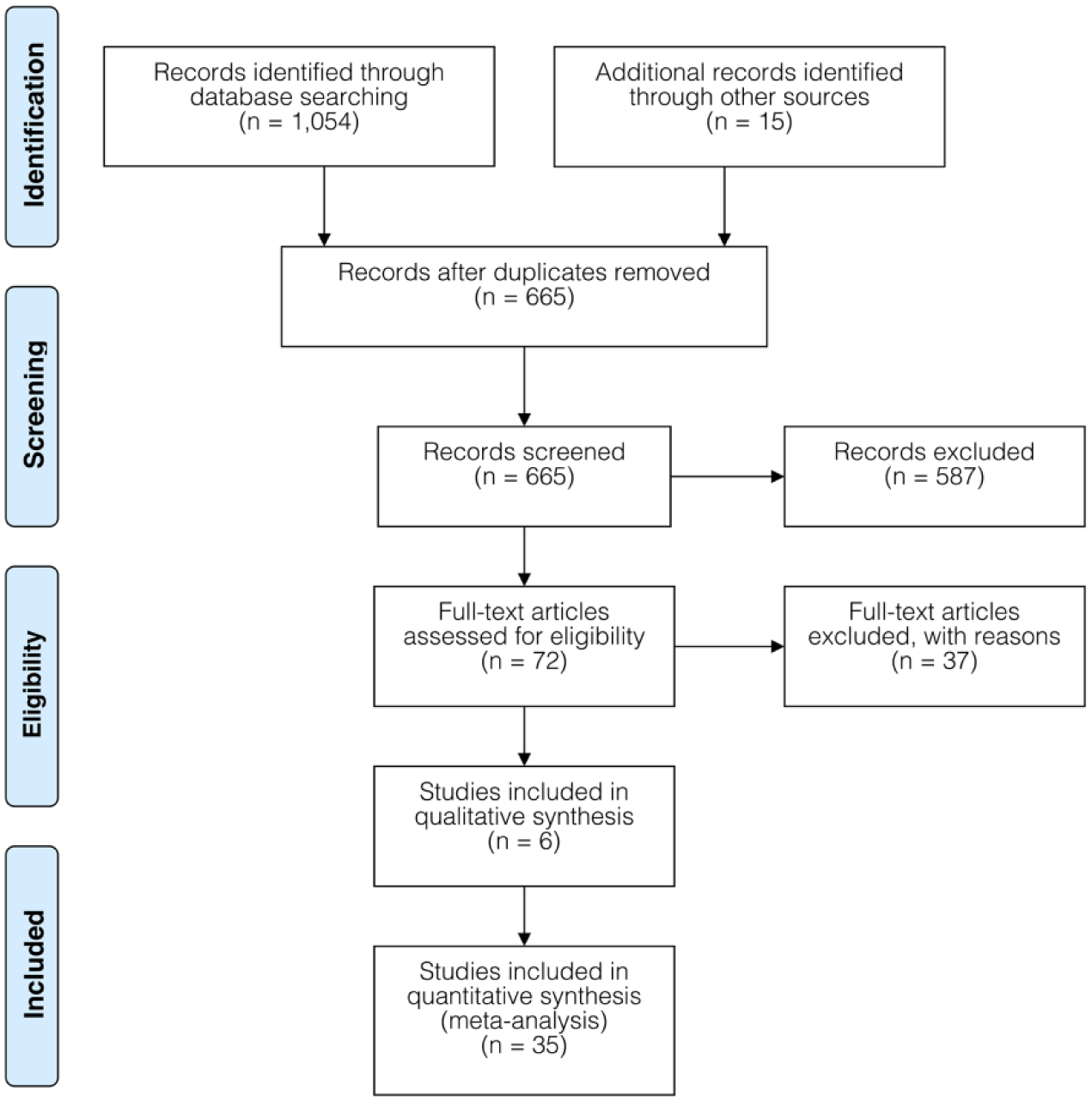
PRISMA 2009 flow diagram.
Summary of Characteristics of Included Randomized Controlled Trials.
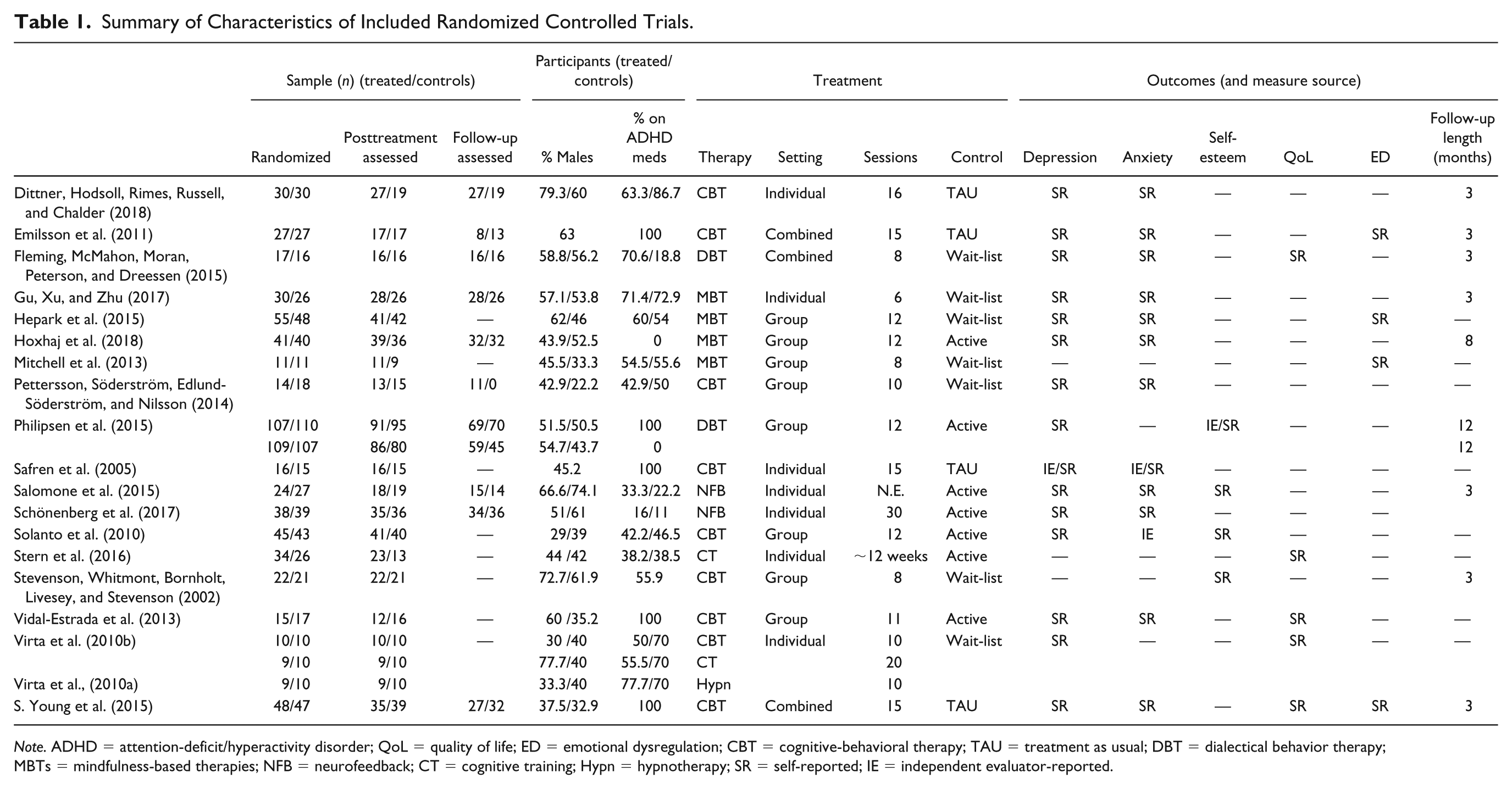
Note. ADHD = attention-deficit/hyperactivity disorder; QoL = quality of life; ED = emotional dysregulation; CBT = cognitive-behavioral therapy; TAU = treatment as usual; DBT = dialectical behavior therapy; MBTs = mindfulness-based therapies; NFB = neurofeedback; CT = cognitive training; Hypn = hypnotherapy; SR = self-reported; IE = independent evaluator-reported.
Summary of Characteristics of Included Pre–Post Studies.
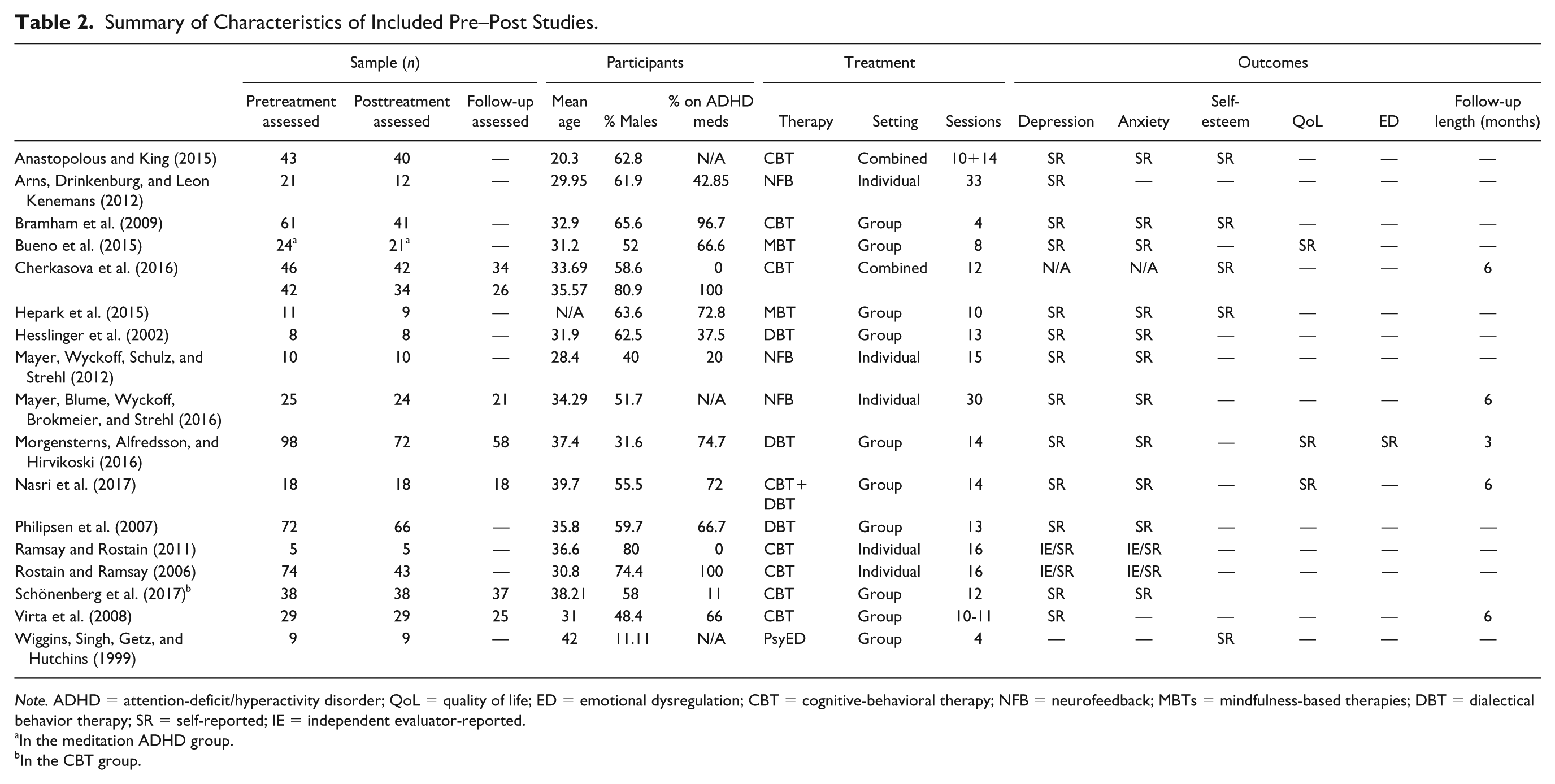
Note. ADHD = attention-deficit/hyperactivity disorder; QoL = quality of life; ED = emotional dysregulation; CBT = cognitive-behavioral therapy; NFB = neurofeedback; MBTs = mindfulness-based therapies; DBT = dialectical behavior therapy; SR = self-reported; IE = independent evaluator-reported.
In the meditation ADHD group.
In the CBT group.
Participants
Considering all the RCTs together, a total of 1,389 subjects were randomized, from which 1,163 were assessed at posttreatment and 629 at follow-up. Of a total of 634 subjects assessed initially in all the included uncontrolled pre–post studies, 521 were maintained at posttreatment and 219 at follow-up. On average, 51.85% of participants were male, age was 34.16 years, and 54.79% of participants were taking medication for ADHD during treatment.
Interventions
A total of 41.67% (n = 15) of the treatment groups underwent CBT, 16.67% (n = 6) DBT and MBT, 13.89% (n = 5) NFB, 5.56% (n = 2) CT, and 2.78% (n = 1) hypnotherapy or PsyEd. On average, the interventions comprised 12.34 sessions. Group and individual treatments were given in 48.48% and 36.36% of the studies, respectively, whereas both were combined in 15.15%.
Comparison
A waiting list group was used in 42.11% of studies, whereas 36.84% and 21.05% of them compared the intervention with an active control group and a TAU group, respectively.
Outcomes
Blinded and unblinded independent assessors were used in 3.12% and 10.93% of outcome measures, respectively, whereas the remaining used only self-reported measures.
Results for Each Therapy
CBT
CBT for ADHD studies obtained a small-to-moderate ES on depression symptoms after treatment, both compared with control groups (standardized mean difference [SMD] = 0.27; 95% CI = [0.02, 0.52]; I2 = 52%) and moderate-to-large on within-subject outcome (SMD = 0.54; 95% CI = [0.35, 0.72]; I2 = 72%; see Supplementary Table 2, Figure 2, and Supplementary Figure 1). This effect increased to moderate-to-large at follow-up assessment (SMD = 0.52; 95% CI = [0.24, 0.80]; I2 = 0%, for between-group outcome; SMD = 0.72; 95% CI = [0.48, 0.96]; I2 = 42%, for within-subject outcome). In the same way, effect on anxiety symptoms was small-to-moderate after treatment for both between-group (SMD = 0.31; 95% CI = [0.01, 0.62]); I2 = 64%; see Supplementary Figure 2) and within-subject outcomes (SMD = 0.49; 95% CI = [0.25, 0.72]; I2 = 82%), increasing to moderate-to-large at follow-up (SMD = 0.73; 95% CI = [0.45, 1.02]; I2 = 0%, for between-group outcome; SMD = 0.74; 95% CI = [0.28, 1.21]; I2 = 84%, for within-subject outcome). Sensitivity analyses showed that between-group ES became null when only active controlled studies were considered, both for posttreatment depression (SMD = −0.15; 95% CI = [−0.47, 0.16]; I2 = 12%) and anxiety (SMD = 0.05; 95% CI = [−0.61, 0.72]).
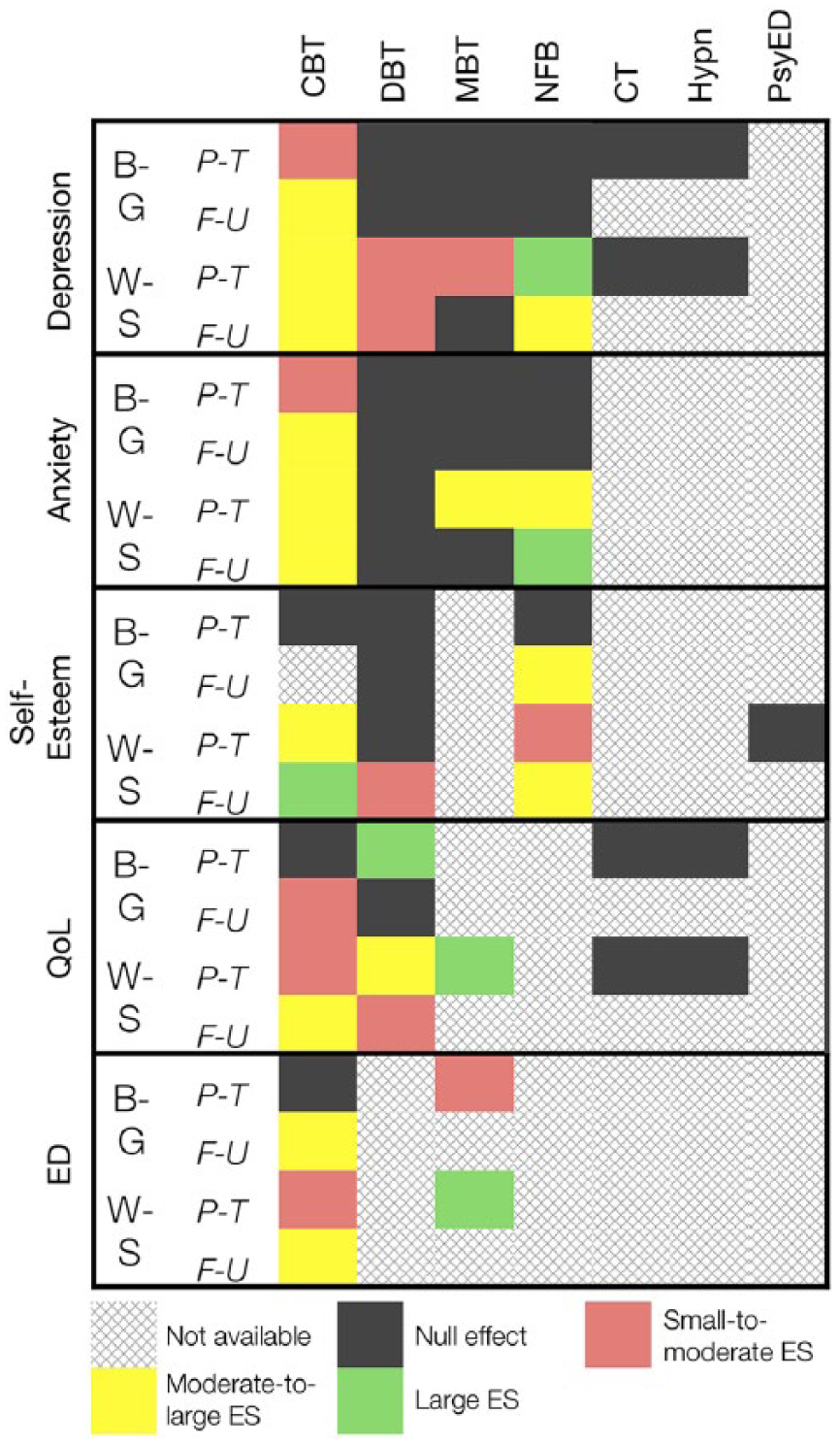
Summary of the results on the main outcomes for each therapy.
No significant effect was found on between-group self-esteem outcomes, but within-subject ES increased from small-to-moderate at posttreatment (SMD = 0.62; 95% CI = [0.31, 0.92]); I2 = 80%) to large at follow-up (SMD = 1.404; 95% CI = [0.45, 1.64]; I2 = 74%; see Supplementary Figure 3). Posttreatment within-subject ES on QoL was small-to-moderate (SMD = 0.28; 95% CI = [0.09, 0.48]; I2 = 80%), which increased to moderate-to-large at follow-up (SMD = 0.57; 95% CI = [0.22, 0.92]), whereas a small-to-moderate effect was found when compared with TAU controls at follow-up (SMD = 0.39; 95% CI = [0.01, 0.78]; see Supplementary Figure 4). Likewise, in comparison with TAU control groups, treatment effect on ED increased from null up to moderate-to-large at follow-up (SMD = 0.64; 95% CI = [0.30, 0.98]; I2 = 0%; see Supplementary Figure 5), whereas after treatment within-subject effect rose from small-to-moderate (SMD = 0.38; 95% CI = [0.16, 0.60]; I2 = 0%) to moderate-to-large (SMD = 0.73; 95% CI = [0.42, 1.03]; I2 = 80%) at follow-up.
Regarding publication bias, trim-and-fill method adjusted the effect on between-group posttreatment anxiety and depression, with a CI including zero after trimming one and two studies, respectively (adjusted SMD = 0.19; 95% CI = [−0.13, 0.53] for anxiety; adjusted SMD = 0.13; 95% CI = [−0.10, 0.37] for depression). On the contrary, Egger test was nonsignificant for these outcomes (bias = 1.83; 95% CI = [−3.35, 7.03]; p = .42 for depression; bias = −1.70; 95% CI = [−10.65, 7.18]; p = .63 for anxiety). No publication bias indicators were identified in the remaining outcomes.
DBT
This intervention showed a small-to-moderate within-subject effect on depression symptoms after treatment (SMD = 0.36; 95% CI = [0.24, 0.48]; I2 = 33%), which was sustained at follow-up (SMD = 0.33; 95% CI = [0.13, 0.53]; I2 = 63%), whereas no significant effect was found compared with control groups (see Supplementary Table 2, Figure 2, and Supplementary Figure 1). All anxiety symptom outcomes were nonsignificant (see Supplementary Figure 2). Effect on self-esteem was only significant for within-subject change at follow-up (SMD = 0.48; 95% CI = [0.34, 0.63]; I2 = 2%). Compared with an active control group, a large ES on QoL was obtained after treatment (SMD = 0.84; 95% CI = [0.25, 1.43]; see Supplementary Figure 4) but was not sustained at follow-up. The moderate-to-large within-subject effect on QoL (SMD = 0.61; 95% CI = [0.06, 1.16]; I2 = 73%) decreased to small-to-moderate at follow-up (SMD = 0.40; 95% CI = [0.17, 0.64]; I2 = 0%).
No publication bias signs were found for this intervention.
MBT
MBTs for ADHD obtained a small-to-moderate within-subject effect after treatment on depression symptoms (SMD = 0.33; 95% CI = [0.17, 0.50], I2 = 31%), but it became null at follow-up (see Supplementary Table 2, and Figure 2). No significant effect was observed on comorbid depression and anxiety symptoms when compared with control groups, nor in within-subject anxiety (see Supplementary Figures 1 and 2). A large ES was obtained on within-subject QoL outcome after treatment (SMD = 1.44; 95% CI = [0.85, 2.03]). The posttreatment effect on ED was small-to-moderate when compared with waiting list controls (SMD = 0.46; 95% CI = [0.15, 0.76]; I2 = 0%) and also in within-subject outcome (SMD = 0.44; 95% CI = [0.28, 0.61]; I2 = 22%; see Supplementary Figure 5).
No publication bias indicators were identified for this therapy.
NFB
A large within-subject ES on comorbid depression symptoms was obtained at posttreatment (SMD = 0.85; 95% CI = [0.62, 1.08]; I2 = 10%), which decreased to moderate-to-large at follow-up (SMD = 0.65; 95% CI = [0.43, 0.86]; I2 = 0%; see Supplementary Table 2 and Figure 2). The within-subject effect on anxiety rose from moderate-to-large after treatment (SMD = 0.72; 95% CI = [0.23, 1.21]; I2 = 80%) to large at follow-up (SMD = 0.85; 95% CI = [0.59, 1.10]; I2 = 10%). The effect on anxiety and depression symptoms was nonsignificant when comparing this intervention with control groups (see Supplementary Figures 1 and 2). When compared with an active control group, the between-group effect on self-esteem increased from null after treatment to moderate-to-large at follow-up (SMD = 0.70; 95% CI = [0.09, 1.31]), whereas the within-subject change increased from small-to-moderate at posttreatment (SMD = 0.47; 95% CI = [0.06, 0.88]) to moderate-to-large at follow-up (SMD = 0.68; 95% CI = [0.19, 1.17]; see Supplementary Figure 3).
No publication bias indicators were found for this treatment.
CT
CT interventions for ADHD obtained a nonsignificant ES (with a CI including zero) on posttreatment between-group and within-subject depression and QoL outcomes (see Supplementary Table 2, Figure 2, and Supplementary Figures 1 and 4).
Hypnotherapy
A nonsignificant effect was found on depression and QoL after treatment, both for between-group and within-subject outcomes (see Supplementary Table 2, Figure 2, and Supplementary Figures 1 and 4).
PsyEd
A null ES was obtained on within-subject self-esteem outcome after treatment (see Supplementary Table 2, and Figure 2).
Risk of Bias Assessment
All outcomes were rated with a high risk of bias (see Figure 3 and Supplementary Figures 6 to 9). Only one study in each of the following outcomes was rated with an unclear risk of bias: anxiety and depression symptoms (Safren et al., 2005), ED (Mitchell et al., 2013), and self-esteem (Philipsen et al., 2015).

Risk of bias assessment summary for depression symptoms outcomes.
Moderator Analyses
ES on ADHD core symptoms
Results of the meta-regressions that could be computed for this covariate are shown in Table 3.
Meta-Regressions for ADHD Symptoms ES Covariate.
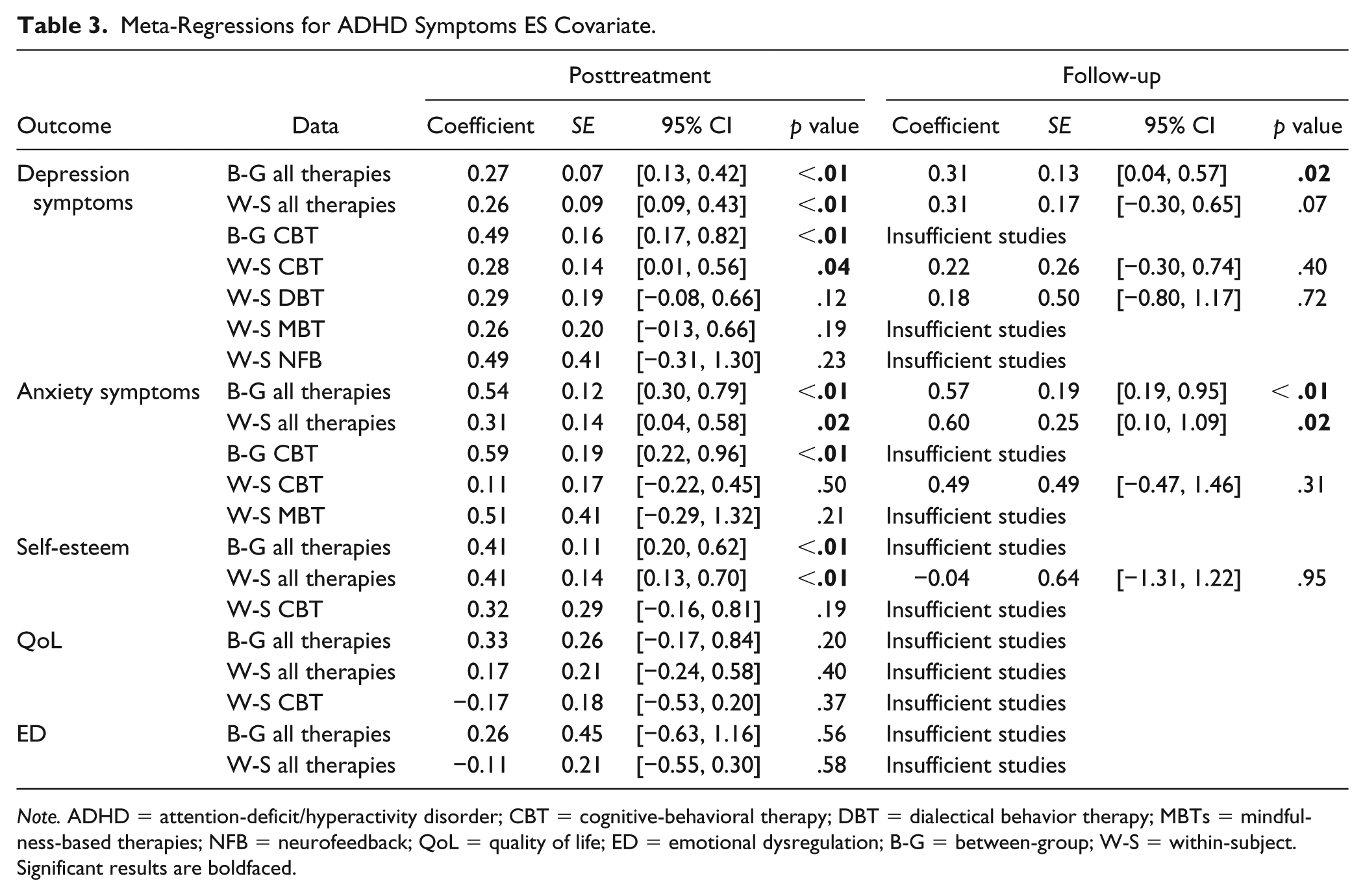
Note. ADHD = attention-deficit/hyperactivity disorder; CBT = cognitive-behavioral therapy; DBT = dialectical behavior therapy; MBTs = mindfulness-based therapies; NFB = neurofeedback; QoL = quality of life; ED = emotional dysregulation; B-G = between-group; W-S = within-subject. Significant results are boldfaced.
When all therapies were merged, higher ES on core symptoms significantly predicted positively the efficacy on depression (coefficient = 0.27, 95% CI = [0.13, 0.42]; p < .01 for between-group; coefficient = 0.31, 95% CI = [0.04, 0.57]; p < .01 for within-subject), anxiety (coefficient = 0.49, 95% CI = [0.17, 0.82]; p < .01 for between-group; coefficient = 0.31, 95% CI = [0.04, 0.58]; p = .02 for within-subject), and self-esteem (coefficient = 0.41, 95% CI = [0.20, 0.62]; p < .01 for between-group; coefficient = 0.41, 95% CI = [0.13, 0.70]; p < .01 for within-subject) at posttreatment. At follow-up, this covariate also positively predicted efficacy on between-group depression (coefficient = 0.31, 95% CI = [0.04, 0.57]; p < .01) and anxiety (coefficient = 0.57, 95% CI = [0.19, 0.95]; p < .01), and within-subject anxiety (coefficient = 0.60, 95% CI = [0.10, 1.09]; p = .02). Regressions were nonsignificant for QoL and ED outcomes.
For CBT, efficacy on between-group depression (coefficient = 0.49, 95% CI = [0.17, 0.82]; p < .01) and anxiety (coefficient = 0.59, 95% CI = [0.22, 0.96]; p < .01) was predicted positively by the ES on ADHD symptoms. For follow-up and within-subject outcomes, regressions were nonsignificant.
Effect on ADHD symptomatology was not a predictor for within-subject efficacy of MBT, DBT, and NFB on depression, nor for MBT on anxiety symptoms.
Risk of bias
ES estimates were significantly lower for studies rated as having an unclear risk of bias on between-group self-esteem, χ2(1) = 4.47, p = .03, and depression, χ2(1) = 4.77, p = .03, after treatment, and on self-esteem at follow-up, χ2(1) = 5.63, p = .02. In the same way, effect of unclear risk of bias-assessed studies was significantly lower for within-subject posttreatment ED, χ2(1) = 4.94, p = .03, and self-esteem at follow-up, χ2(1) = 4.73, p = .03, outcomes. Nonsignificant differences were found in the remaining outcomes.
Therapy
CBT was significantly more effective on between-group depression, χ2(3) = 11.93, p < .01, and anxiety, χ2(3) = 17.31, p < .01, at follow-up (see Supplementary Table 2). Within-subject CBT and NFB effect on depression was significantly higher at the end of treatment, χ2(5) = 18.07, p < .01. DBT was significantly less effective on between-group self-esteem at posttreatment, χ2(2) = 6.11, p = .05 and at follow-up, χ2(1) = 5.63, p = .02; and within-subject anxiety, both at posttreatment, χ2(3) = 12.98, p < .01 and at follow-up, χ2(3) = 20.34, p < .01. MBTs were significantly more effective on within-subject posttreatment QoL, χ2(4) = 14.73, p = .01. PsyEd was significantly less effective on within-subject posttreatment self-esteem, χ2(3) = 12.73, p < .01. Nonsignificant differences were found in the remaining outcomes.
Treatment setting
Individual therapy was significantly more effective on between-group depression after treatment, χ2(2) = 8.26, p = .02, self-esteem at follow-up, χ2(1) = 5.63, p = .02, and also on within-subject depression and anxiety, both at posttreatment, χ2(2) = 24.60, p < .01 for depression; χ2(2) = 12.21, p < .01 for anxiety, and at follow-up, χ2(2) = 15.07, p < .01 for depression; χ2(2) = 53.61, p < .01 for anxiety. Nonsignificant differences were found in the remaining outcomes.
Measure source
Independent-assessed effect on posttreatment was significantly higher on within-subject ED, χ2(1) = 4.66, p = .03. Nonsignificant differences were found in the remaining outcomes.
Control group
Treatment was significantly less effective on depression symptoms when compared with active control groups, χ2(2) = 16.90, p < .01, and self-esteem outcomes, χ2(1) = 8.64, p < .01, at posttreatment, and on anxiety at follow-up, χ2(2) = 20.26, p < .01. In addition, treatment was significantly more effective on depression when compared with TAU group at follow-up, χ2(2) = 14.59, p < .01. Nonsignificant differences were found in the remaining outcomes.
Percentage of participants on medication
This variable positively predicted the efficacy of the interventions on between-group depression (coefficient = 0.01, 95% CI = [0.00, 0.01]; SE = 0.00; p = .02) and anxiety (coefficient = 0.01, 95% CI = [0.00, 0.01]; SE = 0.00; p = .01) at follow-up, and on the within-subject self-esteem at posttreatment (coefficient = 0.01, 95% CI = [0.00, 0.01]; SE = 0.00; p = .01; see Table 3). Meta-regressions for the remaining outcomes were nonsignificant for this covariate.
Number of sessions
This moderator positively predicted the efficacy at posttreatment on within-subject depression (coefficient = 0.03, 95% CI = [0.00, 0.04]; SE = 0.00; p < .01), whereas negatively predicted efficacy on the within-subject QoL after treatment (coefficient = −0.06, 95% CI = [−0.11, 0.01]; SE = 0.02; p < .01; see Table 3). Regressions for the rest of the outcomes were nonsignificant.
Mean age
Mean age of treatment groups negatively predicted the effect of interventions on posttreatment between-group (coefficient = −0.04, 95% CI = [−0.08, −0.00]; SE = 0.02; p = .04), and within-subject (coefficient = −0.03, 95% CI = [−0.07, −0.01]; SE = 0.02; p < .01) QoL, on posttreatment between-group anxiety (coefficient = −0.03, 95% CI = [−0.06, 0.00]; SE = 0.01; p = .02) and on within-subject self-esteem at follow-up (coefficient = −0.39, 95% CI = [−0.76, 0.07]; SE = 0.01; p = .01; see Table 3). Regressions were nonsignificant for the other outcomes.
Percentage of male participants
This variable positively predicted the ES on posttreatment within-subject anxiety (coefficient = 0.01, 95% CI = [0.00, 0.01]; SE = 0.00; p = .04) and self-esteem outcomes (coefficient = 0.01, 95% CI = [0.00, 0.02]; SE = 0.01; p = .04 at posttreatment; coefficient = 0.03, 95% CI = [0.01, 0.05]; SE = 0.01; p < .01 at follow-up; see Table 3). Results were nonsignificant for the remaining outcomes.
Follow-up length
This covariate negatively predicted the effect on between-group anxiety at follow-up (coefficient = −0.17, 95% CI = [−0.30, −0.05]; SE = 0.06; p = .01; see Table 3). Meta-regressions were nonsignificant for the remaining depression and anxiety outcomes and cannot be computed for the rest because of a problem with collinearity or because there were insufficient studies.
Discussion
Several studies have found mixed results for the efficacy of nonpharmacological treatments on comorbid internalizing symptoms in adults with ADHD. In addition, previous systematic reviews observed some support for the efficacy of CBT in improving some comorbid internalizing conditions after treatment. This meta-analytic review aimed to determine the efficacy of different psychotherapies for ADHD symptoms in comorbid internalizing symptoms in adults, both at posttreatment and up to 12 months after the end of the intervention, and likewise to evaluate the influence of different clinically and methodologically relevant moderator variables.
Findings on Nonpharmacological Intervention Efficacy on Comorbid Internalizing Symptoms and the Core Symptoms Improvement as Moderator
Our results indicated that CBT for ADHD improved comorbid depression and anxiety, both when compared with waiting list and TAU control groups and also considering within-subject change. These findings are consistent with previous adult ADHD meta-analyses (Jensen et al., 2016; Lopez et al., 2018), and also with those assessing the efficacy of CBT for internalizing disorders in adults without ADHD, with a similar effect size (Carpenter et al., 2018; Lepping et al., 2017). Effect size on comorbid internalizing symptoms was also similar to those reported on posttreatment core ADHD symptoms (Knouse et al., 2017), but lower than those obtained in the long term (López-Pinar et al., 2018). In addition, CBT for ADHD was significantly more effective than the other therapies in treating comorbid depression and anxiety, particularly in the long term. A possible explanation for these findings might be that CBT programs for adult ADHD include therapy ingredients that have been shown to be effective in the treatment of depression and anxiety disorders, such as cognitive therapy (Cuijpers, Cristea, Karyotaki, Reijnders, & Huibers, 2016) or problem-solving skills (Cuijpers, de Wit, Kleiboer, Karyotaki, & Ebert, 2018), so the treatment could be specific not only for core symptoms but also for comorbidity. On the contrary, results of the meta-regressions showed that ES on core symptoms significantly predicted the between-group efficacy on depression and anxiety. This might suggest that these symptoms were secondary to ADHD, and that CBT improvement of the inattention and hyperactivity/impulsivity symptoms led to the decrease in the associated symptomatology. CBT for ADHD also improved the other comorbid conditions, such as self-esteem (only when within-subject data were considered), and ED. This might be caused by the change to more functional beliefs about themselves, which is an essential therapeutic mechanism in CBT. This cognitive change could in turn improve the expectation of being able to deal with emotional situations (Hirsch et al., 2018), effectively enhancing emotional self-regulation (Bigman, Mauss, Gross, & Tamir, 2016). CBT for adult ADHD also improved QoL in comparison with TAU groups, especially in the long term. Contrary to expected, the reduction in ADHD symptoms did not lead to an improvement of QoL. Thus, this finding might indicate that CBT for ADHD was also specific with this variable. An interesting finding is that the effectiveness of CBT increased at follow-up in all outcomes, and the observed heterogeneity decreased. As suggested by CBT models of adult ADHD, the learning of adaptive coping strategies (both behavioral and cognitive) can reduce the functional impairment caused by neurobiological deficits (Safren et al., 2004). Because CBT efficacy on ADHD core symptoms has proved to be stable for at least a year (López-Pinar et al., 2018), the long-term integration of adaptive coping skills and the subsequent reduction of chronic functional impairment could also result in an improvement in comorbid internalizing conditions. This might have a greater impact as time goes by, once the psychological framework created by the therapy is well established.
Despite sharing several key therapeutic components with CBT (e.g., planning skills, cognitive strategies, among others), results showed that when compared with active control groups, DBT for ADHD only improved the posttreatment QoL, which was not sustained at follow-up. Regarding within-subject change, a small effect was found on self-esteem (only at follow-up) and comorbid depression, whereas the moderate-to-large posttreatment effect on QoL decreased to small at follow-up. These results are in line with those found in individuals with depression disorders without ADHD (Valentine, Bankoff, Poulin, Reidler, & Pantalone, 2015). Unexpectedly, no effect was observed on comorbid anxiety symptoms, despite the fact DBT skills predicted symptom improvement in the clinical population without ADHD (Webb, Beard, Kertz, Hsu, & Björgvinsson, 2016).
Some of the proposed MBT therapeutic working pathways are emotion regulation and somatic awareness (Hölzel et al., 2011). This seems a potential explanation for the improvement observed in posttreatment ED in our study, when these interventions were compared with waiting list control groups. Results also showed a within-subject improvement in this outcome, in addition to anxiety and depression, but gains were not sustained at follow-up. These improvements were not predicted by the treatment effect on ADHD core symptoms. However, no effect was found on depression and anxiety when MBT for ADHD were compared with control groups. Effect of MBT on internalizing comorbidity was inferior to that reported for ADHD core symptoms (Cairncross & Miller, 2016). These poor results were an unexpected finding, as mindfulness-based cognitive therapy (the intervention used by most studies in MBT subgroup) was initially developed for treating recurrent depression (Segal, Williams, & Teasdale, 2002), and MBTs have shown a small-to-moderate effect on anxiety and depression symptoms on the clinical and nonclinical population (Blanck et al., 2018). In contrast, these interventions were the most effective in improving posttreatment QoL when within-subject data were considered, although this finding was based only on one small uncontrolled trial (Bueno et al., 2015).
No effect was found on ADHD comorbid anxiety and depression when NFB was compared with control groups. These results are consistent with those obtained in individuals with a primary diagnosis of depression and anxiety disorders without ADHD (Begemann, Florisse, van Lutterveld, Kooyman, & Sommer, 2016) and with studies assessing the efficacy on ADHD symptoms (Schönenberg et al., 2017). On the contrary, regarding within-subject change, there were improvements in depression, anxiety and low self-esteem, which increased in the long term. Two potential NFB mechanisms were proposed by Mayer et al. (2016): First, intervention improves not only core ADHD symptoms but also comorbid symptoms, and second, reduction of core ADHD symptoms leads to improvements in comorbidity. The direction of the relationship is unknown and needs further investigation, although there are some studies preliminarily suggesting that NFB training could be a promising intervention for depression (Choi et al., 2010) and anxiety disorders (Mennella, Patron, & Palomba, 2017) in the clinical population, but presenting serious methodologic limitations (Begemann et al., 2016). Moreover, meta-regression results also supported the first hypothesis.
Results showed that CT, PsyEd, and hypnotherapy were not effective in treating comorbid internalizing symptoms in adults with ADHD. These results differ from those obtained in the clinical population without ADHD, in which some evidence of improvement of internalizing symptoms has been found after CT (Motter et al., 2016), PsyEd (Donker, Griffiths, Cuijpers, & Christensen, 2009), and hypnotherapy (Golden, 2012) interventions. However, more research is needed to evaluate the usefulness of these interventions, because these findings were based on a small number of trials presenting some methodological shortcomings. Thus, findings concerning these therapies need to be interpreted with caution with regard to adults with ADHD.
Results of meta-regressions (when all interventions were merged) supported the hypothesis that comorbid depression, anxiety, and self-esteem improvements are a secondary gain from the reduction of ADHD symptomatology. Nonetheless, it seems that the treatment is also specific for QoL and ED. These results could have important clinical implications regarding the sequencing of treatments. We know that not treating the symptoms of ADHD is a risk factor for the development of internalizing comorbid problems (Biederman et al., 2011), and our results support that an effective treatment of ADHD in adults could prevent the development of some of these problems and, therefore, alleviate the impairment. Similarly, because the presence of ADHD symptoms is often overlooked in the treatment of anxiety and depression patients, these symptoms should also be considered to improve the evolution of this population (Barkley & Brown, 2008).
Findings of the Moderator Analyses
Given the importance of having an appropriate comparison group, a possible limitation of the findings is that when CBT studies using an active control group were isolated, ES became nonsignificant for depression and anxiety posttreatment outcomes. This might be an indicator of the nonspecificity of CBT for improving these comorbid symptoms, but it has to be interpreted with caution, because it is based on only two studies with different placebo groups (Solanto et al., 2010; Vidal-Estrada et al., 2013). Another possible explanation is, as some authors have suggested, that placebo psychotherapy groups are not fully “inert” (Wampold et al., 2016). When all therapies were merged, therapy efficacy on depression and self-esteem after treatment was significantly lower in comparison with active control groups, which is in line with previous adult ADHD meta-analyses (Knouse et al., 2017; Lopez et al., 2018; López-Pinar et al., 2018), which could mean that treatments were not specifically effective for those outcomes. On the contrary, results supported the specificity of the treatment in improving these outcomes in the long term, and, in addition, in the rest of posttreatment outcomes.
Another clinically relevant finding was that treatment given in an individual setting was more effective on self-esteem, depression, and anxiety comorbid symptoms. This is consistent with the literature about treatment of anxiety and depression disorders (Carpenter et al., 2018). A possible explanation for this is that the ability to fit the specific needs of each case of individual therapy might be more specifically effective for comorbid internalizing symptoms than the support of a group. In addition, the alliance, which is positively related to the outcome of a psychological treatment (Horvath, Del Re, Flückiger, & Symonds, 2011), is significantly stronger in individual relative to group CBT (Mörtberg, 2014).
One important result supporting the robustness of the findings was that no significant difference was found between self-reported and independent-assessed measures in the vast majority of outcomes. This finding is consistent with those reported by previous meta-analytic reviews (Jensen et al., 2016). However, this result must be interpreted with caution because of the small number of studies which included independent-assessed measures.
Another significant result supporting the stability of the gains on depression comorbid symptoms was that follow-up length did not predict the effect on these outcomes. Notwithstanding, the results suggest that the effect on anxiety faded as time passes, differing from those obtained by CBT for anxiety disorders, which reported improvements that were maintained up to 1 year at follow-up (DiMauro, Domingues, Fernandez, & Tolin, 2013).
A higher proportion of males and younger participants predicted better results in some of anxiety, self-esteem, and QoL outcomes, as was suggested by previous literature (Edvinsson et al., 2013; Müller et al., 2017; Piñeiro-Dieguez et al., 2016; Solberg et al., 2018). These findings might be explained because anxiety disorders (Bandelow & Michaelis, 2015) and low self-esteem (Bleidorn et al., 2016) are more prevalent in women and because of the increase with age of the comorbid internalizing problems severity in adults with ADHD (Bramham et al., 2012). However, these results are not consistent with other studies that have found that older people tend to be more satisfied with their lives (Mercier, Péladeau, & Tempier, 1998) and have a higher self-esteem (Bleidorn et al., 2016).
As expected, a higher percentage of participants on ADHD medication predicted better results in depression, anxiety, and self-esteem, which supports the effectiveness of pharmacotherapy on the comorbid internalizing symptoms and is consistent with previous findings in adults with ADHD (Lopez et al., 2018). In addition, shorter treatments predicted worst results in QoL and longer interventions predicted better results in depression after treatment, but not at follow-up. This is consistent with the good-enough-level model about treatment duration. This model states that progressively less gains become acceptable as treatment takes longer, and then longer duration predicts poorer outcomes (Barkham et al., 2006).
Finally, another important finding was that publication bias indicators were found only in posttreatment CBT anxiety and depression outcomes, disappearing at follow-up. The rest of outcomes for this and the other interventions were free from publication bias, which supports the validity of the results and is consistent with previous meta-analyses in the field (Lopez et al., 2018).
Limitations and Future Research
There are some limitations to the study that should be considered when interpreting the results. First, a key limitation of this review is the small number of studies evaluating some interventions (e.g., PsyEd, CT, and hypnotherapy), so the generalizability of the results concerning these psychotherapies is subject to certain limitations and more research about them is needed to ascertain their efficacy on comorbid internalizing symptoms. Second, differences in the designs of the studies and sample size might be responsible for differential efficacy and, therefore, limit the direct comparison between the included interventions. Third, the high risk of bias on most outcomes, mainly due to the use of self-reported and unblinded measures alone, might threaten the validity of results. Fourth, the small number of studies in some subgroups could limit the statistical power of their moderator analyses. Fifth, the merger of all therapy modalities to carry out the moderator analysis may limit the findings regarding how these variables could influence the effect for each of the interventions. Sixth, the small number of studies comparing the treatment with active control groups might limit findings regarding the specificity of the psychotherapies assessed. Seventh, the inclusion of uncontrolled studies could raise issues of internal validity, as this hinders the control of other variables that could influence the observed effect. Finally, the high heterogeneity observed in some of the posttreatment outcomes might limit the generalization of the findings.
To improve the validity of the results, future research should address the lack of independent and blinded assessment of outcome measures, the use of larger samples and comparison groups (preferably an active control), the inclusion of a follow-up assessment, and the assessment of the attrition, including intent-to-treat analyses.
Moreover, as DBT seems a promising intervention for ED in the clinical population (Neacsiu, Eberle, Kramer, Wiesmann, & Linehan, 2014), it could be relevant to study its effect on this variable in adults with ADHD. In addition, further research should be undertaken to investigate the potential benefits of adding well-established therapy components such as behavioral activation (Ekers et al., 2014) to the treatment of comorbid depression in adults with ADHD.
Conclusion
The results of this systematic review offer further empirical support for the efficacy of CBT in treating comorbid internalizing symptoms in adults with ADHD. CBT achieved better improvements in comorbid anxiety and depression symptoms, and in QoL and ED, particularly in the long term, but only compared with waiting list and TAU groups. Improvements in depression and anxiety symptoms were predicted by the reduction of ADHD core symptoms. In addition, there is some preliminary evidence about the utility of improving QoL, ED, and self-esteem of DBT, MBT, and NFB, respectively. Better results were achieved with the therapy given individually, combined with pharmacotherapy, and with a higher proportion of young and male participants. However, it is necessary to interpret these results carefully, because of the small number of studies evaluating some interventions and the high risk of bias determined for many of the outcomes. Despite these limitations, the evidence from this review supports the utility and stability of nonpharmacological interventions, particularly CBT, in treating comorbid internalizing symptoms in a population that tends to develop frequent problems concomitant with the disorder itself. Thus, the addition of these therapies is needed for a comprehensive treatment of adult ADHD.
Supplemental Material
S1_Fig_ForestP_DEP_post_BG – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S1_Fig_ForestP_DEP_post_BG for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S1_Table – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S1_Table for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S2_Fig_ForestP_ANX_post_BG – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S2_Fig_ForestP_ANX_post_BG for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S2_Table – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S2_Table for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S3_Fig_ForestP_SE_post_BG – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S3_Fig_ForestP_SE_post_BG for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S4_Fig_ForestP_QoL_post_BG – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S4_Fig_ForestP_QoL_post_BG for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S5_Fig_ForestP_ED_post_FW – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S5_Fig_ForestP_ED_post_FW for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S6_Fig – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S6_Fig for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S7_Fig – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S7_Fig for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S8_Fig – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S8_Fig for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Supplemental Material
S9_Fig – Supplemental material for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review
Supplemental material, S9_Fig for Efficacy of Nonpharmacological Treatments on Comorbid Internalizing Symptoms of Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review by Carlos López-Pinar, Sonia Martínez-Sanchís, Enrique Carbonell-Vayá, Julio Sánchez-Meca and Javier Fenollar-Cortés in Journal of Attention Disorders
Footnotes
Acknowledgements
The authors would like to acknowledge Virginia Soldino Garmendia for reviewing the manuscript for accuracy, Rosa García Martínez for masking the articles to carry out the independent blinded selection, and Ana Crespo Martínez for making an independent coding of the studies included.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.