
Abstract
While once-daily single-tablet regimens (STRs) are recommended for most people with human immunodeficiency virus (HIV; PWH), some require complex antiretroviral (ARV) regimens due to resistance, contraindications, or drug–drug interactions. We characterized PWH who were virologically suppressed on complex regimens (VS on CR) in a U.S. cohort to inform treatment optimization as new switch options emerge. This retrospective study analyzed electronic medical records from the Trio Health HIV Network and genotypic resistance data from Labcorp. We included PWH ≥ 18 years who were virologically suppressed (viral load [VL] < 200 copies/mL) at complex regimen initiation between January 2016 and November 2023, with ≥6 months from last prescription and ≥1 year of follow-up. Complex regimens included ≥2 of 3 core ARV classes concomitantly, more than once-daily dosing, multi-tablet regimens (MTRs) not replaceable by STRs, or resistance to two ARV classes. Virologic failure (VF) was defined as VL ≥ 500 copies/mL or two consecutive VLs ≥ 200 copies/mL. PWH on ibalizumab, fostemsavir, or lenacapavir were excluded to reflect standard clinical practice. Of 43,236 PWH with ARV prescriptions, 3,320 (8%) were VS on CR. Among these, 69% were on MTRs, 43% used ≥2 core ARV classes, and 11% had resistance to two classes. The median age was 52 years, and 77% were male. Common comorbidities included obesity (69%), neuropsychiatric disorders (35%), and cardiovascular disease (33%). Regimens predominantly included protease inhibitors (77%), nucleoside reverse transcriptase inhibitors (75%), and integrase strand transfer inhibitors (57%). Over a median 2.2-year follow-up, 4% experienced VF. Approximately 8% of PWH on ART remain VS on CR, underscoring the need for education on regimen optimization and novel treatment options for those unable to simplify their therapy.
Keywords
Introduction
Current human immunodeficiency virus (HIV) antiretroviral treatment (ART) guidelines recommend initial regimens consisting of a second-generation integrase strand transfer inhibitor (INSTI; dolutegravir or bictegravir) combined with one or two nucleoside reverse transcriptase inhibitors (NRTIs). These NRTIs include tenofovir-based combinations with lamivudine or emtricitabine.1,2 In prospective clinical trials, these regimens have provided the highest rate of virologic suppression with a low risk of adverse events or emergent resistance.3–5 Available coformulations allow most individuals to take single-tablet regimens (STRs) once daily, which are generally associated with high rates of adherence and virologic suppression.6–7 In addition to their use as first-line treatment, STRs are guideline-recommended as a switch strategy for many people with human immunodeficiency virus (PWH), based on multiple studies.8–11 However, limited data exist characterizing the population of PWH who remain on complex regimens despite these advances, particularly regarding their demographic and clinical profiles, genotypic resistance patterns, and virologic outcomes.
Currently available STRs combine an INSTI, boosted protease inhibitor (PI), or non-nucleoside reverse transcriptase inhibitor (NNRTI) with one or two NRTIs. The emergence of resistance mutations to one or more classes of ART in PWH, particularly those associated with NRTI class, in addition to intolerance/toxicities, drug–drug interactions, and contraindications, sometimes leads clinicians to prescribe complex treatment regimens. These complex regimens generally include multiple tablets without equivalent STRs, greater than once daily schedule, regimens with food requirements and/or booster agents, or regimens composed of three drug classes. These factors may pose challenges related to safety, tolerability, drug interactions, and long-term adherence. While darunavir/cobicistat/emtricitabine/tenofovir alafenamide (DRV/c/FTC/TAF) is formulated as an STR, it was classified as a complex regimen in this study because it contains a boosted PI with known metabolic and cardiovascular risks, requires food for adequate absorption, and is not a guideline-preferred regimen for most PWH.
To define the demographic and clinical characteristics, as well as treatment outcomes, of PWH receiving complex regimens, we conducted a retrospective observational study using a large proprietary longitudinal database that includes records for over 50,000 PWH who had prescriptions for antiretrovirals. By focusing on individuals who were already virologically suppressed at the time of initiating a complex regimen (VS on CR), we aimed to identify PWH who may be candidates for treatment optimization with currently available or emerging therapeutic options. Reasons for complex regimen prescribing may include historical resistance, treatment failure, drug interactions, or prescribing patterns. We examined PWH receiving clinical care across broad geographic regions of the United States.
Methods
Data source and study design
This retrospective, observational, cross-sectional study analyzed de-identified electronic medical records (EMR) from the Trio Health HIV Research Network, combined with genotypic resistance data from Labcorp. At the time of the analysis, the Trio Health HIV Research Network, a proprietary longitudinal database, included records for over 50,000 PWH who had prescriptions for antiretrovirals. The data were sourced from 12 large, HIV-specialized, federally qualified health centers across the United States, ensuring wide geographic representation. These 12 centers represent a subset of the full Trio Health network selected to provide broad geographic coverage across regions with high HIV prevalence. Clinics were included based on data completeness, consistent use of EMR systems compatible with the Trio Health data infrastructure, and geographic distribution. Clinics with insufficient data quality or follow-up coverage were excluded to ensure analytic reliability. To assess representativeness, the demographic and clinical characteristics of the study population were compared with regional HIV surveillance data from publicly available resources. The study population reflected higher proportions of older, male, and virologically suppressed individuals, consistent with an HIV-specialized clinical cohort. Data captured include demographics, diagnoses (ICD-10 codes), laboratory results, and prescriptions. Prescription information was captured from provider prescribing records within the EMR; however, prescription dates reflect when orders were placed and may not correspond exactly to the date medications were dispensed or initiated by patients.
Labcorp provided deidentified, tokenized HIV resistance testing data from clinics within the Trio Health HIV Research Network. Trio Health merged these resistance data with clinical trajectories into a tokenized and de-identified registry, allowing for the evaluation of clinical outcomes based on resistance profiles and treatment histories.
The study covered the period from January 2016 to November 2023. Based on the Department of Health and Human Services regulation (45 CFR 46.104(d)(4)), the central institutional review board (Advarra IRB) deemed the research exempt from the IRB oversight. Investigators did not access any individually identifying information during the study.
To minimize the risk of information bias, data collection from clinics was standardized using uniform data extraction protocols and quality control procedures at all participating sites.
Study objectives
The objective of this study was to describe the characteristics of PWH who were virologically suppressed on complex regimens, including demographics, baseline clinical characteristics, regimens, and comorbidities. We also aimed to characterize genotypic testing frequency and frequency of resistance by class, drug, and mutations of interest (e.g., M184V). Viral blips were defined as isolated viral load (VL) measurements between 50 and 199 copies/mL, preceded and followed by values <50 copies/mL. Additionally, the study aimed to describe virologic outcomes (viral blips, failures, low-level viremia) and individual characteristics that predict virologic failure among people virologically suppressed on complex regimens. ART adherence was characterized in a subset of individuals with dispensing data using the proportion of days covered (PDC), reported as mean (standard deviation [SD]), median (interquartile region [IQR]), and the proportion of PWH with PDC ≥80%. PDC was calculated as the total number of days with active prescriptions divided by the total number of days in the observation period while on the complex regimen, and was assessed only for the subset of participants with available dispensing data from pharmacy records.
Inclusion criteria
Individuals who met the study criteria had ≥1 prior ART, with ≥6 months on complex regimens initiated after January 1, 2016; were aged ≥18 at index (defined as the date of initiation of complex regimen); were virologically suppressed at initiation (<200 copies/mL), a threshold consistent with the DHHS guideline definition of virologic suppression and chosen to capture a broader range of suppressed individuals, including those with low-level viremia between 50 and 199 copies/mL; had ≥1 year of follow-up; and were not enrolled in clinical trials. PWH receiving novel agents, ibalizumab, fostemsavir, or lenacapavir, used exclusively in PWH with few treatment options were excluded. These agents are used in a small minority of patients with highly treatment-experienced HIV and limited remaining options; their inclusion would have reduced the generalizability of findings to standard clinical practice.
Complex regimens were defined as containing (1) two of three core ARV classes used concomitantly (NNRTI, PI, INSTI); (2) darunavir/cobicistat/emtricitabine with tenofovir alafenamide or tenofovir disoproxil fumarate (DRV/c/FTC/TAF or DRV/c + FTC/TDF); (3) more than once-daily dosing; (4) multi-tablet regimens (MTRs) irreplaceable by single-tablet regimens (STRs); or (5) regimens used in individuals with HIV that is resistant to two or more ARV classes (NNRTIs, INSTIs, NRTIs, or PIs). Core classes were defined as NNRTI, PI, or INSTI—thus excluding NRTI.
Definitions
Baseline (index date) was defined as the first prescription date of the first qualifying regimen. Baseline comorbidities were reported based on the codes of the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). Baseline viral loads, comorbidities, and other laboratory results were defined as the closest available values within 12 months of the index date.
Resistance interpretation was provided using the Stanford University HIV Drug Resistance Database. 12 Drug-class resistance was defined as intermediate/high resistance to ≥1 drug within a class. Major mutations were defined according to the Stanford HIVdb algorithm and included mutations listed as conferring intermediate or high-level resistance to any drug within a class. Baseline resistance refers to cumulative genotype results available at any time prior to the index date.
Virologic failure was defined as VL ≥500 copies/mL without subsequent suppression, or two consecutive VLs ≥200 copies/mL at the last observation on the regimen or at switch to subsequent regimen. This composite definition was chosen to distinguish sustained virologic failure from transient viremia or blips, consistent with approaches used in other observational HIV cohort studies.22,23 Low-level viremia was defined as VL 50–199 copies/mL. In a sensitivity analysis, we examined the frequency of individuals with multiple consecutive VL measurements between 200 and 500 copies/mL whose last available VL was ≤199 copies/mL; this pattern was observed in a small minority of patients (<5%), and inclusion or exclusion of these individuals did not meaningfully alter the virologic failure rate. The study period spanned from January 2016 to October 2024.
Statistical analysis
Descriptive statistics for the study population were provided to characterize baseline demographics, clinical characteristics, and comorbidities. For continuous variables, means, standard deviations, medians, and interquartile ranges were reported. For variables with categorical or dichotomous data, counts and proportions were provided. For variables with missing data, proportions were calculated using the number of individuals with available data as the denominator (i.e., excluding those with missing values), and the denominator for each variable was reported alongside the corresponding proportion to ensure transparency.
HIV genotype resistance testing analyses reported the number and proportion of PWH with historical genotype results, the prevalence of specific mutations, drug-class resistance, and individual drug resistance.
The proportions of PWH on qualifying regimens who had low-level viremia at any time during the complex regimen and virologic failure at the end of follow-up were reported for the first qualifying complex regimen (some individuals had more than one qualifying regimen during the study period; the earliest was selected for analysis). In univariate analysis, baseline and regimen characteristics were reported for individuals with virologic failure on complex regimen versus without. Following univariate analysis, Classification and Regression Tree (CART), 13 a nonparametric machine learning discrimination analysis, was used to identify primary drivers of virologic failure at last observation on the regimen using baseline characteristics described further. CART recursively partitions the data to identify the most discriminating predictors, ranking them by normalized importance. The following variables were included in the CART analysis: demographics (age, gender, race, ethnicity, insurance type), baseline clinical characteristics (CD4 count, VL, body mass index [BMI], estimated glomerular filtration rate [eGFR], prior low-level viremia [any documented episode before the index date], prior virologic failure [any documented episode before the index date]), baseline genotypic characteristics (presence of major baseline mutations, number of baseline resistance classes, resistance to INSTI, NNRTI, PI, NRTI), regimen characteristics (drug class, STR vs. MTR, number of drug classes), and baseline comorbidities (cardiovascular disease, neuropsychiatric disorders, diabetes, smoking, substance use, sexually transmitted infections [documented within 12 months of index,including gonorrhea, chlamydia, and syphilis], alcohol use). Variables identified as important in the CART analysis, together with key demographic characteristics and additional variables suggested by univariate analysis and clinical relevance based on prior literature, were entered into a multivariable logistic regression model. A backward stepwise approach was used to derive the final model. We acknowledge that data-driven variable selection approaches have limitations for causal inference, and the results should be interpreted as exploratory rather than confirmatory.
Statistical analyses were performed using R 4.3.0 (R Core Team, 2023) and IBM SPSS Statistics (version 28).
Results
Sample characteristics
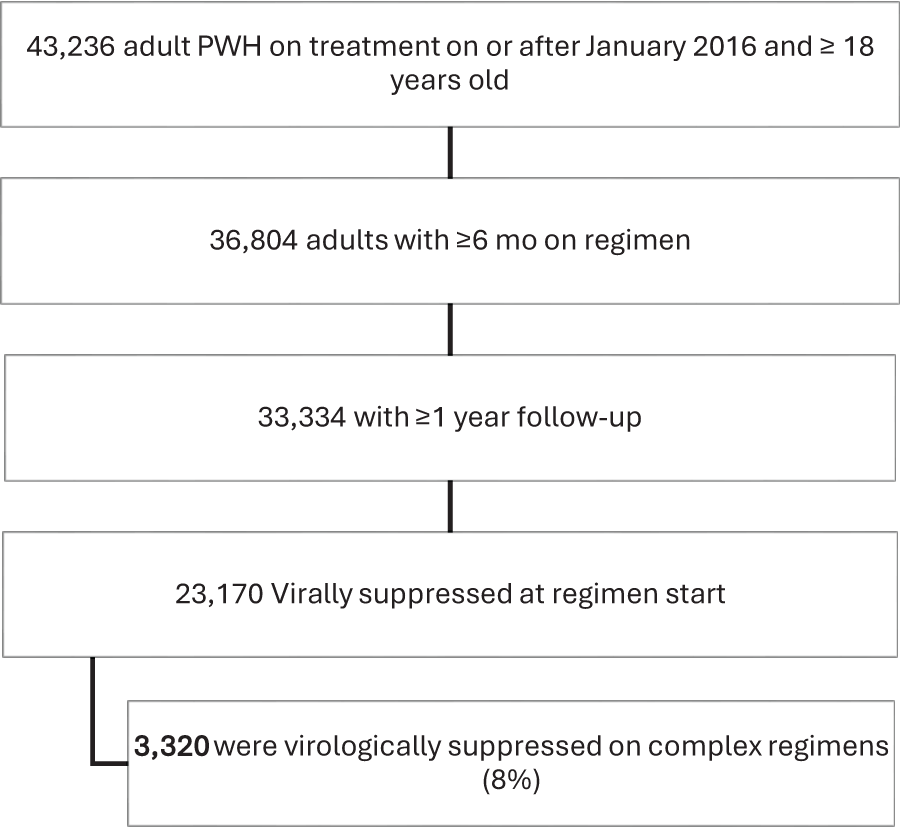
Of 42,236 PWH with new prescriptions after January 1, 2016, 3320 (8%) were VS on CS (Fig. 1). Of them, 2284 (69%) were on MTRs, 1433 (43%) received ART with two of three core classes, 1377 (41%) received DRV/c/FTC/TAF or TDF, 377 (11%) had HIV with resistance mutations to two classes, and 6 (<1%) were taking ART requiring more than once-daily dosing. These categories were not mutually exclusive; for example, individuals on MTRs could also meet criteria for having two core classes or DRV-based regimens.
PWH selection.
The median age of the study population was 52 years (IQR, 16), 77% were male, 44% were Black, 44% were White, 38% had commercial insurance, and 29% had Medicare insurance. Participants had a median follow-up of 5.1 years after study qualification (2.2 years on qualifying complex regimen) and had received a median of two prior ARTs (Table 1). At baseline, 85% of PWH VS on CS had a VL <50 copies/mL. The median (IQR) baseline CD4 was 548 (410) cells/mm3, 7% had a baseline CD4 count <200 cells/mm3, 15% had a baseline eGFR <60 mL/min/1.73 m2, and 69% were overweight or obese based on their BMI. In terms of baseline comorbidities, 35% had neuropsychiatric disorders, 33% had cardiovascular disease, 19% had hyperlipidemia, 9% had diabetes, 6% had HCV, 3% had HBV, 12% had documented substance use, and 19% were documented smokers.
Study Sample Characteristics
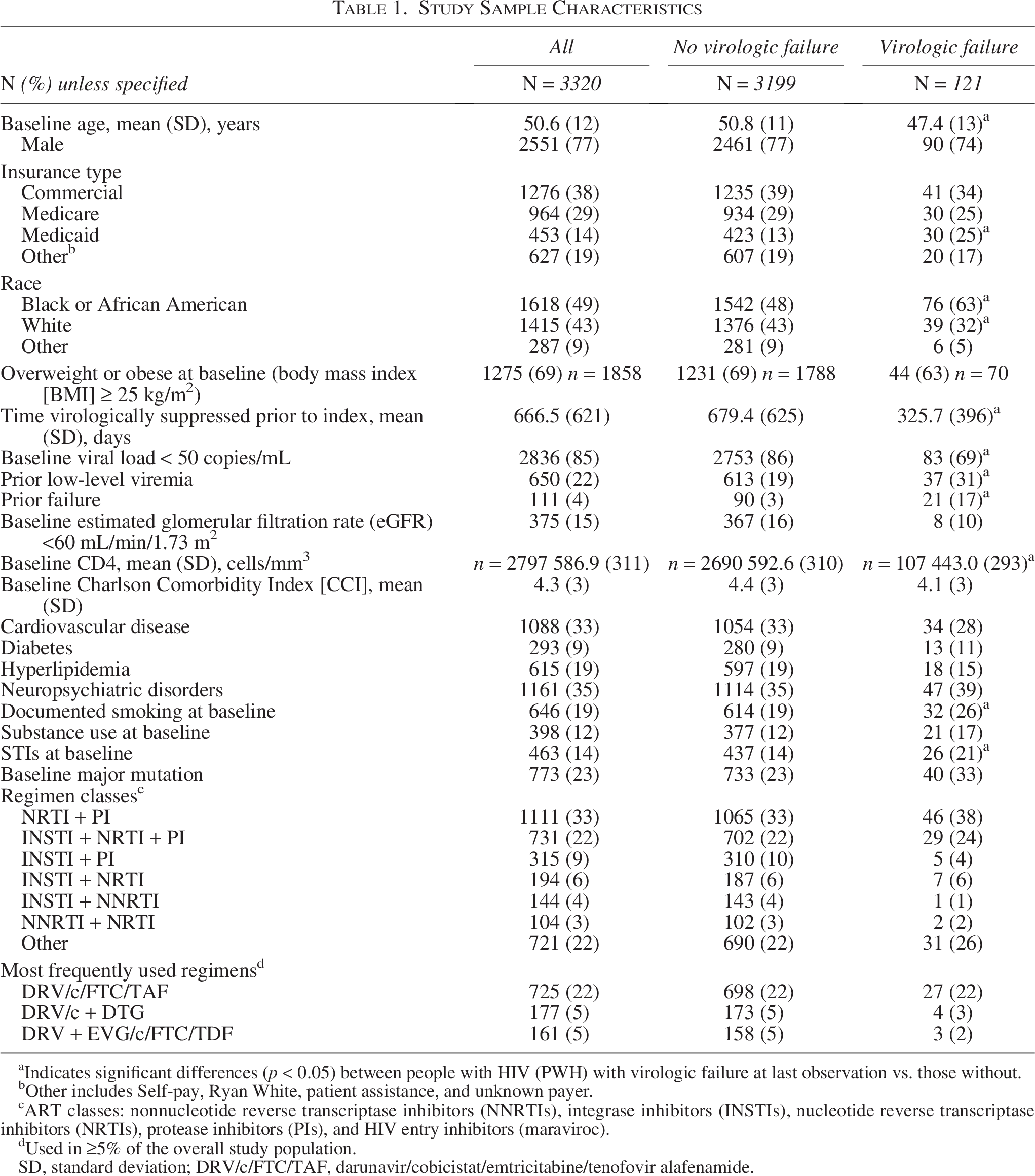
Indicates significant differences (p < 0.05) between people with HIV (PWH) with virologic failure at last observation vs. those without.
Other includes Self-pay, Ryan White, patient assistance, and unknown payer.
ART classes: nonnucleotide reverse transcriptase inhibitors (NNRTIs), integrase inhibitors (INSTIs), nucleotide reverse transcriptase inhibitors (NRTIs), protease inhibitors (PIs), and HIV entry inhibitors (maraviroc).
Used in ≥5% of the overall study population.
SD, standard deviation; DRV/c/FTC/TAF, darunavir/cobicistat/emtricitabine/tenofovir alafenamide.
The most common regimen class combinations were NRTI + PI (23%), INSTI + NRTI + PI (22%), and INSTI + PI (9%); the most common regimens were DRV/c/FTC/TAF (22%), DRV/c + DTG (5%), and DRV + EVG/c/FTC/TDF (5%). Regimens used in the study population included NRTIs (75%), PIs (77%, including 65% boosted PIs), INSTIs (57%), and NNRTIs (24%). Overall, 39% of individuals had regimens with more than two core ART classes (INSTI, NNRTI, and PI).
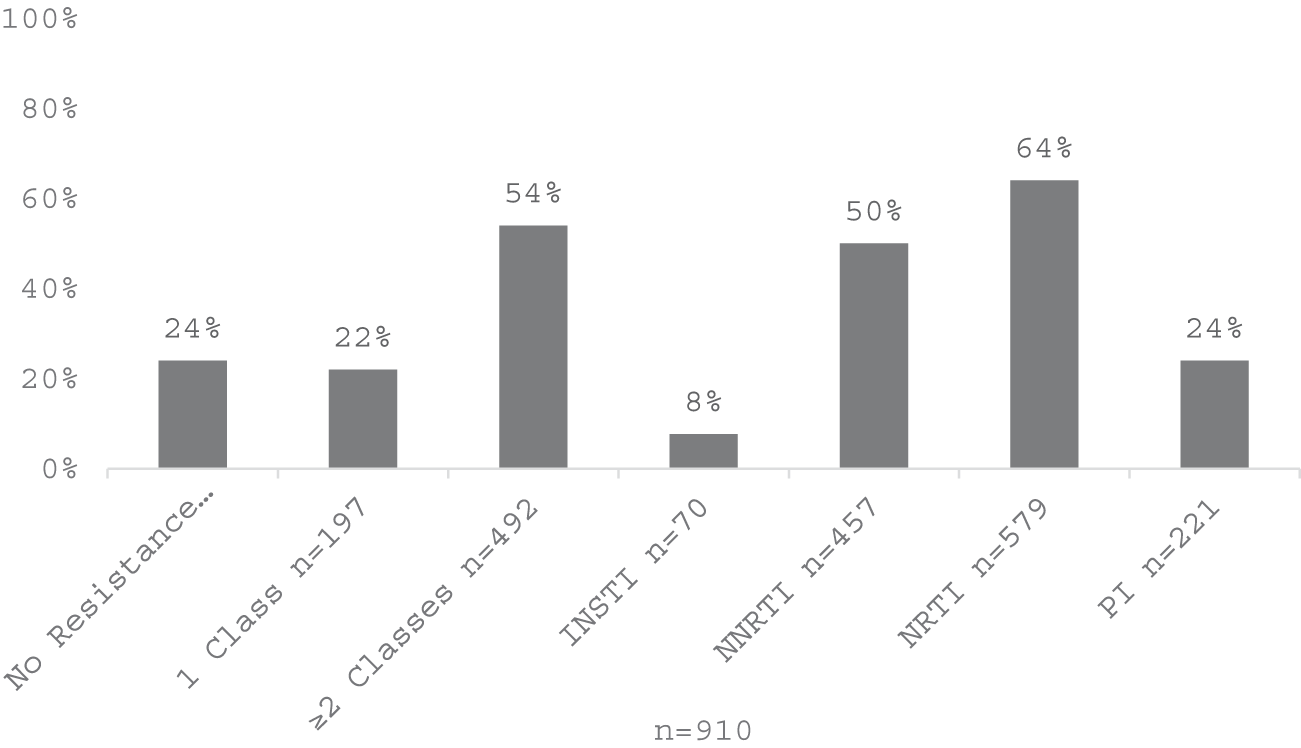
At any time prior to baseline, 1,368 (41%) individuals underwent HIV genotype testing, and 910 (27%) had available genotype test results (the difference reflects tests performed at laboratories other than Labcorp, for which results were not available in the linked dataset; all available genotype data were derived from RNA-based sequencing) (Fig. 2). Of 910 VS on CR with genotype test results prior to baseline, 773 (85%) had HIV with at least one major mutation (64% NRTI, 50% NNRTI, 24% PI, and 8% INSTI), and 54% had HIV with ≥2 class resistance (Fig. 3). The most common major mutations among individuals with test results were M184V/I (55%), K103N/S (30%), and three thymidine-associated mutations: K70R (17%), T215Y/F (16%), and M41L (15%).
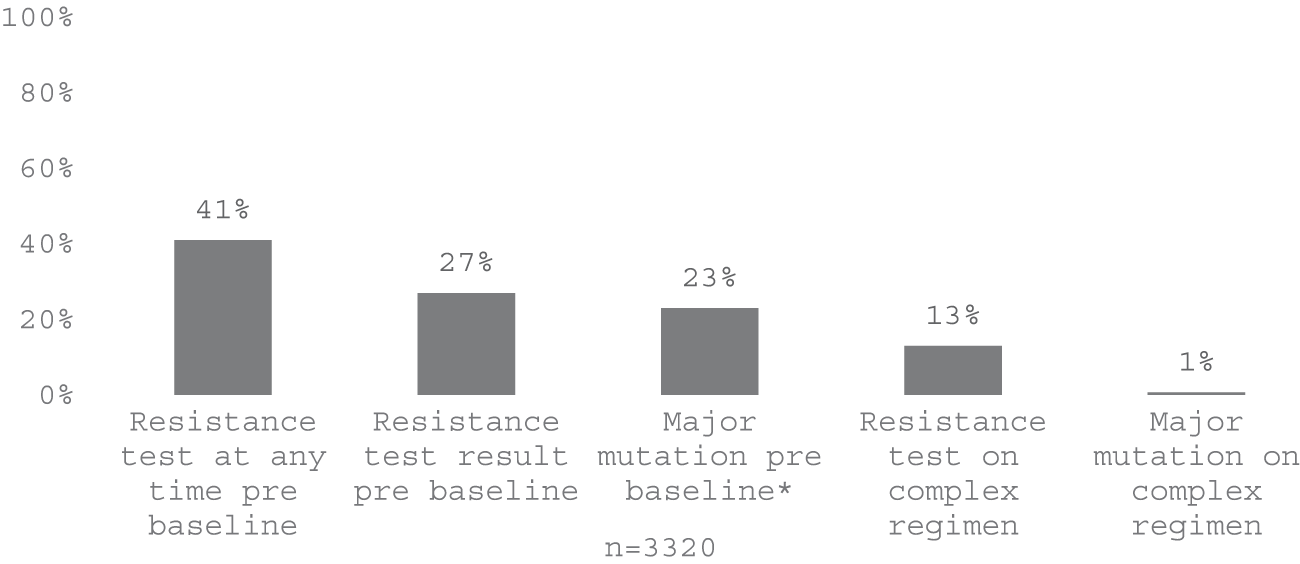
Resistance testing.
Baseline resistance characteristics.
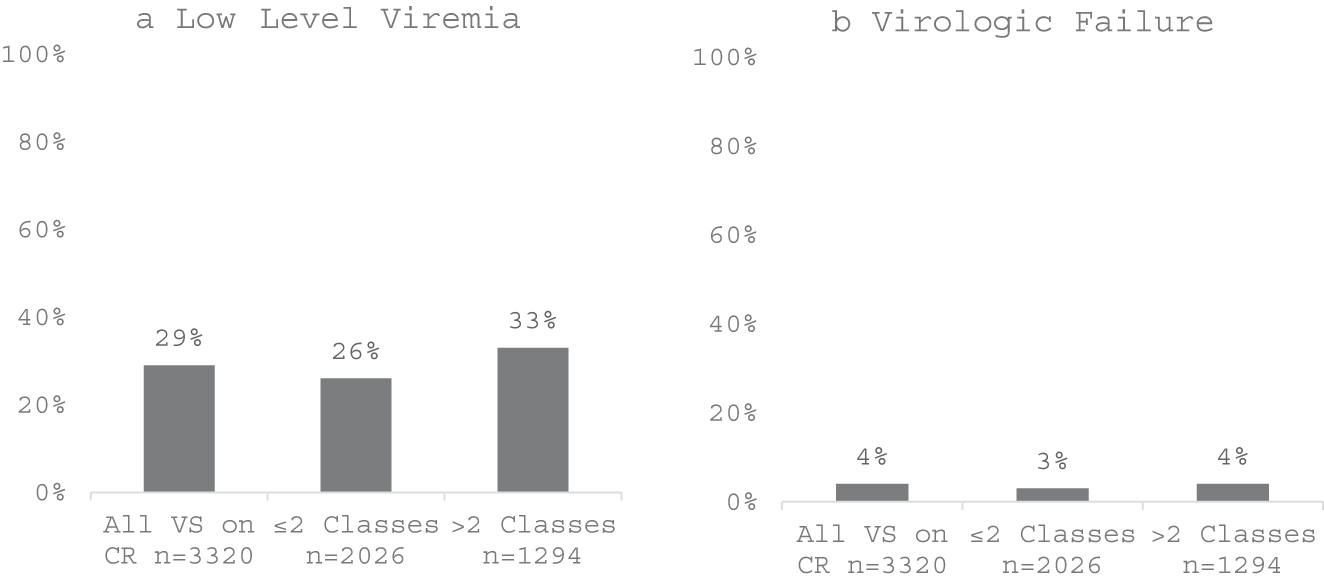
During the median follow-up of 2.2 years among PWH on complex regimens, 121 (4%) had virologic failure and 957 (29%) had low-level viremia (more common on regimens with >2 classes: 33% vs. 26%) (Figs. 4a,b and 5a,b).
Among the subset of PWH with dispensing data (47% of those with prescriptions), the median (IQR) PDC while on complex regimens was 76% (56%), the mean (SD) was 67% (31%), and 47% had a PDC ≥80%. Dispensing data were available for 47% of patients and were derived from 340B pharmacy records. The remaining 53% lacked dispensing data because they obtained medications from pharmacies outside the 340B network. This represents a structural limitation of using 340B data to assess adherence across a diverse clinic population. Patients with and without dispensing data had similar baseline demographic and clinical characteristics, suggesting that the subset with PDC data was broadly representative. However, the absence of dispensing data for the majority of patients limits the generalizability of the PDC findings.
Based on univariate analysis, compared with those without virologic failure, individuals with virologic failure exhibited greater likelihood of several characteristics: younger age (median age, 50 vs. 52 years old; 12% vs. 5% being aged <30 years old), Black race (63% vs. 48%), and insured with Medicaid or Ryan White (25% vs. 13%). Further, individuals with virologic failure had higher proportions of PWH with baseline viral loads between 50 and 199 copies/mL (31% vs. 14%), CD4 counts < 200 cells/mm3 (14% vs. 6%), documented smoking (26% vs. 19%), sexually transmitted infections (21% vs. 14%), and documented substance use (17% vs. 12%) (Table 1). Clinically, PWH experiencing virologic failure were more likely to be on the regimen with >2 core classes (44% vs. 39%) or PI-containing regimens (85% vs. 77%), and were more likely to have a baseline genotypic test result (41% vs. 27%). Additionally, their HIV virus was more likely to possess a major mutation at baseline (33% vs. 23%). PWH with virologic failure were also more likely to have a history of prior treatment failure (17% vs. 3%) or prior low-level viremia (31% vs. 19%).
CART analysis, with the outcome of virologic failure at the last observation on or at the time of switching from the complex regimen, effectively classified 96% of the data, identifying four predictors of virologic failure: failure on any prior regimen, baseline VL (>100 copies/mL), baseline PI resistance, and lower baseline CD4 count (<393 cells/mm3).
Of note, although baseline PI resistance was identified as a predictor of virologic failure by the CART model, only 2% of individuals with baseline PI resistance experienced virologic failure in this cohort. This apparent paradox is explained by the nonparametric nature of the CART approach. CART identifies variables that most effectively partition the data according to normalized importance, meaning that PI resistance can discriminate virologic outcomes even at low absolute event rates when considered alongside other covariates. The presence of PI resistance alone does not solely determine virologic outcome, as additional active agents within a regimen may maintain suppression despite PI resistance mutations. The CART model correctly classified 96% of the overall data, supporting its discriminative value, although it should be interpreted as exploratory given the observational design. To further explore these associations, a logistic regression model was developed. This model incorporated baseline demographics, predictors identified by CART, and additional variables suggested by univariate analysis and previous research.22,23 Variables entered into the model included age, gender, race, baseline substance use, documented smoking, STI, CD4 count < 400 cells/mm3, VL ≥ 100 copies/mL, prior virologic failure, and use of PI, INSTI, or NNRTI.
Based on multivariable backward stepwise logistic regression, several variables were found to be significantly associated with virologic failure on complex regimens: failure on a prior regimen (adjusted odds ratio [aOR] = 5.8, 95% confidence interval [CI]: 3.4–10.1), baseline VL ≥ 100 copies/mL (aOR = 4.0, 95% CI: 2.5–6.5), age <30 (aOR = 2.5, 95% CI: 1.4–4.7), baseline CD4 <400 cells/mm3 (aOR = 2.5, CI 1.6–3.6), NNRTI use as part of the complex regimen (aOR = 1.7, 95% CI: 1.04–2.8).
Discussion
In HIV clinical practice, most people with HIV can achieve and maintain virologic suppression on guideline-recommended regimens. This approach has become increasingly feasible with the widespread adoption of second-generation INSTIs (bictegravir and dolutegravir), which have a high barrier to resistance and can maintain suppression even in the presence of background resistance to other drug classes. Despite this advance, a substantial proportion of PWH remain on more complicated regimens for a variety of reasons. Our goal was to describe the demographic and HIV-related characteristics, as well as the virologic outcomes, of individuals who were virologically suppressed while receiving complex regimens. Based on the study criteria, this analysis found that ∼8%—nearly 1 out of 10—of PWH prescribed ART were receiving complex regimens.
Although INSTIs were prescribed to 57% of VS on CR, reflecting recent convergence in clinical practice, 65% of the individuals in the study were also received boosted PI-based regimens despite the known limitations of these agents, such as increased cardiovascular risk and numerous drug interactions.14,15 In addition, 69% were taking multiple tablets daily and therefore were not benefiting from guidelines-recommended STRs.
Evidence from treatment-switch studies, particularly in resource-limited settings, provides reassurance that virologic suppression can be maintained even in the context of background NRTI resistance. PWH in resource-limited settings frequently maintain suppression despite extensive NRTI resistance. In the 2SD, GHESKIO, and VISEND studies,16–18 PWH receiving second-line boosted PI regimens were successfully switched to INSTI-based regimens (TLD or B/F/TAF), with comparable suppression and no emergent INSTI resistance. These findings suggest that NRTI resistance alone may not necessitate continuation of complex, PI-based, or multi-tablet regimens in all cases and provide evidence supporting the feasibility of treatment optimization in appropriately selected patients, provided there is no INSTI resistance.
While findings from the 2SD, VISEND, and GHESKIO studies demonstrate that PWH are able to optimize treatment today with available STRs, less data exists when considering optimization among PWH who are receiving treatment with multiple core agents (e.g., INSTI + BPI or BPI + NNRTI).16–18 New treatment options for PWH who are virologically suppressed on complex regimens are currently under development. Unlike the previously mentioned switch studies, which focused exclusively on second-line boosted PI regimens, the full ARTISTRY study program is investigating whether a fixed-dose combination of bictegravir (BIC), a guidelines-recommended second-generation INSTI, and lenacapavir (LEN), a first-in-class capsid inhibitor, can optimize treatment for PWH. In the phase 2 ARTISTRY-1 trial, PWH on complex regimens (81% due to resistance, all with ≥2 core agents) were randomized to either continue or switch to BIC + LEN; at week 48, virologic suppression was achieved in 93% of patients in the BIC + LEN arm compared with 90% in the control arm (continuing their current regimen), and the regimen was well tolerated. 19 Fully powered phase 3 clinical trials of coformulated BIC/LEN are currently underway.20,21 Beyond BIC/LEN, other emerging therapeutic strategies for treatment-experienced PWH include long-acting injectable regimens and novel agents targeting different stages of the HIV life cycle, all of which may further expand options for those on complex regimens. Importantly, treatment optimization efforts must account for individual patient histories; a recent study by Bontemps et al. highlighted the challenges of switching from complex regimens in heavily pretreated PWH, underscoring that simplification may not always be feasible and that newer agents will be needed to address the needs of this population. 26
In our study, during a median of 2.2 years of follow-up on complex regimens, only 4% of PWH had treatment failure. The overall high level of treatment success observed in our study was similar to other contemporary reports on individuals who were virologically suppressed at the time of regimen switch, although our study is the first to focus on outcomes in PWH on complex regimens. Min et al. reported that 85 − 90% of PWH maintained suppression annually from 2016 to 2019, with younger age, Black race, and a history of incarceration significantly associated with viral rebound. 22 A CNICS study similarly found 90% maintained suppression over 2 years, with Black race, current smoking, and shorter ART duration associated with viral rebound. 23
Prior regimen failure was the strongest independent predictor of virologic failure in multivariable analysis. Additional independent predictors included demographic and clinical characteristics like age <30 years at baseline, baseline VI ≥ 100 copies/mL, CD4 cell count <400 cells/mm3, and NNRTI use as part of the complex regimen. Many of these factors have been previously described, both in the current and earlier treatment eras.24,25 These factors indicated that many PWH with prior treatment failure likely have adherence barriers that remain even after achieving viral suppression.
Our study has several limitations. The retrospective design is prone to missing important information and cannot invoke proactive queries to fill in missing values. Importantly, this study lacked a comparison group of PWH who did not switch to complex regimens, limiting our ability to determine whether comorbidities or other factors were differentially associated with complex regimen use. Additionally, this study focused exclusively on individuals who were virologically suppressed at the time of complex regimen initiation; outcomes may differ among PWH who initiate complex regimens while not virologically suppressed. Further, study subjects were identified from a database that includes data on all PWH treated at clinics participating in the Trio Health HIV Research Network, irrespective of their demographics or treatment regimens. Data on genotype resistance testing were available for a subset of clinics directly, and linked genotype data were only available from one most commonly used laboratory, which may not be comprehensive. While Trio Health HIV Research Network is geographically distributed to represent HIV incidence across U.S. regions, the findings are specific to the U.S. Health care context and may not be generalizable to other settings, including resource-limited settings in sub-Saharan Africa, or to health care systems in Europe or Latin America, where treatment guidelines, available regimens, and patterns of drug resistance may differ substantially. Further, the network may not describe the entirety of HIV care in the United States. Treatment given by clinicians outside of these facilities was not captured in the database and hence may be underestimated. Additionally, the reasons for prescribing complex regimens were not systematically captured in the dataset, limiting our ability to determine whether these prescribing decisions were clinically appropriate. Individuals with <1 year of follow-up on the complex regimen were excluded, as this duration was considered insufficient to adequately assess virologic response and observe clinically meaningful outcomes. This exclusion may have introduced some selection bias if individuals with poor early virologic outcomes switched regimens before completing 1 year of follow-up. Regarding the virologic failure definition, a small minority of patients (<5%) had multiple consecutive VL measurements between 200 and 500 copies/mL followed by a final viral load ≤199 copies/mL and were not classified as failures; sensitivity analyses confirmed this had minimal impact on overall failure rates. With respect to the backward stepwise model selection approach, this data-driven method may introduce selection bias and reduce reproducibility; findings should be interpreted as hypothesis-generating rather than confirmatory, and future studies using prespecified variable selection approaches are warranted. Missing CD4 count data (15% of patients) also represent a limitation of EMR-based research, as CD4 testing frequency is determined by provider practice rather than study protocol; analyses were performed using available data. The CART methodology, while useful for exploratory identification of predictors, has inherent limitations: It is susceptible to overfitting, particularly with smaller subgroups; results may lack stability across different samples; CART does not provide CIs or p values, limiting statistical inference; and identified predictors may reflect correlations rather than causal relationships. These limitations reinforce that CART findings should be considered exploratory and hypothesis-generating.
This retrospective observational cohort study provides a comprehensive analysis of PWH who were virologically suppressed at the time of initiating complex regimens, representing ∼8% of individuals on ART treatment in the United States. There was infrequent documentation of genotypic testing any time prior to initiation of complex regimens, with a concomitant high prevalence of documented HIV resistance among those with available testing results. During median 2 years of follow-up, only 4% of the study participants had virologic failure at their last observation while receiving complex regimens. Virologic failure was more prevalent for individuals with certain demographic and HIV-specific characteristics, some of which may serve as proxies for factors leading to poor medication adherence or advanced HIV disease. The substantial proportion (69%) of individuals on multi-tablet regimens suggests a potential opportunity for treatment optimization, although the reasons for complex regimen prescribing were not captured in this study and may have been clinically appropriate in some cases. Where applicable, clinician education about currently available guideline-recommended regimens may facilitate treatment optimization, particularly for PWH without INSTI resistance. In addition, the data support development of newer treatment options to support treatment optimization and improve adherence.
Authors’ Contributions
P.E.S. was the major contributor in writing the article. I.M. and J.R. analyzed and interpreted data. J.R. summarized study results and methods. K.J.D., S.P., B.G.-P., J.J.E., C.W., M.R., S.S., K.M., R.A.E., P.B., and S.R. provided critical revisions and interpretation of the data. R.E. served as the principal investigator of the study. All authors read and approved the final article.
Data Availability Statement
The data that support the findings of this study are available from Trio Health; however, restrictions apply to the availability of these data, which were used under license for the current study and are therefore not publicly available. The data are, however, available from the corresponding author upon reasonable request and with permission from Trio Health and Gilead Sciences.
Footnotes
Acknowledgments
The authors would like to acknowledge Joshua Gruber and Megan Dunbar (
Author Disclosure Statement
P.E.S. is a consultant for Gilead Sciences, ViiV Healthcare, and Merck. He received research grants from Gilead Sciences, Merck, and ViiV Healthcare. R.A.E. has received grants from Gilead Sciences and ViiV Healthcare, serves on the Advisory boards for Gilead Sciences and ViiV Healthcare, and is a speaker for Gilead Sciences. He is the Chair of Trio Health Scientific Steering Committee, K.J.D. and B.G.-P. are employees of Gilead Sciences, J.R. and I.M. are employees of Trio Health, S.P. is a former employee of Gilead Sciences, C.W. is an employee of Labcorp, J.J.E. consults for Merck, ViiV Healthcare, Gilead Sciences, and Janssen. The University of North Carolina receives research funding from ViiV Healthcare, Gilead Sciences, and Janssen from which he receives support as an investigator, K.M. advises ViiV Healthcare, Merck, and Gilead Sciences. He is on the speakers’ bureau for ViiV Healthcare, Merck, and Gilead Sciences. He received research grants from ViiV Healthcare, Merck, and Gilead Sciences, M.R. is a consultant for ViiV Healthcare, Gilead Sciences, and Merck and received research funding from these companies, S.S. serves on the Medical Advisory Board for Gilead Sciences and is a Speaker for Gilead Sciences.
Funding Information
This study was funded by the Gilead Sciences.