
Abstract
Objective:
To investigate patterns and trends of co-prescriptions of stimulants and sedatives within the last 6 years at a tertiary care center.
Method:
Patients 18 years of age and older who were dispensed at least one stimulant prescription from an institutional pharmacy between 1/1/2015 and 7/1/2021 were included. Prescription data for any co-prescribed sedative/hypnotic were collected.
Results:
Both the number of stimulant dispenses and the number of patients with stimulant dispenses increased significantly with yearly incidence rate ratios of 1.115 (95% CI [1.110, 1.119]) and 1.090 (95% CI [1.084, 1.096]), respectively. The number of patients with a stimulant dispensed who also had a benzodiazepine or “Z-drug” sedative-hypnotic dispensed at any point in the search timeframe increased significantly with incidence rate ratios of 1.077 and 1.092, respectively. The number of stimulant dispenses, number of patients with stimulant dispenses, and number of patients with a stimulant dispensed who also had both a benzodiazepine and Z-drug dispensed at any point in the search timeframe increased significantly more in Non-White than in White patients.
Conclusions:
The results confirm previous findings of increases in dispensing of stimulants over the past 6 years and report increased polypharmacy of stimulants and sedative-hypnotics.
Introduction
Stimulant prescribing has increased significantly over the past several years, especially among females and adults aged 20 years and older (Board et al., 2020; Brumbaugh et al., 2022; Moustafa et al., 2022; Paiva et al., 2023). Total stimulant prescription sales to adults have surpassed those to children (Safer, 2016). This increase in stimulant prescribing in adults is likely linked to an increase in the diagnosis of Adult ADHD (Oehrlein et al., 2016; Zhu et al., 2018), the recent FDA approval of lisdexamfetamine for treatment of binge eating disorder (Bello & Yeomans, 2017), and an increase in off-label prescribing for indications such as weight loss, fatigue, cognitive enhancement, and depression (Caldwell, 2001; Jeffers & Benotsch, 2014; Sharif et al., 2021).
At the same time, the prescription rates of sedative-hypnotics are increasing (Kaufmann, Spira, Alexander, et al., 2016), coinciding temporally with an increase in overdose mortality involving benzodiazepines among US adults (Bachhuber et al., 2016). Benzodiazepines have high potential for abuse, addiction, physical dependence, and withdrawal reactions, leading to concerns regarding rising prescription rates (Hirschtritt et al., 2021). Indications for benzodiazepines include anxiety disorders, insomnia, agitation, seizures, muscle spasms, and alcohol withdrawal (Olkkola & Ahonen, 2008). For patients with sleep disorders, non-benzodiazepine receptor agonists, also known as Z-drugs, have been prescribed increasingly more often in place of benzodiazepines (Kaufmann, Spira, Alexander, et al., 2016).
There are no studies to our knowledge that investigated the co-prescription of a broad spectrum of stimulants with a broad spectrum of sedative-hypnotics. Furthermore, we found no studies on the co-prescription of stimulants and Z-drugs. Although they have different and sometimes co-existing clinical indications, co-prescribing stimulants with sedatives is counterintuitive due to the opposing nature of their pharmacodynamics. Consistent with their known clinical effects, dextroamphetamine has been shown to enhance cognitive performance on a computerized task whereas alprazolam impaired performance in the same experiment (Mills et al., 2001). However, additional data suggest that potential interactions between stimulants and sedatives are not straightforward. For example, among patients taking sedative medications, those given amphetamine performed significantly worse on a psychomotor vigilance task evaluating sustained attention compared to subjects not given amphetamine (Mills et al., 2001). Furthermore, apparent competition does not apply equally to all effects of these drugs. A prospective study found that dextroamphetamine reversed the amnestic effects of triazolam to a lesser extent than the sedative effects (Mintzer & Griffiths, 2007). More worrisome are unrecognized effects that might lead to misuse or dangerous outcomes. A 2008 study demonstrated that pretreatment with alprazolam decreased dosage discrimination and self-reported effects of amphetamine in human subjects (Rush et al., 2004), creating a scenario in which higher doses may be self-administered to achieve desired effects, including therapeutic benefits or other psychoactive effects (e.g., euphoria). A Norwegian case-control study found that simultaneous use of an amphetamine and a benzodiazepine had the highest odds ratio for arrest for driving under the influence of drugs, higher than any single drug usage (Bogstrand & Gjerde, 2014). A Swedish study found that 46% of individuals suspected of driving under the influence of drugs who were found to have detectable blood levels of alprazolam also had detectable levels of amphetamine (Jones & Holmgren, 2013). This was the most frequently co-ingested substance in this sample, higher than ethanol. Despite these data, the only interaction with sedatives contained in the prescribing information for amphetamine/dextroamphetamine is that it may counteract the sedative effect of antihistamines (Adderall and Adderall XR (amphetamines) Information | FDA, n.d.). Although less is known about the potential interactions between Z-drugs and stimulants, similarly to benzodiazepines, Z-drugs and stimulants have opposing clinical effects, such that the co-prescription of these medications is an important area of investigation.
Previous studies found that stimulants and sedatives are increasingly co-prescribed (Zarkowski, 2020; Zarkowski et al., 2021), but there is little in the literature that has quantified the extent of this potential problem. Thus, this study aimed to investigate patterns and trends of co-prescriptions of stimulants and sedatives within the last 6 years at a large tertiary care center that also provides comprehensive primary care coverage.
Materials and Methods
The Institutional Review Board at our institution determined this retrospective review of prescription records from the pharmacy database and associated information from patients’ medical records to be exempt. The study cohort included patients 18 years of age and older who were dispensed at least one stimulant prescription from one of the institutional pharmacies of a single tertiary care center between 1/1/2015 and 7/1/2021. Patient demographics, Charlson comorbidity index, numbers of hospitalizations and ED visits within 1 year after first stimulant dispense, deaths within 1 year after first stimulant dispense, and history of mental disorders were abstracted from medical records. Prescription data for any co-prescribed sedative/hypnotic were also collected. Dates of all dispenses were collected. Patients who withheld use of their medical record to be used for research purposes, pursuant to Minnesota statute, were excluded. A single dispense was defined as one episode in which a drug was purchased at one of the institutional pharmacies.
Stimulants included: amphetamine, methamphetamine, dextroamphetamine, amphetamine-dextroamphetamine, methylphenidate, dexmethylphenidate, lisdexamfetamine, serdexmethylphenidate/dexmethylphenidate, modafinil, and armodafinil. The sedative/hypnotic class was limited to benzodiazepines and nonbenzodiazepine benzodiazepine receptor antagonist (hereinafter referred to as Z-drugs). Benzodiazepines included: alprazolam, clonazepam, diazepam, chlordiazepoxide, lorazepam, triazolam, clorazepate, oxazepam, temazepam, quazepam, and flurazepam. Z-drugs included: eszopiclone, zaleplon, and zolpidem.
The following data were plotted against time by calendar quarter from 1/1/2015 to 7/1/2021: total number of stimulant dispenses, number of unique patients who were dispensed a stimulant, number of patients with a stimulant dispensed who also had a benzodiazepine dispensed at any point in the study timeframe, number of patients with a stimulant dispensed who also had a benzodiazepine dispensed within 30 days before or after the stimulant, number of patients with a stimulant dispensed who also had a Z-drug dispensed at any point in the study timeframe, number of patients with a stimulant dispensed who also had a Z-drug dispensed within 30 days, number of patients with a stimulant dispensed who also had both a benzodiazepine and a Z-drug dispensed at any point in the study timeframe, and number of patients with a stimulant dispensed who also had both a benzodiazepine and a Z-drug dispensed within 30 days. Poisson regression was used to assess for trends in dispensing over time. Associations are summarized using incidence rate ratios (IRR) and 95% confidence intervals (CI). Average number of stimulant dispenses per patient per year was graphed in a box plot and linear regression was used to assess for annual changes in stimulants dispenses/patient/year over the time frame of the study. Similar analyses were conducted on other the other dispensing trends. The aforementioned analyses were also stratified by race in terms of White versus Non-White patients. Statistical analyses were performed using SAS version 9.4 software (SAS Institute, Inc.; Cary, NC) and R version 4.0.3 (R Core Team, R Foundation for Statistical Computing, Vienna, Austria).
Results
Demographics of all patients who were prescribed a stimulant in our search timeframe are tabulated in Table 1. The median age at which a stimulant was dispensed was 35 (interquartile range [IQR] 25, 49) years. Most patients (57.6%) were female. The most common psychiatric diagnosis was ADHD (52.8%). The majority of patients were White (87.3%).
Demographic and Clinical Data for Study Cohort.
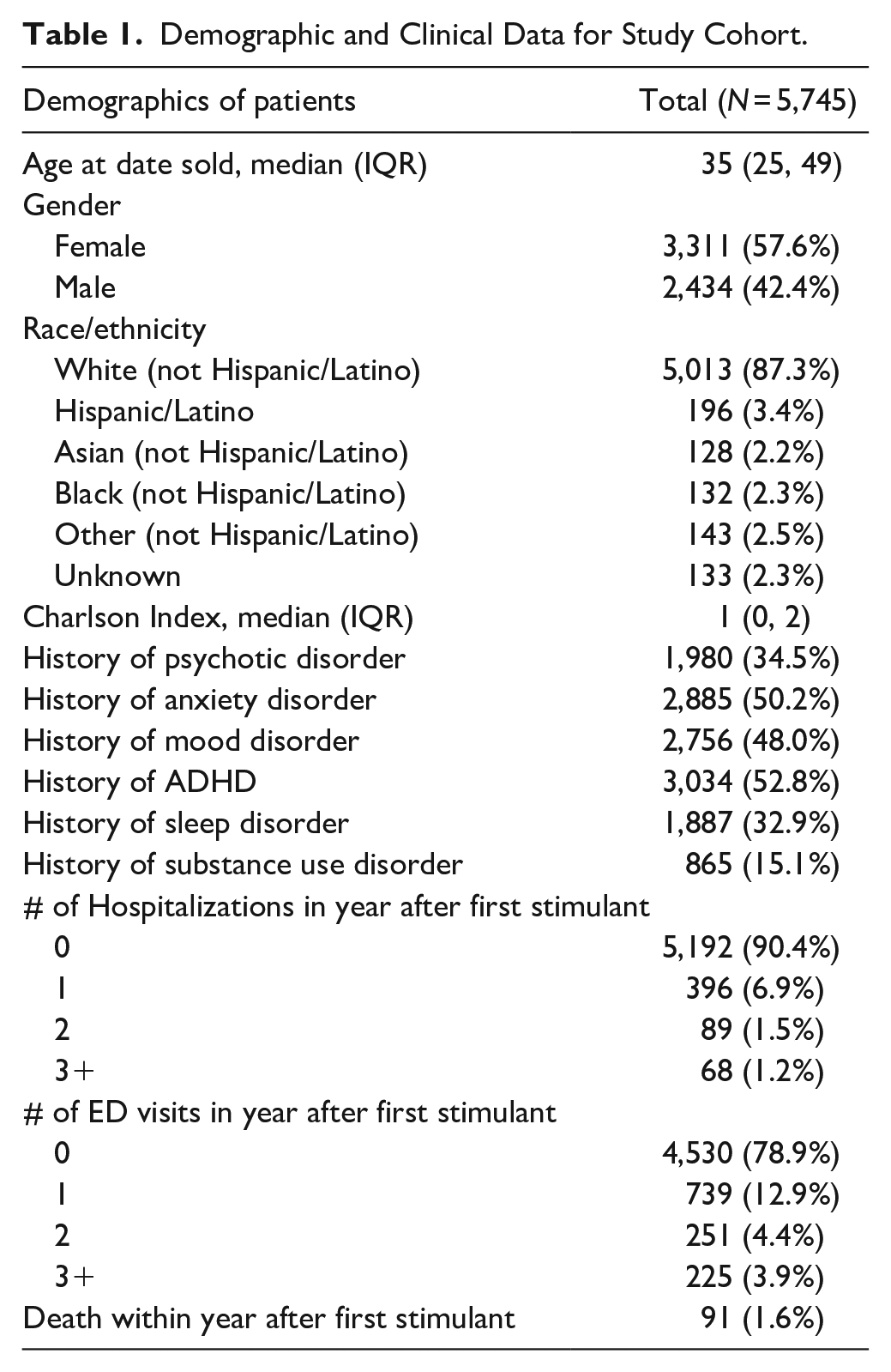
Figure 1 plots the number of stimulants dispensed and the number of patients who were dispensed stimulants against time by calendar quarters from 1/1/2015 to 7/1/2021 with yearly IRRs. Both the number of stimulant dispenses and the number of patients with stimulant dispenses increased significantly with yearly IRRs of 1.115 (95% CI [1.110, 1.119]) and 1.090 (95% CI [1.084, 1.096]), respectively. Among White patients, the IRRs for number of stimulant dispenses and the number of patients with stimulant dispenses were 1.109 (95% CI [1.104, 1.114]) and 1.085 (95% CI [1.079, 1.091]), respectively. Among Non-White patients, the IRRs for number of stimulant dispenses and the number of patients with stimulant dispenses were 1.164 (95% CI [1.148, 1.180]) and 1.132 (95% CI [1.111, 1.154]), respectively. Figure 2 displays a box plot of the average number of stimulant dispenses per patient per year, which also increased over the timeframe of the search by 0.17 per year (95% CI [0.13, 0.22], p < .001). Among White and Non-White patients, the average number of stimulant dispenses increased by 0.17 (95% CI [0.13, 0.22], p < .001) and 0.20 per year (95% CI [0.07, 0.34], p = .003) per patient per year, respectively. Figure 3 plots the co-dispensing data against time by calendar quarters from 1/1/2015 to 7/1/2021 with yearly IRRs. The number of patients with a stimulant dispensed who also had a benzodiazepine, Z-drug, or both dispensed at any point in the search timeframe increased significantly with incidence rate ratios of 1.077 (95% CI [1.065, 1.090]), 1.092 (95% CI [1.074, 1.111]), and 1.072 (95% CI [1.048, 1.098]), respectively. Among White patients, the number of patients with a stimulant dispensed who also had a benzodiazepine, Z-drug, or both dispensed at any point in the search timeframe increased significantly with incidence rate ratios of 1.073 (95% CI [1.060, 1.087]), 1.081 (95% CI [1.061, 1.100]), and 1.057 (95% CI [1.031, 1.083]), respectively. Among Non-White patients, the number of patients with a stimulant dispensed who also had a benzodiazepine, Z-drug, or both dispensed at any point in the search timeframe increased significantly with incidence rate ratios of 1.104 (95% CI [1.057, 1.153]), 1.156 (95% CI [1.095, 1.221]), and 1.211 (95% CI [1.110, 1.321]), respectively. The number of patients with a stimulant dispensed who also had a benzodiazepine, Z-drug, or both dispensed 30 days before or after the stimulant did not increase significantly. Table 2 displays the most commonly dispensed drugs in each class.

Stimulant dispensing data versus time in terms of fiscal quarters from 1/1/2015 to 7/1/2021.
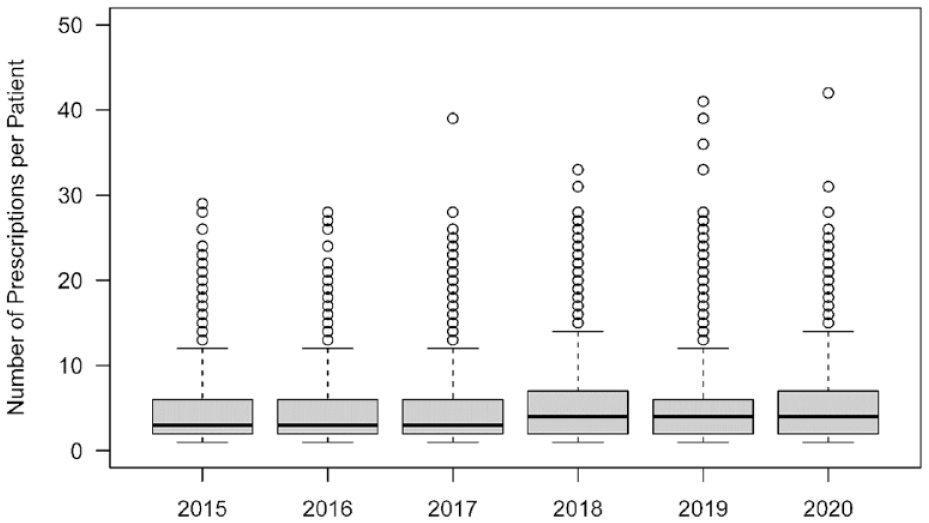
Box plot of average number of stimulant dispenses per patient per year.
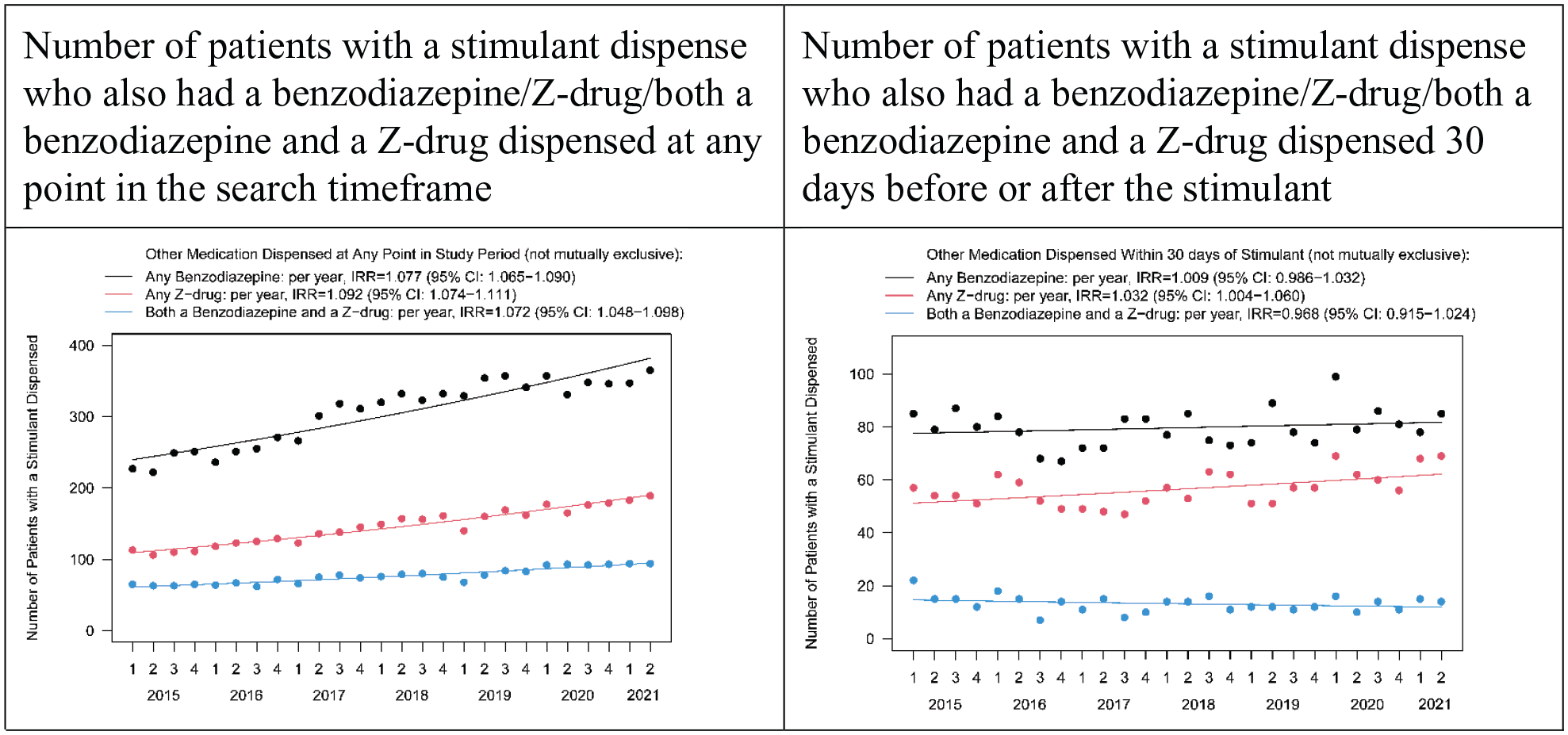
Stimulant dispensing data versus time in terms of fiscal quarters from 1/1/2015 to 7/1/2021.
Top Dispensed Drugs by Year.

Discussion
Throughout the study period, we found significant increases in the number of stimulant dispenses, the number of patients with stimulant dispenses, stimulants dispenses per patient per year, and the number of patients with a stimulant dispensed who also had a sedative/hypnotic dispensed. Specifically, we found an average 9% increase in number of patients purchasing stimulants from our pharmacies annually. As a point of comparison, Board et al. (2020) found the national annual rate of stimulant dispensing to have increased significantly from 5.6 to 6.1 prescriptions per 100 persons from 2014 to 2019, representing a 1.73% annual increase. Furthermore, Moustafa et al. (2022) analyzed data from the Automation of Reports and Consolidated Orders System (ARCOS) to report that amphetamine use in the U.S. increased approximately 2-fold from 2009 to 2018 (from 10 to 21 tons). Such an increase is likely linked to the increasing rates of ADHD diagnoses, especially among adults (Caldwell, 2001). A study using data from the U.S. National Health Interview Survey found the prevalence of ADHD among adults aged 18 to 64 years to have increased by 24.6% from 3.41% in 2007 to 4.25% in 2012 (London & Landes, 2021). Similarly, another U.S. study using National Ambulatory Medical Care Survey data found the prevalence of ADHD diagnoses to have increased by 36% from 1.85% to 2.53% in adults and by 18% from 9.31% to 11.03% in youth from 2008 to 2013 (Fairman et al., 2020). Accordingly, we found that the most common psychiatric diagnosis among all patients who were dispensed a stimulant in our search timeframe was ADHD. Moreover, the median age of patients in our study was 35 years.
There have been recent reports of rises in prescriptions for sedative-hypnotics. Bachuber et al. (2016) found that between 1996 and 2013, the percentage of adults filling a benzodiazepine prescription increased from 4.1% to 5.6% representing a 1.9% annual increase associated with an increase in overdose death rate from 0.58 to 3.07 (95% CI [2.99, 3.14]) per 100,000 adults. Agarwal and Landon (2019) found that, from 2003 to 2015, benzodiazepine prescriptions in ambulatory care increased from 3.8% to 7.4% of visits. Interestingly, they noted that benzodiazepine prescribing was stable among psychiatrists but increased among other specialties and that primary care clinicians accounted for about half of all visits at which benzodiazepines were prescribed. Kaufmann, Spira, Depp, and Mojtabai (2016) reported that, from 2005 to 2012, the proportion of visits with continuing benzodiazepine prescriptions increased significantly from 3.4% to 4.7% and that of non-benzodiazepine benzodiazepine receptor agonists increased significantly from 1.0% to 1.7% (p < .01). However, they found no significant changes in new prescriptions and thus concluded that the increase in sedative-hypnotic prescriptions was more likely attributable to long-term growth in continuing prescriptions rather than new prescriptions.
Although we found no significant increase in patients who were dispensed a stimulant and a benzodiazepine, Z-drug, or both 30 days before or after a stimulant, we did find significant increases in patients who were dispensed a stimulant and sedative/hypnotics at any point in the search timeframe. Similarly, a recent study found that 1 in 3,920 individuals residing in Washington State was prescribed both alprazolam and amphetamine, with the statewide prevalence of this co-prescription having increased 40.2% between 2013 and 2017 (Zarkowski et al., 2021). Furthermore, an analysis of prescription data from the Genoa Healthcare database of 10 participating U.S. community mental health centers from 2016 to 2018 found that alprazolam and amphetamine were co-prescribed to individual patients more often than could have occurred by chance (Zarkowski, 2020). Doctor shopping may have played a role in receiving this combination, as a case-control study found that patients who had multiple clinician episodes (defined as receiving a prescription for the same medication from two or more practitioners filled by two or more pharmacies) were significantly more likely to have received both benzodiazepines and stimulants (Wilsey et al., 2010). This may be a major issue for tertiary referral hospitals treating complex patients often with many comorbidities managed by many clinicians.
Notably, the number of stimulant dispenses and the number of patients with stimulant dispenses increased significantly more in Non-White patients than in White patients. Similarly, the number of patients with a stimulant dispensed who also had both a benzodiazepine and Z-drug dispensed at any point in the search timeframe increased significantly more in Non-White than in White patients. In a study on new prescription stimulant recipients in the US from 2010 to 2020, Brumbaugh et al. found a greater increase in prevalence of prescriptions to American Indian/Alaska Native (OR 2.25, 95% CI [1.88, 2.69]) and Asian (OR 2.46, 95% [CI 2.05, 2.94]) patients compared to White patients (OR 1.24, 95% CI [1.20, 1.28]). The increase of prescriptions to Black patients was significantly lower (OR 1.05, 95% CI [1.00, 1.11]) (Brumbaugh et al., 2022). Studies indicate that in the United States white children are much more likely to be prescribed stimulant medications than Black and Hispanic children, but less is known about potential over- or under prescribing based on race for adults (Hudson et al., 2007). However, racial disparities in the prescribing of opioids is well known (Morden et al., 2021). It is difficult to draw conclusions on the racial differences in prescribing the current study, particularly given the relative lack of racial diversity in this patient sample. Further investigation is warranted to better characterize prescribing differences of stimulants and other controlled medications across racial categories.
Limitations to this study include its retrospective design using data from a single, tertiary care institution. Dispensing records were used as a proxy for prescription consumption by patients. This approach did not capture prescriptions from clinicians of our institution that were filled at outside pharmacies, nor prescriptions received by patients from clinicians outside of our institution. Importantly, this study does not identify patients who may be obtaining prescriptions from multiple clinicians outside this institution. Data from the patients’ Prescription Drug Monitoring Program (PDMP) would have been more inclusive of all controlled substances prescribed and purchased from multiple pharmacies. However, the sharing of even deidentified data is prohibited in the state in which this study was conducted. Furthermore, we did not account for any potential increases in number of total drug dispenses from our pharmacies that may reflect growth in number of patients served. These factors may have biased our findings in the direction of underestimating the extent of the trends reported. On the other hand, our study design did not capture whether medications were discontinued at the time that other medications were started. The search could not capture medication administration schedules actually used by patients. These limitations may have biased our results toward overestimates of polypharmacy in patients who properly discarded discontinued medication or used their medication only as needed, and perhaps rarely. Although the findings of this study are not necessarily generalizable to the general US population, the results are consistent with prior studies, supporting that this likely represents a national trend. Lastly, although the COVID-19 pandemic may have influenced sedative prescriptions, it does not account for the reported multi-year trend.
Future directions include comparing the demographics of patients in this study to those in relevant matched control groups to further elucidate individual-level risk factors for polypharmacy. In addition, it would be useful to investigate the specialties of the clinicians prescribing stimulants and sedative/hypnotics to explore prescriber specific and/or system-level influences. Lastly, it would be beneficial to explore the indications for medications prescribed in cases of polypharmacy to better understand their clinical contexts and risk factors.
In conclusion, this retrospective review of a large pharmacy database confirms previous findings that there has been an increase in dispensing of stimulants over the past several years, and highlights concerns regarding the co-prescription of stimulants and sedatives as part of a larger public health concern.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.