
Abstract
To the Editor:
The landscape of HIV treatment has profoundly changed with the introduction of long-acting injectable (LAI) antiretroviral therapy (ART). Registrational trials and cohort studies have demonstrated that LAI cabotegravir-rilpivirine (CAB-RPV) is efficacious, with low rates of virologic failure (VF). 1,2 Despite consistent efficacy data, operationalization of LAI ART in clinical settings is variable. One such area of variability involves the role of proviral sequencing in identifying those at risk for VF with LAI ART.
Use of proviral sequencing has historically been controversial, largely due to the method’s low sensitivity—sampling ∼0.001% of total body CD4+ T cells—and uncertainty around the relevance of identified mutations and assay cost. 3 Although use was uncommon and sporadic in the contemporary ART but pre-LAI era, it has seen renewed uptake in the LAI era, including at our institution. 4 At the University of Washington (UW), the GenoSure Archive Monogram Biosciences (Labcorp, South San Francisco, CA, USA) proviral sequencing assay is used. An analysis of test utilization across the UW system showed that 12 tests were ordered between 2015 and 2021. In contrast, from the approval of CAB-RPV in 2021 through July 1, 2025, 77 tests were ordered, many to evaluate candidacy for CAB-RPV. Despite this increase, the clinical utility of proviral sequencing has remained unclear, underscoring the need for real-world data to guide its use in LAI CAB-RPV initiation.
At the Madison Clinic at Harborview Medical Center in Seattle, WA, a Ryan White-funded HIV primary care clinic serving the majority of persons with HIV (PWH) on CAB-RPV within the UW system, we incorporated parsimonious use of proviral sequencing in the medical eligibility evaluation for persons virally suppressed on oral ART interested in switching to LAI CAB-RPV. We used early literature regarding potential risk factors for VF with LAI CAB-RPV, including body mass index (BMI) ≥ 30 kg/m2, HIV subtype A6 (documented or suspected based on epidemiological risk), and RPV-associated resistance-associated mutations (RAMs) detected by genotypic testing of plasma viral RNA or “archived” integrated proviral sequences, to inform decision-making. 5,6
We performed a retrospective single-center review of all persons at the Madison Clinic referred for LAI CAB-RPV from May 2021 to July 2025. The UW Institutional Review Board reviewed this study and granted a consent waiver and allowed review of medical records (STUDY00020107). Records for all 263 persons with a referral reviewed by the Madison Clinic team as of July 1, 2025, were manually reviewed to determine the reason for LAI CAB-RPV treatment initiation or deferral and what, if any, additional testing was recommended (Fig. 1). Given the potential consequences of VF on LAI CAB-RPV and limited early data—while still recognizing the unproven utility of proviral sequencing—we began with a measured approach whereby proviral sequencing was recommended only for virally suppressed PWH who lacked relevant resistance or subtype data and had additional risk factors for VF. 5 In contrast, individuals with viremia were managed using more lenient eligibility criteria.
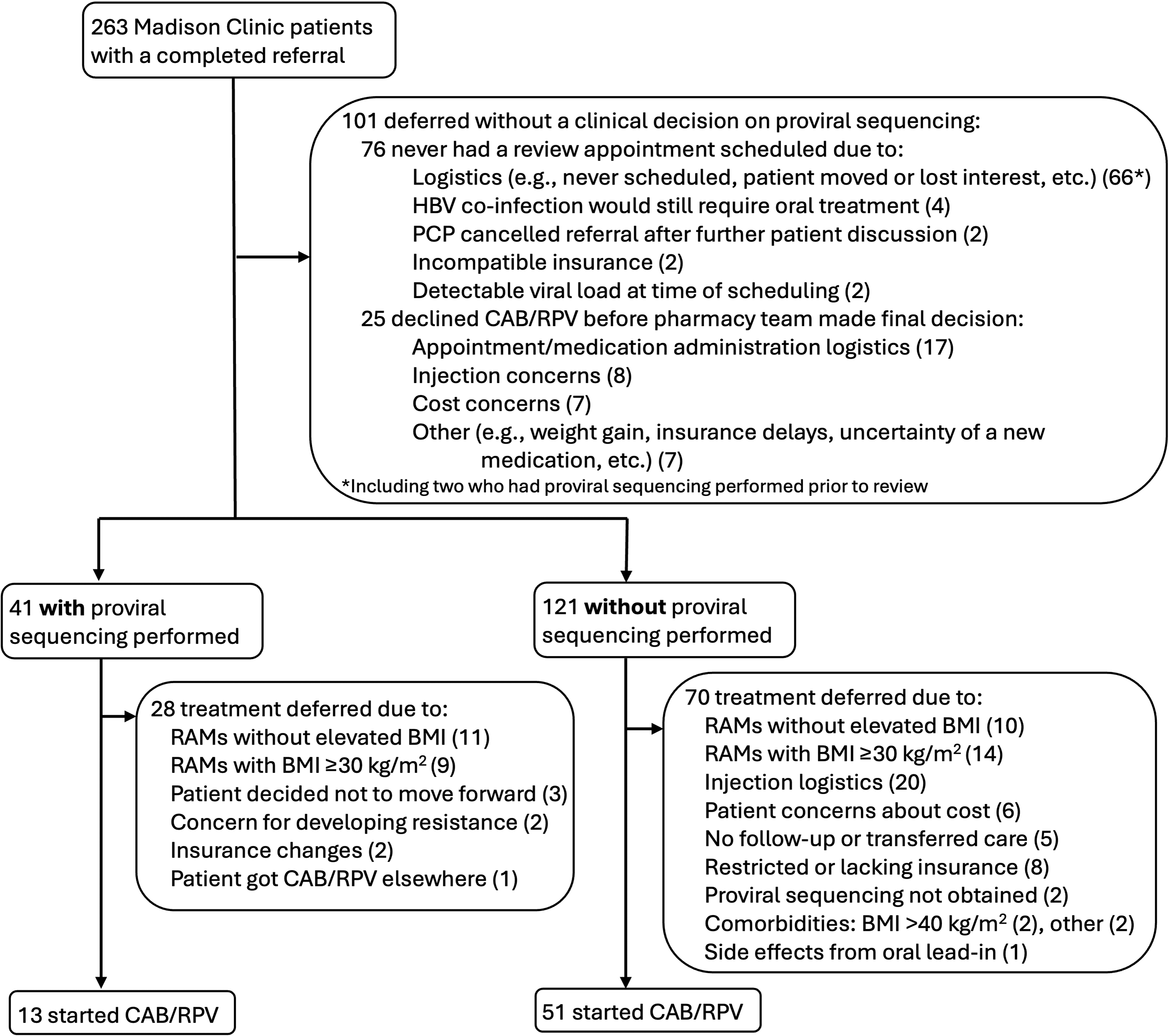
Diagram for long-acting injectable CAB-RPV referrals at the Madison Clinic. CAB-RPV, cabotegravir-rilpivirine.
Sixty-four PWH (from 263 referrals) initiated LAI CAB-RPV at the Madison Clinic between May 2021 and July 2025 (Fig. 1). Proviral sequencing was recommended and performed for 41 of the 263 (16%) to identify “archived” RAMs and HIV subtype prior to making a treatment decision. Of those 41 persons, 13 (32%) started CAB-RPV and 20 (49%) were deferred, in part due to identification of potential RAMs by proviral sequencing (Table 1). Potential RAMs were identified using the 2022 and 2024 Ward 86 protocol mutation lists and the Stanford resistance database. 7 –9 The classification of a mutation as a potential RAM depended on when testing was performed, as the list of relevant RAMs in the Ward 86 protocols and Stanford resistance database changed over time. 7,8 The term “defer” was used intentionally, as patients were counseled that therapy would be reconsidered as additional data, including the possible reclassification of potential RAMs, emerged.
Pre-Long-Acting Injectable (LAI) Cabotegravir-Rilpivirine (CAB-RPV) Demographics and Risk Factor Assessment in Madison Clinic Persons with HIV (PWH) with Full Pharmacy Review and Decision Regarding Proviral Sequencing
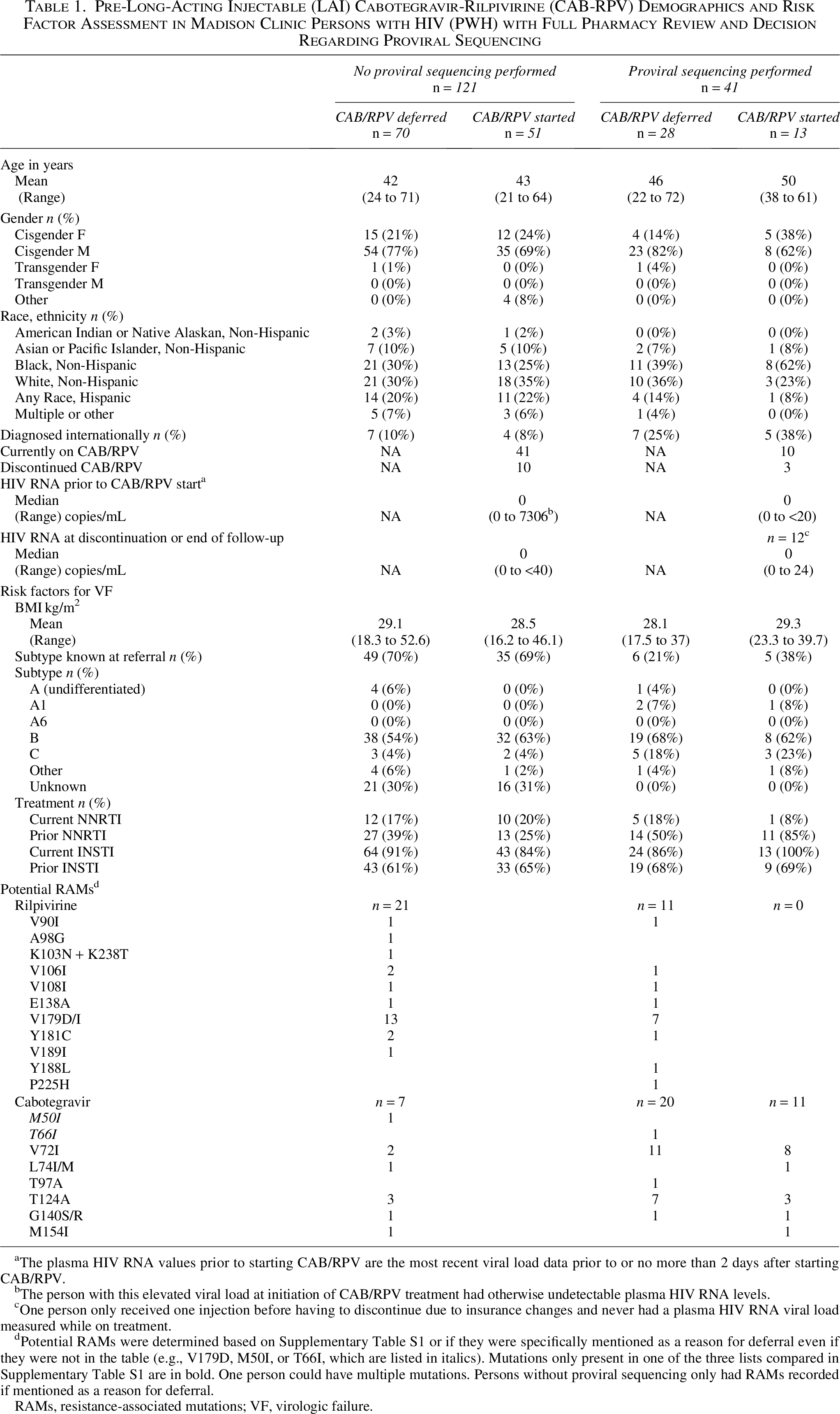
The plasma HIV RNA values prior to starting CAB/RPV are the most recent viral load data prior to or no more than 2 days after starting CAB/RPV.
The person with this elevated viral load at initiation of CAB/RPV treatment had otherwise undetectable plasma HIV RNA levels.
One person only received one injection before having to discontinue due to insurance changes and never had a plasma HIV RNA viral load measured while on treatment.
Potential RAMs were determined based on Supplementary Table S1 or if they were specifically mentioned as a reason for deferral even if they were not in the table (e.g., V179D, M50I, or T66I, which are listed in italics). Mutations only present in one of the three lists compared in Supplementary Table S1 are in bold. One person could have multiple mutations. Persons without proviral sequencing only had RAMs recorded if mentioned as a reason for deferral.
RAMs, resistance-associated mutations; VF, virologic failure.
After a median treatment duration of 14.2 months (range 1–42), with at least 3 months of follow-up for each person who started LAI CAB-RPV, all 64 PWH who started LAI CAB-RPV maintained viral suppression, regardless of whether pretreatment proviral sequencing was performed. There were no treatment failures, defined as ≥2 consecutive HIV RNA levels ≥ 200 copies/mL. Low level viremia was identified in 19 persons (median 25 copies/mL, range 21–142 copies/mL). Despite successful viral suppression, 13 of the 64 who started LAI CAB-RPV discontinued treatment prior to October 1, 2025, due to pain (n = 3), logistical challenges including moving/transferring care (n = 6), insurance changes or high copays (n = 3), or concerns about elevated triglycerides (n = 1).
In this cohort, individuals who underwent proviral sequencing were significantly more likely to be diagnosed with HIV internationally (p = 0.003, z-test) or have had prior exposure to a non-nucleoside reverse transcriptase inhibitor (NNRTI) (p = 0.003, z-test) and significantly less likely to know their HIV subtype prior to referral (p < 0.001, z-test) than persons whose review was completed without this additional testing (Table 1), consistent with our testing criteria.
Our rate of proviral sequencing utilization was lower than that reported in a large cohort study in which proviral sequencing was obtained in 35% (135/383) of referrals but similar to another single center in the UK that described a utilization rate of 13% and a review process akin to ours. 10,11 Even at these rates, our proviral sequencing trends represent a nontrivial increase in testing volume and associated costs, which in part motivated this evaluation.
Although a thorough eligibility review process can limit the need for proviral sequencing, its necessity remains uncertain in this evolving therapeutic area. In the setting of limited early data and the clinical equipoise in a switch to LAI among individuals virally suppressed on oral ART, we initially adopted a cautious approach. Overall, our findings demonstrate excellent viral suppression within our injectable ART program. Proviral sequencing was obtained in 16% of referred patients, reflecting a targeted strategy informed by early literature identifying risk factors for VF. 5 Notably, proviral sequencing identified potential RAMs in some individuals who were ultimately successfully treated with LAI CAB-RPV, most of which occurred at polymorphic sites (Table 1). This finding underscores the evolving interpretation of proviral RAMs and the importance of incorporating nuanced shared decision-making, particularly as integrase inhibitor-based regimens expand globally. 12
Recent work by Mazzitelli and colleagues further highlights the unpredictability of VF on CAB-RPV. 12 In their analysis of 94 cases of VF, only 4.4% met the threshold of ≥2 baseline risk factors. 5,13 These findings suggest that treatment failure can occur even among individuals considered low risk for VF. The authors also note the growing use of proviral HIV-DNA sequencing and call into question its routine utility, cautioning against misinterpretation of archived resistance; for example, integrase RAMs such as G140R may reflect apolipoprotein B mRNA editing catalytic polypeptide-like (APOBEC) -induced hypermutation rather than true drug resistance. 13
As eligibility criteria and guidelines continue to evolve, practices surrounding proviral sequencing remain heterogenous, and its role in treatment decision making remains uncertain. Although our approach has been conservative, use of proviral sequencing nonetheless increased relative to historical practice; based on our internal review, we expect a reduction in its use moving forward, with even more judicious utilization and cautious interpretation. In light of emerging data demonstrating the unpredictability of VF with CAB-RPV, we continue to reassess the extent to which proviral sequencing is necessary at all. 13
Authors’ Contributions
All authors contributed to this work: data collection (K.H.D.C., R.G.K., J.L., M.P., R.L., and J.Z.B.), project ideation (K.H.D.C., R.G.K., A.L.G., L.M.F., and J.Z.B.), article—initial writing (K.H.D.C., R.G.K., A.L.G., L.M.F., and J.Z.B.), and article—editing (K.H.D.C., R.G.K., J.L., M.P., R.L., A.L.G., S.D., L.M.F., and J.Z.B.).
Footnotes
Acknowledgments
The authors would like to thank Drs. Elaine Thomas and Julie Dombrowski for their thoughtful discussions regarding their expedited review process for viremic persons with HIV at the Max Clinic.
Ethical Considerations
The UW Institutional Review Board reviewed this study and granted a consent waiver and allowed review of medical records (STUDY00020107).
Data Availability
The dataset generated from chart review for this study is not publicly available to protect protected health information. Please contact the authors to discuss any reasonable data requests.
Author Disclosure Statement
A.L.G. reports contract testing to UW from Abbott, Cepheid, Novavax, Pfizer, Janssen, and Hologic and research support from Gilead, outside of the described work. The remaining authors report no conflicts of interest.
Funding Information
This work was performed without specific grant funding.