
Abstract
Background
New HIV-1 infections continue to pose a major challenge to ending the HIV epidemic and may facilitate the transmission of drug-resistant strains. In this study, we aimed to determine the proportion of recent HIV-1 infections (RHI) among individuals initiating HIV care at a rural referral hospital in Tanzania and to assess the prevalence of pre-treatment HIV-1 drug resistance (PDR) and circulating subtypes among those with RHI.
Methods
In this cross-sectional analysis, RHI was identified using the Asante HIV-1 rapid recency assay on bio-banked samples from newly diagnosed adult people living with HIV (PLHIV) enrolled in the Kilombero and Ulanga Antiretroviral cohort between March 2019 and March 2022. Risk factors for recent HIV were evaluated using logistic regression analysis. Genotypic resistance testing (GRT) using Sanger sequencing was performed on samples from people with RHI.
Results
Among 599 PLHIV, 24 (4%) were identified with RHI. No factors were found to be associated with RHI. Genotypic resistance testing was successful in 16 of the 24 (67%) participants, of whom 5 (31%) harbored HIV-1 drug resistance mutations: 4/16 (25%) for non-nucleoside reverse transcriptase inhibitors, 2/16 (13%) for nucleoside reverse transcriptase inhibitors, and 1/16 (6%) for protease inhibitors.
Conclusion
The low prevalence of RHI in this hospital-based study suggests a high rate of late HIV diagnosis. Despite the limited sample size, the notable proportion of people with recent infection who had drug resistance highlights a serious public health concern.
Background
People with recent HIV infection (RHI), defined as infection acquired within the past 6 months, 1 pose a significant challenge to global efforts aimed at ending the AIDS epidemic. This early phase of infection is associated with high levels of viremia and increased risk of HIV transmission, partly due to the absence of HIV-specific neutralizing antibodies and limited viral diversity.2,3 It is estimated that 25–50% of new HIV transmissions originate from individuals with RHI. 4 Therefore, timely identification, linkage to care, and initiation of treatment for individuals with recent infection are critical components of effective HIV prevention strategies.
Integrase strand transfer inhibitor (INSTI)-based first-line antiretroviral regimens—particularly those based on dolutegravir—have emerged as a cornerstone in HIV treatment due to their rapid viral suppression and high genetic barrier to resistance. 5 These regimens are central to efforts to achieve the UNAIDS goal of reducing new adult HIV infections to fewer than 200,000 by 2030.6–8 However, concerns remain about the potential impact of widespread dolutegravir rollout in settings with a high prevalence of pre-treatment drug resistance (PDR), especially to nucleoside reverse transcriptase inhibitor (NRTI) backbone drugs. In such contexts, the risk of functional dolutegravir monotherapy could lead to virological failure and the emergence of INSTI resistance mutations. 9
Notably, while many NRTI-associated mutations reduce viral fitness, some—such as M184V—have complex effects that may actually increase susceptibility to other NRTIs, including tenofovir, and can influence overall viral fitness and treatment response. This interplay underscores the importance of understanding specific resistance patterns when evaluating PDR in populations initiating INSTI-based therapy. 10
Emerging evidence suggests that PDR may be more prevalent in individuals with RHI compared to those with chronic HIV infection.2,11–14 In the chronic phase, drug-resistant strains may be outcompeted by wild-type virus and fall below the threshold of detection, particularly in antiretroviral therapy (ART)-naïve individuals. 15
In Tanzania—as in many other sub-Saharan African (SSA) countries—data on PDR in people with recent HIV infection are lacking, as routine HIV resistance testing at diagnosis is not implemented. In this study, conducted at a rural referral hospital in Tanzania, we aimed to determine the proportion of RHI among newly diagnosed, ART-naïve PLHIV in a large rural cohort, identify potential predictors of RHI, and assess the prevalence of PDR and circulating subtypes among those people with recent infection.
Methods and material
Study design and population
This cross-sectional study included newly diagnosed PLHIV enrolled in the Kilombero and Ulanga Antiretroviral Cohort (KIULARCO) between March 2019 and March 2022. Eligible participants were adults aged 15 years and older who were newly diagnosed with HIV, ART-naïve at the time of enrollment, had provided written informed consent, and had a bio-banked plasma sample stored at −80°C available for testing. 16 Participants were enrolled into the KIULARCO cohort through routine HIV care at the Chronic Diseases Clinic of Ifakara (CDCI), a rural referral hospital. HIV testing and enrolment into care occurred through multiple pathways, including vertical transmission programs, provider-initiated testing and counselling during hospitalization or outpatient visits. The analysis utilized plasma samples collected prior to ART initiation.
Study area
This study was conducted at the Chronic Disease Clinic of Ifakara (CDCI), the HIV Care and Treatment Centre (CTC) located within the St. Francis Regional Referral Hospital in Ifakara, southwestern Tanzania. The CDCI is a collaborative initiative between the hospital, the Ifakara Health Institute, the Swiss Tropical and Public Health Institute, and the University Hospital Basel in Switzerland. Established in 2005, CDCI was among the first rural CTCs in Tanzania and provides comprehensive HIV care and free ART in alignment with the Tanzanian National AIDS Control Programme.17,18
Study procedures
At enrollment into KIULARCO, participants undergo a comprehensive clinical evaluation, including assessment of prior ART use. Blood samples are collected for CD4 cell count, full blood count, and clinical chemistry before ART initiation; however, routine baseline HIV viral load (HVL) testing is not performed. In accordance with the 2019 Tanzania National Guidelines for the Management of HIV and AIDS, HVL monitoring begins 6 months after ART initiation and is conducted annually thereafter. Additionally, plasma samples are cryopreserved at −80°C for research purposes.
Between April 1 and May 12, 2023, a total of 610 bio banked plasma samples were selected for recency testing from 934 eligible participants based on availability of Asante HIV-1 Rapid Recency Assay kits. To ensure proportional representation across the study period, participants were stratified by year of enrollment (2019–2022), and random sampling within each year was conducted using a Stata program to select participant IDs. Demographic, clinical, and laboratory data were extracted from the KIULARCO electronic medical record system.
Laboratory procedures
Plasma specimens were retrieved from the KIULARCO biobank, thawed, and tested for recent HIV infection using the Asante HIV-1 Rapid Recency Assay, an immunochromatographic lateral-flow rapid diagnostic test, following the manufacturer’s protocol (Sedia Biosciences, Portland, OR, USA). 19 For specimens identified as probable recent infections based on a positive recency assay result, HVL was measured by quantifying HIV-1 RNA using the Roche COBAS AmpliPrep/COBAS TaqMan system (Roche Diagnostics, Indianapolis, IN, USA).
HIV-1 genotypic resistance testing was performed on specimens with confirmed RHI by sequencing the reverse transcriptase (RT) and protease (PR) regions using the Sanger sequencing technique. Briefly, RNA was extracted from 150 µL of plasma using the PureLink Viral RNA/DNA Mini Kit (Invitrogen, Thermo Fisher Scientific, USA) following the manufacturer’s instructions. 20 RNA extracts were then reverse transcribed and amplified using the HIV-1 Genotyping Kit Amplification Module (Applied Biosystems, Thermo Fisher Scientific, USA). The resulting amplicons were sequenced via the Sanger platform at Macrogen Europe B.V. Sequence data were assembled using BioEdit version 7.2 and interpreted using the Stanford University HIV Drug Resistance Database (HIVdb) Program version 9.2 (https://hivdb.stanford.edu). Moreover, the HIV‐1 subtype was determined using online REGA HIV-1 Subtyping Tool - Version 3.0 from the Stanford HIVdb (https://hivdb.stanford.edu/hivdb). Identified drug resistance mutations were classified as conferring low, intermediate, or high-level resistance. All PR and RT sequences have been submitted to GenBank under accession numbers BankIt2682998 SeqIFA_4 OQ627458 to BankIt2682998 SeqIFA_40 OQ627474.
Definitions and covariates
Participants were classified as having RHI if they tested positive on the Asante HIV-1 Rapid Recency Assay and had a HVL greater than 1000 copies/mL Individuals who tested negative for RHI and had an HVL below 1000 copies/mL were classified as having long-term infection. 21
The study assessed a range of covariates, including age, sex, marital status, HIV status disclosure, highest level of education attained, and distance from the clinic (calculated based on the geographical center of the participant’s residential ward). Tuberculosis status was classified as positive if any of the following criteria were met: (1) positive microscopy for acid-fast bacilli; (2) a positive Xpert MTB/RIF assay (Cepheid, Sunnyvale, CA, USA) in sputum or other extra-pulmonary specimens; (3) chest radiograph findings suggestive of TB accompanied by at least one symptom; (4) a clinical diagnosis based on ICD-10 codes; or (5) initiation of anti-TB treatment.
Additional clinical variables included body mass index (BMI), HIV WHO clinical stage, and CD4 cell count. These parameters were recorded using the closest available measurement taken at enrollment or within 1 month thereafter.
Statistical analysis
Demographic and clinical characteristics were summarized using medians and interquartile ranges (IQR) for continuous variables, and frequencies with percentages for categorical variables. Variables considered a priori as potentially associated with recent HIV infection (RHI) included: age, sex, marital status, HIV status disclosure, highest education level, distance from residence to clinic, tuberculosis status, BMI, HIV WHO clinical stage, and CD4 cell count.
Associations between these variables and RHI were assessed using logistic regression models. Both univariable and multivariable analyses were performed without model selection procedures. Analyses related to PDR were descriptive in nature. All statistical analyses were conducted using Stata version 15.0 (StataCorp, College Station, TX, USA).
Ethical considerations
Written informed consent was obtained from all PLHIV who chose to participate in the KIULARCO study at the time of enrollment. Ethical approval for data and sample collection, as well as for their subsequent analysis, is renewed annually by the Institutional Review Board of the Ifakara Health Institute (IHI/IRB/No16-2006) and the National Institute for Medical Research of Tanzania (NIMR/HQ/R.8c/Vol.I/378). This specific study also received ethical clearance from the Human Research Ethics Committee of the University of the Witwatersrand, South Africa (Ref: M210714).
Results
Study participants
A total of 1659 PLHIV were enrolled in the KIULARCO cohort during the study period. Of these, 934 (56%) met the eligibility criteria for this analysis. From the eligible group, 610 (65%) participants were randomly selected based on the availability of bio-banked samples and recency assay kits. Subsequently, 6 participants were excluded due to invalid RHI assay results, and an additional 5 RHI-positive participants were excluded due to insufficient sample volume for HVL testing. The final analysis included 599 participants (Figure 1). Study participants flowchart.
Participant characteristics
Among the 599 included participants, the median age was 38 years (interquartile range [IQR]: 30–47 years), and 391 (65%) were female. Most participants were married or cohabiting (374; 62%), and 395 (67%) had disclosed their HIV status. A total of 72 participants (12%) reported no formal education.
Characteristics of study participants.
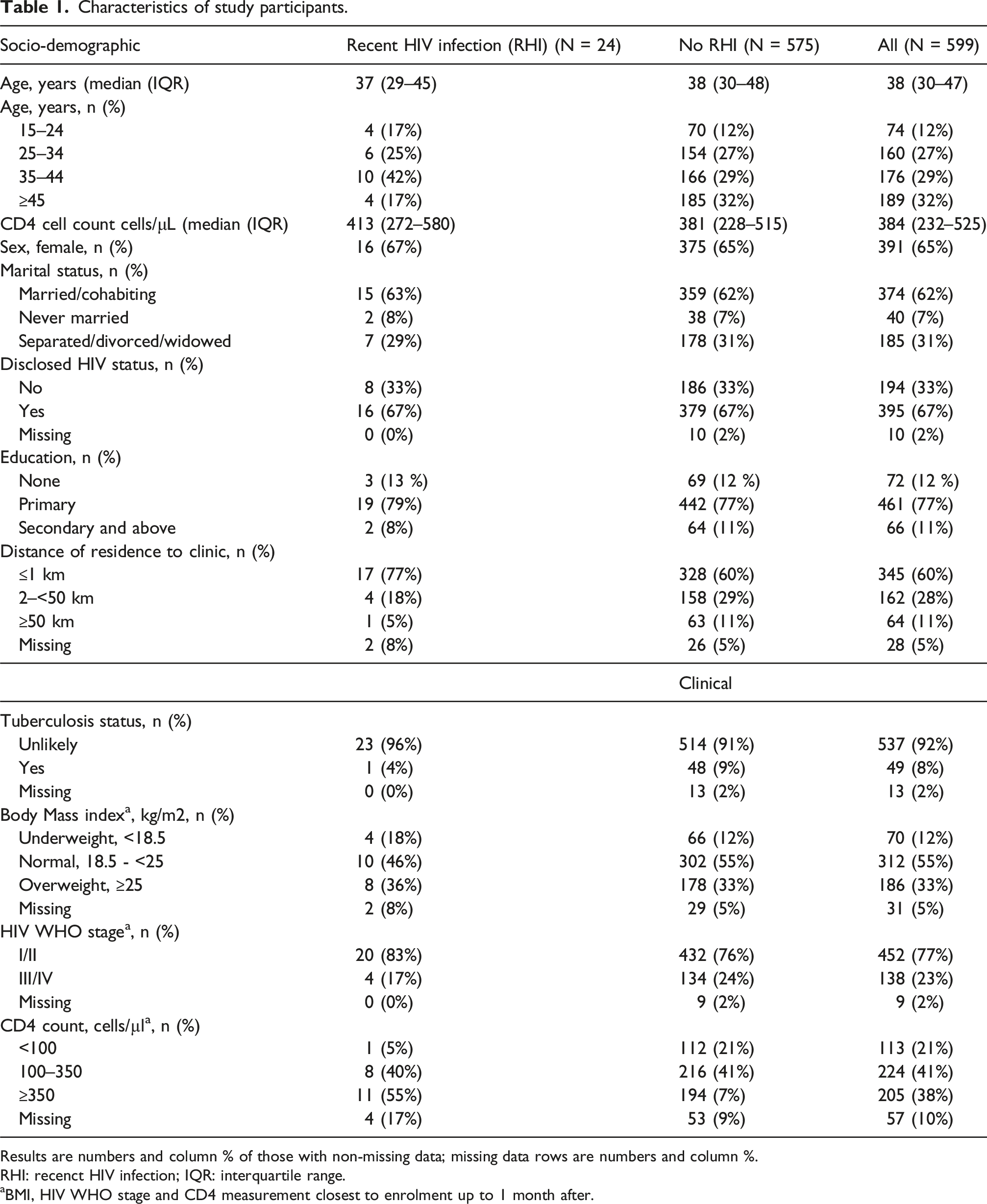
Results are numbers and column % of those with non-missing data; missing data rows are numbers and column %.
RHI: recenct HIV infection; IQR: interquartile range.
aBMI, HIV WHO stage and CD4 measurement closest to enrolment up to 1 month after.
Recent HIV infection and associated factors
Probable RHI was identified in 30 participants (5%). Among these, one participant (3%) had a HVL below 1000 copies/mL and was reclassified as having a chronic infection. Additionally, five participants (17%) had inconclusive RHI test results due to insufficient specimen volume for HVL testing, which also led to reclassification. This left 24 participants (80%) with HVL greater than 1000 copies/mL, resulting in a confirmed RHI prevalence of 4% (24 out of 599) (Figure 1).
Risk factors associated with recent HIV infection.

aOdds Ratios (OR) and 95% confidence intervals (CI) obtained from logistic regression.
bAdjusted for baseline covariates shown, participants with missing data for any of the variables excluded, N = 435.
Pretreatment HIV-1 drug resistance mutations
Distribution of pretreatment drug resistance mutations- and HIV-1 subtype(s) among people with recent HIV-1 infections.

NNRTIs: non-nucleoside reverse transcriptase inhibitors; NRTIs: nucleoside reverse transcriptase inhibitors; PIs: protease inhibitors.
Discussion
In this study conducted at a rural referral hospital in Tanzania, we observed a relatively low prevalence of RHI among newly diagnosed PLHIV, at 4%. Although we did not identify specific factors associated with RHI, we observed a high proportion of PDR mutations among people with recent infection.
The RHI prevalence in our study is lower compared to other studies in the region.22–25 One possible explanation is that most PLHIV in this rural SSA setting tend to seek care late, often when HIV disease is advanced, which may contribute to ongoing transmission and challenges in reducing new infections. Additionally, the referral status of our hospital, which receives patients either referred from lower-level facilities or those presenting with severe illness, may partially explain the lower RHI prevalence observed in our study. It might also be a reason for the high proportion of individuals with recent infection who had advanced clinical disease (i.e., WHO stage III/IV) and low CD4 counts at presentation. 26 In contrast, community-based studies report higher RHI rates; for example, a door-to-door survey in rural Lesotho found an RHI prevalence of 7%, 24 and a study in a fishing community along Lake Victoria, Tanzania, reported 7.4%. 25
Previous studies have identified female sex, younger age, higher education, and marital status as risk factors for RHI in SSA.22–25,27,28 In contrast, our study did not find significant associations between these factors and RHI, likely due to the small number of recent infections. The median age of participants with RHI was 37 years, indicating that new infections may be occurring across at broader age range than previously thought, possibly due to continued risk exposures among older adults and due to late presentation. Other established risk factors—such as engagement in sex work, contact with an HIV-positive partner, and illicit drug use 22 —were not systematically captured in the KIULARCO cohort.
Importantly, one-third of participants with RHI exhibited PDR, which is higher than what we previously reported in the same population among general ART-naive PLHIV. 29 This prevalence is also higher than findings from similar studies conducted in rural African settings among ART-naive PLHIV.30,31 Despite the limited sample size this relatively high proportion of drug resistance mutations is noteworthy and may indicate that people diagnosed with RHI should be a key focus in estimating the burden of PDR. 32 In our rural referral hospital cohort, the highest PDR rates were found for NNRTIs (25%), which have recently been largely replaced by the integrase inhibitor dolutegravir in most SSA countries. The widespread presence of NNRTI resistance could pose a risk to the long-term efficacy of dolutegravir-based regimens, as prior NNRTI resistance has been associated with failure of first-line dolutegravir-based regimens, although the exact mechanisms remain unclear. 33 This underscores the importance of resistance testing before initiating ART.
Furthermore, the prevalence of PDR to NRTIs among individuals with RHI was 12.5%, substantially higher than the 2.5% pooled estimate from our recent systematic review of PDR prevalence in Eastern Africa. 34 Because NRTIs serve as the backbone of dolutegravir-based regimens, resistance to these drugs increases the risk of functional monotherapy, potentially leading to the emergence of dolutegravir resistance, 35 which poses a significant public health threat.
To our knowledge, this is the first study reporting PDR among people with RHI in Tanzania. Several limitations should be noted. First, sequencing was performed only for RHI participants, targeting the RT and protease PR regions, while integrase sequencing was not conducted due to resource constraints. Non-RHI participants were not sequenced and therefore did not serve as a control group. However, existing local data indicate a very low prevalence of INSTI resistance among ART-naïve PLHIV, particularly during the early phase of INSTI-based ART rollout, which coincides with our sampling period (2019–2022). Supporting this, our recent systematic review and meta-analysis of PDR in Eastern Africa (2017–2022) found no major INSTI resistance among ART-naive adults. 34 Similarly, our recent study assessing PDR among individuals experiencing virological failure on dolutegravir-based ART within the same cohort found no evidence of INSTI resistance prior to ART initiation. 29
Second, as a referral hospital study, the RHI prevalence may be underestimated. Third, the small sample size limits our ability to identify risk factors for PDR in people with RHI. Forth, we relied on the Asante HIV-1 rapid recency assay, which, despite initial reports of high sensitivity and specificity,19,36 has demonstrated variable accuracy in some studies. 37
To reduce false positives, viral load testing was incorporated, but visual interpretation of faint assay bands remains subjective and may have led to misclassification. Fifth, PCR amplification and genotypic testing were successful in only 67% of RHI cases, likely due to sample storage issues. Genotypic resistance was assessed using standard Sanger sequencing; the use of ultra-sensitive deep sequencing might have revealed higher rates of drug resistance mutations. Finally, ART history was based on self-report, and it is possible that some individuals classified as having PDR may have had prior ART experience that was not declared. We believe that the use of the term PDR appropriately accounts for this uncertainty and aligns with current WHO guidance for surveillance in similar contexts. 38
Conclusion
This hospital-based cross-sectional study in a rural setting found a 4% prevalence of RHI, underscoring the need for strengthened strategies for early HIV detection and improved linkage to care and treatment—key steps toward achieving the UNAIDS 95-95-95 targets. Although we could not do a direct comparison with non-RHI participants, the observed prevalence of PDR among people with RHI is notable and may have public health implications. These findings should be considered when interpreting the overall burden of PDR, particularly in populations with recent HIV infection.
Footnotes
Acknowledgements
We are deeply grateful to all the patients and staff at the Chronic Diseases Clinic of Ifakara (CDCI) for their participation and support. We also thank the funders of the clinic: the Ministry of Health of Tanzania, the Government of the Canton of Basel, the Swiss Tropical and Public Health Institute, and the Ifakara Health Institute. We extend our sincere appreciation to the National AIDS Control Programme for facilitating the donation of 600 Asante HIV-1 Rapid Recency Tests. Special thanks go to all members of the KIULARCO Study Group for their invaluable contributions.
Authors’ contributions
AJN, JMF, JK, and MW conceptualized the study and designed the experiments. AJN and DM performed the experiments. AJN, JO, and FV analyzed the data. AJN drafted the manuscript. JMF, DM, RN, PSN, JO, FV, DP, JK, and MW critically reviewed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No—G-19-57145), SIDA (Grant No: 54100113), Uppsala Monitoring Centre and the DELTAS Africa Initiative (Grant No: 107768/Z/15/Z). The DELTAS Africa Initiative is an independent funding scheme of the African Academy of Sciences (AAS)’s Alliance for Accelerating Excellence in Science in Africa (AESA) and supported by the New Partnership for Africa’s Development Planning and Coordinating Agency (NEPAD Agency) with funding from the Wellcome Trust (UK) and the UK government. AJN and RN were supported by the Integrated Diagnostic and Sequencing Platform (IDSP) project, funded by the Canton of Basel-Stadt. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.