
Abstract
Adults with autism spectrum disorder often experience co-occurring mental health problems such as attention-deficit/hyperactivity-disorder, as well as impairments in executive function. Sluggish cognitive tempo, a cluster of behaviors including slow processing, daydreaming, and mental fogginess, has been shown to be associated with attention-deficit/hyperactivity-disorder. This study was designed to assess sluggish cognitive tempo in young adults with autism spectrum disorder. Specifically, we sought to establish a preliminary estimate of clinically significant sluggish cognitive tempo symptoms and to better understand its phenomenology and associations with executive function and psychiatric symptoms in the context of autism spectrum disorder. Young adults with autism spectrum disorder (n = 57; age 16–25 years; 84.2% male) completed a laboratory-based executive function task, and parents and participants completed measures of the participants’ sluggish cognitive tempo, attention-deficit/hyperactivity-disorder, depression, and anxiety symptoms. Nearly one-third of the sample exhibited clinically impairing levels of sluggish cognitive tempo. Although sluggish cognitive tempo and attention-deficit/hyperactivity-disorder symptoms were significantly correlated, findings suggest the constructs are distinct. Results also suggest that increased sluggish cognitive tempo is related to executive function impairment and depression, but not anxiety symptoms. Considerations for assessment and long-term impacts of sluggish cognitive tempo for adults with autism spectrum disorder are discussed.
Lay abstract
Adults with autism spectrum disorder often experience a range of co-occurring mental health problems such as attention-deficit/hyperactivity-disorder, as well as difficulties with executive function. Sluggish cognitive tempo, a cluster of behaviors including slow processing, daydreaming, and mental fogginess, has been shown to be associated with attention-deficit/hyperactivity-disorder, and limited research has suggested that individuals with autism spectrum disorder may experience sluggish cognitive tempo. We examined co-occurring mental health problems and executive function in 57 young adults with autism spectrum disorder, aged 16–25 years to better understand sluggish cognitive tempo in autism spectrum disorder. Parents of the young adults answered questions about their children’s sluggish cognitive tempo, attention-deficit/hyperactivity-disorder, depression, and anxiety symptoms, and the young adults completed tests of their executive function. Results demonstrated that nearly one-third of the sample exhibited clinically impairing levels of sluggish cognitive tempo. Although sluggish cognitive tempo and attention-deficit/hyperactivity-disorder symptoms were related, our findings suggest they are not the same constructs. Increased sluggish cognitive tempo is related to more difficulties with executive function and increased depression, but not anxiety symptoms. Results demonstrate that sluggish cognitive tempo may pose heightened difficulties for adults with autism spectrum disorder, making it an important construct to continue studying. Considerations for assessment and long-term impacts of sluggish cognitive tempo for adults with autism spectrum disorder are discussed.
Keywords
Many individuals with autism spectrum disorder (ASD) experience high rates of co-occurring psychiatric symptoms (White et al., 2018) and impairment in executive function (EF; Demetriou et al., 2018; Wallace et al., 2016), which are predictive of poorer outcomes in adulthood (Pugliese et al., 2016). There are several phenotypic similarities between ASD and sluggish cognitive tempo (SCT), such as slow processing and mental fogginess (Reinvall et al., 2017). Despite similarities between ASD and SCT in symptomology and related psychiatric and EF correlates, there is limited research examining SCT in ASD.
Sluggish cognitive tempo
SCT is defined by a set of behavioral and cognitive symptoms including lethargy/apathy, slow processing, excessive daydreaming, and mental fogginess (Becker & Barkley, 2018; Becker, Leopold, et al., 2016). Although SCT is not a formal mental health diagnosis per the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V; American Psychiatric Association, 2013) or International Classification of Diseases, 11th edition (World Health Organization, 2018), it is a measurable behavioral construct that has historically been considered a facet of attention-deficit/hyperactivity-disorder (ADHD), predominantly inattentive presentation (ADHD-I; (Becker & Barkley, 2018; Becker et al., 2014)). However, there has been a shift in research within the last 20 years suggesting that although SCT is highly correlated with ADHD-I, it appears to be its own construct distinct from ADHD-I (Bauermeister et al., 2012; Becker & Barkley, 2018). Specifically, Becker, Leopold, et al. (2016) identified a double dissociation that suggests SCT and ADHD-I function independently of each other and are separately associated with other psychiatric constructs. This finding is supported by several studies using factor analysis to distinguish SCT from ADHD-I and other conditions such as ADHD predominantly hyperactivity/impulsivity presentation (ADHD-HI), anxiety, and depression (Barkley, 2014; Becker et al., 2014; Jarrett et al., 2017; Lee et al., 2014).
SCT appears to be a co-occurring condition experienced by children and adolescents with ASD (Duncan et al., 2018; Reinvall et al., 2017), though no studies have rigorously studied SCT in adults with ASD. Understanding the phenomenology of SCT in ASD is important given that SCT is associated with a range of functional impairments (Becker, Leopold, et al., 2016) and social difficulties (Becker, Withrow, et al., 2016; Marshall et al., 2014). Furthermore, it has been suggested that SCT poses heightened risk for co-occurring depression. Specifically, it is suggested that hypoactivity and mental fogginess associated with SCT lead to challenges with social engagement and processing social information (Becker, Garner, et al., 2019; Rondon et al., 2020; Willcutt et al., 2014) and social isolation and withdrawal (Becker, Garner, et al., 2019), which are risk factors for depression (Coplan et al., 2013; Rudolph et al., 2008). Given that only two studies to-date have examined SCT symptomology and related correlates in ASD (Duncan et al., 2018; Reinvall et al., 2017), additional research is warranted to examine the phenomenology of SCT, particularly in adults with ASD as an under-researched population at risk of these adverse outcomes.
SCT and internalizing symptoms in ASD
Both Duncan et al. (2018; n = 51, 13–18 years old) and Reinvall et al. (2017; n = 55, 5–15 years old) found that youth with ASD who exhibited elevated SCT experienced more internalizing symptoms. However, SCT seems to be differentially related to anxiety and depression based on non-ASD research, as the relationship between SCT and depression seems generally more robust than SCT and anxiety (Becker, Leopold, et al., 2016; del Mar Bernad et al., 2014). This may simply reflect behavioral similarities between SCT and depression (e.g. lethargy/apathy). Alternatively, social difficulties linked to SCT and associated symptoms of apathy, slow processing, and daydreaming (Becker, Garner, et al., 2019) may heighten the risk of developing depression. Given the differing association of SCT with depression and anxiety, grouping them together under the umbrella of internalizing symptoms may not be the most informative approach. Instead, examining disorder-specific relationships with SCT allows for a richer examination of SCT’s clinical profile in ASD.
SCT and EF in ASD
Duncan and colleagues (2018) also identified an EF profile associated with SCT in youth with ASD. They found that SCT was associated with poorer daily life EF (i.e. ability to initiate, plan, organize, and self-monitor) for adolescents with ASD. These results are consistent with studies examining EF in both ASD and SCT samples. Difficulties with EF, particularly initiation, self-organization/planning, cognitive flexibility, and concept formation, are common in individuals with ASD (Demetriou et al., 2018; Kenworthy et al., 2008; Wallace et al., 2016) and have been linked to lower quality of life (de Vries & Geurts, 2015), deficits in adaptive functioning (Wallace et al., 2016) and poorer social skills (Leung et al., 2016). Extant research using ratings of daily life EF suggests that EF, particularly organization/planning, is also impaired for adults with SCT and without ASD (Barkley, 2012; Becker, Leopold, et al., 2016; Jarrett et al., 2017; Wood et al., 2017). However, the association between SCT and EF is less clear when using performance-based tests rather than ratings of daily life EF (Jarrett et al., 2017). Given the apparent link between SCT and increased EF impairment in adolescents with ASD, alongside research suggesting that EF impairment is linked to poorer outcomes in adults with ASD (Wallace et al., 2016), understanding whether SCT is associated with EF impairment may be particularly important for adults with ASD.
This study and hypotheses
This study aimed to build upon limited extant research by examining SCT symptomology in adults with ASD, a population that has not yet been considered in SCT research despite the implications that heightened SCT and its related correlates could pose. Furthermore, the study aimed to analyze disorder-specific relationships between ADHD, anxiety, depression, and SCT, as well as identify the relationship between SCT and EF impairment for adults with ASD. It was hypothesized that (1) SCT and ADHD symptoms would be positively associated, yet distinct from each other; (2) increased SCT would predict increased symptoms of depression and anxiety; and (3) increased SCT would predict poorer EF.
Method
Participants
Data were used from 57 adults, 16–25 years of age (M = 19.05, SD = 2.03) who were enrolled in a randomized controlled trial (RCT) which examined the effects of a college transition readiness curriculum for emerging adults with ASD (White et al., 2017, 2019). Participants were recruited through advertisements in local schools, autism-specific email listservs, and local mental health clinics. Inclusion criteria included: (1) a Full-scale IQ score of ≥80 and (2) an ASD diagnosis, confirmed through either a classification of “autism” on participants’ Individualized Education Plans (n = 19) or a clinical evaluation that included the Autism Diagnostic Observation Schedule-Second Edition (n = 38; Lord et al., 2012), administered by research reliable clinicians. Exclusion criteria included: (1) unmanaged psychopathology that warranted immediate clinical care (including clear suicidal intent or psychosis) and (2) current therapy that may be redundant with content of the transition readiness curriculum. For demographic information on the sample, please refer to Table 1.
Participant demographics (n = 57).
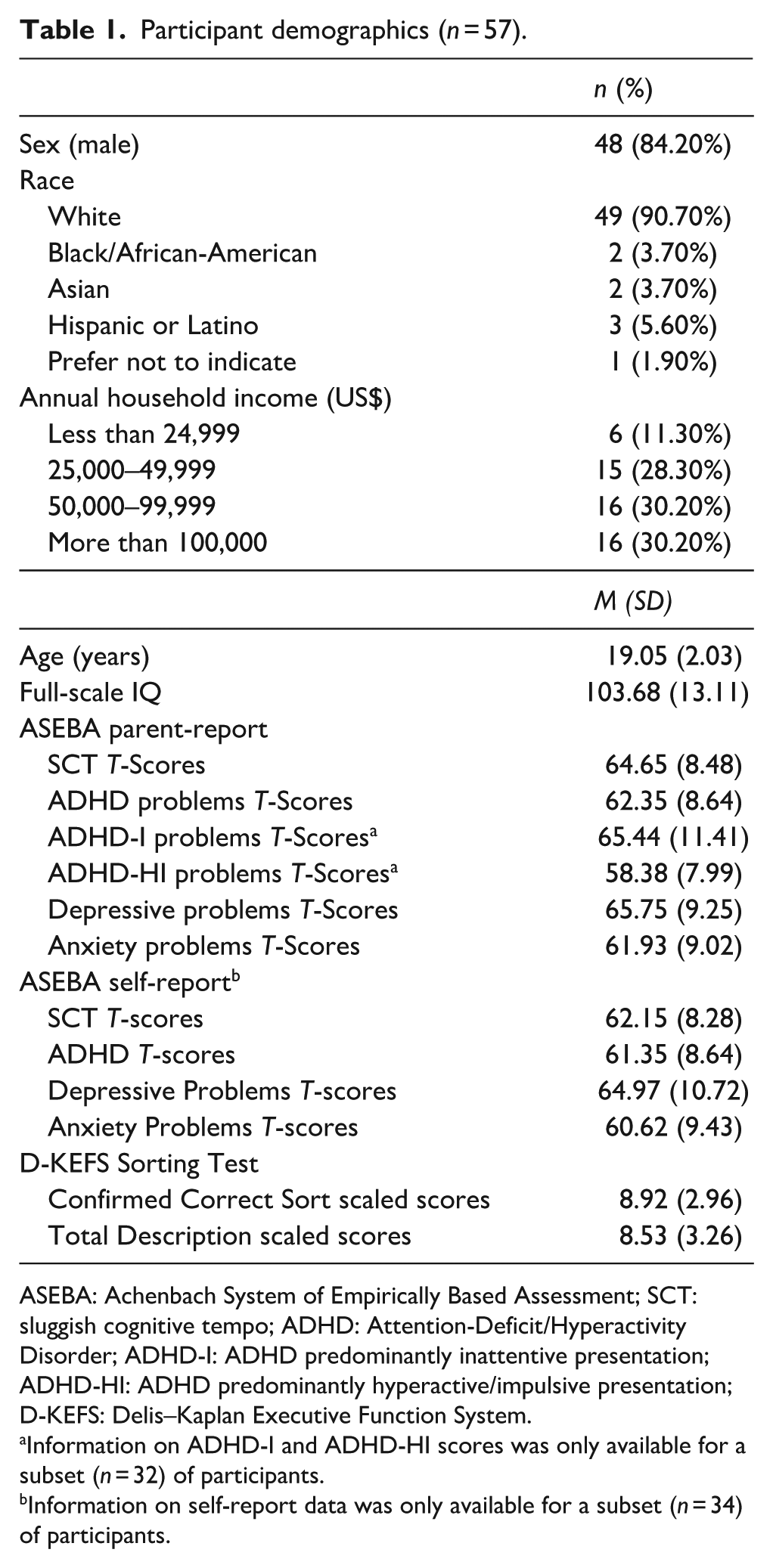
ASEBA: Achenbach System of Empirically Based Assessment; SCT: sluggish cognitive tempo; ADHD: Attention-Deficit/Hyperactivity Disorder; ADHD-I: ADHD predominantly inattentive presentation; ADHD-HI: ADHD predominantly hyperactive/impulsive presentation; D-KEFS: Delis–Kaplan Executive Function System.
Information on ADHD-I and ADHD-HI scores was only available for a subset (n = 32) of participants.
Information on self-report data was only available for a subset (n = 34) of participants.
Only pre-treatment data from the RCT were used for this study. The study was approved by the university’s institutional review board for human subjects research and participants provided consent and/or assent prior to initiating the study. Participants and their parents completed a clinical intake and a battery of questionnaires.
Measures
Achenbach System of Empirically Based Assessment
The severity of symptomology was measured through the Achenbach System of Empirically Based Assessment (ASEBA) battery (Achenbach & Rescorla, 2001, 2003). The Adult Behavior Checklist (ABCL; Achenbach & Rescorla, 2003) was administered to the parents of participants aged 18–25 years and the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001) was administered to parents of study participants aged 16–17 years. A subset of participants (n = 34) also completed the Adult Self Report (ASR; Achenbach & Rescorla, 2003). In this study, T-scores were used from the SCT, ADHD Problems, Depressive Problems, and Anxiety Problems Scales on the ABCL, CBCL, and ASR. For the subset of participants with ABCL data (n = 32), Inattention and Hyperactivity/Impulsivity subscales of the ADHD Problems Scale were also used to determine specific relationships between SCT and the ADHD subtypes (ADHD-I and ADHD-HI). Data on the ADHD subtypes were not available for the CBCL or ASR. T-scores less than 65 (i.e. less than 1.5 SD above the mean) are considered to be within the normal range, those between 65 and 69 (i.e. between 1.5 and 2 SD above the mean) are considered borderline, and T-scores of 70 and above (i.e. 2 or more SD above the mean) are considered clinically elevated (Achenbach & Rescorla, 2001, 2003). T-scores were used as opposed to raw scores to control for differences in the number of items across subscales of the ABCL and CBCL (Berkovits et al., 2017). Reliability, validity, and stability are well-documented for the ASEBA measures (Achenbach & Rescorla, 2001, 2003); see Table 2 for the reported internal consistency for each of the scales used on all three of the ASEBA measures.
Cronbach’s alpha coefficients of the ASEBA subscales.
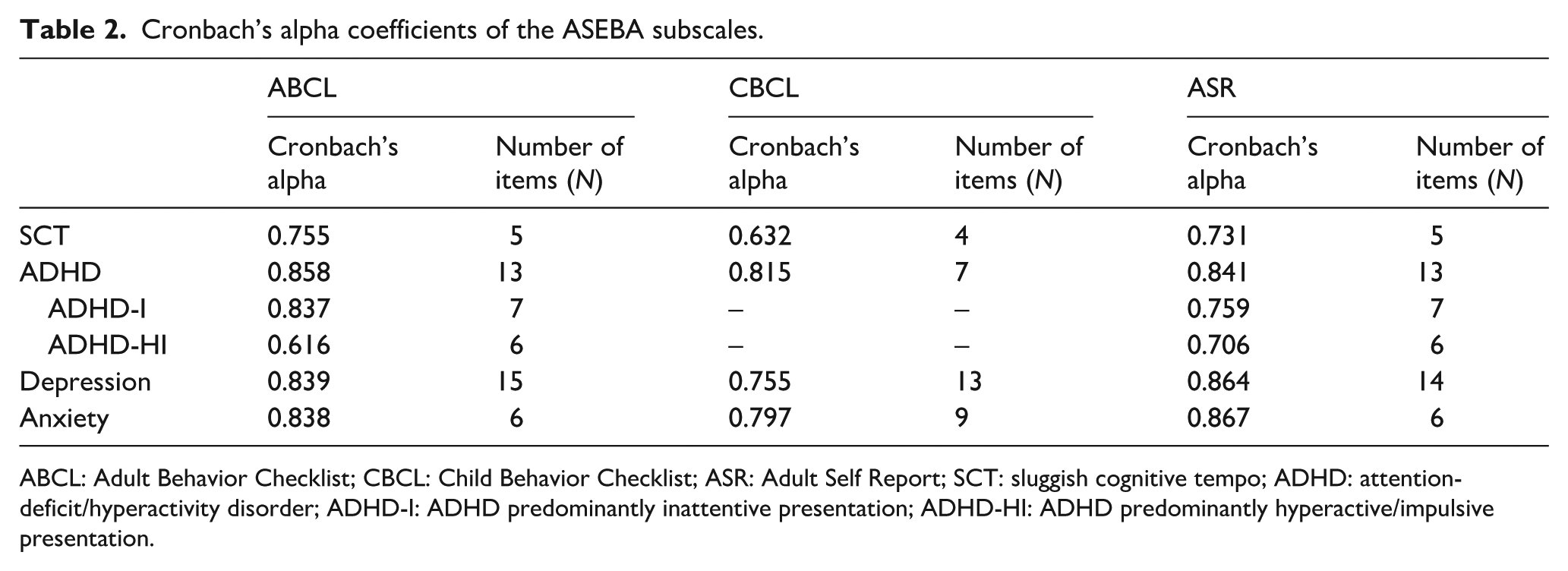
ABCL: Adult Behavior Checklist; CBCL: Child Behavior Checklist; ASR: Adult Self Report; SCT: sluggish cognitive tempo; ADHD: attention-deficit/hyperactivity disorder; ADHD-I: ADHD predominantly inattentive presentation; ADHD-HI: ADHD predominantly hyperactive/impulsive presentation.
Delis–Kaplan Executive Functioning System
The Delis–Kaplan Executive Functioning System (D-KEFS) Sorting Test is a performance-based task designed to measure EF skills of self-organization/planning, initiation, concept formation, and cognitive flexibility (Delis et al., 2001) and has previously been used in ASD samples (Semrud-Clikeman et al., 2014; Solomon et al., 2011). The Confirmed Correct Sorts scaled score reflects the number of correct sorts the participant makes. The Total Description scaled score is a measure of how accurately the participant explains how she/he sorted card groups. The Total Description scaled score builds on EF skills tapped by the Confirmed Correct Sorts scaled score by requiring participants to demonstrate verbal concept formation in addition to spatial concept formation (Delis et al., 2001) and is thought to detect subtler EF deficits given its higher cognitive demand (Delis et al., 2004; Parmenter et al., 2007). Scaled scores have a range of 1–19 with a mean of 10 (SD = 3), where higher scores reflect better EF skills.
Wechsler Abbreviated Scales of Intelligence, Second Edition
The Wechsler Abbreviated Scales of Intelligence, Second Edition (WASI-II) is a measure of cognitive abilities for individuals aged 6–89 years (Wechsler, 2011). The two-subtest Full Scale IQ (FSIQ-2) is a composite of overall IQ from the Vocabulary and Matrix Reasoning subtests. The WASI-II has demonstrated strong reliability and validity, and FSIQ-2 scores are highly correlated with four-subtest Full Scale IQ scores (Wechsler, 2011).
Statistical analyses
Data were analyzed using IBM SPSS Statistics Version 24. Prior to analyses, assumptions for regression analyses, including checking for outliers, were examined. Descriptive statistics and internal consistency of the ASEBA measures were examined. See Table 1 for descriptive statistics and Table 2 for internal consistencies of all ASEBA scales. Correlations between demographic and study variables were run to identify possible covariates needed for primary analyses (see Table 3). In addition, FSIQ-2 scores were positively correlated with both D-KEFS variables; thus, FSIQ-2 scores were entered as a covariate to test the third hypothesis.
Bivariate correlations between demographic and main study variables.
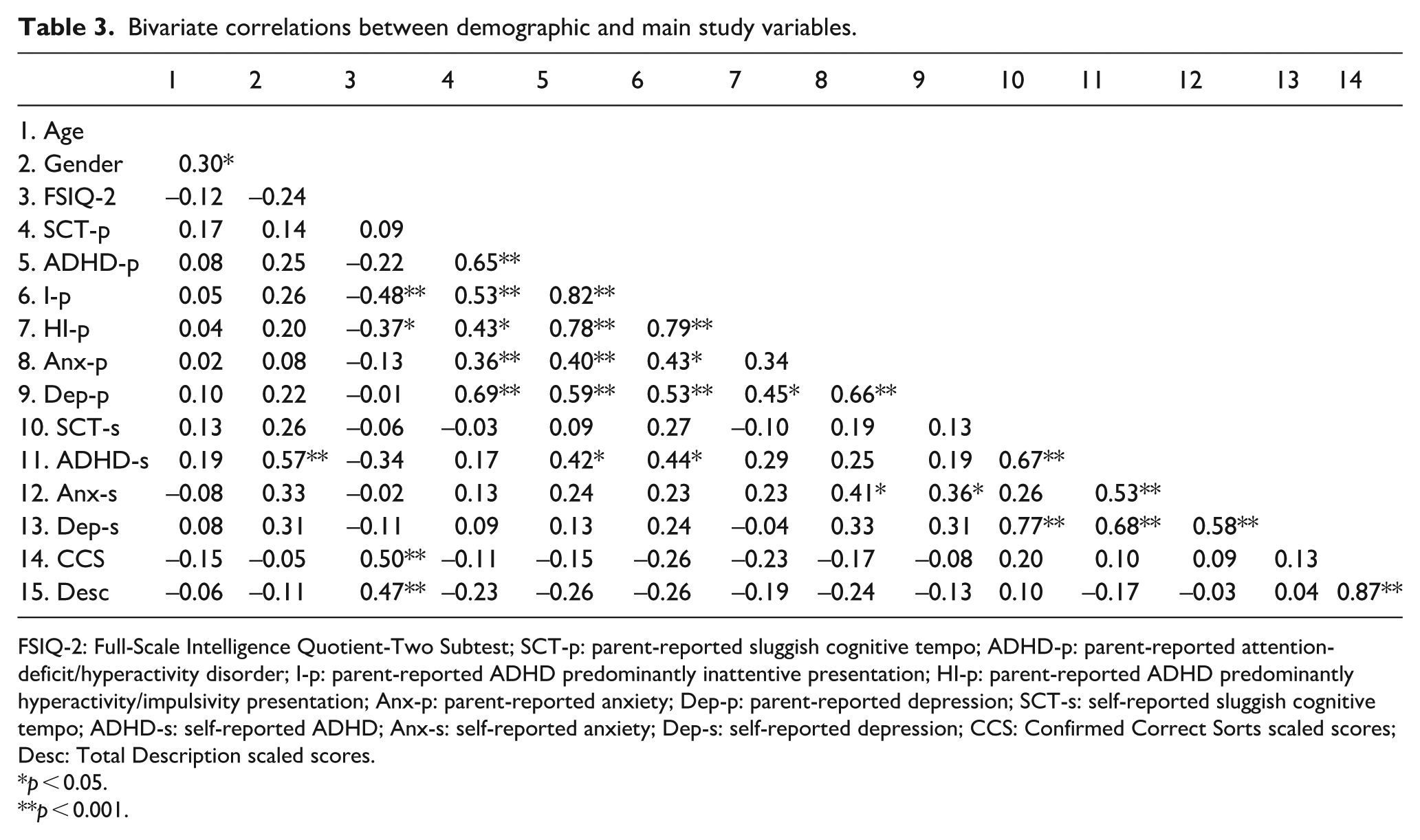
FSIQ-2: Full-Scale Intelligence Quotient-Two Subtest; SCT-p: parent-reported sluggish cognitive tempo; ADHD-p: parent-reported attention-deficit/hyperactivity disorder; I-p: parent-reported ADHD predominantly inattentive presentation; HI-p: parent-reported ADHD predominantly hyperactivity/impulsivity presentation; Anx-p: parent-reported anxiety; Dep-p: parent-reported depression; SCT-s: self-reported sluggish cognitive tempo; ADHD-s: self-reported ADHD; Anx-s: self-reported anxiety; Dep-s: self-reported depression; CCS: Confirmed Correct Sorts scaled scores; Desc: Total Description scaled scores.
p < 0.05.
p < 0.001.
We first conducted frequency analyses to examine the rates of clinically elevated and borderline SCT. We conducted a series of multiple regressions to analyze relationships among main study variables (SCT with ADHD, SCT with anxiety and depression symptoms when controlling for ADHD, and SCT with D-KEFS scores when controlling for FSIQ-2 scores).
Results
Estimate of SCT symptoms
Over one quarter of the sample (n = 16) had a parent-reported T-score in the clinically elevated range on the SCT subscale (i.e. T-score of 70 or above), and an additional 29.80% (n = 17) had a parent-reported T-score that fell within the borderline range (i.e. 65–69). Available ASR data from a subset of study participants (n = 34) was compared to rates of parent-reported SCT symptoms. Only 17.60% of participants (n = 6) rated themselves as having symptoms in the clinically elevated range, and an additional 17.60% of participants rated themselves as having symptoms in the borderline range, for a total of approximately one-third of the adults with self-report data indicating at least borderline levels of SCT.
Correlates of SCT
The assumptions for all regression analyses were met prior to running each model. Increased parent-reported SCT strongly predicted increased parent-reported ADHD, F(1, 56) = 40.71, p < 0.001, R2 = 0.43. Given the strong relationship between the two, exploratory regression analyses using a subset of participants (n = 32) with available data on specific ADHD subtypes were examined. Bivariate correlations demonstrated that SCT was strongly correlated with increased symptoms of ADHD-I (r(32) = 0.53, p = 0.002) and ADHD-HI (r(32) = 0.43, p = 0.015). For the first regression model, ADHD-HI was entered in step 1 to control for shared variance with ADHD-I and SCT was entered in step 2. There was a marginally significant R2 change from step 1 to step 2 (∆R2 = 0.04, ∆F(1, 29) = 3.88, p = 0.058) resulting in a significant overall model that accounted for 67% of the variance (F(2, 29) = 29.12, p < 0.001, R2 = 0.67). Although ADHD-HI was a significant predictor of ADHD-I at both step 1 (β = 0.79, p < 0.001) and step 2 (β = 0.69, p < 0.001), SCT (β = 0.23, p = 0.058) approached statistical significance as a predictor of ADHD-I. For the second regression model, ADHD-I was entered in step 1 and SCT was entered in step 2. There was not a significant change in R2 from step 1 to step 2 (∆R2 < 0.01, ∆F(1, 29) = 0.01, p = 0.913) although the overall model remained significant and accounted for 62% of the variance (F(2, 29) = 23.99, p < 0.001, R2 = 0.62). While ADHD-I strongly predicted ADHD-HI at both step 1 (β = 0.79, p < 0.001) and step 2 (β = 0.78, p < 0.001), SCT (β = 0.02, p = 0.913) did not predict ADHD-HI, suggesting the relationship between SCT and ADHD-HI may be explained by overlap with ADHD-I. See Table 4 for complete information on the predictors in this model.
Multiple regression analyses examining SCT and ADHD.
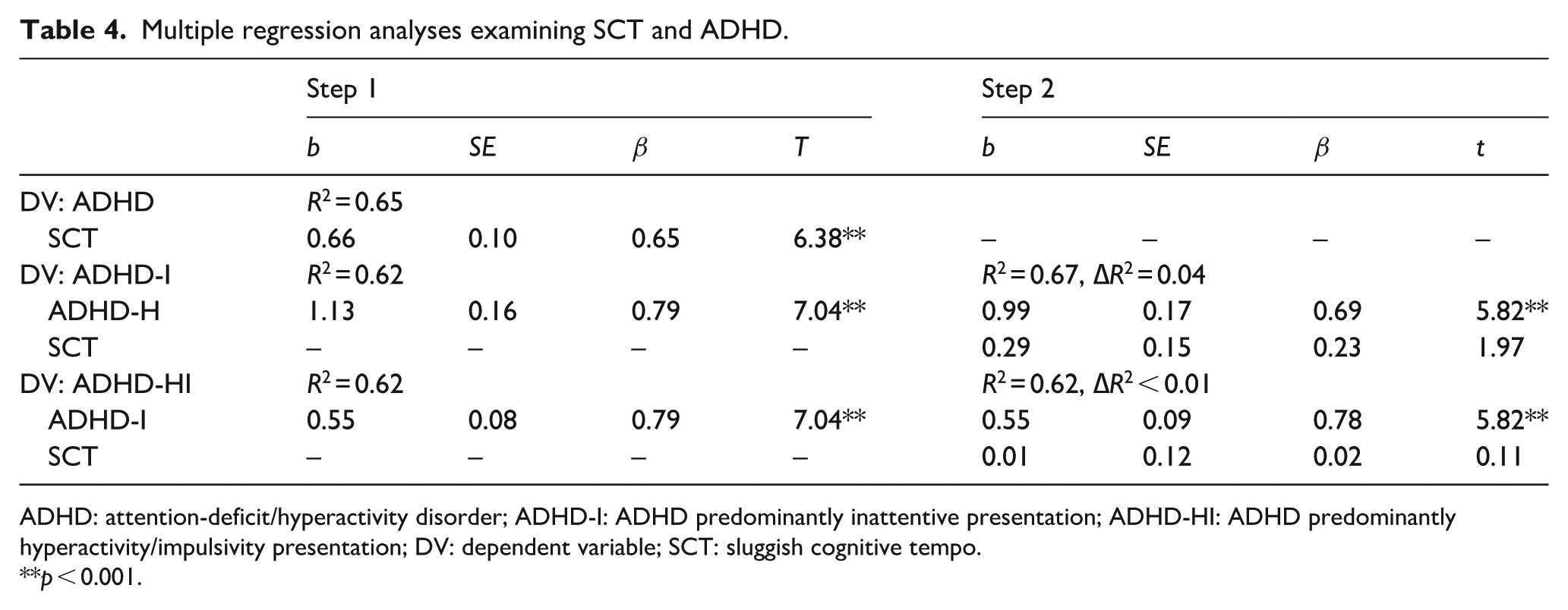
ADHD: attention-deficit/hyperactivity disorder; ADHD-I: ADHD predominantly inattentive presentation; ADHD-HI: ADHD predominantly hyperactivity/impulsivity presentation; DV: dependent variable; SCT: sluggish cognitive tempo.
p < 0.001.
A multiple regression was used to test the hypothesis that parent-reported SCT would predict increased symptoms of parent-reported depression. Based on preliminary analyses, parent-reported ADHD was strongly correlated with both parent-reported depression and SCT; thus, parent-reported ADHD was entered in step 1 of the model to control for shared variance. Parent-reported SCT was entered in step 2, resulting in a significant increase in R2 (∆R2 = 0.17, ∆F(1, 54) = 18.22, p < 0.001). The full model accounted for 51% of the total variance, F(2, 54) = 28.21, p < 0.001, R2 = 0.51. After controlling for parent-reported ADHD (β = 0.24, p = 0.062), parent-reported SCT (β = 0.54, p < 0.001) was a significant predictor of parent-reported depression symptoms. Follow-up exploratory analyses were conducted to determine whether similar results would be found when examining self-report data. Using ASR data available for a subset of participants (n = 34), results similarly showed a significant R2 increase after adding SCT to the model (∆R2 = 0.18, ∆F(1, 31) = 15.86, p < 0.001) and the overall model accounted for 64% of the variance (F(2, 31) = 28.03, p < 0.001, R2 = 0.64). Self-reported SCT (β = 0.58, p < 0.001) was a significant predictor of self-reported depression after controlling for self-reported ADHD symptoms (β = 0.29, p = 0.054). See Table 5 for information on predictors for both models.
Multiple regressions examining SCT and ADHD in relation to depression symptoms.
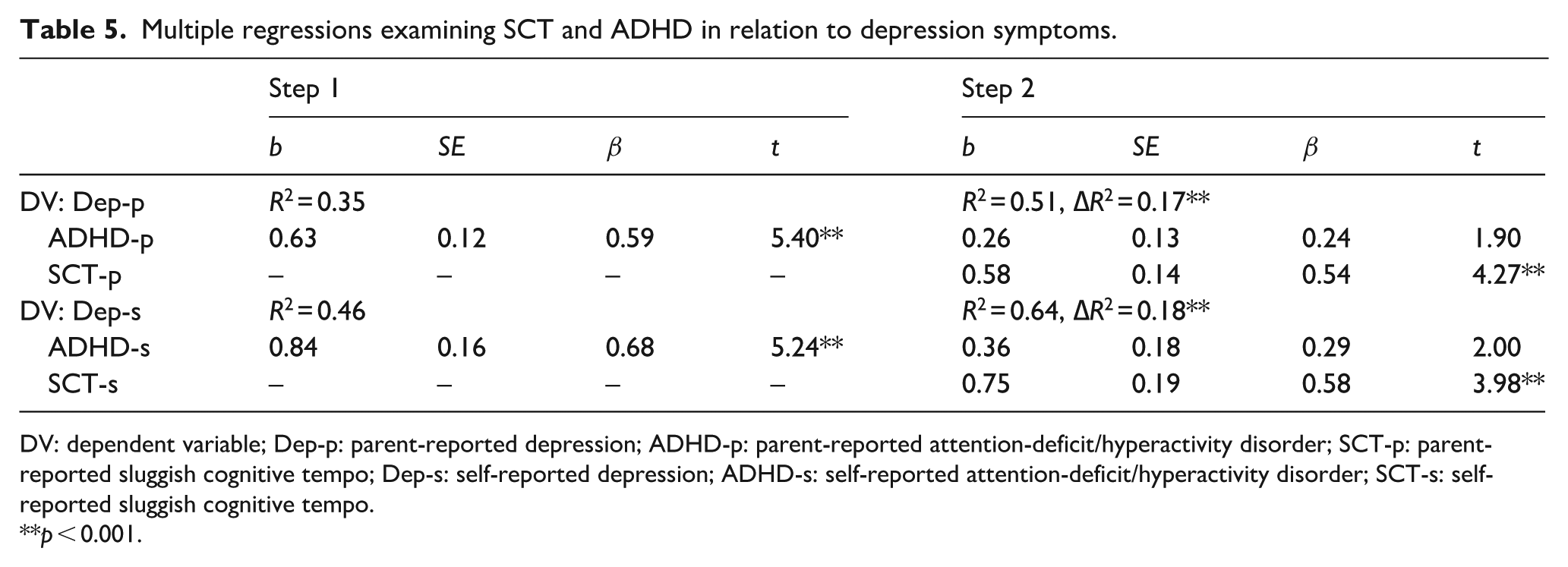
DV: dependent variable; Dep-p: parent-reported depression; ADHD-p: parent-reported attention-deficit/hyperactivity disorder; SCT-p: parent-reported sluggish cognitive tempo; Dep-s: self-reported depression; ADHD-s: self-reported attention-deficit/hyperactivity disorder; SCT-s: self-reported sluggish cognitive tempo.
p < 0.001.
A second regression analysis was conducted to examine the relationship between parent-reported SCT and anxiety symptoms. Preliminary correlations also showed a strong relationship between parent-reported ADHD and SCT, and ADHD and anxiety; thus, parent-reported ADHD symptoms were entered in step 1 of the model to control for shared variance. Parent-reported SCT was entered in step 2. Adding parent-reported SCT in step 2 did not result in a significant R2 change (∆R2 = 0.02, ∆F(1, 31) = 1.05, p = 0.311) although the overall model remained significant (F(2, 54) = 5.72, p = 0.006, R2 = 0.18). Parent-reported SCT (β = 0.17, p = 0.311) was not a significant predictor of parent-reported anxiety symptoms after controlling for parent-reported ADHD (β = 0.29, p = 0.081). Interestingly, ADHD was no longer a significant predictor of anxiety symptoms after adding SCT in step 2. Follow-up exploratory analyses were conducted using self-report data. Similar to parent-report data, there was not a significant increase in R2 after adding self-reported SCT in step 2 of the model (∆R2 = 0.02, ∆F(1, 31) = 0.74, p = 0.396) although the overall model accounted for 29% of the variance (F(2, 31) = 6.42, p = 0.005, R2 = 0.29). Self-reported SCT (β = −0.18, p = 0.396) was not a significant predictor of self-reported anxiety symptoms after controlling for self-reported ADHD (β = 0.64, p = 0.004). See Table 6 for complete information on predictors for both models.
Multiple regressions examining SCT and ADHD in relation to anxiety symptoms.
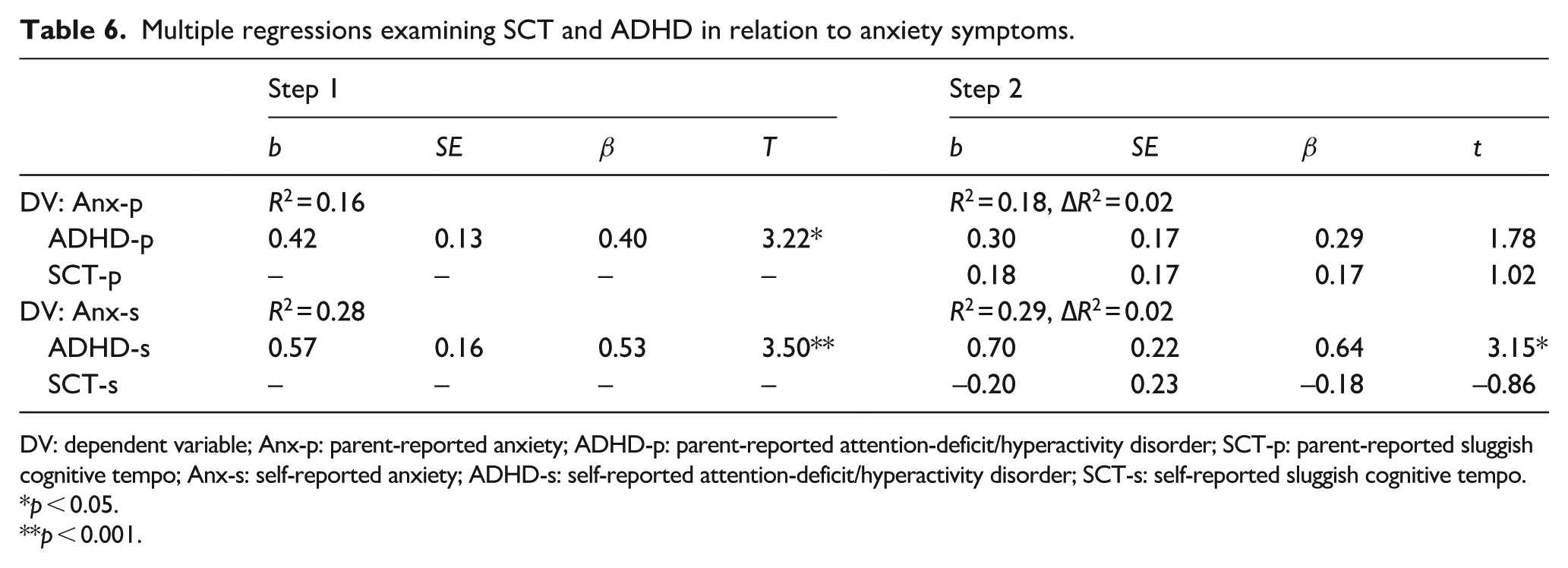
DV: dependent variable; Anx-p: parent-reported anxiety; ADHD-p: parent-reported attention-deficit/hyperactivity disorder; SCT-p: parent-reported sluggish cognitive tempo; Anx-s: self-reported anxiety; ADHD-s: self-reported attention-deficit/hyperactivity disorder; SCT-s: self-reported sluggish cognitive tempo.
p < 0.05.
p < 0.001.
Two separate multiple regression analyses were also utilized to test whether parent-reported SCT would be associated with poorer EF, using the D-KEFS Confirmed Correct Sort and Total Description scaled scores. Initial correlation analyses showed a strong relationship between cognitive ability and both EF variables; thus, cognitive ability was entered in step 1 of both models as a covariate. Parent-reported SCT was entered in step 2. There was not a significant R2 change from step 1 to step 2 in predicting Confirmed Correct Sort scaled scores (∆R2 = 0.03, ∆F(1, 46) = 1.72, p = 0.197) and the overall model accounted for 23% of the variance (F(2, 47) = 6.90, p = 0.002, R2 = 0.23). After controlling for cognitive ability (β = 0.46, p = 0.001), parent-reported SCT (β = −0.17, p = 0.193) was not a significant predictor of D-KEFS Confirmed Correct Sort scaled scores. However, there was a significant R2 change from step 1 to step 2 for the model predicting Total Description scaled scores (∆R2 = 0.08, ∆F(1, 48) = 4.89, p = 0.032) and the overall model accounted for 25% of the variance (F(2, 48) = 8.18, p = 0.001, R2 = 0.25). Parent-reported SCT (β = –0.28, p = 0.032) was a significant predictor of D-KEFS Total Description scaled scores after controlling for cognitive ability (β = 0.44, p = 0.001), suggesting that elevated SCT predicted poorer performance on the EF task as measured by the Total Description scaled score. See Table 7 for complete information on both models.
Multiple regressions examining SCT and cognitive ability in relation to EF.
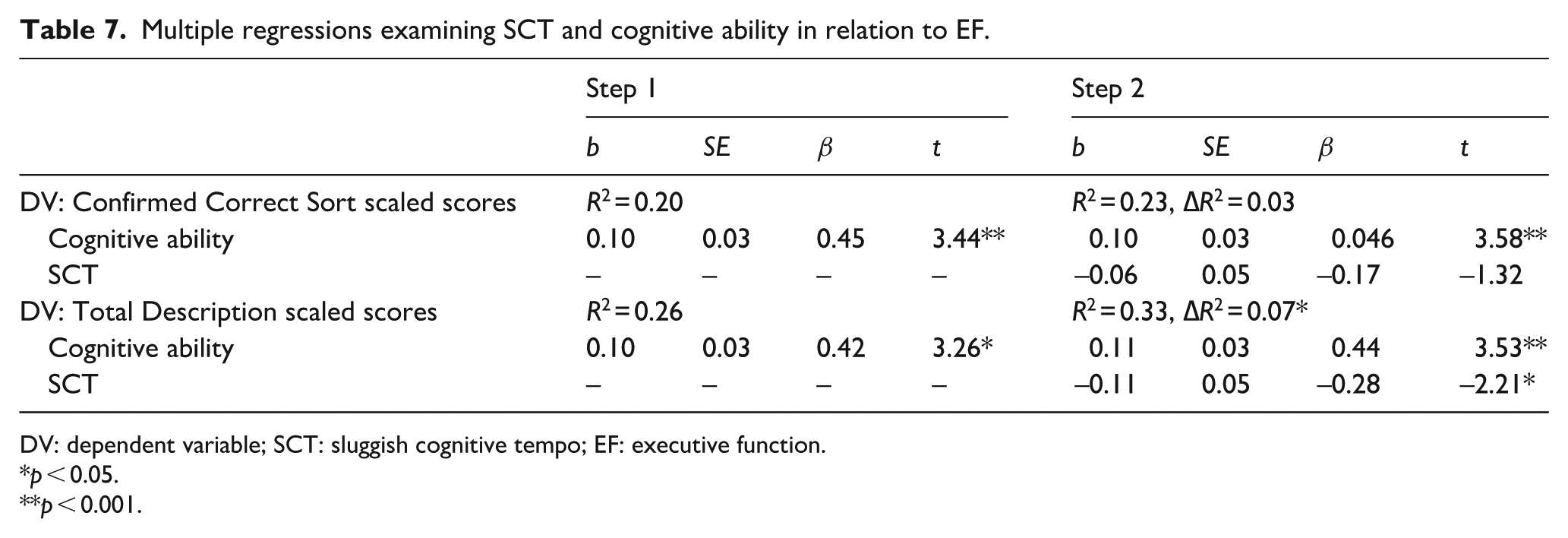
DV: dependent variable; SCT: sluggish cognitive tempo; EF: executive function.
p < 0.05.
p < 0.001.
Discussion
Our findings suggest that a substantial portion of cognitively able young adults with ASD exhibit clinically elevated symptoms of SCT. About 15% of our sample self-reported clinically elevated levels of SCT whereas about one-third of the sample was clinically elevated based on parent report. The degree of parent-reported SCT found in this study is similar to previous research using parent report; Duncan and colleagues (2018) reported about one-third of their sample of adolescents with ASD had clinically elevated SCT. Findings also highlight the importance of multiple informants when examining symptomology in adolescents and adults (De Los Reyes et al., 2015). Additional research is warranted with a larger sample to confirm whether these findings accurately reflect the SCT profile in adults with ASD.
The pattern of association between ADHD symptoms and SCT in this sample is similar to that reported in non-ASD samples (Becker & Barkley, 2018). The relationship between SCT and ADHD-I approached significance after accounting for ADHD-HI symptoms; however, SCT did not predict ADHD-HI after accounting for ADHD-I symptoms. This finding suggests that SCT is not associated with externalizing symptomology, as captured by hyperactivity, in adults with ASD and reflects the extant literature suggesting SCT more closely resembles internalizing symptoms and is protective against externalizing symptoms (Becker, Leopold, et al., 2016; del Mar Bernad et al., 2014). Moreover, SCT did not account entirely for shared variance in ADHD-I and ADHD-HI, suggesting that SCT reflects a separate cognitive symptom profile in ASD, as has been argued by Becker, Leopold, et al. (2016) in youth without ASD. As such, our first hypothesis was supported; SCT appears to be a related but dissociable construct from ADHD in adults with ASD.
Examination of SCT and parent- and self-reported internalizing symptoms indicates that SCT is linked to depression but not anxiety. SCT was a strong and statistically significant predictor of depression suggesting that SCT uniquely accounts for substantial variance in symptoms. This SCT–depression relationship echoes previous research with non-ASD populations which seems logical given similarities in the two constructs (e.g. slowed thinking and motor activity, difficulty concentrating, lack of energy). Recent work by Becker, Webb, and Dvorsky (2019) suggests that SCT predicts future depression symptoms in children; thus, this study’s findings may reflect heightened risk of depression for adults with ASD and increased SCT symptoms. This association also speaks to the potential importance of SCT in the context of distal psychiatric outcomes associated with depression (e.g. social withdrawal, substance abuse, suicide) for adults with ASD. However, prior studies with children and adolescents without ASD also have found a positive association between SCT and anxiety (albeit less robust than the depression association; Becker, Leopold, et al., 2016), which was not the case in this study. The small beta weight size and lack of a statistically significant SCT–anxiety association suggests that co-occurring SCT may not pose a heightened risk for anxiety symptoms among adults with ASD, despite anxiety being an important correlate of SCT in non-ASD samples. Continued research is needed to clarify whether the results of this study accurately reflect a non-significant association between anxiety and SCT in adults with ASD.
Finally, evidence of the relationship between SCT and EF was inconsistent such that SCT negatively predicted the measure of EF requiring spontaneous identification of sorted categories but was not associated with EF as assessed by a task that only required sorting the cards. It is important to emphasize that previous literature has not examined the association between these specific variables in an adult sample with ASD, so these results are interpreted with caution. It has been suggested that the Total Description scaled score measures complex EF because it requires higher cognitive demand (e.g. sorting and verbally articulating the concepts by which the cards have been sorted; Delis et al., 2004; Parmenter et al., 2007). Thus, it may be that this higher order EF requires more top-down processing which may be negatively impacted by SCT. This interaction between SCT and EF, potentially manifested in impaired top-down processing abilities, warrants consideration in the context of the growing research base examining interventions targeting EF deficits in adults with ASD (e.g. Eack et al., 2018). Given the continued finding that SCT presents as distinct from ADHD in these individuals, identification of broader EF deficits via a diagnosis of comorbid ADHD may be insufficient to properly treat EF impairments in this population. Rather, recognition of an additional SCT profile in adults with ASD might allow for modification of treatment protocols in order to better address these compounded deficits.
EF as measured by the Confirmed Correct Sorts total score may reflect more bottom-up cognitive processes to organize and plan card groups which are unaffected by elevated SCT, as compared with the top-down processing inherent to the Total Description scaled score. This pattern of results provides partial support for the hypothesized negative relationship between SCT and EF and is consistent with extant research suggesting that the association between SCT and EF is less clear when using performance-based EF tasks (Jarrett et al., 2017). Despite Duncan and colleagues (2018) finding a stronger relationship between EF impairment and SCT using daily life ratings, our partial findings using a performance-based measure may reflect within-construct measurement difficulties for EF (Jarrett et al., 2017; Toplak et al., 2013). Mixed findings on EF profiles across studies may also suggest that EF impairment associated with SCT is not as clear or pervasive as deficits associated with ADHD, further suggesting SCT is a construct neuropsychologically distinct from ADHD.
Findings should be interpreted within the context of the study’s limitations. Our relatively small sample of predominantly Caucasian male college students with ASD and average cognitive ability limits generalizability beyond the scope of this population. In addition, using the same measure to assess multiple constructs (i.e. ASEBA) presents a poignant methodological bias. However, Becker and colleagues (2014) provide evidence that SCT, ADHD, anxiety, and depression on ASEBA forms load onto different factors, and multiple subscales of the CBCL/ABCL have been used in previous literature to measure co-occurring symptomology (Becker, Garner, & Byars, 2016; Becker & Langberg, 2013; Garner et al., 2010; Raiker et al., 2015). The D-KEFS poses another limitation by providing a broad, multi-component measurement of EF rather than measurement of individual domains of EF that may be related to SCT. Future research utilizing an array of assessment instruments is needed to clarify the relationship between SCT, ADHD, specific EF domains, and other psychiatric symptoms in young adults with ASD. It should also be noted that although internal consistency was generally acceptable or higher (α ⩾ 0.70) for most of the ASEBA scales, the internal consistency of the CBCL SCT scale and ABCL ADHD-HI scale were sub-optimal (α = 0.636 and 0.612, respectively), although no items were determined particularly problematic. However, the CBCL SCT scale has been demonstrated to correlate strongly with longer SCT measures (Skirbekk et al., 2011) and its internal consistency in the current study appears to be consistent with other studies using the scale (Becker, Garner, & Byars, 2016; Becker & Langberg, 2013; Raiker et al., 2015).
To the authors’ knowledge, this preliminary study is the first to examine the presentation of clinically significant SCT symptoms and specific psychiatric correlates in young adults with ASD. Based on parent report, one-third of the young adults in this sample exhibited clinically elevated SCT. Results provide evidence that SCT may be a separate construct from ADHD, as it is in youth and adults without ASD. Evidence for the relationship between SCT and EF impairment is mixed which may be unsurprising given the complexity of EF and within-construct measurement difficulties (Toplak et al., 2013). The association between heightened SCT symptoms and elevated parent- and self-reported depression suggests an impairment profile consistent with recent research suggesting SCT is a risk factor for mood disorders (e.g. depression; Becker, Webb, & Dvorsky, 2019). It seems particularly critical that future research examines SCT symptoms longitudinally in adults with ASD to better understand the impact of SCT on cognitive functioning, mental health, and long-term outcomes. Given emerging evidence that remediation of SCT is possible for children without ASD (Pfiffner et al., 2007), if SCT is found to have a directional impact on outcome, it is possible that SCT may also be amenable to remediation therapeutically in ASD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health, Grant R34MH104337 (P.I.: S.W.W.).
Human and animal rights and informed consent
All study procedures were approved by the institutional review board for human subject research. All participants provided informed consent.