
Abstract
Social difficulties are frequently cited as a core deficit of individuals with Asperger syndrome (AS). This deficit is particularly evident when processing of emotional information is required in social situations. Deficits in theory of mind and executive functions are the two explanatory hypotheses for social deficits in AS that are predominant in the literature; however, each of these explanations has limitations. Emotional intelligence (EI) has emerged as a relatively new explanation for social difficulties in typically developing individuals. Recently, researchers also have demonstrated that EI predicted important social outcomes for individuals with AS. In this study, we explored EI as an alternative or additive explanation for the social deficits observed in young adults with AS in light of the two predominant theories accounting for social difficulties. Implications for practice are discussed.
Keywords
Asperger syndrome (AS), an autism spectrum disorder (ASD), is characterized by “marked and enduring impairments” (Klin, McPartland, & Volkmar, 2005, p. 88) in social interaction, communication, behavior, and language. Unlike “classical” autism (Frith, 1991), individuals with AS demonstrate average to superior intelligence (Wing, 1981) as well as typically developing early language (Szatmari, 2005). Hallmark features of AS include highly specialized skills and circumscribed interests; however, difficulties with social interaction are central to the various clinical diagnostic criteria for the disorder (e.g., American Psychiatric Association [APA], 2000). Deficits in theory of mind (ToM) and/or executive functions (EFs) are two of the most commonly cited explanations for impaired social functioning in AS and in other ASD subtypes.
Although ToM and EF approaches provide valuable information regarding the nature of AS in general, these models have limitations in their prediction of social outcomes in AS (Joseph & Tager-Flusberg, 2004; Klin, 2000), which may be remedied by exploring another important construct. In two recently published studies, we examined emotional intelligence (EI) in AS and found that trait EI was impaired, whereas ability EI remained largely intact (Montgomery et al., 2008; Montgomery, McCrimmon, Schwean, & Saklofske, 2010). In the current study, we examined whether scores obtained from tests measuring ToM, EF, and EI predict, either singularly and/or in combination, social and adaptive outcomes.
A critical limitation of the research examining ToM and EF for explaining social deficits in AS is that researchers typically have described the abilities of individuals within the broader category of ASD. This may be because individuals with AS are often recruited along with others on the autism spectrum to increase sample sizes (cf. Mottron, 2004). Although this research practice is understandable, it is important to remember that AS is currently recognized as a distinct subtype (APA, 2000) in a group of highly heterogeneous conditions, and that in quantitative research, the broader and more diverse the group, the more difficult it is to identify patterns and characteristics. Given the current subtypes, there is interest in exploring the abilities of people with AS to gain insight into this specific ASD group and into the most effective ways to support affected individuals (cf. Baron-Cohen & Klin, 2006). Thus, a second goal of our research was to examine ToM, EF, EI, and social outcomes within a more homogeneous group, specifically young adults with a diagnosis of AS.
ToM
The ToM hypothesis for social deficits in ASD suggests that a “specific, and primarily cognitive, incapacity to attribute mental states such as beliefs, intentions, and desires to the other and self” (Klin, 2000, p. 831) is responsible for social deficits. ToM dysfunction is further proposed to account for a variety of autistic-like symptoms, including deficits in pragmatic language, imaginative play, and empathy (Baron-Cohen, 1995). Although this theory may partly explain the observed behavior in lower functioning individuals on the autism spectrum, some have questioned the ability of the ToM hypothesis to account for the characteristics seen in higher functioning individuals as they may succeed on first-level ToM tasks (Baron-Cohen, Jolliffe, Mortimore, & Robertson, 1997; Dahlgren & Trillingsgaard, 1996) and even demonstrate intact ToM skills in naturalistic contexts (Eisenmajer & Prior, 1996). Others assert that strong verbal skills regulate performance on verbally based ToM tasks (see Eisenmajer & Prior, 1991; Happe, 1994); consequently, individuals with higher verbal skills, such as those diagnosed with AS, could be expected to pass verbal ToM tasks (Klin, 2000). In studies where verbal ability was entered as a covariate, ToM did not predict severity of social impairments in children (Capps, Kehres, & Sigman, 1998; Joseph & Tager-Flusberg, 2004), adolescents, or adults (Fombonne, Siddons, Archard, Frith, & Happe, 1994) with ASD. Moreover, individuals with AS who pass ToM tasks in experimental situations are likely to do so because social stress is reduced and the processing speed demands for integrating social information are less important than in real time (Klin, 2000).
The specificity of ToM for explaining social outcomes in AS also has been questioned as ToM deficits have been observed in other clinical groups such as those with schizophrenia, intellectual disability, and deafness (Corcoran, Mercer, & Frith, 1995; Peterson & Seigal, 1995; Yirmiya, Sigman, Kasari, & Mundy, 1992). Furthermore, although ToM ability and social competence correlate in typically developing children (Liddle & Nettle, 2006), this relationship appears to break down in ASD (Bowler & Thommen, 2000). Moreover, improvement in ToM skills after targeted interventions does not appear to correspond with increased social capabilities (Hadwin, Baron-Cohen, Howlin, & Hill, 1996; Ozonoff & Miller, 1995). Thus, although somewhat helpful to articulate the difficulties that individuals with AS may have understanding others, the evidence does not support ToM deficits as the primary cause of social difficulties in individuals with AS, particularly in adolescents and young adults (Spek, Scholte, & Van Berckelaer-Onnes, 2010).
EFs
EFs are neuropsychological processes involved in overlapping and complex cognitive functions which include planning, cognitive and behavioral flexibility, inhibition, selective attention, and working memory (see Luria, 1966). From this neuropsychological perspective, effective social interaction requires ongoing updating, evaluation, and selection of appropriate responses to verbal and nonverbal social information (Landa & Goldberg, 2005). Previously, researchers have demonstrated that individuals with AS demonstrate deficits on EF tasks, specifically those examining planning, cognitive flexibility, and generativity (Ambery, Russell, Perry, Morris, & Murphy, 2006; Ozonoff, Rogers, & Pennington, 1991; Verte, Guerts, Roeyers, Ooosterlaan, & Sergeant, 2006). However, some researchers have reported no differences in EF performance or mixed results in this population (Manjiviona & Prior, 1999; Miller & Ozonoff, 2000; Rinehart, Bradshaw, Moss, Brereton, & Tonge, 2001). Even in light of mixed results, some posit that it is the difficulties in EF that lead to poor social interaction (Ozonoff, 1997; Solomon, Goodlin-Jones, & Anders, 2004).
Although the EF explanation for social impairments is intuitively sensible, there has been surprisingly little research directly examining EF and its relationship with social outcomes in clearly defined groups of individuals with AS, and in particular, young adults with AS (cf. Ambery et al., 2006). Researchers who have investigated the relationship between the two constructs in AS have not demonstrated significant relationships between them (Joseph & Tager-Flusberg, 2004; Landa & Goldberg, 2005). Consequently, as with ToM, there is little evidence to suggest that problems in EF alone can explain the difficulties that individuals with AS experience in social situations. Given this, it is important to examine whether another construct together with ToM and EF would provide a clearer picture of the nature of the social challenges faced by young adults with AS.
EI
EI is currently conceptualized by two predominant approaches, ability EI and trait EI, which appear to be distinct from personality and general intellectual ability (Brackett & Mayer, 2003; Lopes, Salovey, & Straus, 2003). Ability EI is an interrelated set of cognitive abilities, skills, or capacities that include recognizing the meanings of emotion and the complex relationships between emotions, reasoning, and problem solving on the basis of this information (Mayer, Caruso, & Salovey, 2000). Ability EI positively correlates with self-reported empathy (Ciarrochi, Chan, & Caputi, 2000), life satisfaction, self-reported relationship quality (Ciarrochi et al., 2000; Lopes et al. 2004), and successful social interactions (Lopes et al., 2003), which are all important outcomes that theoretically or directly relate to successful social functioning. Indeed, ability EI also appears to inversely predict social deviance (Brackett & Mayer, 2003).
Trait EI, however, is a series of related competencies in emotion-related areas that may include characteristics such as optimism, self-awareness, self-esteem, and self-actualizations (Bar-On, 1997). Researchers have shown that trait EI demonstrates incremental validity over personality in the prediction of life satisfaction, social network quality, loneliness, and depression-proneness (Palmer, Donaldson, & Stough, 2002; Saklofske, Austin, & Minski, 2003). Inverse associations between trait EI and alexithymia (Parker, Taylor, & Bagby, 2001), psychological distress (Slaski & Cartwright, 2002), and depression (Dawda & Hart, 2000) also have been demonstrated.
As ability and trait EI approaches have been shown to predict important social outcomes in typically developing individuals (Lopes et al., 2004), these two EI models may be useful in explaining the social difficulties that individuals with AS experience in their daily lives. Indeed, Asperger himself noted a “dissonance of cognition and affect” (Frith, 1991, p. 79) for the individuals he studied, and others have noted that individuals with AS have problems processing emotional information. However, there is little documentation linking affective processing with difficulties in social interaction in this population. In what we believe to be the first study of its kind, we demonstrated that individuals with AS were significantly impaired in trait EI, whereas ability EI remained largely intact (Montgomery et al., 2010). Specifically, our AS group reported impaired EI characteristics and performance in emotional interactions in real-life settings but showed intact cognitive skills in relation to emotional information. Clearly, EI is an important determinant of social functioning in individuals with AS. Thus, an important step in understanding the nature of the social impairments observed in AS is to determine whether EI serves as a better predictor or is one of several predictors, including ToM and EF, of social difficulties. The primary purpose of the current study is to explore these two possibilities.
Method
The participants, some of the materials, and the procedures have been described in detail in a previous study (Montgomery et al., 2010) and are summarized below.
Participants
Twenty-five adolescents and young adults (20 males, 5 females) diagnosed with AS (M =18.2 years; SD = 1.38 years; range = 16-21 years) were recruited from schools, mental health settings, and advocacy groups in Manitoba and Alberta, Canada. All participants had an official diagnosis of AS made by a psychiatrist or psychologist and had a verbal IQ ≥ 85. To provide validation of the diagnosis of AS, parents of each participant were asked to (a) document the onset of and quality of language development, and (b) complete the Krug Asperger Disorder Index (KADI; Krug & Arick, 2003). Participants were excluded from the study if a parent reported language delays (i.e., no single words by age 2 years, no phrases by 3 years of age), or if parents could not recall whether their children met the language milestones. In addition, a KADI score ≥ 70 was considered sufficient validation of the participant’s original diagnosis. Participants with comorbid conditions were not excluded unless the condition interfered with their ability to complete the experimental tasks (e.g., selective mutism).
Materials and Procedures
Informed consent (per approved human ethics board protocols at the Universities of Calgary and Manitoba) was obtained from all participants. Participants were assessed by trained graduate student clinicians at the aforementioned sites. Most participants attended one session, but if needed, two visits were scheduled for the assessment battery which typically lasted 4 to 6 hr. Verbal IQ was assessed with the Similarities and Vocabulary subtests from the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999). Upon completion of the WASI, participants completed the Eyes Test–Revised (Baron-Cohen, Wheelwright, Hill, Raste, & Plumb, 2001), four subtests from the Delis–Kaplan Executive Function System (D-KEFS; Delis, Kaplan, & Kramer, 2001), the Bar-On Emotional Quotient Inventory–Short Form (Bar-On EQ-i:S; Bar-On, 2002), the Mayer–Salovey–Caruso Emotional Intelligence Test (MSCEIT; Mayer, Salovey, & Caruso, 2002), and the Behavior Assessment System for Children (2nd ed.; BASC-2; Reynolds & Kamphaus, 2004) in a randomized order. Following the experimental session, participants were given a modest honorarium. Parents of participants were sent the KADI (Krug & Arick, 2003) forms in the mail and returned completed forms in a postage paid addressed envelope.
The Eyes Test–Revised (Baron-Cohen et al., 2001) is an advanced ToM test consisting of 25 items. Individuals examine black and white pictures of the eye region of faces and choose one of four words that best describes the emotion conveyed in the eyes. The Eyes Test–Revised has been found to be sensitive to subtle differences in social sensitivity or “mind-reading” (Baron-Cohen et al., 2001) and is considered to be a social-perceptual measure of ToM (Ferguson & Austin, 2010).
The D-KEFS (Delis et al., 2001) is a measure of executive processes, including planning, reasoning, cognitive flexibility, fluency, and inhibition. The D-KEFS subtests are modifications of well-known traditional tests of EF (Lopez, Lincoln, Ozonoff, & Lai, 2005), but differ from traditional measures in that baseline conditions are provided for each task. This differentiation facilitates the isolation of basic cognitive processes (e.g., motor speed and visual scanning skills) to determine “whether poor performance is due to deficits in more fundamental cognitive skills or deficits in higher-level executive functions” (Delis et al., 2001, p. 3). The core EF tasks for this study were as follows: trail making 4 (letter-number switching; TM4), verbal fluency 3 (category switching total correct; VF3), color-word interference 3 (inhibition; CW3), and color-word interference 4 (inhibition-switching; CW4).
The Bar-On EQ-i:S (Bar-On, 2002) is a self-report measure of trait EI for individuals aged 16 years and older. The measure consists of 51 items and takes approximately 10 to 15 min to complete. The EQ-i:S uses a 5-point Likert-type rating system and generates a total Emotional Quotient (EQ) composite score and seven EQ subscale scores: Intrapersonal, Interpersonal, Stress Management, Adaptability, General Mood, Positive Impression, and Inconsistency Index.
The MSCEIT (Mayer et al., 2002) is a 141-item multiple-choice self-report that takes 30 to 45 min to administer and is intended for use with individuals aged 17 years or older (though use with 16-year-olds is permissible). This ability-EI measure yields a single overall performance score, two area scores for Emotional Experience and Emotional Reasoning, and scores reflecting the four-branch model of EI: (a) perceiving emotions, (b) using emotions to facilitate thought, (c) understanding emotions, and (4) managing emotions to foster personal growth and healthy social relations.
The BASC-2 (Reynolds & Kamphaus, 2004) is a multidimensional inventory of behavior and self-perceptions for individuals 2 to 25 years of age. Two subscales from each of the self (Social Stress and Interpersonal Relations from the BASC-2: SRP) and parent (Social Skills and the Adaptive Composite from the BASC-2: PRS) reports were used in this study as they reflect social abilities as rated separately by the individual and a close caregiver.
The KADI (Krug & Arick, 2003) is a norm-referenced, clinician-administered, 32-item, third-party report designed to collect information on individuals aged 6 years to 21 years and 11 months. The KADI is a relatively reliable and valid screen for identifying individuals with AS (see Stoesz, Montgomery, Smart, & Hellsten, 2011) and can be completed in 5 to 10 min.
Results
The participants’ mean verbal IQ score was 114 (SD = 11.1), whereas the mean KADI score was 94.3 (SD = 12.7). A more detailed description of the participant characteristics and comorbidities can be found in Montgomery et al. (2010). The participants’ data were examined for normality, outliers, skew, and kurtosis. Results suggested that the scores were normally distributed and no outliers were present.
Comparison of ToM, EF, and EI Performance to Normative Data
Single sample t tests (two-tailed) were conducted to examine whether the AS group differed significantly from the normative samples presented in the manuals of the ToM, EF, and EI measures. For the Eyes Test–Revised, results revealed that our AS group scored significantly lower than the normative group, t(24) = −2.616, p = .015, and significantly better than the AS group in a validity study, t(24) = 3.634, p = .001. For the EF scales, the AS group showed a significant deficit on CW4, t(24) = −2.547, p = .018, and a trend toward significance on CW3, t(24) = −1.77, p = .09. They performed similarly to typical controls on VF3, t(24) = 1.422, p = .168, and TM4, t(24) = −1.365, p = .185. Previously, we documented that the same group of individuals with AS was impaired on the trait EI measure (Bar-On EQ-i:s), whereas their ability EI (MSCEIT) was intact or better than expected (see Montgomery et al., 2010). In addition, the AS group’s BASC-2 scores revealed a significant weakness on the parent-reported measure of Social Skills and the Adaptive Composite. Self-reported BASC-2 Social Stress and Interpersonal Relations scores were not significantly different from the clinical norms; however, we should note that for this measure, clinical norms compare our group with others with clinical conditions, not typically developing individuals and as such, reports likely underestimate difficulties.
Correlations Between Variables
The correlations (two-tailed) between the variables are presented in Table 1. A Bonferroni correction was not applied, as we consider this study to be exploratory. Findings indicated that neither age nor verbal IQ was significantly correlated with any of the variables in this study. Scores on the Eyes Test–Revised were also not correlated with any of the other variables. However, scores from two D-KEFS subtests (TM4 and VF3) were significantly correlated with the MSCEIT Total EIQ scores. We have previously reported that the BASC-2 self-report of Social Stress scores were negatively correlated with Bar-On EQ-i:S Total EQ and that significant positive correlations were demonstrated for the Bar-On-EQ-i:S Total EQ composite and participant’s self-report of Interpersonal Relations on the BASC-2 (see Montgomery et al., 2010).
Zero-Order Correlations Between Variables.
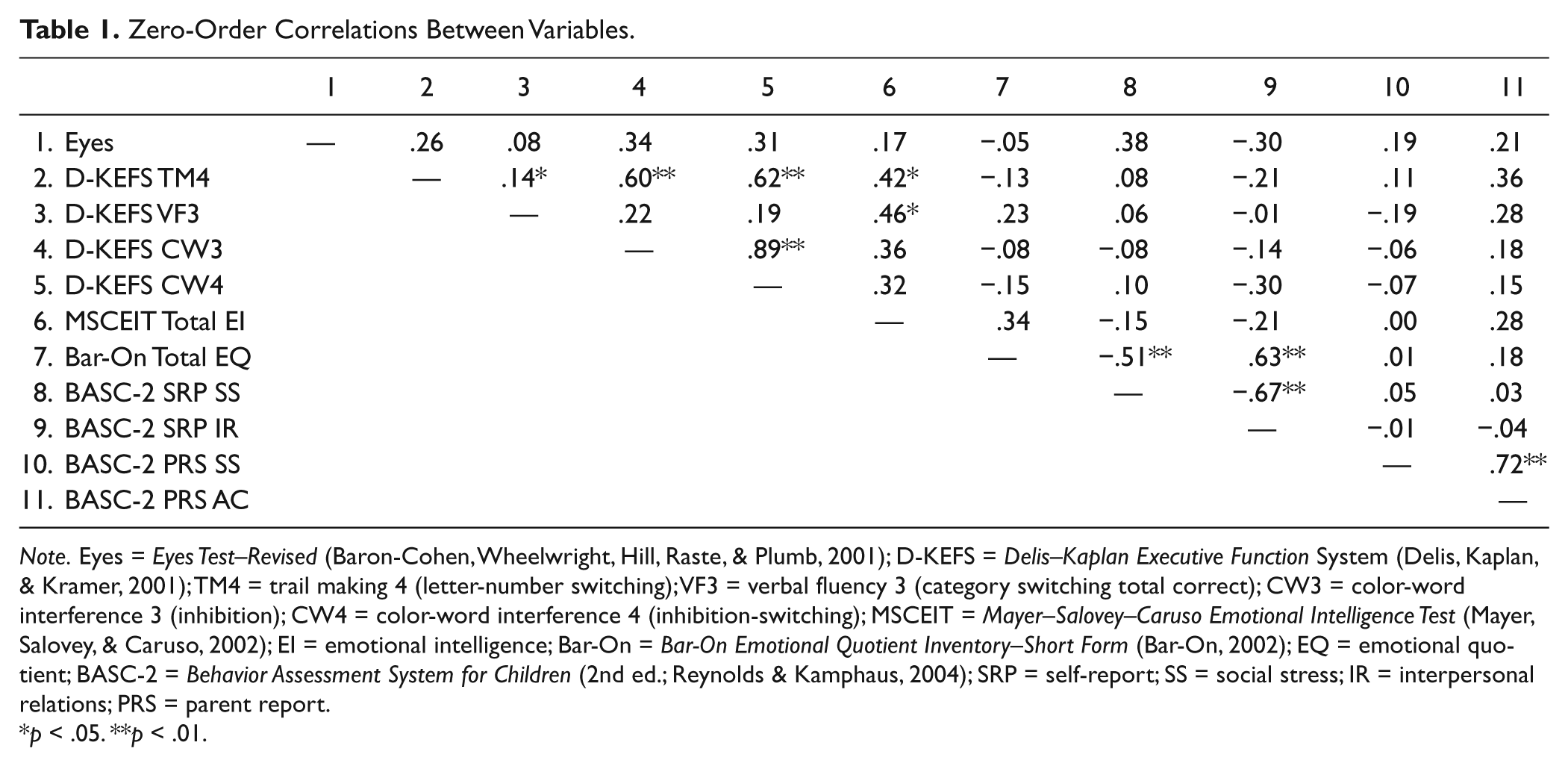
Note. Eyes = Eyes Test–Revised (Baron-Cohen, Wheelwright, Hill, Raste, & Plumb, 2001); D-KEFS = Delis–Kaplan Executive Function System (Delis, Kaplan, & Kramer, 2001); TM4 = trail making 4 (letter-number switching); VF3 = verbal fluency 3 (category switching total correct); CW3 = color-word interference 3 (inhibition); CW4 = color-word interference 4 (inhibition-switching); MSCEIT = Mayer–Salovey–Caruso Emotional Intelligence Test (Mayer, Salovey, & Caruso, 2002); EI = emotional intelligence; Bar-On = Bar-On Emotional Quotient Inventory–Short Form (Bar-On, 2002); EQ = emotional quotient; BASC-2 = Behavior Assessment System for Children (2nd ed.; Reynolds & Kamphaus, 2004); SRP = self-report; SS = social stress; IR = interpersonal relations; PRS = parent report.
p < .05. **p < .01.
Prediction of Social Outcomes
To examine prediction of social outcomes, a series of multiple regression equations was planned. As per guidelines for multiple regression (Tabachnick & Fidell, 2007), only those variables that were at least moderately correlated (>.30) with the outcome variables were retained. Using this criteria and the relevance of the variable to social outcomes, only two outcome variables were deemed appropriate for inclusion in the regression procedures: (a) BASC-2 Social Stress and (b) BASC-2 Interpersonal Relations (see Table 2).
Standardized Regression Coefficients for Predicting Model 1—Interpersonal Relations and Model 2—Social Stress.
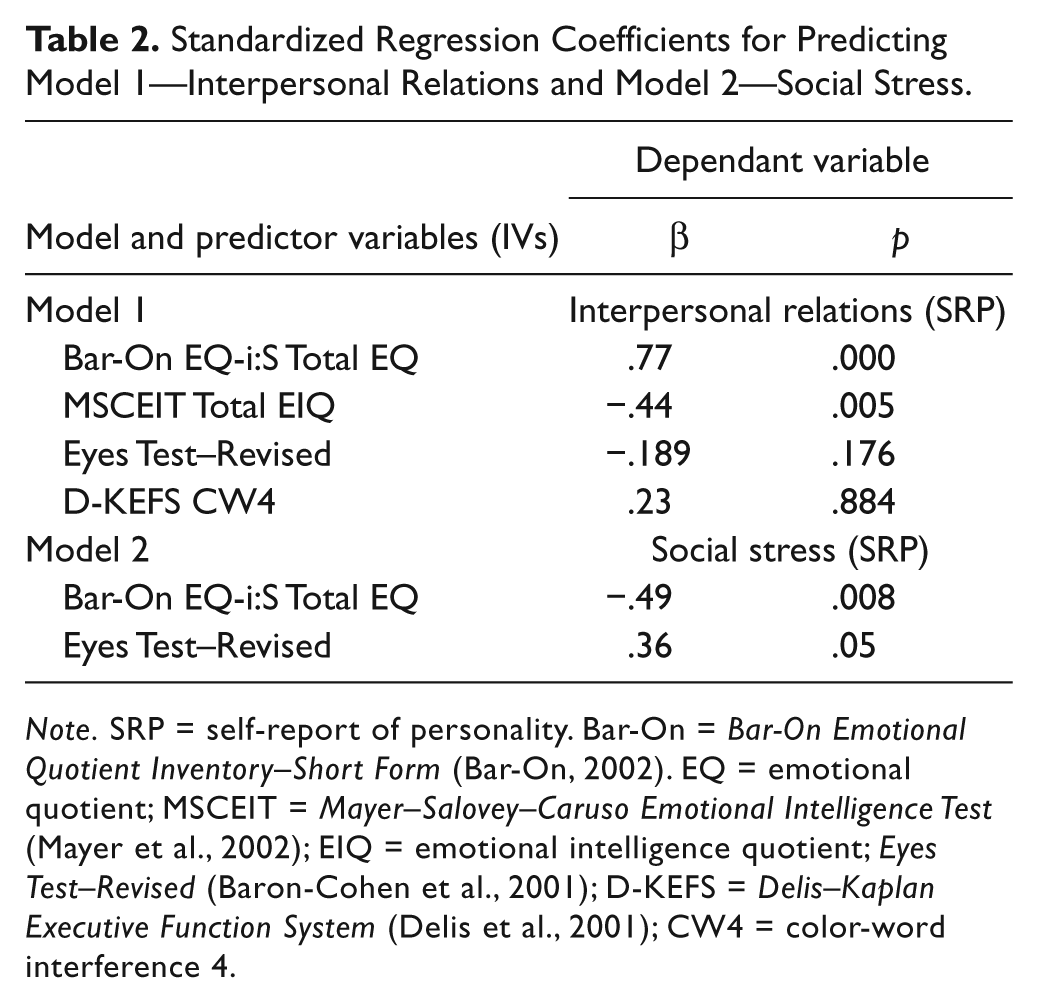
Note. SRP = self-report of personality. Bar-On = Bar-On Emotional Quotient Inventory–Short Form (Bar-On, 2002). EQ = emotional quotient; MSCEIT = Mayer–Salovey–Caruso Emotional Intelligence Test (Mayer et al., 2002); EIQ = emotional intelligence quotient; Eyes Test–Revised (Baron-Cohen et al., 2001); D-KEFS = Delis–Kaplan Executive Function System (Delis et al., 2001); CW4 = color-word interference 4.
The standard method was chosen for regression procedures as it is the most conservative and recommended approach for small samples sizes (Brace, Kemp, & Snelgar, 2006). A significant model emerged: F(3, 22) = 8.76, p < .000, with the model explaining 56% of the variance (adjusted R2 = .56) in Interpersonal Relations scores. Only the EI variables were significant predictors in this model (see Table 2). Multiple regression analysis was conducted to explore the prediction of social outcomes via the BASC-2 self-report of Social Stress. Again, a significant model emerged: F(2, 22) = 6.81, p =.005, with the model explaining 33% of the variance (R2 value) in Social Stress scores. Both the Bar-On EQ-i:S Total EQ and the Eyes Test–Revised were significant predictors in this model (see Table 2).
Discussion
ToM, EF, and EI in AS
We examined ToM, EF, and EI results and explored the ability of these constructs to predict social outcomes for individuals with AS. The AS group demonstrated more subtle ToM impairments than a combined AS/high-functioning autism (HFA) group (see Baron-Cohen et al., 2001); nevertheless, they showed significant impairments when compared with the normative group. Few sources have explicitly examined ToM in AS; however, our findings are consistent with the literature demonstrating that many individuals with AS have relatively intact ToM abilities (compared with those with autism) or are able to pass ToM tasks in laboratory settings (Bowler, 1992; Ziatas, Durkin, & Pratt, 1998). Nonetheless, the finding that our group demonstrated subtle impairments (compared with the mixed ASD group) may be an important consideration for clinicians and researchers alike.
In terms of EF, we examined core areas which have been put forth as problematic for those with AS: cognitive flexibility, verbal fluency, and inhibition. Investigations of cognitive flexibility in ASDs have generally found these to be consistent areas of difficulty (see Ozonoff, South, & Provencal, 2005). In contrast, some researchers have found that adults with AS show deficits in verbal fluency (Ambery et al., 2006), whereas others have found intact verbal fluency in children (Manjiviona & Prior, 1999) and young adults (McCrimmon, Schwean, Saklofske, Montgomery, & Brady, 2012). Some have reported difficulties with inhibition in adolescents and young adults (Kleinhans, Akshoomoff, & Delis, 2005; McCrimmon et al., 2012), whereas others have indicated the opposite (Ambery et al., 2006). However, the varied results between studies for some of the EFs may be impacted by differing operational definitions for AS (e.g., sometimes AS and HFA are combined), unique approaches to exclusion criteria, and differences in experimental tasks.
In the current study, we found that participants demonstrated weakness on a task of inhibition (CW3) and significant impairments on a task of combined inhibition and cognitive flexibility (CW4). However, they performed well on tasks of cognitive flexibility and fluency. It is important to note that many of our participants also reported a comorbid diagnosis of AD/HD. Individuals with AD/HD are thought to have a core deficit in inhibition (Barkley, 1997a, 1997b; Pennington & Ozonoff, 1996) and perform poorly on tests of inhibition, such as the Stroop task (Ozonoff & Jensen, 1999; Willcutt et al., 2001). While the AS and AD/HD populations have been reported to demonstrate impaired cognitive flexibility, some researchers have found that individuals with AD/HD have more severe impairments in this aspect of functioning than do those with ASD (Geurts, Verter, Oosterlaan, Roeyers, & Sergeant, 2004). In contrast, when participants with AD/HD or ASD were compared with age- and IQ-matched typically developing controls, individuals with ASD demonstrated less profound impairments than those with AD/HD (Happe, Booth, Charlton, & Hughes, 2006). Our results indicate that, while it was only approaching significance, inhibition appears to be the most impaired EF in our group. This was particularly marked when tasks also required cognitive fluency. Although the comorbidities in our group may be seen by some as a limitation to this research, we feel that our group may be a more accurate reflection of the everyday experiences of those with AS because of the inclusion of the commonly occurring coexisting conditions.
We previously reported that young adults with AS were impaired in trait EI but were not impaired on ability EI (see Montgomery et al., 2010). This finding suggested that when provided with the time to reason through information, young adults with AS were not impaired in the cognitive processes involved in decoding and responding to emotional situations. In contrast, the same group reported impairments in their actual social interactions involving emotional exchanges. Overall, these findings suggest that young adults with AS have the knowledge and cognitive ability to reason with emotional information, but their application in natural settings is impaired.
Predictors of Social Outcomes
Exploration using EI (Bar-On EQ-i:S Total EQ and MSCEIT Total EIQ), EF (CW4), and ToM (Eyes Test–Revised) as predictors of Interpersonal Relations was conducted. Surprisingly, neither ToM nor EF contributed to the prediction of this outcome variable. When ToM and trait EI (Bar-On EQ-i:S Total EQ) were explored as predictors of Social Stress, the resulting model predicted 33% of the variance, an improvement from our previous model using trait EI alone which predicted 19% of the variance in this outcome variable (Montgomery et al., 2010). Interpretively, it appears that increased ToM skills and less developed EI predicted social stress. These results suggest that ToM is useful for understanding perceived social stress in AS; however, it does not account for the poorer social interactions demonstrated by young adults with AS. The findings also support the assertion that EI predicts important social outcomes (Austin, Saklofske, & Egan, 2005; Brackett, Mayer, & Warner, 2004) and likely has implications for investigations of EI interventions for individuals with AS. ToM did not significantly contribute to the prediction of self-reported Interpersonal Relations. These results suggest that ToM is useful for understanding perceived social stress in AS; however, it does not account for their poor social interactions. The findings also support the assertion that EI predicts important social outcomes (Austin et al., 2005) and likely has implications for EI intervention research for individuals with AS.
Limitations
It is important to point out that our results should be interpreted with caution and considered preliminary at this stage for several reasons. First, we tested a relatively small sample and used an accessible, rather than randomly selected sample, which may limit the generalizability of our findings. Second, as noted above, our participants reported a high rate of comorbid AD/HD diagnoses. Although AD/HD and ASD cannot technically be comorbid (see Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV; APA, 1994]), recent investigations and revisions to the DSM criteria question this assertion, and it does indeed appear to be worthy of future research (e.g., Gargaro, Rinehart, Bradshaw, Tonge, & Sheppard, 2011). Finally, our social outcome measure for this study was limited in that it provided only clinical norms, meaning that in terms of deficit, our groups are compared only with other clinical groups and as such the nature of their impairments may be underemphasized.
Educational Implications
In light of the finding that our participants had intact ability EI, yet weak trait EI, we suggest that assessment of individual strengths, weaknesses, and skill sets is essential prior to implementing targeted programming. Moreover, our finding that ToM was relatively intact in our participants may also have implications for common interventions. For example, if improving both EI and ToM decreases social stress, then targeting both may be helpful. Furthermore, clinicians may find it helpful to include EI and ToM measures in their assessment batteries when the referral question is concerned with increased levels of social stress. However, in light of the finding that higher ToM scores predicted social stress, it will be important to consider strategies to buffer this phenomenon in intervention designs. For example, it may be necessary to teach individuals to expect to feel uncomfortable when they understand other’s perceptions better. In our clinical work, we have found that preparing individuals for “typical” reactions of others has indeed been beneficial in helping them to cope with their own increasing awareness of social feedback.
Our study also has implications for the individualizing interventions for those with AS. Assuming that individuals with AS have a similar profile of strengths and weakness as other groups of individuals on the spectrum may interfere with the success for interventions. For example, if an individual’s ability EI is intact, and interventions focus on teaching content that has already been mastered, not only is intervention time wasted, but it also makes it unlikely that individuals will “buy into” interventions. Consequently, we assert that it is inappropriate to assume all individuals have the same pattern as found in our participants, and as such, individual assessment prior to intervention is essential.
The finding that trait EI is weak for young adults with AS, combined with the likelihood that trait EI can be enhanced (Bar-On, 2003) and that it predicts important social outcomes (see Lopes et al., 2004) leads us to what we believe are the natural extensions of this research: the implementation of interventions to improve trait EI. As such, the most important implication of our research is the potential for interventions targeting trait EI to improve the lives of individuals with AS. Future researchers will examine this hypothesis.
Conclusion
Our primary purpose was to examine ToM, EF, and EI as predictors of social outcomes in AS. Results indicated that trait and ability EI, but not ToM, predicted self-reported Interpersonal Relations for young adults with AS; however, trait EI and ToM predicted self-reported Social Stress. Finally, although we expected that EF variables would be important predictors of Interpersonal Relations, our analysis revealed otherwise. Weak correlations between scores obtained from the EF and social skills measures were consistent with other research showing that EF predicted communication symptoms, but not social interaction difficulties in ASD (see Joseph & Tager-Flusberg, 2004). Thus, future researchers should focus on exploration of EF and social skills with specific ASD subgroups, including AS. Furthermore, measures of real-life social experiences would be helpful to understand the real-life implications for individuals. Despite limitations, the current study provides the first step in highlighting the importance of including EI along with other constructs in future research examining the social impairments in individuals with AS and points to the potential of EI interventions for improving social interactions for those with ASD. Not only will the information from EI measures advance research about the nature of social impairments in AS but will also help clinicians design appropriate assessment batteries and intervention strategies.
Footnotes
Acknowledgements
The authors gratefully acknowledge the following individuals for their assistance with data collection and other aspects of this project: Dr. Vicki L. Schwean, Dr. Don H. Saklofske, Danielle Brady, Yvonne Hindes, Keoma Thorne, Jo-Anne Burt, and Candace Kosak.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a grant from the Alberta Center for Child, Family, and Community Research.