
Abstract
Keywords
Recent theoretical (Bozhilova et al., 2018) and empirical (Lanier et al., 2021) work has drawn attention to the possible relation between ADHD and mind-wandering, defined by the unintentional shifting of thought from the external environment (Fredrick et al., 2020). Due to the nature of metacognitive deficits in ADHD, it has been hypothesized that mind-wandering may underlie ADHD symptoms and associated impairments (Bozhilova et al., 2018). Indeed, several studies in clinical and nonclinical adult samples have found ADHD symptoms to be associated with greater self-reported mind-wandering (Biederman et al., 2019; Lanier et al., 2021) and more frequent task-unrelated thought during sustained attention tasks (Jonkman et al., 2017). In addition, greater self-reported mind-wandering has been independently associated with increased impairment and reduced well-being while controlling for ADHD symptoms (Mowlem et al., 2019). In sum, a growing body of research supports a link between ADHD symptomatology and mind-wandering in adult samples.
Despite these findings, a recent systematic review (Lanier et al., 2021) noted that there is a shortage of studies with non-young adult samples, and only one study to our knowledge has tested ADHD and mind-wandering in adolescence. In a sample of adolescents with ADHD, adolescent-reported anxiety and ADHD inattentive (IN) symptoms were uniquely associated with greater self-reported mind-wandering (Figueiredo et al., 2020). Additional research is needed to replicate and extend these findings, particularly by examining co-occurring symptoms that may in part account for mind-wandering among individuals with ADHD.
Sluggish cognitive tempo (SCT) includes behaviors such as excessive daydreaming, inconsistent alertness, lethargy, and staring, and there is strong empirical support that SCT is distinct from ADHD-IN in child, adolescent, and adult populations (Becker et al., 2016). However, ADHD and SCT frequently co-occur, with approximately 25% to 40% of youth with ADHD experiencing elevated SCT symptoms (Barkley, 2013; Marshall et al., 2014; Servera et al., 2018). It has thus been suggested that co-occurring SCT symptoms may represent an important collection of behaviors that predict a differential pattern of functioning and impairment among youth with ADHD. For instance, research has found that adolescent-reported SCT, but not ADHD-IN symptoms, is uniquely related to greater self-reported depression, anxiety, and suicidal ideation among adolescents with ADHD (Becker et al., 2020). Given the nature of SCT, it has been suggested that mind-wandering may relate to, and possibly underpin, SCT symptoms that are characterized in part by excessive internal distractibility (Adams et al., 2010; Barkley, 2014). Only one study has examined SCT symptoms in relation to mind-wandering. Specifically, in a large sample of college students, SCT symptoms were more strongly associated than ADHD symptoms with a self-report measure of mind-wandering (Fredrick et al., 2020). However, no study has tested whether SCT symptoms are associated with greater mind-wandering in adolescence or in individuals diagnosed with ADHD. It is especially important to examine the possible association between SCT and mind-wandering in adolescence, given evidence that symptoms of SCT increase during this developmental period (Leopold et al., 2016).
The present study builds on previous research by being the first to test whether SCT symptoms are uniquely associated with greater self-reported mind-wandering while controlling for ADHD and internalizing symptoms among adolescents diagnosed with ADHD. This is important given growing interest in understanding both mind-wandering within ADHD (Bozhilova et al., 2018) and the role of SCT in ADHD heterogeneity (Becker & Willcutt, 2019). In addition to controlling for ADHD symptom severity, adolescent anxiety and depressive symptoms were also included as covariates, given previous research showing these symptom domains to each be associated with excessive mind-wandering (Figueiredo et al., 2020; Marchetti et al., 2016).
Method
Participants
Participants were 79 adolescents (70% male) aged 13 to 17 years (M = 14.96, SD = 1.10) diagnosed with ADHD. Approximately two thirds (n = 60) met criteria for ADHD predominantly inattentive presentation based on the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS; Kaufman et al., 1997, 2013) interview conducted with the adolescent’s parent; the remaining participants met criteria for ADHD combined presentation. Based on the K-SADS interview conducted separately with the adolescent and his or her parent, 10.1% (n = 8) met criteria for a co-occurring internalizing disorder and 7.6% (n = 6) met criteria for co-occurring oppositional defiant disorder (ODD). Approximately one third (n = 29) of the adolescents were taking medication for ADHD. The majority of adolescents were non-Hispanic White (n = 63), with remaining participants Black (n = 8), Multiracial (n = 7), or Hispanic (n = 1). All participants had an IQ ≥ 70 (range = 72–132) based on the Kaufman Brief Intelligence Scale, Second Edition (KBIT-2; Kaufman & Kaufman, 2004).
Procedures
This study was approved by the institutional review board (IRB). Data used in the present study were collected during an inclusion visit as part of a broader study focused on sleep in adolescents with ADHD (Becker et al., 2019a). The recruitment materials for the broader study focused on examining sleep in adolescents with ADHD, though the study was not specific to adolescents with sleep problems. Recruitment materials were distributed via local schools, in the community, and at the institution where the study was conducted. Parents who contacted the research staff in response to these recruitment activities were given additional information and were administered a phone screen to assess initial eligibility. At the inclusion/exclusion evaluation, all parents signed informed consent, and youth provided signed assent. All adolescents were required to meet full Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) criteria for ADHD predominantly inattentive presentation or ADHD combined presentation on the K-SADS interview conducted with the parent to be eligible. Exclusion criteria included a diagnosis of autism, bipolar disorder, obsessive-compulsive disorder, or psychosis (per parent report during the phone screen or assessed during the K-SADS interview); possible presence of sleep-disordered breathing, periodic limb movement disorder, or restless leg syndrome; history of epilepsy or head trauma resulting in loss of consciousness; IQ < 70; regular high caffeine use (more than one coffee/energy drink or three caffeinated soft drinks per day); highly atypical sleep duration (routinely obtaining <6 hr of >9.5 hr on school nights); or obligations that required a bedtime later than 10:00 p.m. or waking prior to 6:00 a.m. See Becker et al. (2019a) for additional details.
Measures
SCT symptoms
The Child Concentration Inventory, Second Edition (CCI-2; Becker, 2015), was used to measure adolescent self-reported SCT symptoms. The CCI-2 consists of 16 items rated on a four-point scale (0 = never to 3 = always), with higher scores indicating higher frequency of SCT symptoms. The CCI-2 has shown strong internal consistency (αs = .80–.95; Becker et al., 2019a; Sáez et al., 2019) and moderate correlations with parent- and teacher-reported SCT (rs = .29–.36) (Sáez et al., 2019). Three adolescent-reported items previously found to show poor discriminative validity were not used in the present study (Becker et al., 2020; Sáez et al., 2019) In addition, to eliminate potential contamination of the SCT scale with the Imaginal Process Inventory (IPI) daydreaming measure of mind-wandering described below, one item (“I daydream”) was removed from the SCT scale in the present study. Internal consistency for the resulting 12-item total mean SCT scale in the present study was good (α = .87).
ADHD symptoms
The Conners-3 Short (Conners, 2008) is a widely used self-report questionnaire that includes core symptoms of ADHD. Adolescents reported on the frequency of six inattentive items and five hyperactive-impulsive (HI) items on a four-point scale (0 = not true at all [never, seldom], 3 = very much true [very often, very frequently]). In the present study, mean subscale scores were calculated for ADHD-IN (α = .86) and ADHD-HI (α = .83).
The Vanderbilt ADHD Diagnostic Parent Rating Scale (VADPRS) was used to measure parent-reported adolescent ADHD symptoms. The VADPRS (Wolraich et al., 2003) includes all nine inattentive (ADHD-IN) and nine hyperactive-impulsive (ADHD-HI) DSM ADHD symptoms. Each item is rated on a four-point scale (0 = never, 3 = very often). In the present study, mean subscale scores were used for ADHD-IN (α = .90) and ADHD-HI (α = .90).
Depression and anxiety symptoms
The Revised Child Anxiety and Depression Scales (RCADS) was used to evaluate adolescent-reported internalizing symptoms. The RCADS (Chorpita et al., 2005) is a 47-item measure that assesses anxiety and depression disorder symptoms on a four-point scale (0 = never, 3 = always). The RCADS has good psychometric properties and has demonstrated excellent reliability and validity in clinical and nonclinical samples (Chorpita et al., 2000, 2005) including in youth evaluated for ADHD specifically (Becker et al., 2019b). In the present study, mean scores for the total anxiety (α = .92) and depression (α = .76) scales were calculated.
Mind-wandering
The IPI (Singer & Antrobus, 1966) daydreaming frequency subscale was used to measure adolescent-reported mind-wandering. The 12-item IPI daydream-ing frequency subscale instructs participants to respond to their frequency of daydreaming over the past week on a five-point scale. The IPI daydreaming frequency subscale has often been used as a measure of mind-wandering and has been correlated with task-unrelated thoughts during sustained attention tasks (Mrazek et al., 2012; Stawarczyk et al., 2012). Internal consistency was good in the present study (α = .96).
Analyses
First, zero-order correlation analyses were conducted to examine the correlations among the study variables. Adolescent sex and race were binary variables (see Table 1), and correlations involving these variables are point-biserial correlations. A correlation of .10 is considered a small effect, .30 is considered a medium effect, and .50 is considered a large effect. Next, two hierarchical regression analyses were conducted to examine whether SCT symptoms were associated with mind-wandering above and beyond other psychopathology dimensions. Specifically, ADHD-IN, ADHD-HI, depression, and anxiety symptoms were entered at Step 1, and then SCT symptoms were entered at Step 2. The first (primary) regression model included adolescent self-reported ADHD symptoms such that all psychopathology dimensions were completed by the same informant (adolescent self-report). The second regression model replaced adolescent-reported ADHD symptom dimensions with parent-reported ADHD symptom dimensions.
Intercorrelations and Descriptive Statistics of Study Variables.
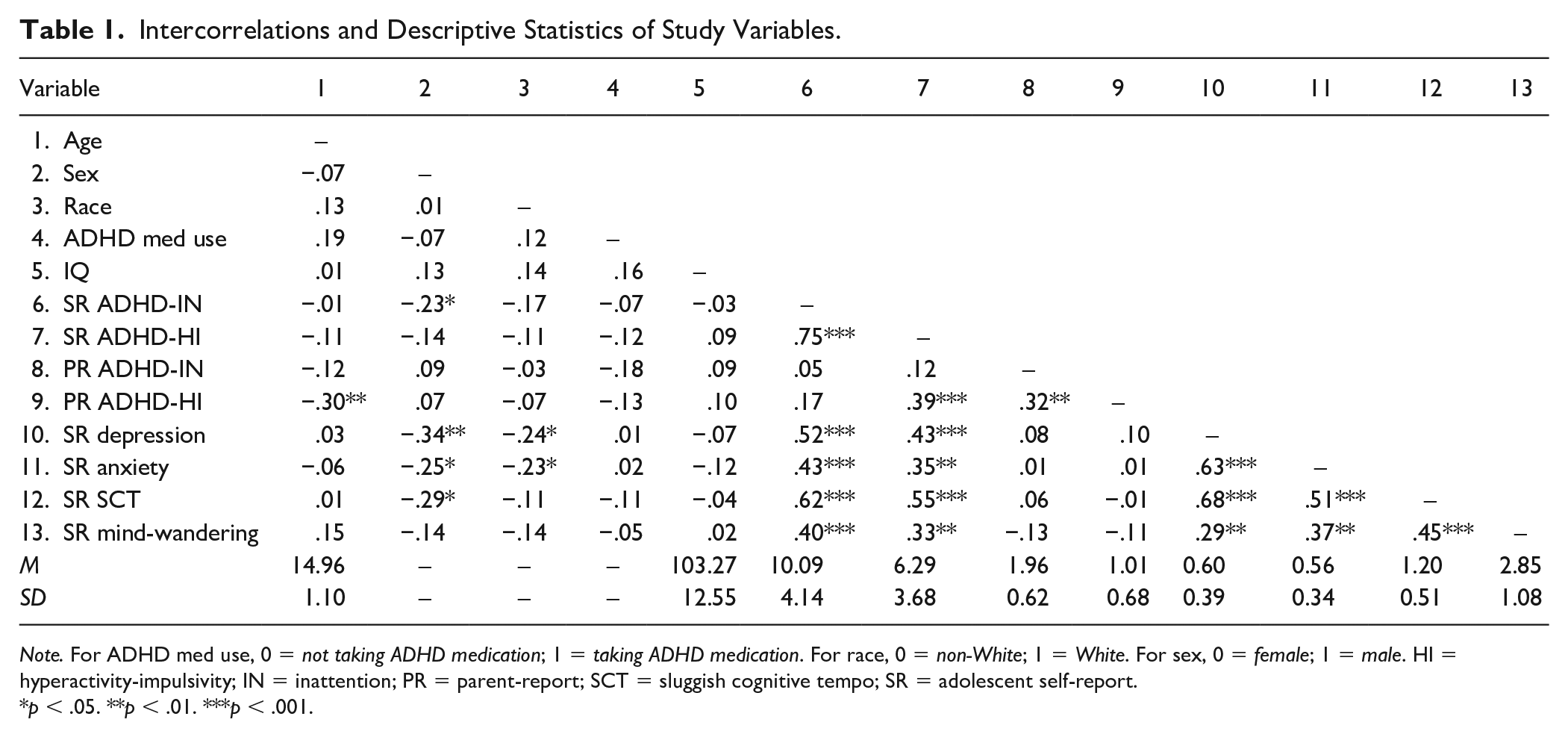
Note. For ADHD med use, 0 = not taking ADHD medication; 1 = taking ADHD medication. For race, 0 = non-White; 1 = White. For sex, 0 = female; 1 = male. HI = hyperactivity-impulsivity; IN = inattention; PR = parent-report; SCT = sluggish cognitive tempo; SR = adolescent self-report.
p < .05. **p < .01. ***p < .001.
Results
Correlation Analyses and Descriptive Statistics
Descriptive statistics and intercorrelations among study variables are provided in Table 1. Age, sex, race, ADHD medication use, and IQ were not significantly correlated with mind-wandering (all ps > .05) and are not considered further. All adolescent-reported psychopathology dimensions were significantly, moderately associated with greater mind-wandering (rs = .30–.45, all ps < .01; see Table 1). Parent-reported ADHD-IN and ADHD-HI symptom dimensions were not significantly associated with adolescent-reported mind-wandering (both ps > .05).
Regression Analyses
The hierarchical regression analysis examining adolescent-reported psychopathology symptoms in relation to mind-wandering is shown in Table 2. In Step 1, no variable was uniquely associated with mind-wandering (self-reported ADHD-IN and anxiety had marginal associations, ps = .09 and .06, respectively; Step 1 R2 = .21). In Step 2, above and beyond self-reported ADHD and internalizing symptom dimensions, self-reported SCT symptoms remained significantly associated with greater mind-wandering (β = .35, p = .027; ΔR2 = .05). No other psychopathology dimension was significantly associated with mind-wandering in the regression analysis (all ps > .05).
Regression Analysis Examining Self-Reported Sluggish Cognitive Tempo and Other Psychopathology Dimensions in Relation to Mind-Wandering on the Imaginal Process Inventory in Adolescents With ADHD.

Note. HI = hyperactivity-impulsivity; IN = inattention; SCT = sluggish cognitive tempo.
p < .10. *p < .05. **p < .01. ***p < .001.
The hierarchical regression analysis was repeated using parent-reported ADHD symptom dimensions instead of adolescent self-reported ADHD symptoms dimensions. The pattern of findings was unchanged. In the model using parent-reported ADHD symptoms, adolescent-reported anxiety symptoms were significantly associated with greater mind-wandering at Step 1 (β = .29, p = .038; Step 1 R2 = .17). However, when SCT symptoms were added at Step 2, anxiety was no longer significantly associated with mind-wandering (β = .23, p = .08). At Step 2, SCT symptoms was the only psychopathology dimension to be significantly associated with mind-wandering (β = .43, p = .004; ΔR2 = .09). 1
Discussion
Although there has been recent interest in mind-wandering and ADHD (Lanier et al., 2021), research has overlooked the role of SCT symptoms, and studies with populations outside young adulthood are almost entirely nonexistent. Thus, the current study tested whether adolescent SCT symptoms would be uniquely associated with greater self-reported mind-wandering while controlling for ADHD symptoms and internalizing symptoms in a sample of adolescents with ADHD. Findings showed that adolescent-reported SCT symptoms, but not adolescent- or parent-reported ADHD symptoms or adolescent-reported internalizing symptoms, were uniquely associated with greater self-reported mind-wandering. These findings are an important contribution to the literature in light of growing interest in mind-wandering and ADHD and underscore the need to incorporate SCT symptoms as this body of research continues to advance.
SCT and Mind-Wandering
Although all adolescent-reported psychopathology dimensions were significantly positively associated with mind-wandering in the correlation analyses, SCT symptoms were the only symptom domain associated with greater self-reported mind-wandering in the regression analyses. Although a recent systematic review indicated that mind-wandering may be a central feature of ADHD (Lanier et al., 2021), in addition to a study showing adolescent-reported ADHD to be uniquely related to mind-wandering (Figueiredo et al., 2020), findings from the present study suggest that ADHD’s association with mind-wandering may in fact be better, or at least in part, explained by co-occurring SCT symptoms.
Findings from the current study are consistent with a small but growing body of research identifying unique relations between SCT and patterns of task-unrelated thought (Becker et al., 2020; Fredrick et al., 2020). Specifically, SCT symptoms have been found to be more strongly associated than ADHD symptoms with greater mind-wandering and rumination in a large sample of young adults (Fredrick et al., 2020). In addition, a recent study found adolescent-reported SCT symptoms, but not ADHD-IN symptoms, to be uniquely associated with more ruminative responses (Becker et al., 2020). Findings from the present study add to this area of research and suggest that SCT, more so than ADHD-IN and internalizing symptoms, may be marked by excessive internal distractibility (Adams et al., 2010). Although adolescents with ADHD often experience a wide range of attentional problems, adolescents with elevated SCT symptoms may have particular trouble with task performance as a result of excessive internal thoughts unrelated to the present task.
Limitations and Future Directions
Despite strengths of the current study, a few limitations are worth noting. First, the cross-sectional nature of the study prevents inferences regarding causal relationships between SCT and mind-wandering. Future research would benefit from testing whether SCT symptoms are prospectively associated with greater mind-wandering (and vice versa). Second, the current study relied on self-report measures of psychopathology and mind-wandering, with the exception of parent-reported ADHD, and it would be highly useful for future studies to include experimental measures of mind-wandering during a sustained attention to response task and other informants of SCT. An interesting next step will be to test whether adolescent SCT symptoms explain the frequency of mind-wandering during experimental designs (e.g., sustained attention tasks) compared with ADHD symptoms. Third, our study included a relatively small sample of adolescents with ADHD and had eligibility restrictions related to sleep and caffeine intake, and it will be important for future studies to replicate our findings in larger samples with broader inclusion criteria, as well as to evaluate whether SCT is similarly associated with mind-wandering in youth with and without ADHD.
Conclusion
This study examined mind-wandering in adolescents diagnosed with ADHD, an important population that frequently experiences co-occurring SCT symptoms. The current study is the first to demonstrate that adolescent-reported SCT symptoms are uniquely associated with greater self-reported mind-wandering in adolescents with ADHD. When SCT symptoms were examined simultaneously with ADHD and internalizing symptoms, only SCT symptoms remained significantly associated with greater mind-wandering. These findings highlight the importance of including SCT in studies seeking to better understand the interrelations between ADHD and mind-wandering.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the U.S. National Institutes of Health (NIH).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant R03MH109787 from the National Institute of Mental Health (NIMH). S.P.B. is supported by award number K23MH108603 from the NIMH.