
Abstract
Objective:
A pilot study to preliminarily examine the effects of Prism EFP NeuroFeedback (NF) in adult ADHD.
Method:
Prism EFP NF is a form of NF specifically designed to target emotional dysregulation (ED) through down regulation of amygdala activity. Prism EFP NF has been shown to improve other disorders with significant ED. Nine participants with adult ADHD received an open trial of Prism EFP NF consisting of fifteen sessions over 8 weeks; all completed at least 5 weeks of treatment with seven completing all 8 weeks. Outcomes were assessed by change in ADHD symptoms from baseline to End of Treatment.
Results:
About two-third reduction was seen in total DSM ADHD symptom scores (primary outcome measure) with improvement observed in all other clinical measures. No significant adverse events were seen.
Conclusion:
This preliminary trial found substantial effects of Prism EFP NF on ADHD/ED symptoms and global impairment.
Keywords
Relationship to the Work of Joseph Biederman MD
This manuscript describes a pilot study using a amygdala-targeted NeuroFeedback to target emotional regulation symptoms in adults with ADHD; one intent of this investigation was to examine if symptoms of emotional dysregulation improved with Prism EFP NF, would core DSM inattentive and hyper-active impulsive symptoms also be ameliorated. This work would be of high interest to Dr. Joseph Biederman. He and his co-investigators at Massachusetts General Hospital performed critical studies identifying symptoms of emotional dysregulation and helped establish the term deficits of emotional self-regulation (DESR) in adults with ADHD. They established that these symptoms were common and highly impairing. The current investigation builds upon his ongoing interests in the development of novel treatments for ADHD and co-traveling symptoms, such as emotional dysregulation.
Background
Adult Attention Deficit Hyperactivity Disorder (ADHD) is a common and highly impairing disorder, with average world-wide and US prevalences of 3.4% and 4.4%, respectively (Fayyad et al., 2007; Kessler et al., 2006). Although many patients respond to stimulant and non-stimulant pharmacotherapy, a significant percentage do not and there are concerns about side effects and misuse and diversion of stimulant medications (Anbarasan et al., 2022); this highlights the need for a safe and effective non-pharmacologic intervention in the treatment of adults with ADHD. NeuroFeedback (NF) has been investigated as a potential non-pharmacologic treatment for ADHD for several decades. EEG based NF uses feedback from certain brain regions or brain wave ratios to attempt amelioration of ADHD symptoms; examples include sensorimotor-rhythm (SMR) NF and theta-beta wave ratio (TBR) NF from frontal or central midline electrodes (Arnold et al., 2021; Cortese et al., 2016). These forms of traditional NF have generally found modest effect sizes in children with ADHD (Arnold et al., 2021); however, a meta-analysis from Cortese et al. of traditional NF in ADHD found that positive effects were smaller when raters were blinded, or sham controls were used (Cortese et al., 2016). Furthermore, a recent larger study of 142 children with ADHD aged 7–10 treated with TBR NF versus sham NF found no significant differences in effects treatment between NF or sham NF at the end of treatment or at 13-month follow-up (Arnold et al., 2021).
However, it should be noted that these studies of NF targeted DSM core symptoms of Inattention (IA) and Hyperactivity-Impulsivity (HI) in ADHD via SMR or TBR feedback. Symptoms of emotional dysregulation (ED) commonly co-travel in adults with ADHD; these symptoms include symptoms of over-emotionality, changeable mood, feeling easily hassled or overwhelmed and having one’s feelings easily hurt when criticized (L. A. Adler et al., 2017). These symptoms also tend to be less responsive to traditional pharmacotherapies than core (IA and H-I) ADHD symptoms (L. A. Adler et al., 2013). The amygdala has been shown to be a key area in the limbic system to regulate emotions and affect (Aday et al., 2017). NF guided by amygdala-targeted fMRI-EEG-Pattern (EFP NF) is an intervention that is designed to downregulate amygdala activity and therefore target symptoms of ED (Keynan et al., 2019).
Prior studies have shown efficacy of amygdala-targeted NF using functional MRI changes to strengthen functional connectivity between the amygdala and ventromedial prefrontal cortex and improved emotional regulation (Marxen et al., 2016; Paret et al., 2016). However, the practicality of using fMRI-NF in clinical practice is limited given its high costs and limited availability. To address this limitation, Prism EFP NF was developed utilizing machine learning algorithms on simultaneously acquired EEG and fMRI data to create a model of weighted coefficients of the EEG signal that best predicts blood-oxygen level-dependent (BOLD) activity in the amygdala (Meir-Hasson et al., 2014, 2016). Prism EFP has been shown to reflect the amygdala fMRI BOLD activity and thus this intervention relies on only EEG signals recorded from a matrix of electrodes placed over different locations on the scalp to evaluate amygdala related activity and determine the reinforcing feedback during training (Keynan et al., 2016). This intervention has been shown to be effective in other mental health disorders where ED is a major presenting symptom, such as PTSD (Hendler & Adler, 2023; Shani, 2021). In Prism EFP NF, the EFP signal of the amygdala is assessed in real-time during the NF session as the subject engages in an interactive audio-visual interface. This feedback is used to adjust the stimuli, such that the subject is encouraged to engage in behaviors to reduce the amygdala-associated EFP value. Given the limited success of traditional NF therapy in adult ADHD once control groups are included and the difficulty in treating symptoms of ED in adult ADHD as noted above, we conducted an open pilot trial of Prism EFP NF in nine adults with ADHD with total DSM ADHD symptom score on the AISRS as the primary outcome measure. We posit that both ED and traditional core ADHD symptoms may improve through this form of NF.
Methods
NeuroFeedback: Prism EFP NF was delivered via 15 sessions over 8 weeks (where a minimum of 12 sessions was considered treatment completion); each session involved 25 min of training including a three-minute calibration, and then five cycles of NF. A session started with a three-minute baseline calibration and each cycle included a one-minute local baseline (rest) followed by three-minute Neurofeedback (regulate) and 30 s break periods.
Prism is an FDA approved EEG-NF device (GrayMatters Health Ltd, 2023). Prism provides self-neuromodulation training via an amygdala-derived-fMRI-guided statistical model for processing EEG signals. The amygdala-EFP model uses the EEG signal from eight scalp electrodes to produce an amygdala-derived EFP biomarker signal. Prism interprets the real-time EEG signal to compute the amygdala-EFP biomarker during a training session; this signal is used in real time to control an audio-visual interface displayed on a computer monitor of a noisy/distressing medical waiting room with avatar patients who become agitated and approach the receptionist in an angry manner. The training results in the subject learning to downregulate the amygdala-EFP biomarker, such that the avatars relax and sit down (ClinicalTrials.gov NCT04891614) (Hendler & Adler, 2023).
Patients with stable psychiatric comorbidities, excluding bipolar disorder or psychotic disorders, were allowed to participate. If patients were on psychiatric medications, they were held constant for the duration of the trial.
Ratings: DSM-5 Adult ADHD was confirmed at screening via administration of the Adult ADHD Clinician Diagnostic Scale (ACDS) v1.2. Clinician ratings of Total ADHD Symptoms (IA + HI) and ADHD ED symptoms were obtained via the Adult ADHD Investigator Symptom Rating Scale (AISRS-Expanded). Participant self-reports of Executive Function Deficits (Overall: Global Executive Composite—GEC) and Emotional Dysregulation Symptoms (Behavior Regulation Index—BRI) were obtained via the Behavior Rating Inventory of Executive Function-Adult (BRIEF-A) Scale. Impairment was measured via the Clinical Global Impression Scale- Severity (CGI-S). These scales were obtained weekly during the 9-week protocol which included screening, Prism EFP NF baseline followed by eight weekly sessions, and a 2-weeks period without treatment.
Suicidality was assessed using the Columbia-Suicide Severity Rating Scale (C-SSRS). Participant demographics, medical/psychiatric histories, and medications were self-reported.
The ability to regulate the amygdala-EFP signal was examined via changes in the active regulation score (µv²). Active regulation score measures the EFP activity level when the patient is successfully lowering the EFP signal in the neurofeedback training below the activity level recorded at baseline. As mentioned above, each session contains five cycles that leads to five active regulation scores. To trace the dynamics of the EFP signal regulation, the treatment was divided into four periods. The first session was used as baseline to determine the subject’s initial ability to regulate the EFP. The beginning consisted of sessions 2 to 5, the middle comprised of sessions 6 to 9, and the end consisted of sessions 10 to 13. For each period, the active regulation average across cycles and sessions was determined.
The study was conducted in outpatients at the NYU Grossman School of Medicine with approval of the IRB at the School of Medicine. All clinical assessments were conducted remotely via secure tele-video administration of scales, while all safety assessments and Prism EFP NF sessions were performed with study personnel in person. All clinical assessments were administered by a board-certified psychiatrist with over 5 years’ experience in adult ADHD research (LAA or DA). Participants gave written informed consent to participate prior to enrollment.
Adult ADHD Clinical Diagnostic Scale (ACDS) v1.2
The diagnosis of Adult ADHD was determined using the Adult ADHD Clinical Diagnostic Scale v1.2 (L. A. Adler et al., 2015; L. Adler & Cohen, 2004). It is a semi-structured diagnostic interview designed to evaluate both childhood and recent (past year) adult ADHD symptoms. This tool is widely recognized to capture ADHD symptoms, including all DSM-5 criteria A1 and A2 symptoms, employing developmentally appropriate prompts and questions. The symptom severity is rated 1 (never) to 4 (severe). The scale provides a binary “yes” or “no” diagnosis of DSM-5 adult ADHD and also identifies the presentation type (L. A. Adler et al., 2015; L. Adler & Cohen, 2004).
The Adult ADHD Investigator Symptom Rating Scale (AISRS)
The AISRS, a validated measure for treatment efficacy, is utilized to assess ADHD symptoms (Meunier et al., 2021; Spencer et al., 2010). It encompasses 18 items aligned with the DSM-5 criteria for inattentive (IA) and hyperactive-impulsive (HI) domains. It is designed as a semi-structured interview with suggested prompts for each symptom for adults. Ratings are assigned on a 4-point scale with 0—absent, 1—mild, 2—moderate, and 3—severe. These scores are categorized into two domains: IA and HI, with a maximum score of 27 points each. The primary outcome measure for this trial is the total score of DSM ADHD symptoms (IA + HI)—the total DSM ADHD symptom score, which has served as an indicator of treatment response in prior studies. The scale has been expanded to contain 13 additional items: nine items of executive function deficits (EFD) and four items of ED (L. A. Adler et al., 2009; Meunier et al., 2021; Silverstein et al., 2019; Spencer et al., 2010).
Behavior Rating Inventory of Executive Function—Adult Version (BRIEF-A)
The Brief-A is a standardized self-report assessment tool that has been validated for evaluating executive function in adults (Roth et al., 2005). It consists of 75 items and is structured around three main scales: The Metacognition Index (MI), The Behavioral Regulation Index (BRI), and The Global Executive Complex (GEC). Within these scales, there are nine clinical subscales. Of note, the BRI contains a subscale on emotional regulation. The GEC score is calculated by combining the scores from all nine subscales. Raw scores are converted into T-scores, which provide insight into a person’s level of executive functioning (Roth et al., 2005). T-scores equal to or greater than 65 indicate clinically significant impairment.
The Clinical Global Impression Scale Severity (CGI-S)
The CGI-S is a commonly utilized clinical evaluation tool for assessing the severity of ADHD symptoms. The impairment is scored on a seven-point Likert scale where a score of 1 signifies normal functioning while a score of 7 indicates the most severe impairment (Guy, 1976).
The Columbia Suicide Severity Rating Scale (C-SSRS)
The C-SSRS is a scale designed to assess the presence of suicidal ideation or behaviors and immediacy of suicide risk (Posner et al., 2011).
Participants: Nine subjects participated and ranged in age from 25 to 54 years (mean = 33.0, 8.8 SD years, seven Females, seven White, one Asian, and one Hispanic). Eight had combined presentation ADHD, while one had primarily inattentive presentation. Seven patients did not have concomitant psychiatric disorders; two had major depression in remission and were on stable doses of SSRIs which were held constant throughout the trial. Five participants were not taking ADHD medications during the trial; one participant was taking atomoxetine and buspirone. Another subject was taking lisdexamfetamine and two others were taking mixed amphetamine salts. Doses of ADHD medications were held constant throughout the trial. Seven participants completed the trial. One subject dropped out after week 5 because of inability to attend future visits; another dropped out after week 7 because of a pending change in ADHD medications.
Data Analyses: The effects of treatment were assessed by calculating means and standard deviations with their 95% confidence intervals (CIs) on the primary and secondary outcome measures and determining the changes in these measures from baseline to End of Treatment (EoT). The last visit in treatment was utilized as the final visit. Missing data was handled via last observation carried forward. Active regulation scores were analyzed via two-sided Wilcoxon tests comparing the active regulation score to the first session. As two participants did not complete the follow-up phase of protocol, these data were not included in analyses but given the small numbers will be clinically described.
Results
Participants were able to successfully moderate the amygdala-EFP signal: The Active regulation score decreased by −0.8 in the first session; by −1.8 in beginning (sessions 2–5) and mid (sessions 6–9); and by −2.25 at end sessions (sessions 10–13) (first to end sessions p < .016, other changes NS). Reduction of the active regulation score over time indicates that participants were successful in performing Prism EFP NF (Figure 1). There were significant reductions in ADHD symptoms (AISRS DSM Total Score—the primary outcome measure), self and clinician—reported EFD symptoms (AISRS EFD Score, BRIEF GEC T-SCORE) and ED Symptoms (AISRS ED Score, BRIEF BRI T-SCORE), respectively and clinician rated impairment (CGI-S) from Baseline to EoT (see Table 1). Six of the seven participants who completed the follow-up phase maintained improvement in their EoT clinical ratings but saw some waning of the improvement over time. One participant was able to maintain a similar level of improvement during this generalization phase. No significant adverse events, including suicidality, were observed during the trial.
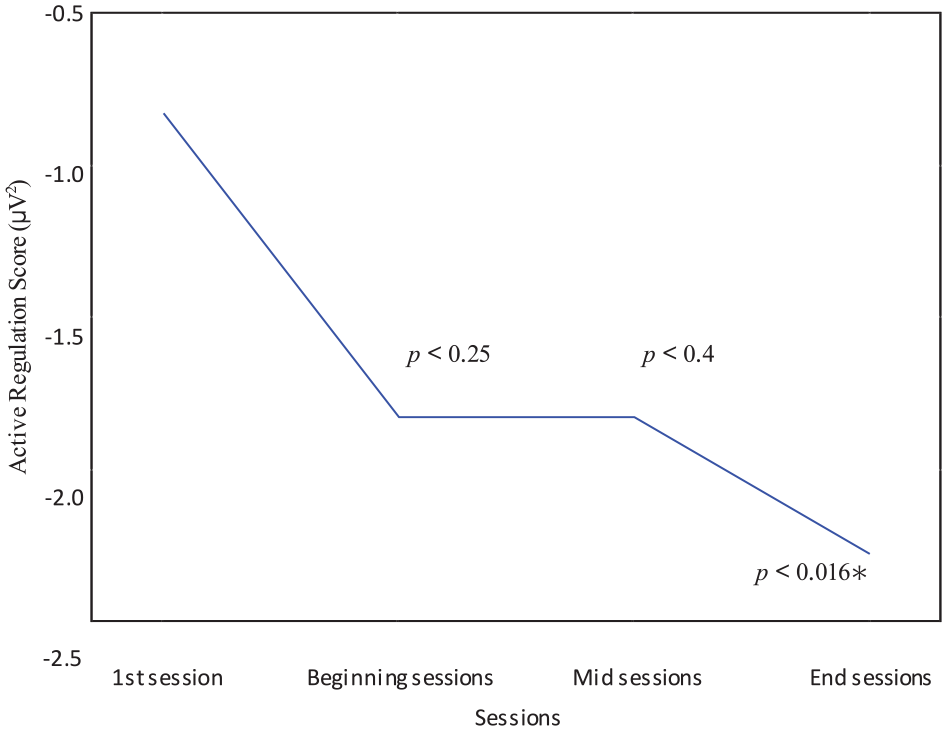
Regulation of Amygdala-derived EFP signal.
Mean Clinical Measure Scores at Baseline and End of Treatment with Confidence Intervals.
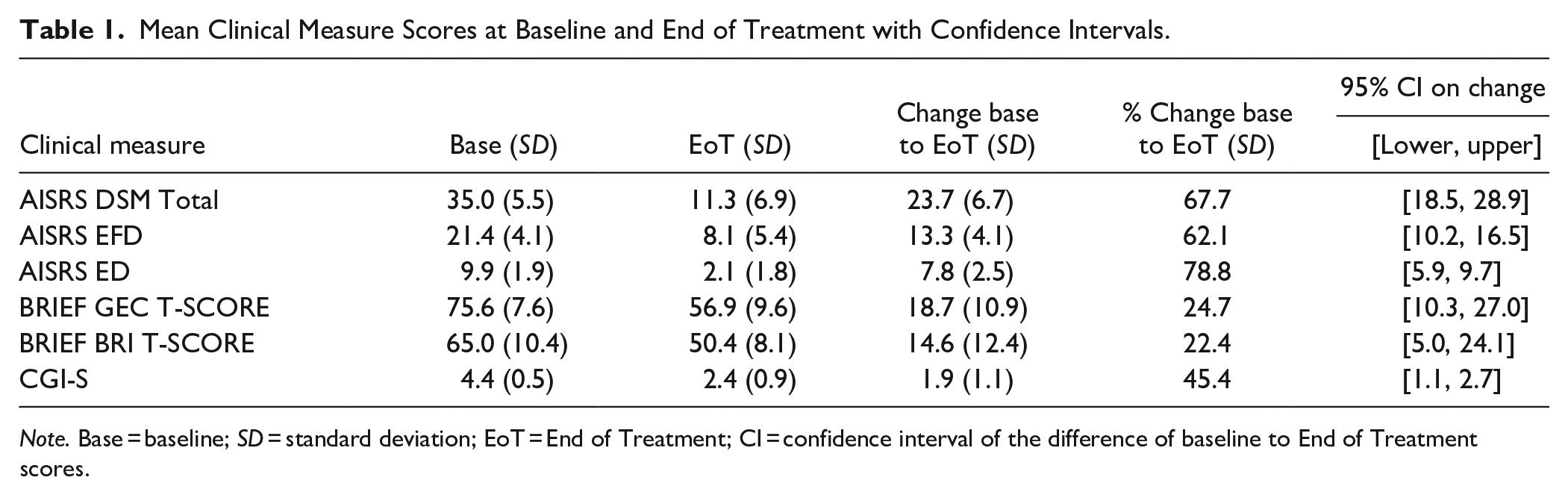
Note. Base = baseline; SD = standard deviation; EoT = End of Treatment; CI = confidence interval of the difference of baseline to End of Treatment scores.
Conclusions
This pilot study of Prism EFP NF in adults with ADHD showed significant improvement in overall ADHD symptoms, emotional dysregulation (both clinician and self-report), executive function, and impairment in nine participants. The magnitude of improvement (68%) from baseline to EoT on the primary outcome measure, the AISRS DSM Total ADHD symptom score, was larger than seen in trials of non-stimulant selective norepinephrine re-uptake inhibitors like atomoxetine (L. A. Adler et al., 2009) and viloxazine (Nasser et al., 2021), although these non-stimulant trials were conducted on larger samples and under more controlled conditions. The improvement was within the range of symptomatic improvement reported in stimulant trials in adult ADHD (Cortese et al., 2018). Four of the nine participants were on stable doses of ADHD medications throughout the trial; the magnitude of response total DSM ADHD scores in these participants was similar to those not on medication. However, definitive conclusions regarding potential effects of concomitant use of ADHD psychotropic medications cannot be made, given the small sample sizes.
Interpretation of these results should be viewed with caution given the pilot nature, small sample size and absence of comparator or control (sham) groups in this trial; comparator or sham controls would have added significantly greater ability to understand the applicability of these results (Cortese et al., 2016; Keynan et al., 2019). Of note, if similar control effects were noted with Prism EFP NF as with other NF methodologies in ADHD, a substantial portion of the improvement noted might be removed when accounting for the true effect size of treatment, as sham effects can yield up to 25% improvement (Cortese et al., 2020). Potential confounders of the small sample (leading to sampling bias) and high expectation bias for the participants given the substantial amount of time they spent in the clinic receiving what they perceived as a novel treatment during this trial must be noted; the issue of expectation bias contributing to potential placebo effects in ADHD trials has been established (Faraone et al., 2022) and may a factor in the larger effect noted. There is also a potential issue of pseudo-specificity in that what was being measured as changes in ADHD related ED may have not been specific to ADHD. Finally, changes noted in ED subscale of the AISRS were larger than those reported in the meta-analysis of the effects of stimulants and atomoxetine on emotional lability in adults by Moukhtarian et al. (2017). Of note, the participant reported ED changes on the BRIEF BRI T-Score was substantially smaller than those seen on the AISRS ED subscale (circa ¼ the size); potential contributing factors to this difference could be scale differences (there are only four items on the AISRS subscale) versus reporter bias. The AISRS is an investigator scale, while the BRIEF-A is a self-report one.
This trial, as compared to prior trials of NF in adult ADHD, used NF derived from EFP feedback on amygdala downregulation targeting ED, which is a novel approach in NF in adult ADHD. The fact that this study employed a mechanism of NF which focused on emotional regulation might have been critical to the positive results seen in this study, while prior studies of EEG NF in ADHD have not been shown to be consistently efficacious (Arnold et al., 2021; Cortese et al., 2016). The participants in this study all loaded significantly for emotional dysregulation on both clinician and self-report measures, which highlighted that this form of NF which focusses on amygdala downregulation may not be suitable for all patients with adult ADHD. A factor analysis found that although ED is a common co-occurring and impairing symptom in adult ADHD, it is not present in all patients, and when present, does not always load equally in terms of ADHD core IA and HI symptom burden (Arnold et al., 2021). Finally, the approach of treating ADHD core symptoms via focusing on the treatment of a co-traveling symptom set such as ED is somewhat unique. It should be noted that the antidepressant vortioxetine, which has been shown to improve the co-traveling symptoms of executive function deficits in patients with depression, was examined in a failed placebo-controlled trial in adults with ADHD (Biederman et al., 2019).
Future planned studies include a larger trial Prism EFP NF in adult ADHD, utilizing a more varied patient sample and a sham control to further examine the breadth of the effect of Prism EFP NF under more controlled settings. We also intend to examine the persistence of the effect after conclusion of the treatment paradigm and the correlation of changes in ADHD symptoms with the active regulation index in order to examine the relationship between Prism EFP NF measures and ADHD symptom change.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lenard A. Adler MD has the following disclosures over the last 3 years: Grant/Research support to NYU Grossman School of Medicine from Shire/Takeda, Otsuka Pharmaceuticals, Corium; Consultant to Supernus Pharmaceuticals, Bracket/Signant, SUNY, Neurocentria, National Football League, Major League Baseball, Otsuka; Royalty payments (as inventor) from NYU Grossman School of Medicine for license of adult ADHD scales and training materials since 2004.; Charles R Marmar MD serves on Advisory Board of Receptor Life Sciences, Otsuka Pharmaceuticals and Roche Products Limited. He has the following disclosures over the last 3 years: National Institute on Alcohol Abuse and Alcoholism, National Institute of Mental Health, Department of Defense- CDMRP US Army Research Office (DARPA), Bank of America Foundation, Brockman Foundation, McCormick Foundation, Home Depot Foundation, New York City Council, New York State Health, Mother Cabrini Foundation, Tilray Pharmaceutical, Ananda Scientific.; Talma Hendler MD PhD is an employee of GrayMatters Health that has patent owned PRISM software provided for the study. Dr. Hendler has stock options as an employee and innovator for GrayMatters.; Yaakov Stern PhD is an employee of GrayMatters Health, which provided the PRISM software for this research.; Oded Kraft is a co-founder and the CEO of GrayMatters Health, which provided the PRISM software for this research.; Deepti Anbarasan MD declared no potential conflicts of interest in the last 3 years.; Dayeon Cho declared no potential conflicts of interest in the last 3 years.; Terry L. Leon declared no potential conflicts of interest in the last 3 years.; Taylor Sardoff declared no potential conflicts of interest in the last 3 years.; Olivia Descorbeth declared no potential conflicts of interest in the last 3 years.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Investigation funded through philanthropic gift to Department of Psychiatry, Adult ADHD Program, NYU Grossman School of Medicine; software provided by GrayMatters Health.