
Abstract
Objective:
Though psychiatric illnesses have been associated with increased COVID-19 infection risk, limited information exists about the relationship between ADHD and COVID-19.
Methods:
Using the TriNetX COVID-19 Research Network, we examined the impact of ADHD diagnosis and treatment on COVID-19 infection rates and outcomes.
Results:
ADHD patients had greater risk of COVID-19 (risk ratio (RR) 1.11, 95% CI [1.09, 1.12]). Increased risk was higher in females than males, and highest among Asian and Black patients. Within 60 days after COVID-19 diagnosis, ADHD patients had lower rates of hospitalization (RR 0.91, 95% CI [0.86, 0.96]) and mechanical ventilation (RR 0.69, 95% CI [0.58, 0.83]), and a nonsignificant reduced death rate (RR 0.65, 95% CI [0.42, 1.02]). Patients who recently received ADHD medication had higher rates of COVID-19 (RR 1.13; 95% CI [1.10, 1.15]).
Conclusion:
ADHD poses increased risk for COVID-19, but may reduce risk of severe outcomes. ADHD medications modestly impacted COVID-19 risk.
Introduction
COVID-19, caused by SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), has emerged as a major public health crisis (Peters, 2020; Sun et al., 2020) accounting for 613 million cases and 6.5 million deaths worldwide (to Sept 29th, 2022) (WHO Coronavirus (COVID-19) Dashboard). Risk factors linked to COVID-19 susceptibility and severity include physiologic conditions like hypertension and diabetes (Matsushita et al., 2020), as well as psychiatric conditions (Liu, Ni, et al., 2021; Wang et al., 2021).
Two studies using large electronic medical records in the US reported increased risk for COVID-19 infection in patients with psychiatric diagnoses, independent of known physical or medical risk factors. One study used the IBM Watson Health Explorys database, with 15,110 total COVID-19 patients (Wang et al., 2021); the other used the TriNetX US dataset of 62,354 COVID-19 patients (Taquet et al., 2021). A study from South Korea during the early stages of the pandemic (216,418 COVID-19 patients) found no significant association between infection rates and diagnosed mental illnesses, but reported significant associations with severe COVID-19 outcomes (Lee et al., 2020).
Merzon et al. examined the association of COVID-19 and ADHD using a cohort of 14,022 patients (1,416 with COVID-19) from the Israel Leumit Health Services database. ADHD patients, particularly those not treated for ADHD, were more susceptible to COVID-19 infection than those without ADHD and those who received ADHD pharmacotherapy (Merzon et al., 2021). Similar results of increased risk for infection were also reported in untreated pediatric ADHD patients from Israel when compared with medically-treated children (Cohen et al., 2022), and in adult ADHD patients in the US when compared with those without a diagnosed mental disorder (adjusted OR = 5.82, 95% CI [5.46, 6.20], p < .001) (Wang et al., 2021). In a subsequent study (1,870 COVID patients), Merzon et al. (2022) reported that ADHD was associated with more severe symptoms of COVID-19 (OR 1.81, 95% CI [1.29, 2.52], p < .05) and referral for hospitalization (OR 1.93, 95% CI [1.06, 3.51], p = .03). Liu, Tan, et al. (2021) also reported a modestly increased risk for hospitalization due to COVID-19 in genetically predicted ADHD. However, it was not clear if any potential confounders such as demographic and socioeconomic factors were accounted for in that study. ADHD patients who had stimulant treatment prescribed within the past year were found to have lower rates of healthcare encounter and mortality within 30 days of their COVID-19 infection compared to untreated patients (Tuan et al., 2022). No other studies have directly examined the impact of ADHD or any current ADHD medication status on COVID-19 severity. In a retrospective analysis of COVID-19 infection, mortality, and recovery rates at the US state level, Arbel et al. (2021) reported that COVID-19 recovery rates were positively associated with ADHD prevalence across states. They suggested the intriguing possibility that ADHD may provide an evolutionary advantage (Arbel et al., 2021), although this seems unlikely given genetic studies indicating that natural selection has acted against ADHD-associated alleles (Esteller-Cucala et al., 2020). Another study that examined the correlation between the prevalence of ADHD and COVID-19 infection and mortality rates at the global level from 156 countries found inconsistent results (Rajkumar, 2022).
Given the conflicting results from prior studies and the high prevalence of ADHD in the population, our study leveraged a large dataset collected from the TriNetX global COVID-19 Research Network during 2020 to determine whether there is a relationship between ADHD diagnosis and pharmacotherapy, and COVID-19 infection rates and severity of clinical outcomes.
Methods
TriNetX is a global research network of de-identified electronic medical record (EMR) data on diagnoses, laboratory and diagnostic tests and results, procedures, and treatments. Data is pooled from healthcare organizations (HCOs) in 19 countries. Our study used the TriNetX COVID-19 Research Network, which contains de-identified EMR data from over 100 million patients across 65 HCOs. Further information on TriNetX is provided in the Supplemental File. The present study included 1,124,774 patients diagnosed with COVID-19 between January 20, 2020 and December 31, 2020. The timeframe extended from the first case reported in the US to roughly the end of the US pre-vaccination period. Because the present study involved de-identified patient data, this study was exempted from institutional review.
Criteria for COVID-19 Cases
COVID-19 positive cases were identified by either a positive laboratory test or a COVID-19 diagnostic code (See Supplemental File) following the World Health Organization and Centers for Disease Control and Prevention (CDC) COVID-19 criteria and the TriNetX query guidelines. The study population was limited to patients over 10 years of age and those who had any type of healthcare encounter during the study period. The complete set of diagnostic codes included COVID-19 (U07.1 and U07.2), pneumonia due to COVID-19 (J12.82), other coronavirus as the cause of diseases classified elsewhere (B97.29), coronavirus infection, unspecified (B34.2), and personal history of COVID-19 (Z86.16), as well as positive antigen or antibody laboratory results, with the exclusion of other viral diseases (B25-B34). Acute COVID-19 positive cases were identified by removing a relatively small percentage of patients with only IgG+ or IgA+ results, or a history of COVID-19 (Z86.16), who lacked any other diagnostic code, positive antigen, or IgM+ specific laboratory results. COVID-19-negative cohorts were defined by the absence of any diagnostic or lab test codes (also excluding B25-B34).
ADHD Diagnostic Criteria
The ADHD cohort consisted of patients with the ICD-10 diagnostic category F90 and all subcategories. The non-ADHD cohorts consisted of patients without any of the above diagnostic codes.
Propensity Score-Matching
We used TriNetX’s propensity score matching (PSM) algorithm to control for socioeconomic factors, demographic characteristics (age, sex, race, and ethnicity), and medical (including psychiatric) conditions reported in the literature for association with risk of either COVID-19 infection or increased COVID-19 severity. The PSM algorithm identifies the best-matched subject from the larger cohort using “greedy nearest neighbor matching” with a caliper of 0.1 pooled standard deviations for each subject in the smaller cohort. The pooled matched cohorts were verified for their propensity scores and used in our comparative analysis.
The complete list of variables used in PSM is shown as results in Tables 1, 2, 4 and 5, and Supplemental Tables 2, 3, 4, and 5, including age (Fadl et al., 2021), hypertension and diabetes (Matsushita et al., 2020), thyroid disease (Hariyanto & Kurniawan, 2020), malignancy (Liang et al., 2020), obesity (Petrakis et al., 2020), lower respiratory diseases (Clark et al., 2020; Williamson et al., 2020); kidney failure (Clark et al., 2020), immune system disorders (Gao et al., 2021; Pablos et al., 2020; Zhong et al., 2020), enteritis and colitis (Rizzello et al., 2021), pulmonary embolism (Gao et al., 2021), tuberculosis (Sy et al., 2020) cerebrovascular disease (Li et al., 2020), metabolic syndrome (Costa et al., 2020), and certain blood types (Zietz et al., 2020).
Demographic Characteristics of COVID-19 Patients in ADHD and Non-ADHD Populations.

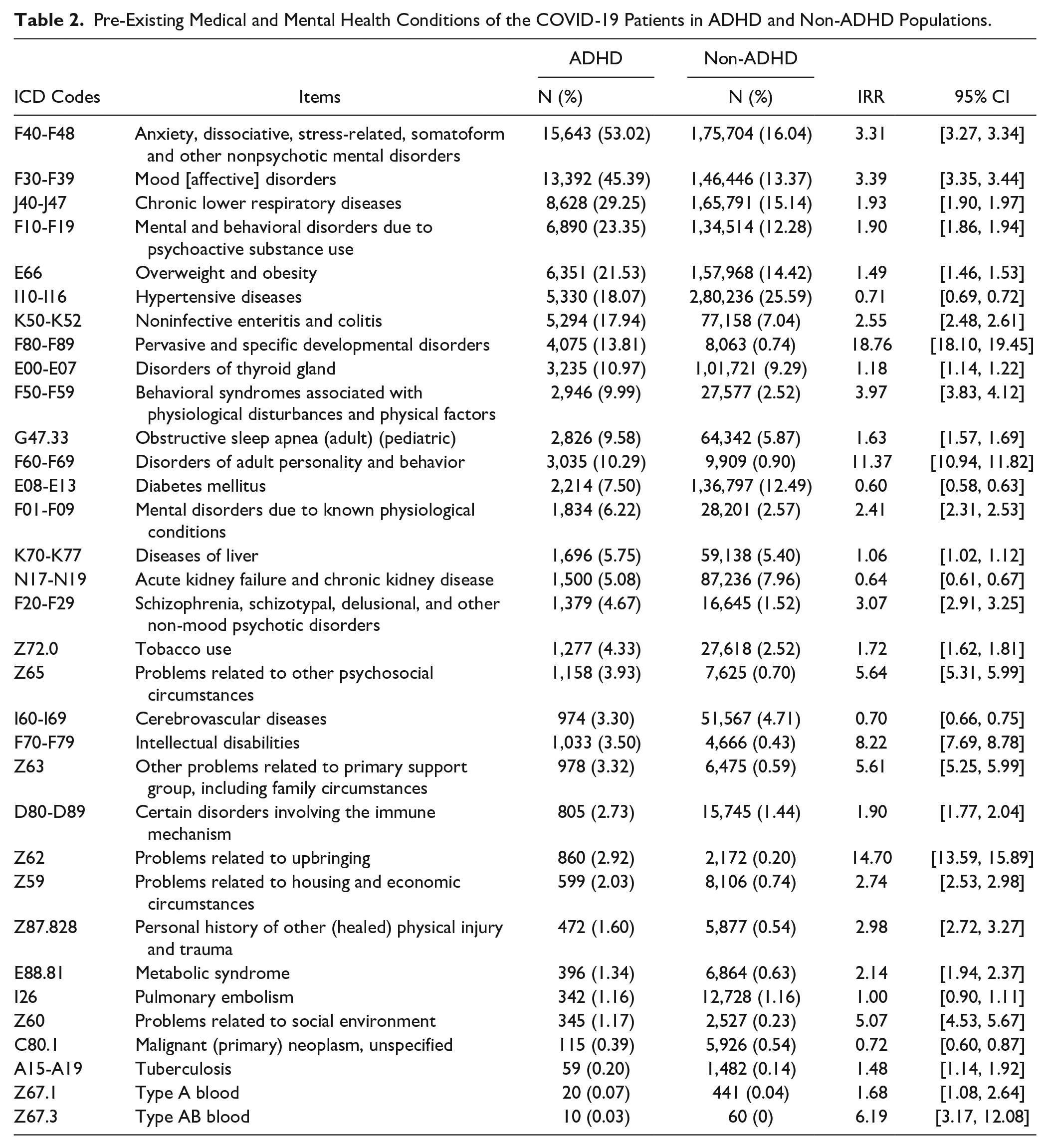
Pre-Existing Medical and Mental Health Conditions of the COVID-19 Patients in ADHD and Non-ADHD Populations.
ADHD and Risk for COVID-19 Infection
We assessed the overall rates of COVID-19 infection between the ADHD and non-ADHD cohorts, with separate analysis across five main race categories (Black or African American, American Indian or Alaska Native, Asian, Native Hawaiian, and white) and between male/female groups. We matched these groups for age and ethnicity (Hispanic, non-Hispanic, and unknown) and used a generalized linear model to determine whether COVID-19 infection rates were statistically different between ADHD and non-ADHD cohorts (both pre- and post-matching), and whether race and sex influenced the effect of ADHD on infection rates. We also examined the odds ratios (ORs) of COVID-19 infection rates between ADHD and non-ADHD cohorts across race and sex groups.
ADHD Diagnosis and COVID-19 Severity
To assess the association between ADHD diagnosis and COVID-19 severity, we established matched cohorts of COVID-19 patients with or without ADHD. We compared the following adverse outcomes between the cohorts within 60 days after COVID-19 infection: hospitalization, defined as any inpatient visit; mechanical ventilation (CPT codes: 39.65, 31500, 5A1935Z, 5A1945Z, 5A1955Z, 1015098, 0BH17EZ, 0BH13EZ, 0BH18EZ, and 1022227); and death. We repeated the outcome analysis separately for acute COVID-19 cases only, and for two age subgroups (10−30 and ≥30).
Analysis of ADHD Pharmacotherapy and COVID-19 Infection and Severity
To determine the relationship between ADHD pharmacotherapy and COVID-19 infection, we generated matched cohorts of ADHD patients who either had or had not received ADHD treatment. ADHD treatment was defined as prescription of either amphetamine (RXCUI code 725), dextroamphetamine (3288), methylphenidate (6901), clonidine (2599), guanfacine (40114), or atomoxetine (38400) during the study period, without receipt of any psychotherapeutic services (ICD-10 codes GZ5, GZ6, and CPT code 1021137) during the study period. Non-treated ADHD patients received neither pharmacotherapy nor any psychotherapeutic services during the same period. Cohorts matched for the complete set of demographics, medical, psychiatric, and socioeconomic factors were compared for COVID-19 infection rates.
We examined COVID-19 severity in ADHD patients who received any of the above pharmacotherapy without psychotherapy within two months prior to COVID-19 infection, and in ADHD patients who did not receive pharmacotherapy or psychotherapy within that 2 month period. Treated and untreated cohorts were matched for demographic, medical, psychiatric, and social factors.
We compared matched cohorts for rates of hospitalization, mechanical ventilation, and death within 60 days following COVID-19 infection. This was repeated separately for acute COVID-19 cases only.
Statistical and Sensitivity Analysis
We used risk ratios (RR) to measure the association between ADHD and rates of COVID-19 infection and severe outcomes. To determine if our results are unique to ADHD and COVID-19, we repeated the above analysis for two other common psychiatric disorders, major depressive disorder (MDD) and autism spectrum disorder (ASD), as well as the influenza virus. MDD was chosen to represent a common psychiatric disorder in adulthood, and ASD was chosen to represent a childhood-onset developmental disorder. Influenza was chosen to represent a common upper respiratory viral infection. PSM with the full list of risk factors was used to create matched cohorts in these analyses. In the cases of MDD and ASD, ADHD was included in the PSM-matching list to replace MDD or ASD.
Results
ADHD Diagnosis and COVID-19 Infection
1,124,774 patients had a history of COVID-19 during the study period. Of these, 29,502 had a lifetime diagnosis of ADHD, and 1,095,272 never had a diagnosis of ADHD. After PSM, the overall COVID-19 infection rate was 8.2% in all ADHD patients. This rate was significantly higher than the 7.4% in non-ADHD patients (RR 1.12, 95% CI [1.09, 1.12] p < .0001).
COVID-19 patients with ADHD were younger (29.6 ± 15.1) than those without ADHD (45.4 ± 19.6). The significant difference was consistent for all race and sex subgroups (ADHD effect F(1,18) = 144.94, p < .0001, Supplemental Table 1). We found no significant differences between sexes or across races. The proportion of Hispanic patients did not differ between ADHD and non-ADHD groups or between sexes. The proportion endorsing unknown ethnicity was significantly lower in the non-ADHD groups than in ADHD groups (chi2(1) = 25.33, p < .0001) and differed across races (chi2(4) = 96.7, p < .0001), with a significant interaction between race and ADHD status (chi2(4) = 19.9, p = .0005) and a non-significant effect of sex.
Due to these significant differences in age and ethnicity, we used the PSM algorithm to generate matched non-ADHD cohorts with age and ethnicity profiles similar to those of the ADHD cohorts in each race and sex subgroup. COVID-19 infection rates were significantly higher in all ADHD cohorts compared to both pre- and post-matched non-ADHD cohorts for all race and sex subgroups (pre-matched chi2(1) = 35.4 and post-matched chi2(1) = 50.3, both p < .0001, Supplemental Table 1 and Figure 1A). Females had significantly higher COVID-19 infection rates than males (sex effect pre-matched chi2(1) = 10.5, p = .001 and post-matched chi2(1) = 16.3, p = .0001). For ADHD cohorts, infection rates were similar across all races. For non-ADHD cohorts, however, both Asian males and females had significantly lower infection rates (pre-matched race effects chi2(4) = 125.4, and post-matched chi2(4) = 33.5, both p < .0001).
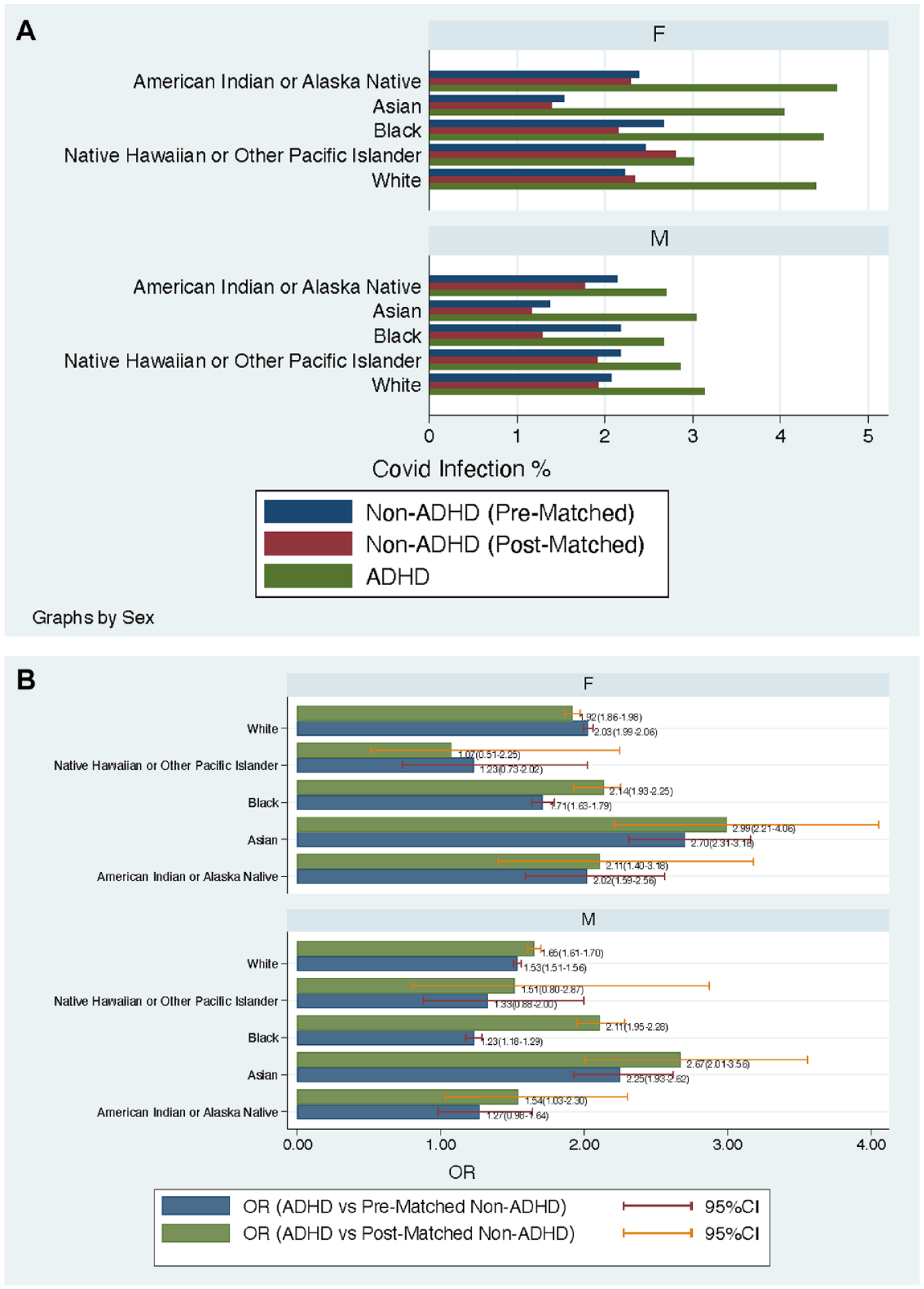
(A) COVID-19 infection rates between ADHD and non-ADHD cohorts in different race and sex subgroups. Non-ADHD groups were further matched to the ADHD groups for age using propensity score matching algorithm in TriNetX. Infection rates in both pre-matched and post-matched non-ADHD groups were lower than those of ADHD groups. (B) Odds ratios (OR) COVID-19 infection rates between ADHD versus non-ADHD groups (pre- and post-matched) are plotted for different race and sex groups, with 95% confidence intervals (CI) shown.
The odds ratios (ORs) comparing ADHD and non-ADHD patients were significantly above one for all race and sex groups except the Native Hawaiian/Other Pacific Islander group, likely due to its small sample size (Figure 1B). Significantly higher ORs were observed for females than males (chi2(1) = 5.97, p = .02), and for post-matched than pre-matched comparisons (chi2(1) = 4.4, p = .04). ORs were significantly different across races (chi2(4) = 59.2, p < .001): Asian patients had the highest ORs, followed by Black patients of both sexes.
ADHD Diagnosis and COVID-19 Severity
In addition to being younger, COVID-19 patients with ADHD were significantly more likely to be male, white, and non-Hispanic than non-ADHD patients (Table 1). ADHD patients had more comorbidities including anxiety disorders, mood disorders, chronic lower respiratory disease, obesity, noninfective enteritis and colitis, schizophrenia, tobacco use, intellectual disability, and adverse family circumstances, but less hypertension, diabetes mellitus, acute and chronic kidney disease, cerebrovascular disease, and primary neoplasm (Table 2).
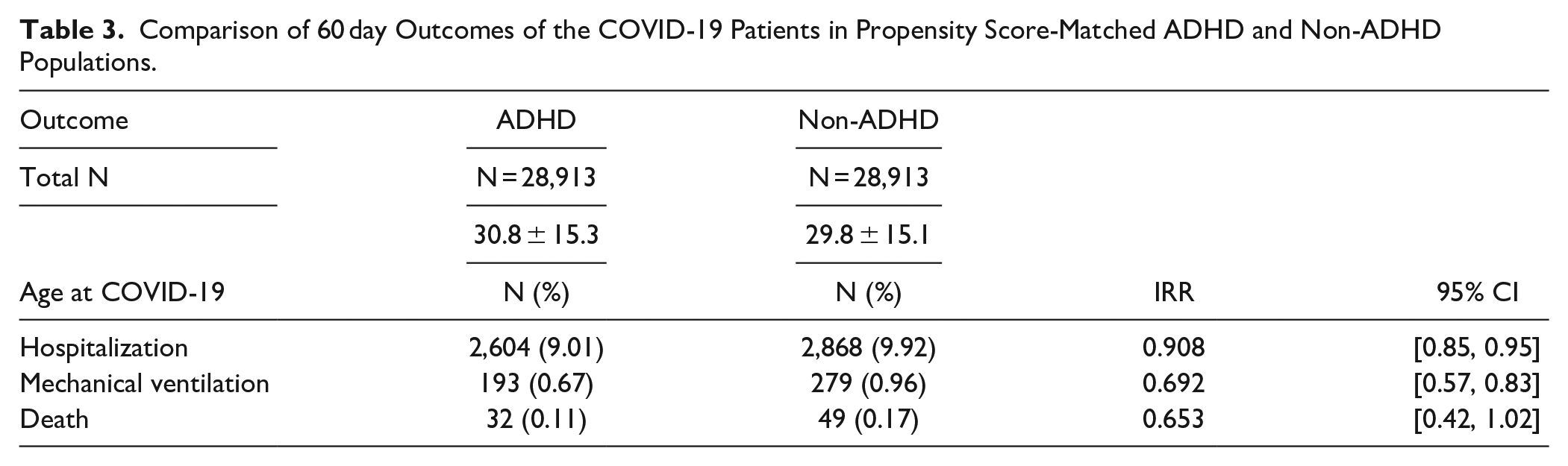
Full PSM resulted in 28,913 matched individuals in both the ADHD and non-ADHD groups, with similar compositions by age (29.8 ± 15.1 and 30.8 ± 15.3 for ADHD and non-ADHD cohorts, respectively), race, and ethnicity (Supplemental Table 2), as well as socioeconomic problems and preexisting psychiatric and medical conditions (Supplemental Table 3).
Comparing severe outcomes between matched cohorts during the 60 days following COVID-19 diagnosis, patients with ADHD had significantly lower rates of hospitalization (RR 0.91; 95% CI [0.85, 0.95]; p = .0002) and mechanical ventilation (RR 0.69; 95% CI [0.57, 0.83]; p < .0001) compared to those without ADHD. Death rates were also lower, but the difference was not statistically significant (RR 0.65; 95% CI [0.42, 1.02]; p = .06, Table 3). Limiting the analysis to acute infections removed COVID-19 patients with only IgG+ or IgA+ results or a personal history of COVID-19 (2.1% of the total). The results for all three outcomes were more significant (hospitalization RR: 0.86, 95% CI [0.83, 0.90]; mechanical ventilation RR: 0.60, 95% CI [0.51, 0.70]; and death RR: 0.57, 95% CI [0.44, 0.73]; all p < .0001).
Comparison of 60 day Outcomes of the COVID-19 Patients in Propensity Score-Matched ADHD and Non-ADHD Populations.
A separate analysis of younger (<30) and older (≥30) populations showed that the significant reduction in hospitalization and mechanical ventilation rates due to ADHD remained for the older group, but was not significant for the younger group (Supplemental Figure 1).
ADHD Treatment and COVID-19 Infection Rate and Severity
Among ADHD patients, 186,290 received pharmacotherapy without psychotherapy for ADHD during the study period; 396,971 received no treatment. Analysis of fully post-matched cohorts showed that ADHD patients who had received pharmacologic treatment had a significantly higher infection rate (9.82%) than those who did not receive treatment (8.7%, RR 1.13; 95% CI [1.10, 1.15], p < .0001).
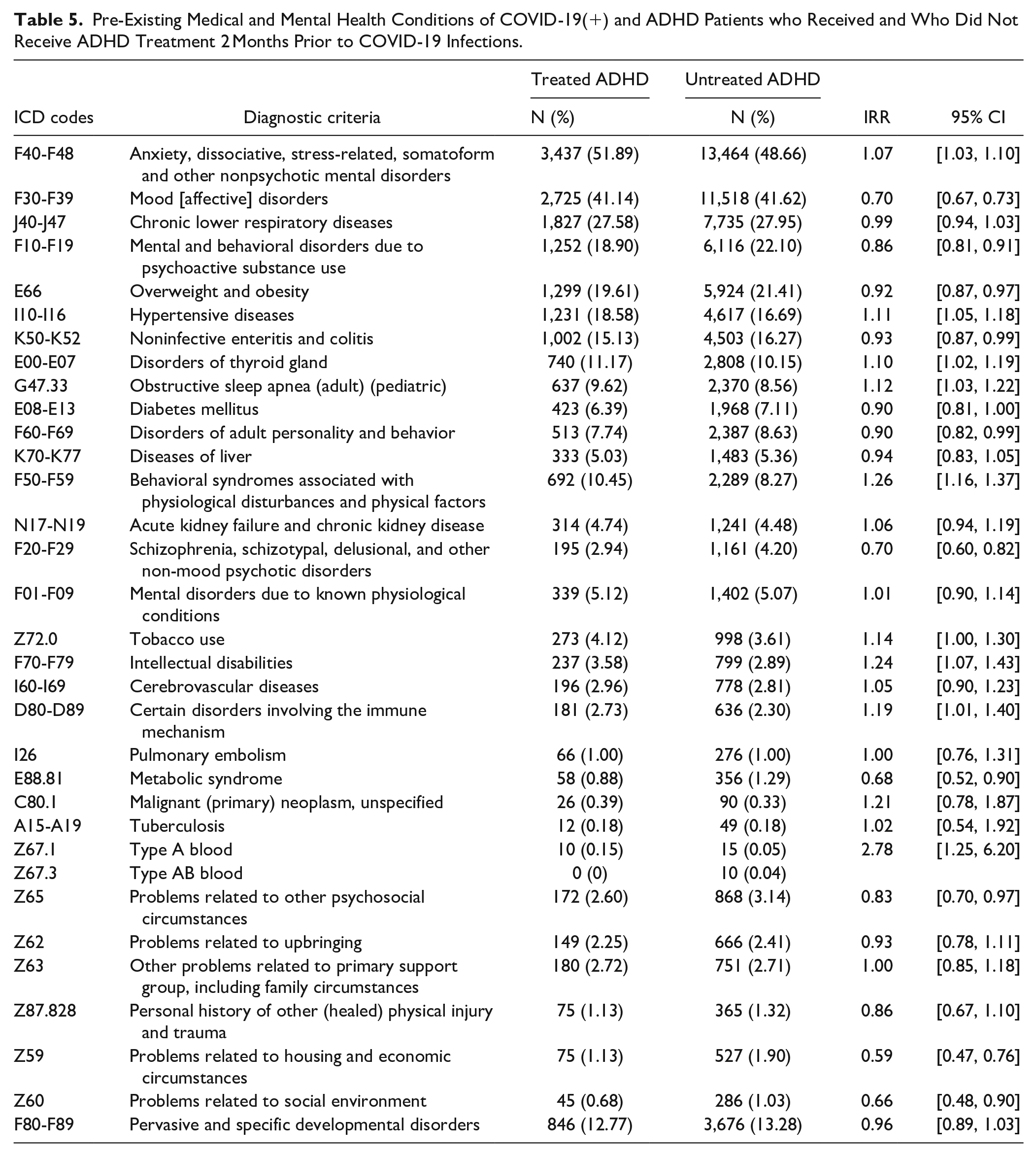
Among COVID-19 patients with ADHD, 6,624 received treatment within 2 months prior to infection, while 27,671 did not. The pre-matching demographic, socioeconomic, and medical profiles of treated- versus untreated COVID-19 patients with ADHD are listed in Tables 4 and 5. PSM produced matched cohorts with similar profiles (Supplemental Tables 4 and 5).
Demographic Characteristics of COVID-19(+) Patients With Treated and Untreated ADHD.

Pre-Existing Medical and Mental Health Conditions of COVID-19(+) and ADHD Patients who Received and Who Did Not Receive ADHD Treatment 2 Months Prior to COVID-19 Infections.
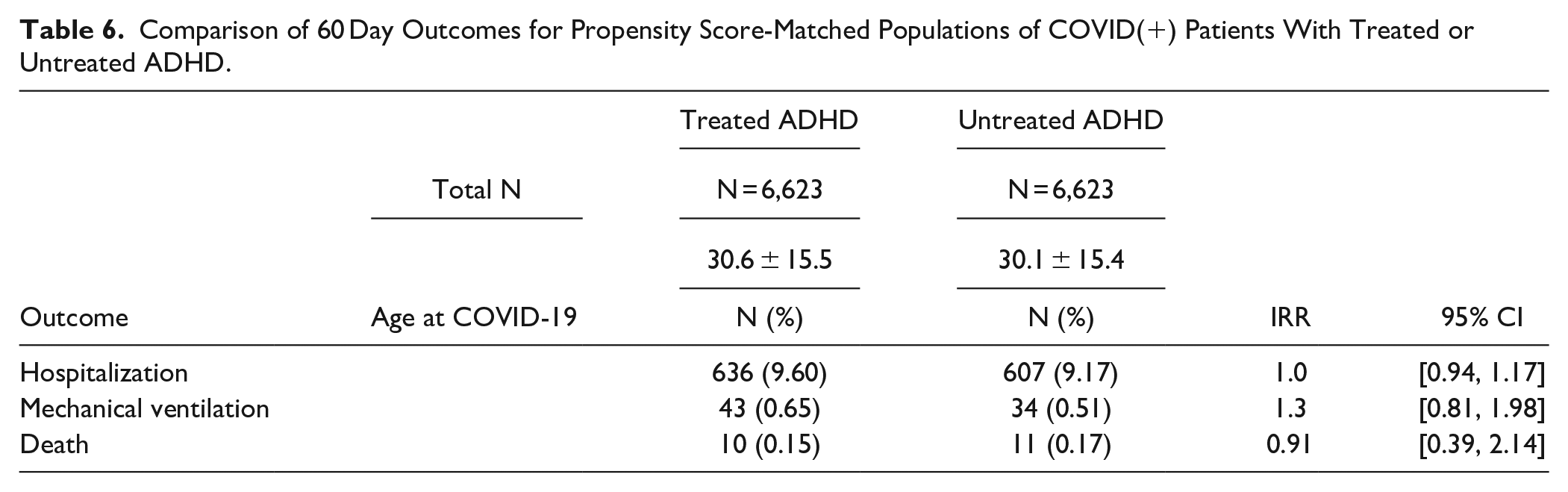
For the adverse outcomes within 60 days following COVID-19 infection, we found no significant association with recent ADHD treatment. After PSM, patients in the treated and untreated groups had similar rates of hospitalization (RR 1.05; 95% CI [0.94, 1.17]; p = .388), mechanical ventilation (RR 1.27; 95% CI [0.81, 1.98]; p = .304), and death (RR 0.91; 95% CI [0.39, 2.14]; p = .827) (Table 6). Limiting the analysis to only acute COVID-19 cases excluded 9.2% of the sample. After PSM, the results for adverse outcomes remained similar for mechanical ventilation (RR 1.23; 95% CI [0.79, 1.92]; p = .36) and death (RR 1; 95% CI [0.42, 2.40]; p = 1.00), but there was significantly greater risk for hospitalization (RR 1.14; 95% CI [1.02, 1.27]; p = .017).
Comparison of 60 Day Outcomes for Propensity Score-Matched Populations of COVID(+) Patients With Treated or Untreated ADHD.
Comparative Analysis: MDD
A total of 180,535 patients with COVID-19 had diagnosed MDD. Compared to fully matched non-MDD patients, MDD patients had a significantly higher infection rate (10.14% vs. 7.06%; RR 1.44, 95% CI [1.43, 1.4], p < .0001). Within 60 days following COVID-19 infection, they also had a significantly increased hospitalization rate (RR 1.15, 95% CI [1.13, 1.17], p < .0001) but decreased death rate (RR 0.74, 95% CI [0.68, 0.80], p < .0001), with no difference in mechanical ventilation (RR 1.01, 95% CI [0.96, 1.07], p = .63) (Supplemental Table 6).
Comparative Analysis: ASD
A total of 4,200 patients with COVID-19 had diagnosed ASD. Compared to non-ASD patients with matched age and sex, ASD patients had a significantly lower infection rate (6.64% vs. 6.97%; RR 0.95, 95% CI [0.92, 0.99], p = .007). Compared to non-ASD COVID-19 patients fully matched for all variables, ASD patients also had a significantly increased hospitalization rate (11.2% vs. 8.52%, RR 1.31; 95% CI [1.15, 1.5]; p < .0001), but no significant differences for mechanical ventilation (RR 1.08; 95% CI [0.74, 1.59]; p = .69) or death (RR = 1.00; 95% CI [0.42, 2.4]; p = 1.00) within 60 days following COVID-19 infection (Supplemental Table 7).
Comparative Analysis: Influenza
22,783 patients with ADHD had influenza during the same study period. Compared to age and sex-matched non-ADHD patients, ADHD patients had a significantly higher rate of influenza infection (2.49% vs. 1.92%; RR 1.30; CI [1.26, 1.33]; p < .0001). Compared to non-ADHD influenza patients fully-matched for all variables, ADHD patients had significantly decreased rates of all three adverse outcomes, including hospitalization (RR 0.80; CI [0.77, 0.84]; p < .0001), mechanical ventilation (RR 0.77; CI [0.67, 0.88]; p = .0008), and death (RR 0.42; CI [0.30, 0.58]; p < .0001) within 60 days of influenza diagnosis (Supplemental Table 8). After full PSM, ADHD patients treated for ADHD during the study period had a significantly increased rate of influenza infection (2.4%) compared to untreated patients (2.3%) (RR 1.06; 95% CI [1.02, 1.11]; p = .0031). After full PSM, receipt of ADHD treatment within 2 months prior to influenza diagnosis had no significant effect on rate of hospitalization (RR 1.01; 95% CI [0.92, 1.12]; p = .803), death (RR 1.08; 95% CI [0.50, 2.37]; p = .841), or mechanical ventilation (RR = 0.99; 95% CI [0.74, 1.32]; p = .940) (Supplemental Table 9).
Discussion
Our study sought to assess the relationship between the likelihood and severity of COVID-19 infection, and ADHD diagnostic status and pharmacotherapy. We used a large confederated EMR of COVID-19 patients from multiple global HCOs and a comprehensive PSM algorithm to control for potential confounding demographic and socioeconomic variables and preexisting psychiatric and medical conditions. We observed that, while ADHD patients had a significantly elevated risk for contracting COVID-19, after infection they had significantly lower rates of hospitalization and mechanical ventilation than non-ADHD patients. Recent pharmacotherapy for ADHD, surprisingly, was associated with significantly higher rate of COVID-19 infection. These effects of ADHD status and treatment appeared to be non-specific to COVID-19, as similar patterns were observed for influenza. However, the effects appeared to be unique to ADHD, since parallel analyses of MDD and ASD yielded different patterns. Notably, our findings could not be accounted for by age, sex, race, ethnicity, or comorbid conditions associated with ADHD.
Our study replicated prior findings (Cohen et al., 2022; Merzon et al., 2021; Wang et al., 2021) that ADHD diagnosis is associated with increased rate of COVID-19 infection. Our results also replicated the previously-reported disparity of COVID-19 rates in men and women with ADHD, and the increased infection rate in patients with depression (Wang et al., 2021). However, Merzon’s et al. (2021) study reported a nonsignificant association between COVID-19 infection and depression/anxiety.
Our results for COVID-19 outcomes differ from a previous report that among those with COVID-19, ADHD is associated with increased hospitalization rates (Merzon et al., 2022). Compared to our study, Merzon’s study had a smaller sample size and accounted for fewer potential confounding variables and comorbidities. Our additional analysis, which used the same set of confounding variables as those in Merzon’s study, did not markedly change our results based on full-spectrum PSM (results not shown). Thus, the discrepancy is likely due to other factors. One potential factor is age, which has a known significant effect on COVID-19 severity. Merzon et al. (2021) used a relatively younger cohort of COVID-19 patients (mean age 29.03; SD:14.8), whereas our cohort had a mean age of 45.0 (SD: 19.6). The ADHD patients in our cohort were on average 15.8 years younger than those without ADHD (29.6 vs. 45.4). The ages of ADHD and non-ADHD patients were not reported separately in Merzon’s study, although their stratified analysis by age replicated their significant finding of increased referral for hospitalization due to ADHD in adult patients (ages 20−40, 40−60), but not patients under 20. Notably, the number of patients in these subgroups was extremely small (17−111). On the contrary, our results showed that the association of ADHD with less-severe COVID-19 outcomes was only significant for the older group (≥30). In the younger group (<30), the effects were not significant and, consistent with Merzon et al., there was a reversed trend, where ADHD was associated with a lower rate of hospitalization (Supplemental Figure 1).
Unlike ADHD, MDD and ASD were associated with increased rate of hospitalization. Wang et al. (2021) also reported higher hospitalization rates for COVID-19 patients with depression than those without a mental disorder diagnosis. Merzon et al. (2022), however, reported a nonsignificant association with depression. Altogether, these findings suggest that mental disorders have different relationships with COVID-19, perhaps due to variation in behavioral and biological characteristics.
In contrast to prior reports, we found a significantly higher COVID-19 infection rate in ADHD patients treated with pharmacotherapy within 2 months than in untreated patients. In addition to different demographics and healthcare systems, as well as smaller sample sizes in the Israeli studies (Cohen et al., 2022; Merzon et al., 2021), the extent of prior or comorbid medical or psychiatric conditions, as well as demographic and psychosocial confounders unaccounted-for in the earlier studies, may contribute to the discrepancies. In addition, prior studies have examined the relationship between history of ADHD pharmacotherapy in the past year and COVID-19 infections or clinical outcomes (Cohen et al., 2022; Merzon et al., 2021). None had examined the impact of the most recent treatments.
Nevertheless, our results should be viewed cautiously due to potential confounders. It is possible that recently-treated ADHD patients in our sample represent more severe ADHD cases (Banaschewski et al., 2017); severe ADHD symptoms pose increased risk for contracting COVID-19 (Pollak et al., 2022). Furthermore, currently treated ADHD patients may have more access to healthcare providers and COVID-19 tests, and were thus more likely to be tested. Indeed, treated ADHD patients in our cohort reported slightly but significantly more average COVID-19 tests than untreated patients (2.2 vs. 2.05 tests during the study period, t = 5.56, p < .0001). Health insurance status may affect how patients seek treatment and COVID-19 testing. However, we do not have sufficient data on insurance status and could not control for this variable in the present study. Nevertheless, all our cohorts were generated with an index event that required a healthcare encounter within the study period. Future studies accounting for insurance status are needed to clarify the impact of health insurance on clinical outcomes.
With these potential confounders as caveats, it is worth considering biological mechanisms that could explain the observed association between ADHD, ADHD pharmacotherapy, and COVID-19 infection and severity. Animal studies have suggested that methylphenidate treatment leads to oxidative stress (Martins et al., 2006; Schmitz et al., 2012), suppression of T-cells (Millichap, 1997), altered neuroinflammation, and blood-brain-barrier dysfunction (Coelho-Santos et al., 2018). Although speculative, we cannot exclude the possibility that pharmacotherapy for ADHD may interact with already-elevated inflammation in ADHD (Instanes et al., 2018; Zhou et al., 2017) and induce adverse biological changes in the host immune and antiviral systems.
Given the role of dopamine in ADHD treatment (Faraone, 2018), another biological interpretation involves Dopa decarboxylase (DDC), the enzyme that catalyzes dopamine, serotonin, and histamine biosynthesis. DDC co-expresses with Angiotensin I Converting Enzyme 2 (ACE2), the gene which encodes the main receptor for SARS-CoV2, SARS-CoV, and MERS-CoV (Nataf, 2020). DDC suppresses flavivirus replication when overexpressed, and viral replication has been shown to decrease DDC mRNA levels (Frakolaki et al., 2019). DDC expression was substantially higher in COVID-19 patients, and the viral load in COVID+ nasopharyngeal swab samples was positively associated with ACE2 expression and negatively correlated with DDC expression (Mpekoulis et al., 2021). The expression response of DDC and ACE2 in nasopharyngeal tissue may be part of the orchestrated antiviral response and suggests a possible role for the dopamine and serotonin pathways in COVID-19 pathophysiology (Attademo & Bernardini, 2021).
Another potential mechanism involves 14-3-3 proteins, a family of small signaling molecules with a broad range of cellular functions (Aghazadeh & Papadopoulos, 2016; Kleppe et al., 2011; Obsilová et al., 2008). Genetic variants of the gene YWHA, encoding for the 14-3-3 protein, have been associated with ADHD (Jacobsen et al., 2015). Interestingly, 14-3-3 proteins interact with RNA viruses, including HCV, HIV, and Zika virus (Nathan & Lal, 2020). Recent work shows that SARS-CoV-2 nucleocapsid protein binds to 14-3-3 in a phosphorylation-dependent manner and that the sequestration by 14-3-3 is a cellular response for the control and inhibition of replication, transcription, and packaging of the SARS-CoV-2 genome (Tung & Limtung, 2020).
Our study has some limitations. Although we used a large, rich, real-world dataset, and controlled extensively for confounding variables, unaccounted-for confounders may remain. Our analysis also lacked patient stratification based on COVID-19 or ADHD severity; such stratification could have provided a more nuanced examination of outcomes.
Despite these limitations, our findings definitively confirm previous reports that ADHD is associated with increased risk for COVID-19 infection. Our results also suggest there could be a protective effect associated with ADHD status that reduces the need for hospitalization and ventilation in COVID-19 patients. As we observed similar protective effects of ADHD against influenza, future studies should explore the biological mechanisms underlying these relationships, which may offer potential therapeutic targets for viral infections.
Supplemental Material
sj-docx-1-jad-10.1177_10870547221129305 – Supplemental material for Association Between ADHD and COVID-19 Infection and Clinical Outcomes: A Retrospective Cohort Study From Electronic Medical Records
Supplemental material, sj-docx-1-jad-10.1177_10870547221129305 for Association Between ADHD and COVID-19 Infection and Clinical Outcomes: A Retrospective Cohort Study From Electronic Medical Records by Kathleen P. Heslin, Aminat Haruna, Regina A. George, Shiyu Chen, Ishak Nobel, Kathryn B. Anderson, Stephen V. Faraone and Yanli Zhang-James in Journal of Attention Disorders
Supplemental Material
sj-tiff-2-jad-10.1177_10870547221129305 – Supplemental material for Association Between ADHD and COVID-19 Infection and Clinical Outcomes: A Retrospective Cohort Study From Electronic Medical Records
Supplemental material, sj-tiff-2-jad-10.1177_10870547221129305 for Association Between ADHD and COVID-19 Infection and Clinical Outcomes: A Retrospective Cohort Study From Electronic Medical Records by Kathleen P. Heslin, Aminat Haruna, Regina A. George, Shiyu Chen, Ishak Nobel, Kathryn B. Anderson, Stephen V. Faraone and Yanli Zhang-James in Journal of Attention Disorders
Footnotes
Acknowledgements
Dr. Zhang-James is supported by the European Union’s Seventh Framework Program for research, technological development and demonstration under grant agreement no 602805 and the European Union’s Horizon 2020 research and innovation program under grant agreements No 667302.
Dr. Faraone’s research has received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement No. 667302 and 965381; NIMH grants U01MH109536-01, U01AR076092-01A1, R0MH116037 and 5R01AG06495502; Oregon Health and Science University, Otsuka Pharmaceuticals and Supernus Pharmaceutical Company.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Zhang-James, Dr. Anderson, Kathleen Heslin, Aminat Haruna, Regina A George, Shiyu Chen, Ishak Nobel declare no conflicts of interest.
In the past year, Dr. Faraone received income, potential income, travel expenses, continuing education support and/or research support from Aardvark, Akili, Genomind, Ironshore, KemPharm/Corium, Noven, Ondosis, Otsuka, Rhodes, Supernus, Takeda, Tris and Vallon. With his institution, he has US patent US20130217707 A1 for the use of sodium-hydrogen exchange inhibitors in the treatment of ADHD. He also receives royalties from books published by Guilford Press: Straight Talk about Your Child’s Mental Health; Oxford University Press: Schizophrenia: The Facts; and Elsevier: ADHD: Non-Pharmacologic Interventions. He is also Program Director of ![]() .
.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.