
Abstract
Despite inattention being one of the most common symptoms of Post-COVID-19 Syndrome (PCS), there is a gap in the literature regarding its treatment. This report presents a case of attentional symptoms and fatigue that emerged after the SARS-CoV-2 infection. The symptoms were similar to ADHD in adults, although the 61-year-old patient had never experienced inattention symptoms before. The patient was initially treated with Methylphenidate and then Lisdexamfetamine. Both were adapted to the needs and treatment response presented by the patient. After several changes in the therapeutic regimen, including the addition of Bupropion, the patient achieved remission of his symptoms. This case highlights the importance of treating PCS inattention and fatigue as an ADHD-like syndrome, despite the evident different etiology of symptoms. It would be necessary to replicate these findings to confirm our results, thus benefiting other patients currently affected by this syndrome.
Introduction
Post-COVID-19 Syndrome (PCS) or Long COVID refers to enduring sequelae after SARS-CoV-2 infection. It is defined as signs, symptoms, or abnormal clinical parameters affecting any organ or body system, persisting for more than 2 weeks after COVID-19 onset and not returning to a healthy baseline, irrespective of the viral status (Tenforde et al., 2020). Acute symptoms may persist, or new symptoms may appear, especially neuropsychiatric ones (Lopez-Leon et al., 2021). The prevalence of residual symptoms is 35% in outpatient settings, rising to 87% among patients hospitalized due to COVID-19 (Tenforde et al., 2020). PCS is common regardless of severity or hospitalization (Raveendran et al., 2021). The most common neuropsychiatric symptoms are fatigue (58%), headache (44%), and attention symptoms (27%). Memory loss is also common (16%) (Lopez-Leon et al., 2021). A recent meta-analysis suggested that the proportion of individuals experiencing symptoms of fatigue for 12 or more weeks was 32%, while 22% had cognitive impairment (Ceban et al., 2022).
The condition of cognitive sequelae after COVID-19 infection is also called “Brain Fog” in the neurological field, which represents a mental state including problems with language fluency, memory recall, inattention, executive functions, processing speed, and others (Becker et al., 2021; Kao & Frankland, 2022). These symptoms are comparable to those present in myalgic encephalomyelitis, chronic fatigue syndrome (ME/CFS), and mast cell activation syndrome (MCAS) (Theoharides et al., 2021). There is no recommended pharmacotherapy for Brain Fog, and treatment has focused on establishing individualized cognitive rehabilitation. Some case reports, such as the one by Warren et al. (2022), did not demonstrate clear benefits with the use of acetylcholinesterase inhibitor Donepezil.
Even though PCS is being increasingly recognized and researched, to the best of our knowledge, there is scarce description or guidance in the literature on how to treat attentional symptoms and fatigue in PCS. Therefore, we aim to describe for the first time in the literature the course and treatment of a patient with PCS displaying ADHD-like symptomatology.
Materials and Methods
The present investigation consists of a single case study. The patient was treated on an outpatient basis, being self-referred. The PCS treatment lasted 18 months, and the patient is still under care. Written informed consent was obtained from the patient for the publication of this case report and his magnetic resonance images. Brain Magnetic Resonance Imaging (MRI) was performed in a high magnetic field machine (3.0 Tesla), in the axial, sagittal, and coronal planes, in pondered T1, T2, FLAIR, gradient, and diffusion sequences, without gadolinium.In addition, blood tests related to the clinical condition were also undertaken. The case was described and discussed following the CARE guidelines for case reports (Riley et al., 2017), available in Supplementary Material.
Adult ADHD Self-Report Screening Scale (ASRS)
The ASRS is a self-report scale designed to screen potential cases of adult ADHD in the community. Developed by the World Health Organization (WHO), it consists of 18 questions asking the frequency of inattention, hyperactivity, and impulsivity symptoms listed in DSM-IV (Kessler et al., 2005). The severity of the symptoms over the prior 6 months is rated on a 5-point Likert-type scale (0–4 = never, rarely, sometimes, often, to very often), with the total score ranging from 0 to 72. A score above 24 is indicative of ADHD. Mattos et al. (2006) made a transcultural adaptation to Brazilian Portuguese, ensuring satisfactory equivalence between versions. The scale demonstrates high diagnostic accuracy, discriminating between clinical and control populations (AUC = 0.904, 95% CI: [0.888, 0.921]) (Brevik et al., 2020). The patient’s symptoms were measured on five occasions to monitor treatment response: pre-treatment, during methylphenidate use, after methylphenidate interruption, after lisdexamfetamine use, and during bupropion use, as depicted in Figure 1.
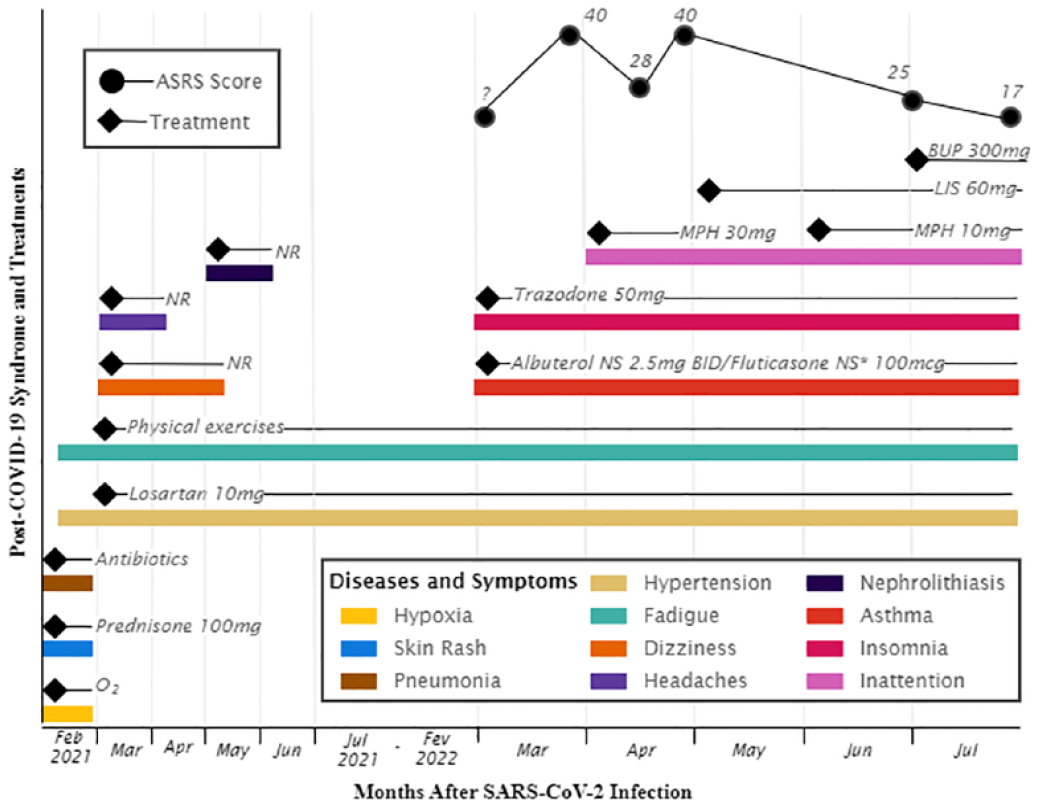
Chronology of PCS and its symptoms, treatments employed, and ASRS scores during and after SARS-CoV-2 infection in the 61-years-old patient.
Results
Case Report
A previously healthy 61-year-old man, white European-Brazilian descendent, married, college professor, 80 kg, 177 cm (BMI = 25.5 kg/m2), had an episode of COVID-19 in February 2021. On the ninth day, he developed a severe skin rash, and on the 10th day, his oxygen saturation dropped below 90%. He was then admitted to the hospital with a high fever, pneumonia, and only 50% lung function. He received antibiotics that effectively resolved the pulmonary infection, prednisone up to 100 mg/day, and oxygen without needing intubation. Hospitalization lasted for 15 days, after which he was released with high blood pressure (treated with losartan 10 mg/day until today) and fatigue. Prednisone was soon discontinued, and physical exercises were prescribed to recover muscle mass, lung function, and intense fatigue. He developed some other conditions commonly linked to PCS, such as headaches (the first month after leaving the hospital), dizziness (first 2 months), and nephrolithiasis (the third month, not usually linked to the syndrome) (Lopez-Leon et al., 2021). By the fourth month, his lung function had improved to 70%. Asthma emerged in March 2022 (13 months later), and it is still being treated with Albuterol nebulizer solution 2.5 mg BID and Fluticasone Intranasal 110 µg once a day. Insomnia also appeared in March 2022, leading the patient to seek psychiatric evaluation for the first time. Trazodone 50 mg/day was prescribed with good response and continues to be used until now.
Attention difficulties and memory loss appeared later (April 2022), gradually increasing over a few weeks, even though the patient had never had symptoms of ADHD and carried a healthy lifestyle before COVID-19. The patient began to show symptoms similar to ADHD in adults, such as often forgetting everyday things like taking current medicines, losing personal belongings, leaving the garage door open when leaving or entering the house, as well as forgetting professional commitments. In addition, difficulties with reading, planning, and monitoring his actions were reported. The ADHD-like symptoms were severe, causing difficulties in performing everyday personal and professional tasks. Hyperactivity or impulsivity symptoms were not clinically significant. So, the best phenomenological description of the case would be a predominantly inattentive ADHD-like presentation due to Post-COVID-19 Syndrome. It should be noted that there were neither current nor lifetime symptoms of Major Depression, Bipolar Disorder, or any Anxiety Disorder.
The ADHD-like symptoms were measured using the Adult ADHD Self-Report Screening Scale (ASRS), a gold-standard rating scale for ADHD in adults (Anbarasan et al., 2020). The patient’s ADHD-like symptoms scored 40 points on the ASRS scale a few weeks after the onset of the attentional symptoms. After this evaluation, we decided to treat him as an ADHD-like case. Although adult ADHD guidelines usually recommend long-acting medications for treating ADHD, the medicine chosen was Immediate-Release Methylphenidate (IR-MPH) because there were no concerns with adherence, abuse, rebound, driving, or multiple dosing (Kooij et al., 2010). Also, IR-MPH was easier to tailor to the patient’s needs, considering that it could be fractionated, initiating with shallow doses and gradually increasing. The intention was to change the medication to a long-acting preparation after dose adjustment.
IR-MPH was started with 5 mg/day and increased to 10 mg TID. IR-MPH initially effectively reduced ADHD-like symptoms to 28 points on the ASRS scale (30% reduction from baseline). It was also slightly effective on fatigue but soon ceased to work. Increasing the doses was not well tolerated due to insomnia. ASRS returned to baseline (40 points), and IR-MPH was switched to Lisdexamfetamine (LDX) 30 mg upon waking. Fatigue was fully treated with the use of this psychostimulant. The patient did not experience side effects with LDX, but ADHD-like symptoms remained unchanged after some weeks. We then doubled the LDX dose to 60 mg upon waking and soon to 70 mg.
The patient usually woke up at 5 AM and followed routines, such as taking his medications, reading the newspaper, making breakfast, getting ready and driving to work. All these behaviors were disturbed by inattention. The use of LDX in the morning—even with doses of 70 mg—improved these morning symptoms. However, it was not enough to cover all hours of the day. The patient complained of inattention during night hours, which before COVID-19, he used to do intellectual activities. As there was no difference in effectiveness between 60 or 70 mg of LDX and no 16-hr extended-release ADHD medication in Brazil, we chose to split LDX into two doses, initially 30 mg at 5 AM and 30 mg at 10 AM. Even with this scheme, the psychostimulant coverage was insufficient to encompass the whole day. So we add 10 mg of IR-MPH in the morning to fill in the remaining hours not yet covered by medication, thus avoiding insomnia caused by this psychostimulant and postponing the use of the two doses of LDX to 30 mg at 8 AM and 30 mg at 12 AM, getting, thus, complete coverage at all hours of the day. This scheme was used for 1 month resulting in a reduction to 25 points in ASRS (37,5% reduction from baseline).
The patient was still not fully recovered. New attempts to increase psychostimulant dose caused insomnia (IR-MPH) or were ineffective (LDX). Then, Bupropion XL was used up to 300 mg/day to improve the response further. After 5 weeks, a reduction to 17 from the baseline 40 ASRS points was obtained, representing a 57,5% reduction and remission of symptoms, since the cutoff of the scale is 24 points. The final combination of medications was IR-MPH 10 mg at 5 AM, LDX 30 mg at 8 and 12 AM, Bupropion XL 300 mg at 8 AM, and Trazodone 50 mg before bed to treat insomnia. This drug combination has remained well tolerated and effective since its implementation. The treatment was effective on ADHD-like symptoms, fatigue, memory loss, and insomnia. The only adverse effect of the final drug combination was a weight loss of 5 kg that did not disturb the patient. The chronology of PCS, treatments, and ASRS scores can be seen in Figure 1.
Brain Images
The brain MRI examination indicated hippocampi with normal morphology, thickness, and signal intensity. In addition, the sella turcica was found to be partially empty, indicating probable pituitary atrophy. Other cranioencephalic structures are without detectable alteration. Selected images are available under request.
Blood Tests
The blood tests only indicated high LDL and total cholesterol results, which are unrelated to the reported psychiatric problems. Concerning the other exams performed, particularly those related to pituitary function (TSH, FSH, LH, testosterone total, cortisol, SDHEA), results were within the expected range, suggesting adequate functioning despite the structural neuroimaging results. Table 1 contains the test results and references according to the patient sex and age.
Laboratory Tests Results with Reference Range for a Male, 61-years-old Patient.

Patient Perspective
“Despite being very weak, my first days out of the hospital were almost euphoric because I was alive. I had never heard about Post-COVID; maybe the term was not even coined at that time. I initially found that fatigue was the only symptom that did not improve. Later, a worrisome attention deficit suddenly appeared. The practical blunders I made bordered on the comical but were dangerous. For example, I forgot to take medication, or I took it twice or took it at another time. I felt insecure, I started to drive as little as possible for fear of causing an accident. Luckily and unexpectedly, the medication that was effective in the attention deficit also helped with the fatigue. Today I am much more like the person I used to be. On one occasion, I did not take my attention deficit medication and had a bad day due to oblivion. It is hard to see that attention deficit and fatigue worsen significantly without medication. I am afraid these medications are here to stay. But, Hallelujah! At least there are medications for this! Neurological symptoms frighten more than others and are also more difficult to resign. I am afraid that something new might still emerge, fear of early decline or neurological disease. I got back to driving safely, working almost as before. It is not exactly my life before, but I can be happy. I accompanied people in the hospital with greater suffering than mine, and many died. Not a few are left with disabling sequelae. I am living beyond expectation.”
Discussion
We evaluated and treated a patient with cognitive and behavioral symptoms arising after a SARS-CoV-2 infection that were consistent with PCS. The clinical picture was similar to a case of ADHD, although the 61-year-old patient had never had ADHD. The possibility of Mild Cognitive Impairment (MCI) causing the symptoms were excluded from the differential diagnosis for many reasons: (a) an unexpectedly fast and severe onset (around 30 days) of symptoms; (b) the emergence of attentional symptoms simultaneously with asthma, both linked to PCS and its inflammatory state; (c) and clinical response to psychostimulants, a class of medications not used to treat MCI; (d) neurological investigation with MRI of the brain indicated cranioencephalic structures without detectable change, but a probable pituitary atrophy. PCS was also relevant here because the late onset of cognitive deficits is not uncommon among patients with this condition. The risk for the onset of cognitive deficits, including attentional ones, remained present in a large sample up to 2 years after the SARS-CoV-2 infection (Taquet et al., 2022).
The ADHD-like condition was severe and impaired the patient’s performance in daily life. We considered him an ADHD-like case, trying to follow ADHD treatment guideline recommendations closely (Kooij et al., 2010). However, adaptations in medication choices were needed, considering the results obtained at each stage of the treatment plan. Using a patient-centered and needs-based approach, the treatment plan considered the patient’s demands at work and home, representing symptom control throughout all hours of the day and into the evening. At first, LDX was divided into two doses, combined with IR-MPH, to prolong the duration of medication coverage. Finally, Bupropion was successfully added to improve the response further. The result was tailored to the patient’s conditions and available medications. Combining different types of ADHD medications to obtain the best therapeutic result has been recommended as the ideal procedure in specific cases, such as the present one (Jain et al., 2017). Whether such complex treatments will be needed in other cases of PCS is a matter of further investigation.
By now, the literature concerning the pharmacological treatment of PCS is limited, despite neuropsychiatric sequelae being highly prevalent. The lack of evidence on how to treat PCS can hamper the decision-making process of clinicians. Conceiving and approaching the described case as a Post-COVID-19 ADHD-like Syndrome (PCAS), that is, as an ADHD phenocopy, allowed a good evolution of the treatment. This approach could be generalized to similar PCS conditions. Indeed, Manu (2022) has suggested the potential utility of Methylphenidate in PCS treatment, considering the usefulness of this drug in improving fatigue, attention, concentration, and memory. Methylphenidate has been shown to be effective in managing fatigue (Belloni et al., 2021) and working memory deficits (Pievsky & McGrath, 2018). In the presented case, fatigue and memory loss improved considerably with psychostimulant use. This should be highlighted because fatigue is the most common symptom of PCS (Lopez-Leon et al., 2021).
ADHD and PCS have different etiologies despite the similar symptom profile. The first is a neurodevelopmental disorder with onset in childhood and a chronic course (American Psychiatric Association, 2013). On the other hand, PCS seems to be related to inflammatory sequelae. Elevation in at least one measure of inflammation was usually reported in patients with Long COVID (Schou et al., 2021). The causal relationship between some pro-inflammatory cytokines, mood symptoms, and cognitive decline is well established (Sartori et al., 2012). COVID-19 patients suffer from a significant increase in cytokines, which is supposed to be the main factor in the pathogenesis of PCS (Schou et al., 2021). Therefore, neuropsychiatric symptoms of PCS may result from autoimmune brain lesions that accompany the chronic inflammatory state caused by the SARS-CoV-2 virus. Indeed, COVID-19 was associated with cortical atrophy in parahippocampal and orbitofrontal regions and cognitive dysfunction (Crunfli et al., 2022). However, the case report indicated only pituitary atrophy without cortical thickness atrophy or hippocampal lesions. Indeed, there are reports of post-COVID pituitary atrophy (Mirza et al., 2022). To further investigate this, blood tests of hormones produced or controlled by the pituitary gland were requested for the patient, such as TSH, FHS, and cortisol, all of which revealed no abnormalities. Besides, the patient did not present clinical alterations related to panhypopituitarism. Therefore, even with severe PCS, the patient did not exhibit neurological or physiological alterations that could explain the cognitive symptoms. In the same way that occurs with ADHD, not all adult patients affected might have identifiable structural brain changes (Hoogman et al., 2017, 2019). Regardless of the inflammatory causes, the treatment was effective in ameliorating the symptoms and functioning of this PCS case, as much as it does in adults with ADHD. Therefore, it might be more beneficial to treat the consequences of the inflammatory state in patients with PCS rather than the state itself.
The limitations of this work are inherent to a case study. It would be essential to replicate the findings in more patients with PCAS to confirm the effectiveness of treating PCS cognitive symptoms as ADHD-like. Also, the long-term evolution of PCAS is unknown and a subject for forthcoming studies. The emergence of COVID-19 and PCS, featuring a multitude of symptoms and the lack of clear pharmacotherapy guidelines, have posed new challenges for clinicians. Advances in the evidence-based treatment for PCS would be an important gain for affected individuals. Neurological approaches considering these symptoms as a Brain Fog comparable to myalgic encephalomyelitis, chronic fatigue syndrome (ME/CFS), or mast cell activation syndrome (MCAS) (Theoharides et al., 2021) used lifestyle changes and acetylcholinesterase inhibitors as treatments, but with poor results (Warren et al., 2022). In this case report, we demonstrate a clear and consistent benefit in choosing and treating PCS (and Brain Fog) as an ADHD-like case. This approach and improvement could be extended to other patients affected by this syndrome.
Future directions include replicating, in randomized controlled trials, the treatment effect of stimulants in Post-COVID ADHD-like Syndrome. Also, the biological mechanism underlying cognitive disturbances after COVID-19 infection should be better elucidated to enable the tailoring of interventions. Finally, the persistence and course of PCS symptoms throughout time should be monitored to identify changing patterns.
Supplemental Material
sj-docx-1-jad-10.1177_10870547231168338 – Supplemental material for Successful Treatment of Post-COVID-19 ADHD-like Syndrome: A Case Report
Supplemental material, sj-docx-1-jad-10.1177_10870547231168338 for Successful Treatment of Post-COVID-19 ADHD-like Syndrome: A Case Report by Marcelo Moraes Victor, Letícia Müller Haas, Eugenio Horácio Grevet and Luís Augusto Rohde in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EHG was on the speaker's bureau for Shire for the last three years. LAR has received grant or research support from, served as a consultant to, and served on the speakers' bureau of Abbott, Aché, Bial, Medice, Novartis/Sandoz, Pfizer/Upjohn, and Shire/Takeda in the last 3 years. The ADHD and Juvenile Bipolar Disorder Outpatient Programs chaired by Dr Rohde have received unrestricted educational and research support from the following pharmaceutical companies in the last 3 years: Novartis/Sandoz and Shire/Takeda. Dr Rohde has received authorship royalties from Oxford Press and ArtMed. MMV and LMH declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.