
Abstract
Objective:
To explore outcomes of stimulant treatment for ADHD in pediatric populations with particular attention to bipolar disorder (BPD).
Method:
We conducted a literature search of PubMed articles published prior to August 25, 2022 that focused on BPD, mania, and psychosis prior to, or as result of, stimulant treatment. We excluded studies: (1) unrelated to stimulants, (2) general stimulant research, (3) articles older than 40 years, (4) study protocols, or (5) case reports.
Results:
A total of 11 articles met all inclusion/exclusion criteria. Some reports found stimulant treatment safe and well-tolerated in children with comorbid BPD and ADHD. Others found evidence of treatment-emergent mania (TEM), discontinuation, and other adverse events with stimulant treatment.
Conclusion:
Poor outcomes associated with stimulant treatment in pediatric populations with BPD necessitate work to identify patients at risk of serious stimulant-related adverse events. Our results were limited by automated search filters and a pediatric, primarily male sample.
Introduction
Stimulants are generally the first line treatment for attention-deficit hyperactivity disorder (ADHD). Stimulants are a prescription drug class that increase the synaptic availability of dopamine by targeting the dopamine transporter (NDA, 2018). Commonly used drugs in this class include variants of amphetamine and methylphenidate (MPH; Biederman & Spencer, 2008; Greenhill et al., 2002). Roughly 2 million stimulant prescriptions are written each year in the United States (Kim et al., 2023).
Stimulants are considered effective in the treatment of ADHD, but little is known about their impact on ADHD when comorbid with bipolar disorder (BPD). ADHD is frequently comorbid with mood disorders. Studies report that between 5% and 47% of children with ADHD have comorbid major depressive disorder (MDD; Diler et al., 2007; Pliszka, 1998; Wilens et al., 2002), and 18% to 20% of school-age children with ADHD have comorbid BPD (Biederman et al., 2004; Wilens et al., 2002; Wozniak et al., 1995). Longitudinal studies demonstrate that children with ADHD may go on to develop these mood disorders as well as psychotic disorders during the course of treatment (Biederman et al., 2006). The association of ADHD with BPD is due, in part, to shared genetics as indicated by family studies (Althoff et al., 2005; Biederman et al., 2013; Faraone et al., 1997, 2012) and genome-wide association studies (Demontis et al., 2023; van Hulzen et al., 2016), but can occur pharmacologically induced and is a predictor of switch.
In general, stimulants have been shown to be exceedingly effective, safe, and well-tolerated for treating children and adults with ADHD (Biederman et al., 2006; Riera et al., 2017; Spencer et al., 2005); however, serious adverse events have been reported. The U.S. Food and Drug Administration (FDA) conducted a review of controlled trials for prescription stimulants in 2006. They found stimulant-associated psychotic events that were rare but seriously impairing (1.48 per 100 person-years, 95% CI: 0.74–2.65 per 100 person-years). The FDA review led to the addition of a warning about psychosis on stimulant labels in 2007 (Mosholder et al., 2009). The label also warns that stimulants may cause treatment-emergent psychotic or manic symptoms in patients with no prior history, or exacerbation of symptoms in patients with pre-existing psychosis. Other literature has also identified occurrences of new-onset psychosis in adolescents and young adults due to stimulant treatment (Moran et al., 2019). High comorbidity of psychiatric disorders, particularly ADHD and BPD, may affect the potential for adverse events such as psychosis, exacerbation of mania, or treatment-emergent mania (TEM) with stimulant treatment. The impact of stimulant treatment on causing or exacerbating BPD is unknown.
Although stimulants are widely prescribed and have a strong safety and efficacy record (Boland et al., 2020; Faraone et al., 2006; Fredriksen et al., 2013), little is known about those at risk for severe adverse outcomes including exacerbation of mania, TEM, and psychosis. To this end, we conducted a systematic literature review that aimed to investigate what is currently known about these serious adverse events after stimulant treatment in pediatric populations with ADHD and with or without pre-existing BPD.
Methods
Literature Search
We performed a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) systematic review to identify peer-reviewed articles that examined the relationship between stimulant treatment and adverse mood events and/or psychosis. We searched the PubMed electronic database using automated search filters, limiting our search to clinical trials, randomized-control trials, and meta-analyses published prior to August 25, 2022. See Supplemental Material for the search terms used (S1).
Selection Criteria
Two authors (H.O. and J.W.) screened the titles and abstracts of all articles for relevance and eligibility. We included studies that examined activation/manic switch or poor outcomes in pediatric patients who were prescribed stimulants or participated in a trial of stimulants. The following exclusion criteria were applied: (1) unrelated to stimulants, (2) general stimulant research, (3) articles older than 40 years, (4) study protocols, or (5) case reports. The authors then further screened the articles through assessing the full text for relevance. In addition to the database search, authors H.O. and J.W. identified and selected additional individual articles by reviewing the references of articles identified in the database search and assessing them for inclusion using the same criteria.
Data Extraction
Data were extracted from the quantitative studies using a standardized extraction form designed for this review by author H.O. Data extracted included: aim of investigation, sample (population age group, gender makeup of sample, sample size, and clinical diagnosis of study population, when provided), methods, and main findings.
Results
Identified Articles
As seen in Figure 1 (Haddaway et al., 2022), our PubMed search resulted in 5,657 articles. After using PubMed’s automated selection filters (specifically “Clinical Trial,” “Randomized Control Trial,” and “Meta-Analysis”), we identified a total of 257 unique articles for screening. After a preliminary screen of titles, 218 of the 257 articles were excluded and 39 articles were identified for further review. After assessing articles for eligibility according to pre-determined inclusion and exclusion criteria, a total of two articles from the literature search met all criteria. Excluded were: (1) articles unrelated to stimulants (n = 5), (2) general stimulant research (n = 28), (3) articles older than 40 years (n = 3), (4) study protocols (n = 1), and (5) case reports (n = 0).
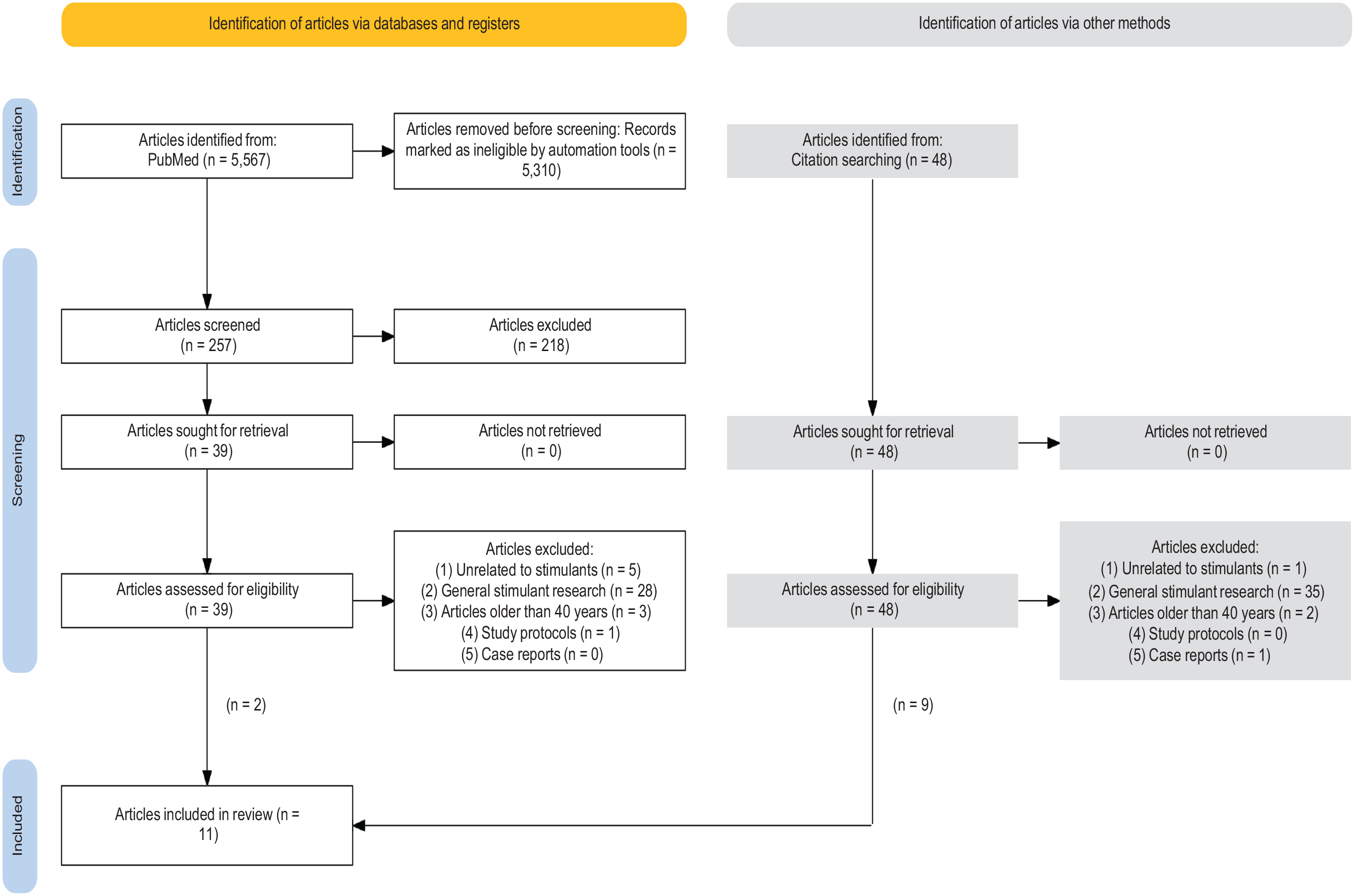
PRISMA flowchart.
Forty-eight additional articles were identified via reference lists as potentially relevant and retrieved for review. Of these 48 articles, 39 articles were excluded for the following reasons: (1) articles unrelated to stimulants (n = 1), (2) general stimulant research (n = 35), (3) articles older than 40 years (n = 2), (4) study protocols (n = 0), and (5) case reports (n = 1). From articles identified from reference lists, nine articles met all inclusion criteria. Across both search methods, a total of 11 articles met inclusion and exclusion criteria and were included in the literature review (see Table 1).
Outcomes Associated With Stimulant Treatment in Children and Adolescents.

Note. MPH = methylphenidate; BPD = bipolar disorder; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders Fourth Edition; ARS-IV = ADHD Rating Scale-IV; CDRS-R = Children’s Depression Rating Scale, Revised; YMRS = Young Mania Rating Scale; AEs = adverse events; ARP = aripiprazole; SNAP-IV = Swanson, Nolan, and Pehlham Teacher and Parent Rating Scale-IV; ASD = autism spectrum disorder; FDA = U.S. Food and Drug Administration; DISC = dominance, influence, steadiness, and conscientiousness assessment; CBCL = child behavior checklist; CLAM = Conners, Loney, and Milich Scale for ADHD; TEM = treatment-emergent mania.
From formal literature search.
Individually collected article.
The studies included in this review focused on pediatric or adolescent populations with an age range of 3 to 19 years old (Brikell et al., 2021; DelBello et al., 2001; Faedda et al., 2004; Findling et al., 2007; Froehlich et al., 2020; Galanter et al., 2003; Madjar et al., 2019; Mosholder et al., 2009; Soutullo et al., 2002; Wigal et al., 2006; Zeni et al., 2009). Ten of the 11 studies provided information regarding gender of the sample. All of these samples were predominantly male: 75% (Findling et al., 2007), 64.3% (Zeni et al., 2009), 71% (Brikell et al., 2021), 86.9% (Madjar et al., 2019), 80.4% (Galanter et al., 2003), 65.9% (Faedda et al., 2004), 73.5% (DelBello et al., 2001), 63.5% (Soutullo et al., 2002), 73% (Wigal et al., 2006), and 71% (Froehlich et al., 2020), respectively. Sample sizes in the articles ranged from N = 16 to 9,133 individuals.
Two studies examined patients with comorbid pediatric BPD and ADHD (Findling et al., 2007; Zeni et al., 2009). Three studies examined patients with a diagnosis of pediatric BPD (DelBello et al., 2001; Faedda et al., 2004; Soutullo et al., 2002) and six studies examined patients with a diagnosis of ADHD (Brikell et al., 2021; Froehlich et al., 2020; Galanter et al., 2003; Madjar et al., 2019; Mosholder et al., 2009; Wigal et al., 2006). Of the six ADHD studies, one included patients with symptoms of mania that were not necessarily within the threshold of BPD diagnosis (Galanter et al., 2003) and one included a patient sample where 52% had comorbid oppositional defiant disorder (ODD; Wigal et al., 2006).
Effects of stimulants in these populations were assessed through a variety of methods and outcomes across the 11 studies. Our review examined the occurrence of treatment-emergent mania (TEM), psychosis, or activation, as well as other potential indicators of poor response to stimulant treatment including stimulant discontinuation, switch to new treatment, and poor adherence.
Studies Examining Populations With ADHD
Six of the 11 studies examined stimulant-related outcomes in general ADHD populations (Brikell et al., 2021; Froehlich et al., 2020; Galanter et al., 2003; Madjar et al., 2019; Mosholder et al., 2009; Wigal et al., 2006). Three of these examined stimulant-related adverse events in general. One study examining clinical trial data submitted to the FDA found a total of 11 total psychosis/mania adverse events reported across 49 randomized control trials of ADHD medications. There were no adverse events reported for individuals receiving a placebo in the same trials. Additionally, 865 case reports from the FDA Adverse Event Reporting System safety database identified symptoms of psychosis or mania from drugs used for ADHD treatment, with 90% of these cases having no prior history of a related psychiatric condition (Mosholder et al., 2009). In a treatment study examining the safety and tolerability of MPH, 30% of parents reported moderate to severe adverse events with irritability as the most common adverse event (Wigal et al., 2006).
Three of the 11 studies included in this review examined rates of discontinuation or switch following treatment. In one study of children with ADHD who initiated stimulant treatment, 45% (n = 3,370) discontinued and 15% (n = 1,137) switched to non-stimulants (Brikell et al., 2021). Additionally, polygenic risk scores of BPD and schizophrenia were associated with discontinuation of stimulants (Brikell et al., 2021). Another study found that in children with ADHD prescribed MPH between ages 6 and 8 years, 74.5% had a drug adherence below 50% (Madjar et al., 2019). Furthermore, of this sample of children, those who were prescribed antipsychotics were more likely to have higher adherence for MPH in childhood and were more likely to be prescribed antidepressants between ages 12 and 18 years (Madjar et al., 2019). In one treatment study, 11% of the MPH-treated group had to discontinue due to adverse events which included emotional outbursts and irritability (Wigal et al., 2006).
Of the six studies examining general ADHD populations, one study examined the effect of pre-existing comorbid emotional symptoms in children with ADHD treated with MPH (Froehlich et al., 2020). In this crossover trial of MPH, stimulant-naïve children ages 7 to 11 years were monitored for short-term adverse effects. Children with high symptoms of anxiety/depression at baseline continued to experience these symptoms after MPH treatment but decreased in their ratings of irritability compared to baseline. Paradoxically, children with low symptoms of anxiety/depression and low symptoms of ODD experienced higher levels of irritability after MPH treatment (Froehlich et al., 2020). Another study examined children with ADHD with and without mania symptoms defined by proxy (DISC mania proxy, 10% of sample, n = 29, and CBCL mania proxy, 11.1% of sample, n = 32) and found that the children with these symptoms were not significantly more likely to experience adverse events than children with ADHD without mania symptoms. However, in this study, four children did experience stimulant-related adverse events which included emotional constriction, buccal movements, skin picking, depressed mood, crying, appetite loss, and listlessness (Galanter et al., 2003).
Studies Examining Populations With BPD
Three studies in our review examined samples of children with pediatric BPD (DelBello et al., 2001; Faedda et al., 2004; Soutullo et al., 2002). Two of these studies found that adolescents with BPD who were exposed to stimulants had a significantly earlier age of onset of BPD compared to those without stimulant exposure (10.7 years vs. 13.9 years; DelBello et al., 2001 and 13.7 years vs. 15.1 years; Soutullo et al., 2002, respectively). DelBello et al. (2001) found younger age of onset of BPD following exposure to more than one stimulant. In addition, Soutullo et al. (2002) found that adolescents with BPD who were exposed to stimulants had a significantly more severe overall course of illness during hospitalization (as defined by length of stay, need for pro re nata (PRN) medication, and seclusion and restraint orders) compared to those without history of exposure.
The third study found significant TEM associated with stimulants (Faedda et al., 2004). This study included children with BPD treated with antidepressants or stimulants and reported TEM in 35 of the 69 children exposed to any psychoactive agent, with 75.7% of the cases associated with antidepressants and 24.2% associated with stimulant use. Additionally, the risk of TEM was twice as likely in girls than boys and more likely in younger patients, for both stimulant and antidepressant use (Faedda et al., 2004).
Studies Examining Populations With ADHD and BPD
Two studies in our review had samples of comorbid pediatric BPD and ADHD and looked specifically at MPH as a stimulant treatment in patients with stabilized BPD (Findling et al., 2007; Zeni et al., 2009). Neither of these two studies observed poor outcomes of stimulants, and both studies found that the drug was well-tolerated without TEM, worsening of mood, or psychosis. Neither study found a significant treatment effect of MPH in the number of adverse events (Findling et al., 2007; Zeni et al., 2009). MPH treatment was not effective for symptoms of BPD or MDD as measured by clinician ratings (Findling et al., 2007; Zeni et al., 2009); however, a significant treatment response for depressive symptoms according to patient self-report on the Kutcher Adolescent Depression Scale (KADS) was reported in one study (Zeni et al., 2009).
Discussion
The aim of this review was to explore whether stimulant treatment exacerbates or causes BPD. We examined poor outcomes of stimulant treatment including TEM, psychosis, or activation in pediatric populations. Our systematic literature search resulted in only 11 articles. Given the stimulant label warnings, the severity of psychosis or TEM as an outcome, the high rate of comorbidity of ADHD with mood disorders, and the high number of stimulant prescriptions each year, this review demonstrates a substantial gap in the literature. Clinicians look to the evidence base to help determine when it is safe to prescribe a stimulant to a child with BPD as well as predictors for which children with ADHD and without BPD will experience TEM or psychosis as an outcome. The scarcity of available articles on this topic highlights the need for additional research investigating outcomes of stimulant treatment in pediatric populations.
Our literature search identified only five articles that reported on stimulant outcomes in children with pre-existing BPD (DelBello et al., 2001; Faedda et al., 2004; Findling et al., 2007; Soutullo et al., 2002; Zeni et al., 2009). Children with ADHD have high rates of comorbidity with mood disorders: 5% to 47% with MDD and 18% with BPD (Diler et al., 2007; Pliszka, 1998; Wilens et al., 2002). Although prescription stimulants including MPH and various dextroamphetamines are well-tolerated and effective with limited overall side effects (Biederman & Spencer, 2008), few articles address their safety and efficacy in children with ADHD and comorbid BPD. Pediatric MDD and BPD are best treated with antidepressants and mood stabilizers, respectively (Kupfer, 2005), and may worsen when treated with stimulants. Considering the significant prevalence of children with ADHD and comorbid mood disorders, additional research regarding the tolerability of stimulant treatment for pediatric patients with both ADHD and BPD would improve patient safety.
In 2007, the FDA collected adverse events reported after treatment with stimulants and found a significant enough number of cases to issue a warning label for inclusion on stimulant prescriptions moving forward (Mosholder et al., 2009). There is additional support for caution in the use of stimulants from individual clinical case studies (Chakraborty & Grover, 2011; Henning et al., 2019; Koehler-Troy et al., 1986). For example, in one study, a child with ADHD experienced psychotic and manic-like symptoms after the initiation of MPH (Ross, 2006).
Two studies of populations with ADHD investigated the impact of pre-existing mood and anxiety symptoms on stimulant response. Galanter et al. (2003) found that children with mood symptoms as defined by proxy measures were not significantly more likely to have adverse outcomes after stimulant treatment, but four children did experience adverse events including emotionality. Froehlich et al. (2020) paradoxically found that children without pre-existing mood and anxiety symptoms were more likely to experience irritability as an outcome of stimulant treatment. The literature suggests that pre-existing characteristics such as personality and stress level could potentially influence response to stimulant treatment (Corr & Kumari, 2000; Hamidovic et al., 2010). Studies attending to features that predict poor outcome with stimulant treatment would be useful for clinical practice.
Only two of the included studies indicated that MPH had no significant negative mood outcomes, specifically for youth with comorbid BPD and ADHD (Findling et al., 2007; Zeni et al., 2009). However, in both trials BPD was well stabilized prior to the addition of stimulant medication, which may not be common in clinical practice. The importance of BPD stability prior to treatment with stimulants is supported by a large retrospective study reporting that among adults with untreated BPD, relative risk of mania significantly increases in the first 3 months after initiation of MPH monotherapy (Viktorin et al., 2017).
The three studies addressing stimulant use in children with BPD reported concerning adverse outcomes. Faedda et al. (2004) found that TEM as a result of stimulant use was reported to be significantly more likely in youth with BPD, although TEM occurred at a lower rate than with antidepressant use. This finding is consistent with substantial prior evidence of antidepressant use as a precursor to emergent mania (Baumer et al., 2006; Bhowmik et al., 2014); however, a small amount of evidence suggests the same serious adverse outcomes can occur with stimulant treatment. Two of our studies found that children with BPD who were treated with stimulants had an earlier age of onset of BPD (DelBello et al., 2001; Soutullo et al., 2002), and one of these two studies found an earlier age of onset in children who received more than one stimulant medication (Soutullo et al., 2002), suggesting that stimulant use can accelerate the course of BPD in children in a dose-related manner. As reported in adults, children with early onset BPD treated with stimulants rather than mood stabilizers could develop a worsening course and potential treatment resistance (Post et al., 2010).
Stimulant discontinuation was reported as an outcome in three of the studies in the review (Brikell et al., 2021; Madjar et al., 2019; Wigal et al., 2006). While not in itself a proxy for TEM, the most commonly reported reason for medication discontinuation is resultant adverse effects (Gajria et al., 2014; Roborel de Climens et al., 2020). Wigal et al. (2006) indicated that 11% discontinued stimulants due to emotional outbursts and irritability. Brikell et al. (2021) found that polygenic risk scores of BPD were associated with stimulant discontinuation. Madjar et al. (2019) reported a high percentage of children with low MPH drug adherence and noted that those who were prescribed antipsychotics were more likely to have higher stimulant adherence and those with high stimulant adherence were more likely to later be prescribed antidepressants, raising the question as to whether stimulant side effects were treated with additional medications for mood symptoms.
In a study of N = 9,341 children with ADHD which was not included in our review, investigators examined treatment plans across a 1-year period and reported that 18.7% switched away from stimulants and 5.5% of those patients switched to atypical antipsychotics (Ben Amor et al., 2014). Out of the 9,341 patients, 23.6% had documented psychiatric or neurological comorbidities. When looking just at the group with comorbidities, the prevalence of switching away from stimulants was 31.6% and 11.5% of those patients switched to atypical antipsychotics (Ben Amor et al., 2014). In this study, switching to antipsychotic medication was not rare. A substantial minority of patients, especially those with comorbidity, switched from stimulants to antipsychotics, suggesting emergent symptoms of mania and/or psychosis. Future studies of stimulant use would benefit from studying discontinuation rates, subsequent treatments, and reasons for switch.
Taken together, the majority of studies included in this review support vigilance for symptoms of mania when prescribing stimulants, in pediatric populations both with and without pre-existing BPD. This limited evidence indicates that stimulant use in populations with comorbid BPD or mood dysregulation, as well as those without, could lead to serious adverse events, TEM, and discontinuation, and is enough to merit further research in this area.
This review should be viewed in the context of its limitations. We used automatic filters through the PubMed database which may have missed articles that could be relevant to our review. We did not preregister our search through PROSPERO (prospectively registered systematic review) which may have reduced our bias. The included articles had primarily male samples which hinders the generalizability of our findings. We included articles solely pediatric populations, although whether or not stimulants can cause or exacerbate BPD in adults is also an important issue. Our review did not address whether TEM as a stimulant side effect would resolve or result in ongoing BPD. Due to the small number of articles we were able to identify, our review combines individual clinical trials with larger meta-analyses, and thus not all reports included carry comparable weight and quality.
Our findings indicate the need for more work on the adverse outcomes of stimulants in causing or exacerbating BPD. While we found evidence that stimulant treatment can be both effective and well-tolerated in pediatric populations with stabilized BPD, most of the articles we found reported concerning evidence of TEM in patients both with and without pre-existing BPD. Given the limited number of articles we were able to collect for this review, more research is needed to guide clinicians in their treatment decision to safely use stimulant medication in pediatric patients.
Supplemental Material
sj-docx-1-jad-10.1177_10870547231218045 – Supplemental material for Stimulant Treatment and Potential Adverse Outcomes in Pediatric Populations With Bipolar Disorder: A Systematic Review of the Literature
Supplemental material, sj-docx-1-jad-10.1177_10870547231218045 for Stimulant Treatment and Potential Adverse Outcomes in Pediatric Populations With Bipolar Disorder: A Systematic Review of the Literature by Hannah O’Connor, Chloe Hutt Vater, Maura DiSalvo, Stephen V. Faraone and Janet Wozniak in Journal of Attention Disorders
Footnotes
Author Note
This work is published in honor of Joseph Biederman. Dr. Joseph Biederman was a pioneer in child psychiatry and the founder of the field of pediatric psychopharmacology. His career was dedicated to examining the cause, diagnosis, and treatment of ADHD and other psychiatric disorders across the lifespan. He worked to explore treatments for highly comorbid disorders and to define emotional dysregulation and establish the diagnosis of pediatric bipolar disorder. His exploration of psychopharmacology in children with emotional dysregulation set the background for this work, and he was a great mentor to the authors and to hundreds of others in his more than 40-year career at Massachusetts General Hospital. This manuscript was started during Dr. Biederman’s last months at work. We know he would be pleased to see work on stimulant treatment in children with emotional dysregulation published and discussed in the literature.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.