
Abstract
Background:
ADHD diagnosis rates are rising; however, currently, no effective treatment method that has been identified. This study compared the efficacy of CBT + M with M for adult ADHD.
Methods:
PubMed, Embase, WOS, and Cochrane Library databases were searched up to July 29, 2023. Literature screening and data analysis were conducted.
Results:
The six randomized controlled studies included. Meta-analysis showed that CBT + M was more effective than M in improving ADHD symptoms. Subgroup analysis showed developed countries significant in ADHD symptoms improvement. At the 3-month, CBT + M was superior to M, but at the 6 and 9 months, no statistically significant differences were observed.
Conclusion:
CBT + M is more effective than M in improving adult ADHD symptoms and maintains an advantage for at least 3 months. It is recommended to intensifying CBT treatment after 3 months. Country and economy may influence results. Combined therapy for ADHD should be prioritized in developed countries.
Background
Attention deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by symptoms such as being easily distracted, lacking persistence, difficulty sustaining attention, and exhibiting disorganized behaviors (American Psychiatric Association, 2013). A study published in 2015 indicated a global prevalence of 3.4% for ADHD in children and adolescents (Polanczyk et al., 2015). Among children aged 3 to 12, the prevalence of ADHD is 7.6%, while adolescents aged 12 to 18 have an ADHD prevalence of 5.6% (Salari et al., 2023). A meta-analysis published in 2021 reported a prevalence of 2.58% for persistent adult ADHD and 6.76% for symptomatic adult ADHD (Song et al., 2021). ADHD has different prevalence rates in different countries, and tends to decline with decreasing income levels. The prevalence rate of adult ADHD is 3.6% in high-income countries, 3.0% in upper-middle-income countries, and 1.4% in lower-middle/low-income countries (American Psychiatric Association, 2013; Fayyad et al., 2017; Simon et al., 2009), which may be associated with insufficient diagnostic levels in low-income countries. Evidence indicates that ADHD is a prevalent mental health disorder in underdeveloped Slovenia in which it is still underdiagnosed compared to Western countries. Nevertheless, the ADHD prevalence in Slovenia has been on the rise over the years, increasing from 0.032% in 1997 to 0.082% in 2012; it is estimated to be 1% in 2020, which is 6.3 times higher than that in 1997 (Štuhec et al., 2015). Currently, despite effective treatments for ADHD, many child, adolescent, and adult patients remain undiagnosed and untreated in a timely manner (Stuhec & Locatelli, 2017). Therefore, ADHD has become an urgent issue.
It is widely acknowledged that ADHD is a lifelong condition, with symptoms persisting into adulthood in two-thirds of individuals. As a chronic condition, adult ADHD has a significant impact on patients’ quality of life and may lead to antisocial behaviors that negatively affect society. The treatment of ADHD is primarily pharmacotherapy, especially for adult ADHD (NICE, 2019), and the effectiveness of pharmacological treatment for adult ADHD varies. Currently, medications such as methylphenidate (MPH), amphetamines (AMP), and second-line drugs are commonly used for ADHD treatment (Caye et al., 2019). In the updated guidelines from the UK, psychostimulant medications are notably effective and considered the first choice, while non-stimulant medications do not yield strong effects (Bolea-Alamañac et al., 2014). In recent studies, lisdexamfetamine (LDX) has demonstrated superior efficacy over drugs such as methylphenidate in both pediatric and adult populations. Some research suggests that it is not just a supplemental medication to methylphenidate but currently the most effective drug for treating ADHD (Stuhec et al., 2019). Despite its inclusion in guidelines, not all countries have access to this medication (Bolea-Alamañac et al., 2014). However, medications are not without flaws. It has been reported that 20% to 50% of adults either do not respond well to medication, categorized as “non-responders,” or cannot tolerate the side effects.
Non-pharmacological treatments of ADHD included CBT, psychoeducation, neurofeedback therapy, standard working memory training, and self-alert training (SAT). A meta-analysis conducted in 2020 has indicated that CBT is the most common non-pharmacological intervention utilized, and most studies have reported that CBT can improve ADHD symptoms (Nimmo-Smith et al., 2020). CBT is a psychological therapy that integrates cognitive therapy (CT) and behavior therapy (BT) (Thoma et al., 2015). As a well-established psychological therapy, CBT is widely used to relieve anxiety, depression, and substance abuse. Some existing research suggests that CBT can alleviate emotional issues in patients and mitigate the risk of substance abuse (Borza, 2017; Copeland et al., 2001; Nakagawa et al., 2017). An earlier meta-analysis with smaller sample sizes has demonstrated that CBT is an effective means of treating ADHD (Jensen et al., 2016).
CBT has been demonstrated to be helpful in treating ADHD and may yield long-term benefits. A study on CBT for children with comorbid ADHD and anxiety conducted in Australia showed that children with ADHD who received CBT treatment for anxiety had significantly improved hyperactive symptoms (Gould et al., 2018). Another randomized controlled trial on adults with ADHD conducted in the UK found that adding CBT to standard treatment was more effective in reducing ADHD symptoms and improving occupational and social functions than standard treatment alone (Dittner et al., 2018). According to a review article, CBT is an effective treatment for adult ADHD, particularly when combined with pharmacotherapy (Mongia & Hechtman, 2012). However, existing meta-analyses of CBT for adult ADHD do not carefully differentiate between traditional CBT and new therapies based on CBT, such as DBT and MBCT. The purpose of this review is to investigate the efficacy and efficacy duration of CBT combined with pharmacotherapy compared to pharmacotherapy alone in adults with ADHD. The objectives are (a) to systematically assess the quality of randomized controlled trials examining the efficacy of CBT combined with pharmacotherapy for adult ADHD, (b) to employ meta-analysis to determine whether CBT combined with pharmacotherapy is superior to pharmacotherapy alone in reducing ADHD symptoms, (c) to investigate whether the efficacy of CBT combined with pharmacotherapy is influenced by the economic development level of the country, and ultimately (d) to provide recommendations for future clinical decision-making based on the research findings.
Method
Search Strategy
This systematic review and meta-analysis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021). The study was registered in the International Prospective Register of Systematic Reviews with the registration number CRD42023409309.
Electronic databases, including PubMed, EMBASE, Cochrane, and Web of Science, were searched from the inception of the database up to July 29, 2023, to identify relevant studies for the meta-analysis. The reference lists of included studies were manually searched to collect potentially eligible studies. Clinical Trials.gov was also searched for completed and ongoing trials. The final literature search was conducted on July 29, 2023. The search used Mesh terms such as Attention Deficit Disorder with Hyperactivity and Cognitive Behavioral Therapy along with related free terms, and the study type was restricted to randomized controlled trials (RCTs), as exemplified in PubMed. The search strategy is provided in the appendix. Only English-language publications with ADHD symptoms as the primary outcome measure were included.
Inclusion and Exclusion Criteria
The inclusion criteria for the meta-analysis were as follows:
P: Participants included individuals aged 18 years or older, diagnosed with ADHD based on any diagnostic criteria, irrespective of disease severity or the presence of comorbidities or complications. Additionally, patients had received pharmacological treatment for ADHD.
I: The intervention in the treatment group was traditional CBT in combination with pharmacotherapy.
C: The control measure in the control group was pharmacotherapy alone.
O: Outcomes of interest include ADHD symptoms, depression, anxiety, inattention, hyperactivity-impulsivity, social function, antisocial symptoms, and CGI scores.
S: All blinded RCTs were included.
The exclusion criteria were as follows:
(1) Experimental group receiving CBT alone.
(2) Studies where full-text articles or data could not be obtained, for instance, if the original text was unsearchable or follow-up results could not be found on experimental registration pages.
(3) Case reports, abstracts, conference papers, reviews, meta-analyses, non-RCTs, and presentations at EPA, ECNP, APA, and ESCAP congresses.
(4) Duplicate publications.
(5) Studies utilizing non-traditional CBT, such as mindfulness-based therapies or dialectical behavior therapy.
(6) Animal studies.
Study Selection and Data Extraction
Two reviewers independently performed literature screening. Simultaneously, published meta-analyses were checked to ensure the inclusion of any additional eligible literature. The titles and abstracts were checked to exclude studies that did not meet the inclusion criteria. Then the full texts of the remaining studies were read to select eligible articles. Any discrepancies were resolved through discussion between the two reviewers, and consultation with a third party if necessary.
Data extraction was performed independently by two researchers using pre-defined electronic forms. The following information was recorded: first author, publication year, study design type, sample size, country, gender, age, assessment scales, and follow-up time.
The primary outcomes in the included studies encompassed scores on rating scales such as the Conners’ Adult ADHD Rating Scale (CAARS), ADHD Self-Rating Behavior Questionnaire (ADHD-SR), RATE-S Scale (RATE), and Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS). Secondary outcomes included scores on rating scales such as the Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), Hamilton Anxiety Scale (HAM-A), Hamilton Depression Scale (HAM-D), Clinical Global Impression Scale (CGI-S), and Barkley ADHD Current Symptoms Scale (BCS) for measures of depression, anxiety, inattention, hyperactivity-impulsivity, social functioning, antisocial symptoms, and clinical global impression. All outcome measures were continuous variables, and therefore, median and standard deviation values at intervention and follow-up time points were extracted from each article. If standard errors were reported, they were converted to standard deviations.
Quality Assessment
Two reviewers (Li and Zhang) independently assessed the quality of the RCTs using the Cochrane risk-of-bias assessment tool, which includes seven domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other potential sources of bias (other bias). Each domain was rated as low risk, unclear risk, or high risk of bias (Higgins et al., 2011).
Statistical Analysis
Our outcome measures included ADHD symptoms, depression, anxiety, inattention, hyperactivity-impulsivity, social functioning, antisocial symptoms, and clinical global impression (CGI) scores at the end of intervention and follow-up. The standardized mean difference (SMD) with 95% confidence interval (CI) was used as the effect size, where a negative SMD indicated greater symptom improvement in the intervention group compared to the control group, with larger absolute values indicating more significant symptom improvement.
Heterogeneity was evaluated using Cochrane I2 statistics, with p < .05 or I2 > 50% considered statistically significant heterogeneity (Higgins & Thompson, 2002). In cases of significant heterogeneity, a random-effects model was used, and sensitivity analysis, subgroup analysis, or meta-regression was performed to identify sources of heterogeneity. Sensitivity analysis was conducted by systematically excluding the studies one by one to examine the source of heterogeneity and reliability of the results. Statistical analyses were conducted using Revman 5.3 or STATA 15.1 software.
Results
Overview of Study Screening Results
A total of 1,490 articles were identified from PubMed, Cochrane Library databases, Embase, and WOS databases and imported into Endnote X9 for literature screening. Meta-analyses and reviews (n = 130), case reports, conference abstracts, errata, guidelines, letters (n = 32), and non-English articles (n = 4) were excluded. After further screening of abstracts and titles, 87 articles were excluded due to inappropriate control groups, 465 articles were excluded due to non-ADHD&CBT studies, 48 articles were excluded due to non-RCT studies, and 704 articles were excluded due to age restrictions. Then, 20 articles were reviewed in full text, and we excluded those without access to original data (6), irrelevant outcome measures (4), and conference proceedings (4). Finally, six RCTs were included in the meta-analysis (Figure 1). The six experiments conducted in Iceland, China, Switzerland, and the United States were published between 2005 and 2022. A total of 416 participants were included in the six studies, with an average age of 33.23 (SD = 11.28). All six studies were RCTs (Table 1) (Corbisiero et al., 2018; Emilsson et al., 2011; Pan et al., 2022; Safren et al., 2005; Young et al., 2015, 2017). A total of 416 participants were included in the final analysis, with 208 in the intervention group and 208 in the control group. All included participants received pharmacotherapy prior to the start of the experiment. The experimental group underwent CBT or a CBT-based R&R2ADHD model in conjunction with pharmacological treatment, while the control group, in addition to receiving pharmacotherapy, was provided with standard clinical management (SCM), treatment as usual (TAU), or nonpharmacological consultation (NC) as a control for CBT, which did not improve patients’ adverse cognition.
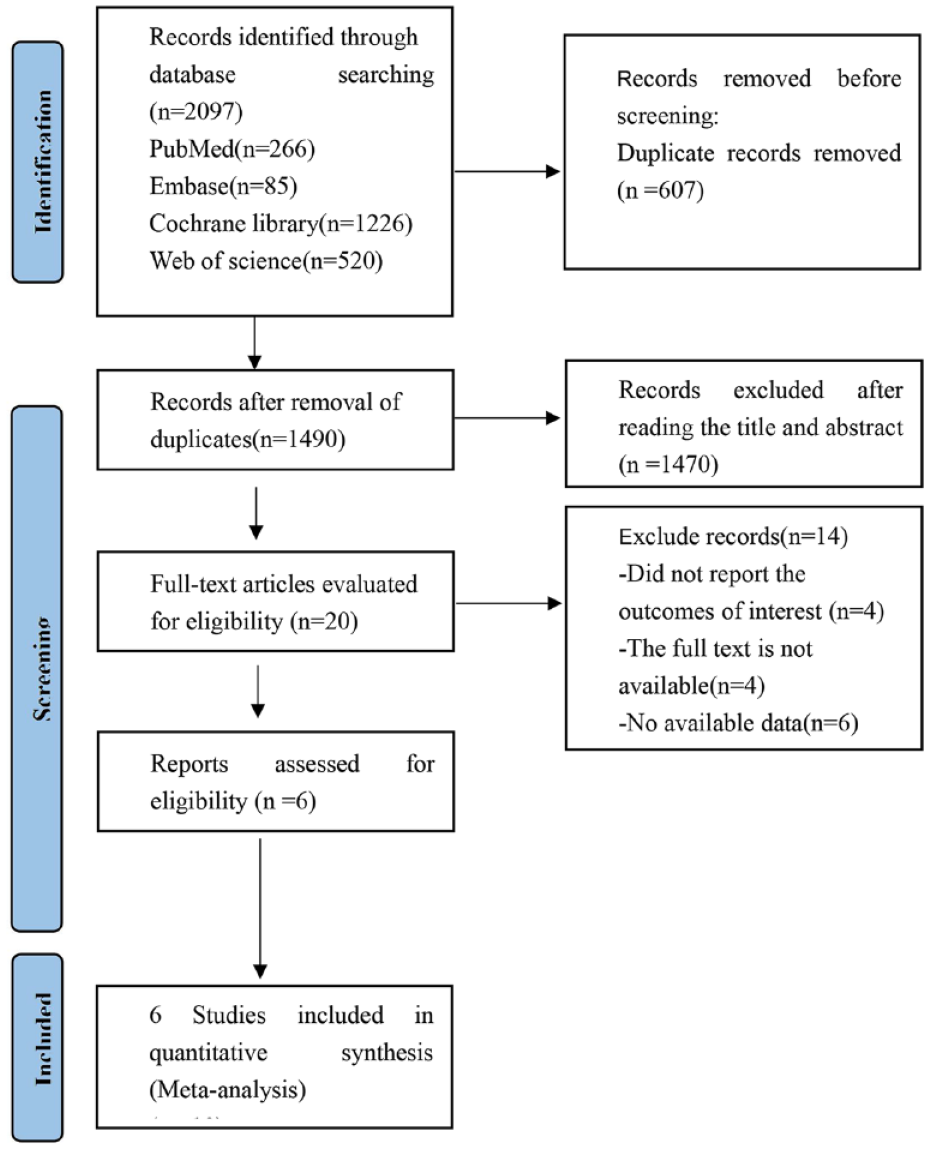
PRISMA flow diagram of the study process. PRISMA, Preferred Reporting Items for Systematic review and Meta-analysis.
Characteristics of Included Literature.
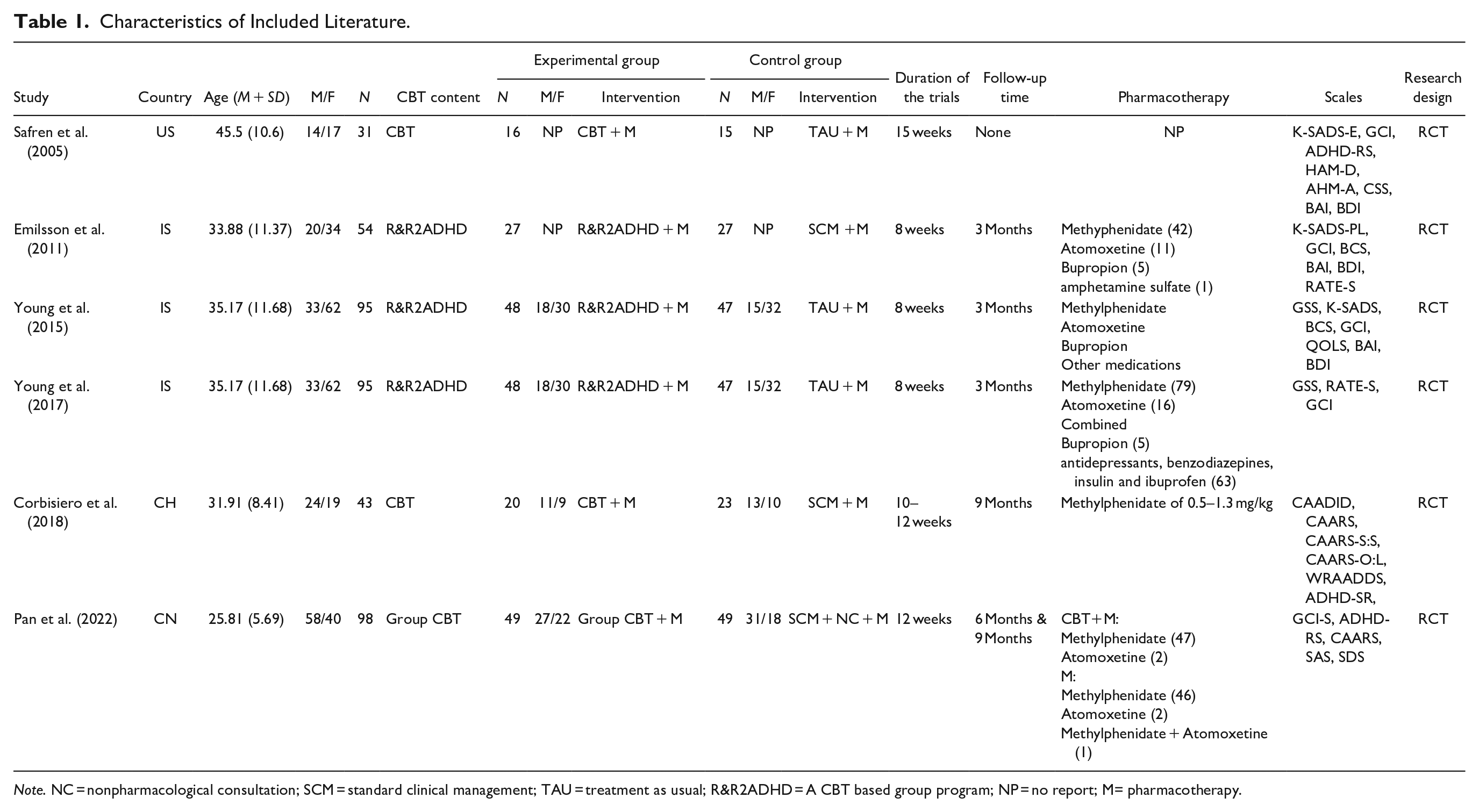
Note. NC = nonpharmacological consultation; SCM = standard clinical management; TAU = treatment as usual; R&R2ADHD = A CBT based group program; NP = no report; M= pharmacotherapy.
Details of the risk-of-bias assessment are presented in Figure 2.
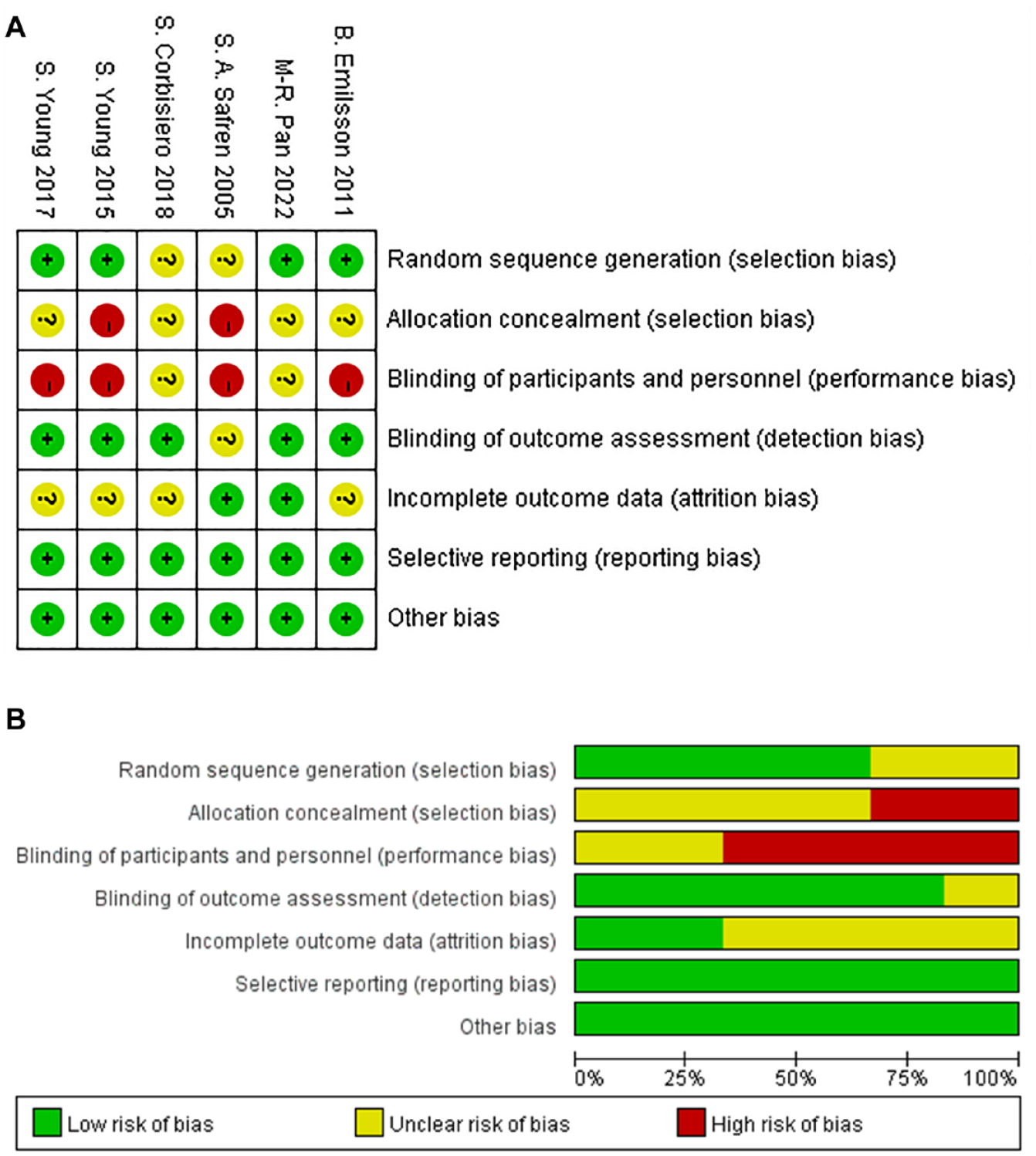
(A) Risk of bias summary; (B) Risk of bias graph.
Risk of Bias Within Studies
We assessed the risk of bias for all RCTs. In two studies, the random sequence generation method was inadequately described, resulting in a moderate risk for random sequence generation, whereas four studies provided detailed descriptions of the random sequence generation, resulting in a low risk. In two studies, a high risk was assigned for allocation concealment due to the absence of appropriate blank controls in the control group; the remaining studies with unclear allocation concealment were assigned a moderate risk. Four studies exhibited a risk of unblinding, resulting in a high risk for blinding of participants and personnel. An additional two studies had a relatively lower risk of unblinding, leading to a moderate risk for blinding of participants and personnel. One study did not provide a detailed description of the assessors, resulting in a moderate risk for the blind outcome assessment, while the remaining five studies provided detailed information about the assessors and assessment methods, leading to a low risk. Four studies did not report detailed lost to follow-up information but did report the number of participants lost to follow-up, resulting in a moderate risk for incomplete outcome data. The other two studies had comprehensive reporting, yielding a low risk. All six articles showed no evidence of selective reporting, resulting in a low risk. All six reports did not exhibit other biases, resulting in a low risk.
Primary Outcomes
Six RCTs studies were included in this meta-analysis. Five studies used rating scales such as RATE, K-SADS, BCS, CSS, ADHD-RS, and CAARS to evaluate the improvement of ADHD symptoms at both the end of treatment and follow-up, while one study evaluated ADHD symptoms improvement only at the end of treatment. Therefore, meta-analyses were performed separately for the end of treatment and follow-up time points. The meta-analysis, using a fixed-effects model (p = 0.33, I2 = 12%), revealed that CBT combined with pharmacotherapy can significantly improve symptoms of ADHD compared to pharmacotherapy alone at the end of treatment (SMD = −0.43, 95% CI [−0.60 to −0.27], p < .00001), as shown in Forest plot 1 (Figure 3A). Five studies conducted follow-up evaluations at 3, 6, and 9 months. A random-effects model was used for the meta-analysis due to significant heterogeneity (I2 = 56%, p = .02), and the results showed that CBT combined with pharmacotherapy was more effective in improving ADHD symptoms than pharmacotherapy alone at the end of follow-up (SMD = −0.45, 95% CI [−0.70 to −0.19], p = .0005), as shown in Forest plot 2 (Figure 3B). Sensitivity analysis did not reveal any sources of heterogeneity (Figure 4).
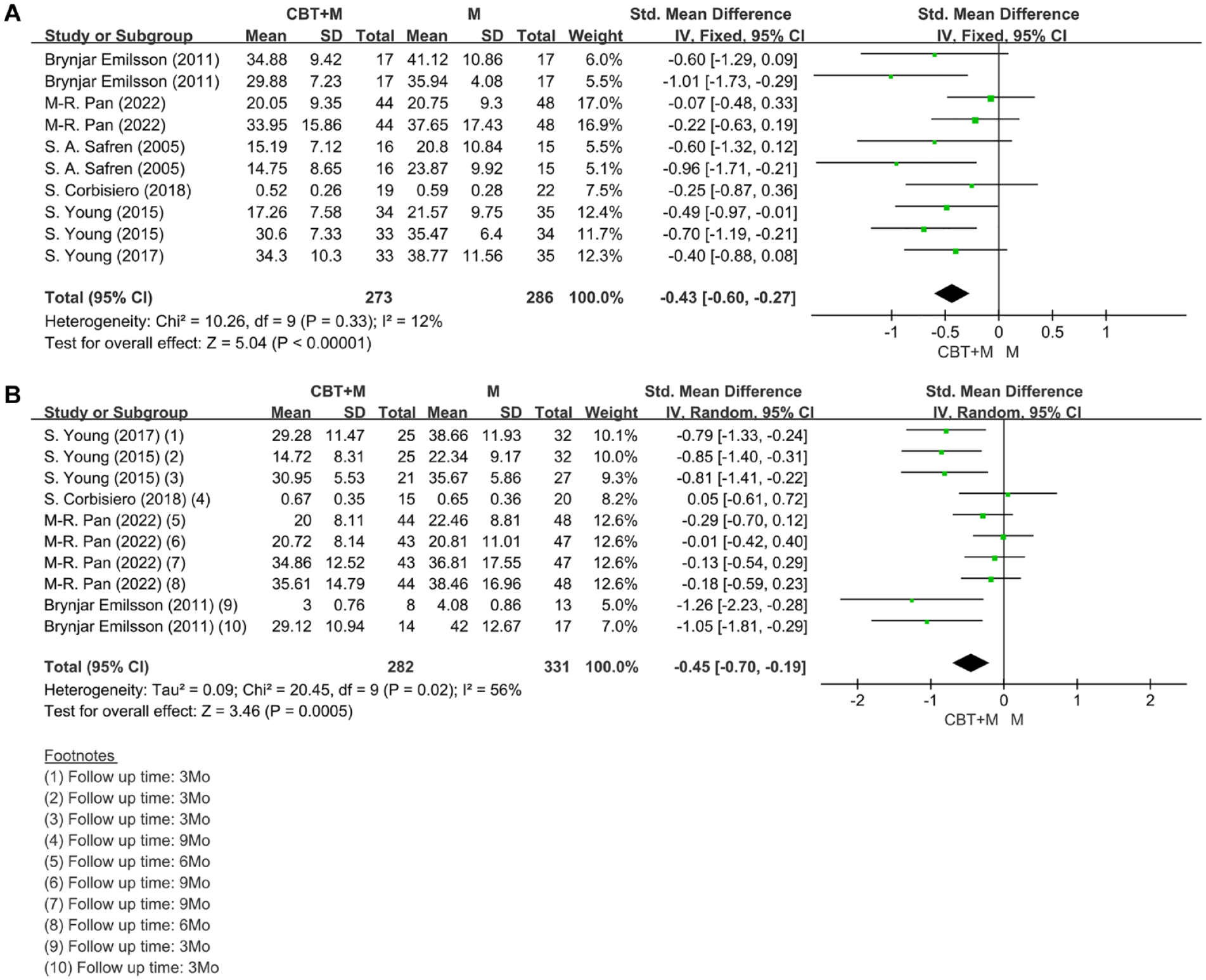
(A) Forest Plot 1: Improvement of ADHD symptoms at the end of treatment; (B) Forest Plot 2: Improvement of ADHD symptoms at follow-up. (A) Forest Plot 1 presents data obtained by the same author using different scales of same paper in the end time; (B) Forest Plot 2 displays data gained by the same author using different scales in the different follow-up times within the same publication.
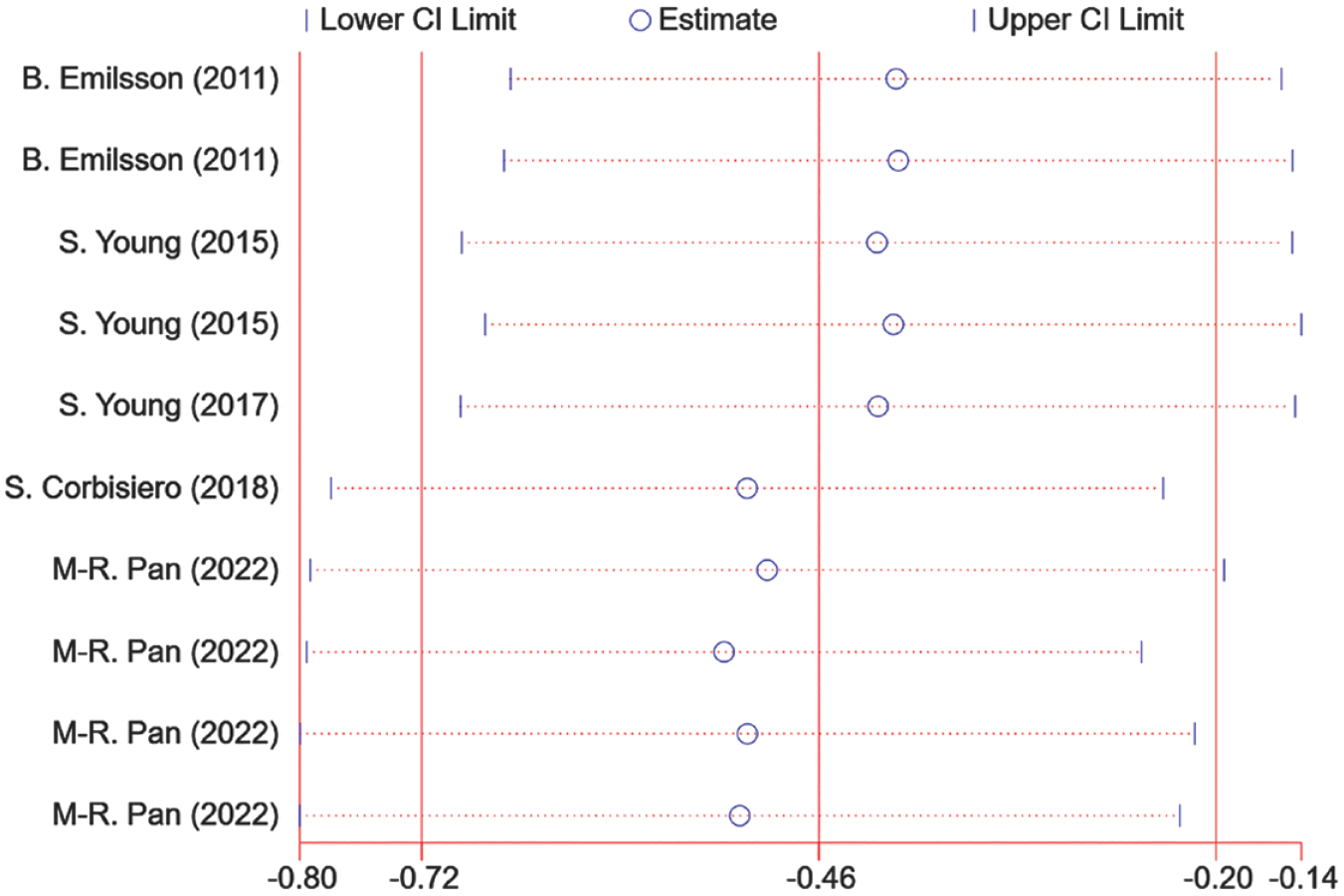
Sensitivity analysis based on improvement of ADHD symptoms at follow-up..
We conducted meta-regression analyses on control group type, country, level of national development, choice of assessors and assessment methods, and follow-up duration. The meta-regression analysis results revealed that factors contributing to heterogeneity included the use of non-pharmacological interventions (p = .010), country of subjects (p = .015) and economic development level (p = .000), choice of evaluation approach by researchers (p = .002), and follow-up time point (p = .000).
Secondary Outcomes
The secondary outcome measures included hyperactivity-impulsivity, impaired social functioning, antisocial symptoms, anxiety, depression, inattention, emotional control, and CGI scores. The BCS, K-SADS, ADHD-RS, RATE, SAS, HAMA, BAI, SDS, BDI, HAMD, CAARS, and GCI-S scales were used to evaluate the secondary outcomes at the end of treatment and during follow-up in the studies. The meta-analysis showed that CBT combined with pharmacotherapy was significantly more effective than pharmacotherapy alone in improving social function, antisocial symptoms, anxiety, depression, inattention, emotional control, and CGI scores at the end of both treatment and follow-up. CBT combined with pharmacotherapy and pharmacotherapy same showed reduction in Hyperactivity-impulsivity at any time, but there was no significant difference (SMD = −0.12/−0.34, 95% CI [−0.38 to 0.14/−0.69 to 0.02], p = 0.38/.06). Specific data are presented in Table 2. Meta-regression analysis revealed that for depression, heterogeneity during follow-up may be due to the country of participants (p = .001) and economic development level (p = .000), the choice of evaluation approach by researchers (p = .000), and follow-up time point (p = .000); for inattention, heterogeneity may be related to follow-up time (p = .000); for hyperactivity-impulsivity during follow-up, heterogeneity may be attributable to the country of subjects (p = .004) and economic development level (p = .002), different evaluation approaches chosen by researchers (p = .018), and follow-up time point (p = .002). For data with substantial heterogeneity, we conducted sensitivity analysis using Stata, and no sources of heterogeneity were identified.
Secondary Outcome Measures.
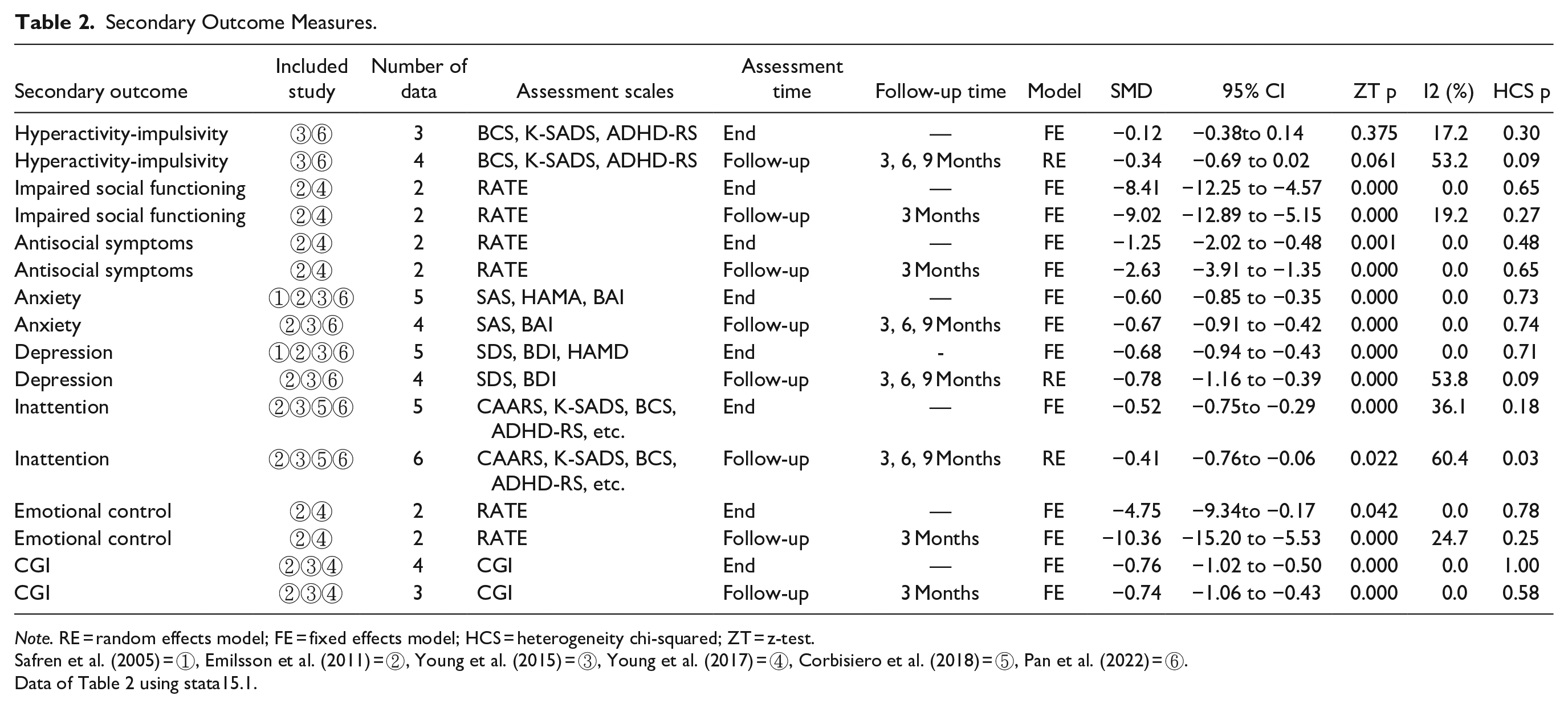
Note. RE = random effects model; FE = fixed effects model; HCS = heterogeneity chi-squared; ZT = z-test.
Safren et al. (2005) = ①, Emilsson et al. (2011) = ②, Young et al. (2015) = ③, Young et al. (2017) = ④, Corbisiero et al. (2018) = ⑤, Pan et al. (2022) = ⑥.
Data of Table 2 using stata15.1.
Subgroup Analysis
Subgroup analysis by country and economic development level
Due to the variation in the countries where the included studies were conducted, a subgroup analysis was performed based on the country to differentiate the outcomes of ADHD symptoms after treatment completion. Three experiments by Young et al. (2017), Emilsson et al. (2011), and Young et al. (2015) were conducted in Iceland, one experiment by Safren et al. (2005) was conducted in the United States, one experiment by Pan et al. (2022) was conducted in China, and one experiment by Corbisiero et al. (2018) was conducted in Switzerland. The overall I2 was 12%, indicating low heterogeneity; therefore, a fixed-effects model was used. There was no significant heterogeneity within the subgroups of Iceland, China, and the United States (I2 = 0.0%). The subgroup analysis revealed that in Iceland and the United States, CBT combined with pharmacotherapy had significantly superior efficacy compared to the control group receiving pharmacotherapy alone (SMD = −0.59, 95% CI [−0.84 to −0.35], p < .00001), (SMD = −0.77, 95% CI [−1.29 to −0.25], p = .004). Meanwhile, in China and Switzerland, no significant difference was observed in efficacy between the experimental and control groups (SMD = −0.15, 95% CI [−0.44 to 0.14], p = 0.32; SMD = −0.25, 95% CI [−0.87 to 0.36], p = 0.42), as shown in Forest Plot 3 (Figure 5A).
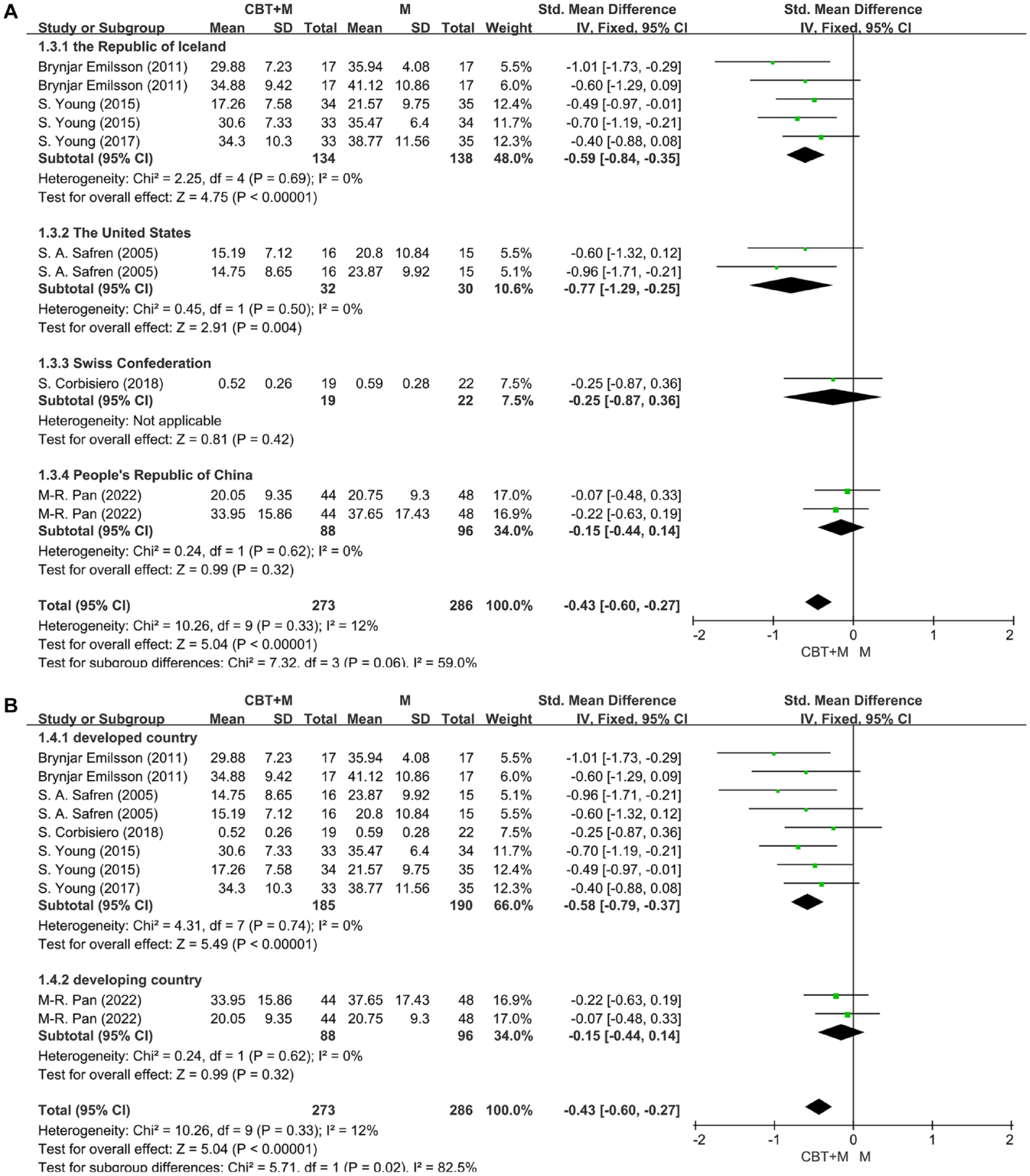
(A) Forest Plot 3: Subgroup analysis based on country for ADHD symptoms at the end of treatment. (B) Forest Plot 4: Subgroup analysis based on economic development level for ADHD symptoms at the end of treatment.
Moreover, we further divided the countries into developed and developing countries based on their economic development level. The classification of developing and developed countries is based on 2019 World Bank data. Countries with a gross national income (GNI) per capita of $12,536 or more are considered high-income, that is, developed countries, while those with GNI per capita lower than this threshold are classified as developing countries. Five experiments by Young et al. (2017), Emilsson et al. (2011), Young et al. (2015), Safren et al. (2005), and Corbisiero et al. (2018) were conducted in developed countries, and one experiment by Pan et al. (2022) was conducted in a developing country. The subgroup analysis demonstrated that in developed countries, the experimental group had superior efficacy compared to the control group (SMD = −0.58, 95% CI [−0.79 to −0.37], p < .00001). In contrast, the results from studies conducted in developing countries showed that the experimental group exhibited a slight reduction in symptoms, but the difference was not significant (SMD = −0.15, 95% CI [−0.44 to 0.14], p = 0.32), as shown in Forest Plot 4 (Figure 5B).
Subgroup analysis by follow-up time point
The stability of the results regarding ADHD symptoms may also be influenced by the time points of follow-up. Therefore, further subgroup analysis was conducted based on the follow-up time points. Specifically, in the studies by Young et al. (2017), Emilsson et al. (2011), and Young et al. (2015), the follow-up duration was 3 months. In the study by Corbisiero et al. (2018), the follow-up period was 9 months. The study by Pan et al. (2022) included two follow-up time points, namely 6 months and 9 months. The subgroup analysis showed that at 3 months, the experimental group had superior efficacy compared to the control group (SMD = −0.89, 95% CI [−1.17 to −0.60], p < .00001), while at 6 months and 9 months, there was no significant difference between the experimental and control groups (SMD = −0.23, 95% CI [−0.52 to 0.06], p = 0.12 at 6 months; SMD = −0.05, 95% CI [−0.32 to 0.22], p = 0.73 at 9 months), as shown in Forest Plot 5 (Figure 6).
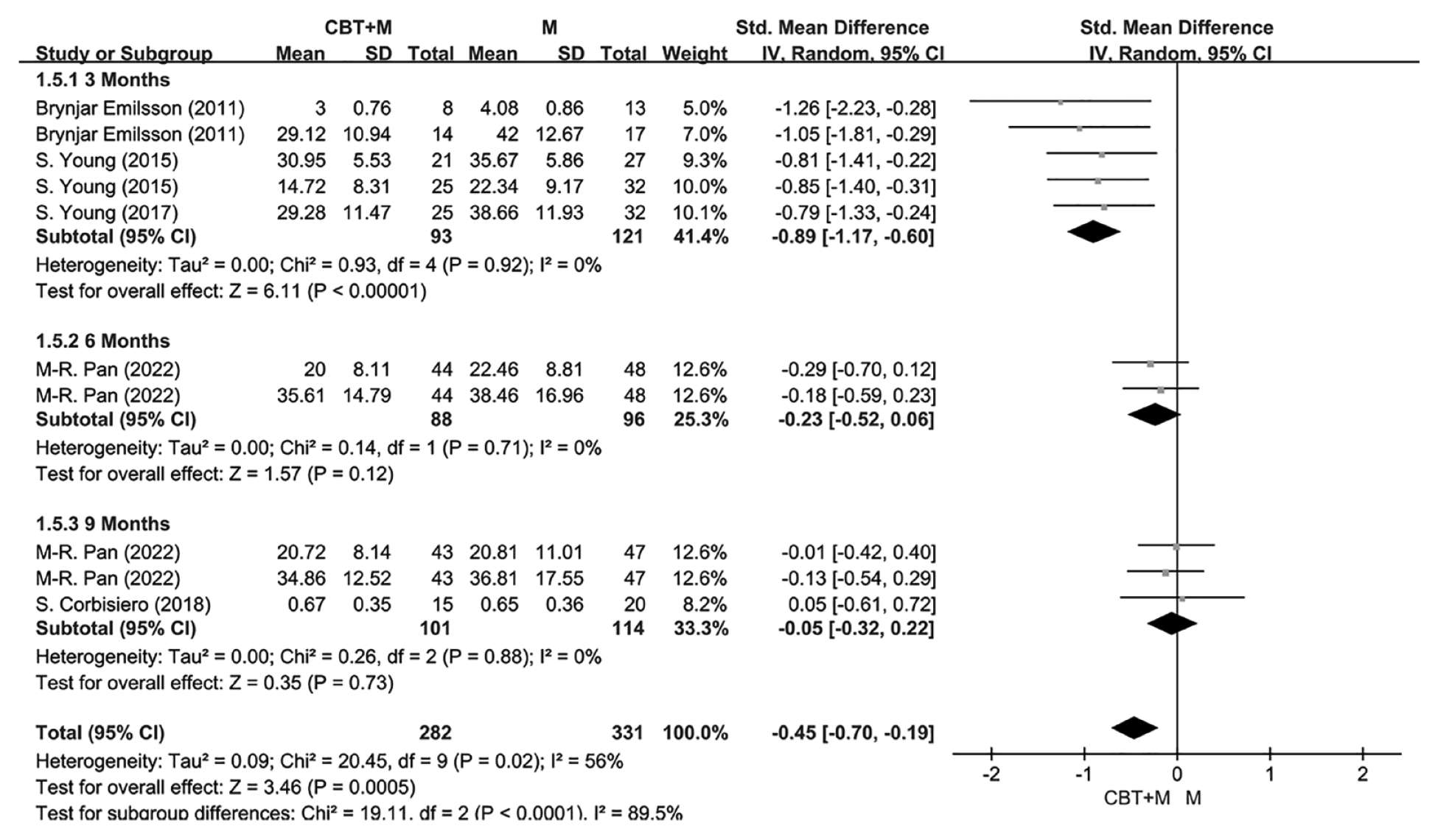
Forest Plot 5: Subgroup analysis based on different follow-up time points for ADHD symptoms.
Discussion
Our study results indicate that CBT combined with pharmacotherapy is more effective in improving symptoms of adult ADHD compared to pharmacotherapy alone, and this significant improvement can be observed both at the end of treatment and during follow-up assessments. For secondary outcome measures such as impaired social functioning, antisocial symptoms, depression, anxiety, inattention, and emotional control, the combination of CBT and pharmacotherapy showed more pronounced improvements compared to pharmacotherapy alone at both the end of treatment and follow-up. Additionally, at both treatment completion and follow-up, the combination treatment had a more significant improvement in CGI scores compared to pharmacotherapy alone. However, for the primary outcome measure of hyperactivity-impulsivity symptoms, there was no significant difference between CBT combined with pharmacotherapy and pharmacotherapy alone, both at the end of treatment and during follow-up assessments. Furthermore, we found that the efficacy of CBT combined with pharmacotherapy versus pharmacotherapy alone may vary with the country where the study was conducted. Furthermore, the economic development level of a country may have an impact on the efficacy of the two treatment approaches. Specifically, in developed countries, the combination treatment was significantly more effective than pharmacotherapy alone, while in developing countries, there was no significant difference between the two groups. Moreover, subgroup analysis by follow-up time points showed that the combination treatment was superior at 3 months. However, no significant differences were observed between the two groups at 6 and 9 months, indicating that the benefits of CBT combined with pharmacotherapy may persist for a minimum of 3 months.
In light of this finding, future research is desired to ascertain whether intensifying CBT treatment after 3 months can yield greater benefits for patients.
CBT has been established as an effective treatment approach for improving ADHD symptoms, and numerous research teams have conducted extensive investigations in this area. Building upon this foundation, researchers exploring “new wave” CBTs, such as DBT and MBCT, have also begun to explore their application in treating adult ADHD (Halmøy et al., 2022; Hepark et al., 2019; Hofmann et al., 2010). However, traditional CBT remains frequently recommended in some guidelines (NICE, 2019) and is also the most commonly mentioned approach in current research (Nimmo-Smith et al., 2020). Therefore, it is important to distinguish between traditional CBT and derivative therapies such as dialectical behavior therapy (DBT), mindfulness-based cognitive therapy (MBCT), and acceptance and commitment therapy (ACT), as they are based on distinct conceptual frameworks.
The core of classical CBT is to change maladaptive cognitions, while the new-wave CBT modifies this approach. For example, MBCT focuses on the present rather than ruminating on the past or worrying about the future. ACT encourages patients to accept negative thoughts and feelings rather than attempting to eliminate or change them (Hofmann et al., 2010). The core dialectic between acceptance and change is central to DBT (Swales, 2009). Although there is an increasing emergence of non-pharmacological therapies like new-wave CBT, traditional CBT, as the most commonly used approach at present, has a more mature foundation and has been tested in numerous studies. Therefore, it is necessary to differentiate between CBT and new-wave CBT, as this may be more helpful in exploring effective therapies for adult ADHD.
As demonstrated in this study, utilizing traditional cognitive-behavioral therapy (CBT) in conjunction with pharmacotherapy for adult ADHD generally yields better outcomes compared to using pharmacotherapy alone, and this advantage can be sustained for at least 3 months. Therefore, it can be concluded that CBT combined with pharmacotherapy, based on the principles of traditional CBT theory, is more effective in alleviating ADHD symptoms, as well as reducing the negative impact on social function, depression, anxiety, and other related aspects in adults with ADHD. This not only benefits the patients but also reduces the burden imposed by adult ADHD on society.
However, this study has several limitations. First, the inclusion of a limited number of studies due to restrictions in searched databases, languages, and study designs, including two articles authored by the same person, may impact the persuasiveness of the findings. Second, some of the control groups included in this study did not receive any non-pharmacological interventions but instead received routine treatment only, posing a potential risk of blinding and introducing selection bias. Additionally, new research has started to explore subtyping adult ADHD patients with different psychiatric features, psychosocial functioning, and comorbidities (Sobanski et al., 2008). However, the literature included in this study did not adequately differentiate these different patient types, potentially limiting the generalizability of the conclusions to clinical practice. Moreover, the limited number of countries included in the studies may restrict the applicability of the findings to certain regions. Lastly, the use of different medications, such as amphetamines and methylphenidate, in the pharmacotherapy across the studies may compromise the reliability of our results (Cortese et al., 2018). For instance, some adverse reactions of atomoxetine may occur over an extended duration, suggesting that in prolonged treatment, placebo might be more advantageous over atomoxetine (Banaschewski et al., 2006). However, the studies we included were all short-term studies; hence, certain positive results should be interpretated with caution.
Another limitation of this study is the absence of updated medications in the included studies. With evolving guidelines, LDX has been found to exhibit superior efficacy and is recommended (Stuhec et al., 2019). In the future, research combining LDX with CBT could be conducted, potentially yielding greater benefits for patients.
The six studies incorporated different follow-up durations, as not all studies conducting follow-ups at 3, 6, and 9 months, which may contribute to the lack of statistically significant results between 6 and 9 months. Reports of follow-ups at 9 months were only available from the studies by Corbisiero et al. (2018) and Pan et al. (2022), while follow-ups at 6 months were solely reported by Pan et al. (2022), and neither of these studies conducted follow-ups at 3 months. Emilsson et al. (2011), Young et al. (2015), and Young et al. (2017) exclusively reported follow-ups at 3 months. Due to the relatively limited number of included studies, we were unable to conduct further analysis on this result, which is also a limitation of this study.
Additionally, as some studies did not rigorously document dosage, we were unable to delve deeper into whether different medications and dosages might have an impact.
Given the limited quality of the included literature, our results may harbor a certain degree of bias. Further research should focus on incorporating more low-bias literature to enhance the reliability and accuracy of results, thus providing clinicians with more dependable evidence-based guidance.
Our findings strongly support the conclusion that the efficacy of CBT combined with pharmacotherapy surpasses that of pharmacotherapy alone in clinical practice for treating adult ADHD. Further research is needed to validate whether the combined therapy is indeed more effective for improving adult ADHD than pharmacotherapy alone. Furthermore, our results provide potential directions for future research by suggesting the differentiation of countries and their economic development levels. This would allow for a more detailed examination of the advantages of CBT combined with pharmacotherapy over pharmacotherapy alone in various countries and under different economic contexts. This conclusion that CBT combined with medication therapy is superior to pharmacotherapy alone also provides further evidence for guideline development.
Supplemental Material
sj-docx-1-jad-10.1177_10870547231214969 – Supplemental material for Efficacy of Cognitive Behavioral Therapy Combined with Pharmacotherapy Versus Pharmacotherapy Alone in Adult ADHD: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jad-10.1177_10870547231214969 for Efficacy of Cognitive Behavioral Therapy Combined with Pharmacotherapy Versus Pharmacotherapy Alone in Adult ADHD: A Systematic Review and Meta-Analysis by Yanxi Li and Lina Zhang in Journal of Attention Disorders
Supplemental Material
sj-docx-2-jad-10.1177_10870547231214969 – Supplemental material for Efficacy of Cognitive Behavioral Therapy Combined with Pharmacotherapy Versus Pharmacotherapy Alone in Adult ADHD: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-jad-10.1177_10870547231214969 for Efficacy of Cognitive Behavioral Therapy Combined with Pharmacotherapy Versus Pharmacotherapy Alone in Adult ADHD: A Systematic Review and Meta-Analysis by Yanxi Li and Lina Zhang in Journal of Attention Disorders
Footnotes
Acknowledgements
Not applicable.
Author Contributions
Conceptualization: Yanxi Li; Methodology: Yanxi Li; Formal analysis and investigation: Yanxi Li; Writing—original draft preparation: Yanxi Li; Writing—review and editing: [Yanxi Li]; Funding acquisition: Lina Zhang; Resources: Lina Zhang; Supervision: Lina Zhang.
And all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
All analyses were based on previous published studies, thus no ethical approval and patient consent are required.
Trial Registration
The study was registered in the International Prospective Register of Systematic Reviews with the registration number CRD42023409309.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article (and its Supplementary Information files).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.