
Abstract
The objective of the study was to examine the change in child homicides in Sweden between the 1990s and the 2000s based on a study of all cases registered during the periods 1990-1996 and 2002-2008. The results show a significant annual 4% decrease in the number of child homicides, with the main decline being due to a decrease in cases of filicide–suicide among both fathers and mothers. One possible explanation for the decrease may be the increases in the general prescription of antidepressant medication. However, other factors may also have played a significant role in the decline as well.
Introduction
The term child homicide is often used to denote the unlawful killing of an individual below the age of 15 (Lehti, Kääriänien, & Kiviuori, 2012; Pritchard, 2012; Yarwood, 2004). In many Western countries, child homicides have been found to account for 5% to 10% of all deaths among children below the age of 15, thereby making homicide at least about the fifth most common cause of death in this age group (Hjern & Bremberg, 2002; Pritchard & Sharples, 2008). In the research, child homicides are usually divided into a number of categories (cf. Lehti et al., 2012; Liem & Koenraadt, 2008; Yarwood, 2004), with the most well-established being filicide (the killing of one’s own child), neonaticide (a parent killing a newborn within the first 24 hours of life), filicide–suicide (a parent killing his or her child and committing suicide), familicide (the killing of one’s own child or children and partner, followed by the offender’s suicide), and other child homicide (siblings, stepparents, or a person outside the family killing a child). One central finding noted in the research on child homicides relates to the relationship between child homicides and homicide–suicides. International studies report that filicide cases constitute only 2% of all homicides but 8% of all homicide–suicides (National Confidential Inquiry [NCI], 2009). Male perpetrators of filicide in particular have been found to commit suicide to a substantial extent—40% to 60% according to Hatters Friedman, Hrouda, Holden, Noffsinger, and Resnick (2005), who suggest that this may be related to an overall higher suicide rate in males.
Another central finding is the relatively high proportion of female offenders. Around one third to 40% of all child homicide perpetrators have been found to be females in both Anglo-Saxon as well as Scandinavian and central European countries (Lehti et al., 2012; Somander & Rammer, 1991; Yarwood, 2004). This appears to be a much larger proportion than the 10% that females usually account for among homicide offenders in general in European countries (National Council for Crime Prevention, 2011). Mothers killing their offspring, usually prior to the age of 1 year, constitute a large proportion of the female perpetrators of child homicide (Fiala & LaFree, 1988; Lehti et al., 2012; Somander & Rammer, 1991).
Decreasing Child Homicide Rates in Many Western Countries 1960-2000
Yet another central, and positive, finding is that the child homicide rates in many Western countries have declined since the 1960s. Pritchard (2012) reports declines of 20% to 100% in a number of European countries between the 1970s and the 2000s. Also, several national studies have reported decreases, including studies from the United States (Bureau of Justice Statistics, 2010; Finkelhor & Jones, 2006), Hungary (Törö, Fehér, Farkas, & Dunay, 2010), Finland (Lehti et al., 2012), and Sweden (Granath, 2012). However, there is no consistency between these countries regarding either the ages of the victims to which the decreases relate or the exact period during recent decades during which the decrease has been most apparent (Gilbert et al., 2011).
Regarding the Scandinavian countries, child homicide rates decreased substantially between the 1960s and the 2000s in both Finland and Sweden. Lehti et al. (2012) reported that the main decrease in Finland appeared during the 1970s and related to all types of child homicide with the exception of maternal filicide–suicide. Furthermore, the authors found the decline to be correlated with general changes in gender attitudes and family structure (more liberal attitudes toward divorces and a greater acceptance of single mothers, for example), as well as with improvements to and an expansion of maternity and child care institutions. According to the authors, these changes have lessened both the motivations and the opportunities for child homicides. Similar explanations have been proposed for the decrease noted in Sweden between the 1960s and the 1990s (Rying, 2004; Somander & Rammer, 1991). Among other factors, Somander and Rammer (1991) highlight the significance of the decriminalization of abortion in Sweden in 1975, but state that this should be viewed as a tentative conclusion.
How and Why Have Child Homicides Declined in Sweden Since the 1990s?
In Sweden, however, a decrease in child homicides has also been apparent between the 1990s and the 2000s. During the mid-1990s in particular, the number of victims aged 0 to 14 years declined rather sharply according to cause-of-death-statistics (see Figure 1). As a result, the Swedish child homicide rate declined from about 0.4 per 100,000 inhabitants aged 0 to 14 years in the 1990s to about 0.27 per 100,000 in the 2000s. This decline is comparable with that of the mid-1970s noted by Somander and Rammer (1991). The child homicide rate in Sweden during the 2000s is probably at its lowest in modern times and has also been found to be lower than those of neighboring Western European countries such as the Netherlands and Finland (National Council for Crime Prevention, 2011).
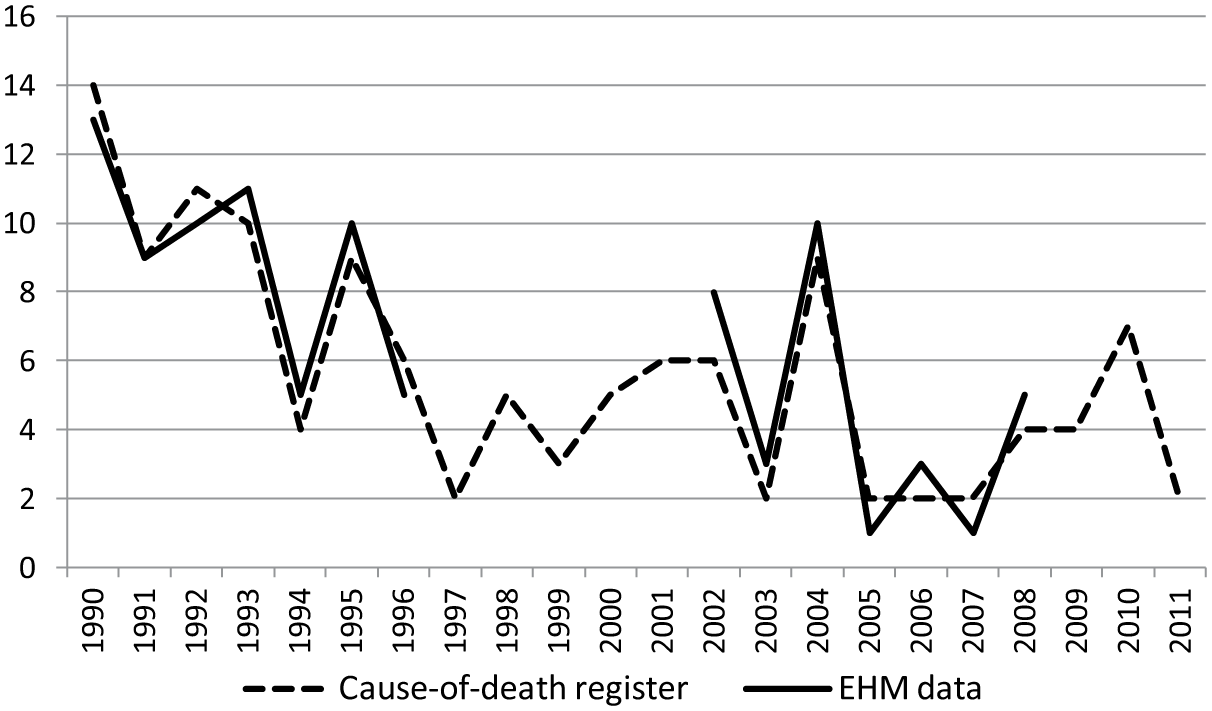
Number of child homicide (<15 years old) victims in Sweden 1990-2011 according to the national Cause-of-Death register and the EHM data, respectively (1990-1996 and 2002-2008).
While the decrease in child homicides in Sweden since the 1990s has been noted in national studies of homicide trends, the structural changes that might be involved have not yet been extensively examined in research. Therefore, efforts to explain the decrease have only been presumptive and have not been tested against data to any major extent. One hypothesis that has been outlined focuses on better treatment provision for mentally ill parents, with the expansion of prescriptions for antidepressant medication (Rying, 2004). Another hypothesis focuses on a heightened level of interventions from social services in relation to children at risk (Granath, 2012). Importantly, recent compilations of homicide data (e.g., the European Homicide Monitor [EHM] project; see National Council for Crime Prevention, 2011) provide new opportunities for in-depth analyses of child homicide in Sweden since the 1990s. Data have been compiled for research purposes by the National Council for Crime Prevention in Sweden, based on a broad set of variables for all homicides during the periods 1990-1996 and 2002-2008, respectively. These data include all registrations of child homicides, irrespective of whether the perpetrator committed suicide. Against this background, the aim of the current study is to further describe the changes in child homicide in Sweden during the 1990s and the 2000s. A focus will be directed at the types of child homicide cases—in terms of the gender of the perpetrators and victims, the perpetrator–victim relationship, suicide features, and so on—that appear to be related to the decline.
Data and Method
This study is designed as a consecutive study of all cases of homicide with a victim below 15 years of age in Sweden between 1990-1996 and 2002-2008. Thus, a child is defined in this study as an individual from birth to the age of 14. The additional inclusion of youths aged 15 to 17 years would have involved a risk of distorting the overall analysis by including youth brawls resulting in death and intimate partner killings among young couples. This age group was therefore excluded. Homicide is defined as an intentional criminal act of violence by one or more human beings resulting in the death of one or more other human beings. This definition roughly covers the definition used in the U.S. National Violent Death Reporting System (NVDRS), as employed by the U.S. Department of Health and Human Services (Centers for Disease Control and Prevention, 2003).
We use a data set comprising all cases of homicide in Sweden in 1990-1996 and 2002-2008 collated by the Swedish National Council for Crime Prevention. This data set is an extension of an international data set on homicide, known as the EHM, which includes similar data on all cases of criminal homicide (as defined above) in 2003 and 2006 in Finland, the Netherlands, and Sweden (National Council for Crime Prevention, 2011). We therefore refer to the data used in the article as the EHM data.
These EHM data are based on police reports, police investigations, and court judgments, and include information on both solved and unsolved cases. This means that information is not always available about the perpetrators associated with each case. However, a majority of the cases do include this information, since the clearance rate for homicide is high, particularly in homicides of children. Information about offenders who committed suicide or died for other reasons prior to conviction is also included in these data, and these cases are defined as having been solved. This constitutes an advantage by comparison with many other homicide studies, which often exclude filicide–suicides cases, since the researchers sample subjects from the forensic mental health or prison systems (Friedman et al., 2005).
Data for the entire period 1990-2010 are yet not available, however, since the collation of the database remains a work in progress. It was therefore only the two periods 1990-1996 and 2002-2008 that had been subject to quality control and were ready for external research use in 2012. However, these two periods cover both a number of years prior to the decline in the mid-1990s and a number of years subsequent to this decline (see Figure 1). The data therefore nonetheless provide opportunities to study structural changes related to the decline.
As can be seen from Figure 1, there is a substantial correspondence between the annual numbers of child homicides in Sweden according to the EHM data and the Swedish Cause-of-Death register, respectively. However, the numbers of homicides registered in the two sources are not identical. One explanation is that the national cause-of-death statistics include all persons registered as resident in Sweden, regardless of where the homicide took place, whereas the EHM data are based on cases that occurred within the country, regardless of the victim’s country of residence. This discrepancy is common in national homicide monitoring data in Western European countries, and usually means that the national cause-of-death statistics show somewhat lower numbers of homicides than data based on recorded crime, such as the EHM data (Liem et al., 2013). In addition, there may be a small number of homicides cases that are included in the EHM data based on police investigations, or even court judgments, where the body of the victim has not been found, which means that the case will not have been entered into the national cause-of-death statistics. Yet another explanation for the differences between the two sources displayed in Figure 1 is that some cases included in the cause-of-death statistics have later been redefined as accidents or as events other than homicide in the courts of appeal or the Supreme Court. This may explain why the cause-of-death statistics for individual years may show somewhat higher numbers of homicides than the EHM data. It is reasonable to assume that these small numerical discrepancies will not threaten the validity of the analyses conducted in this study. However, the cause-of-death data will be used to validate the trends found in the EHM data and examine the overall trend in rates of child homicides.
Assessments of the Cases
All assessments of the cases were based on the police files, the verdicts from the court (in solved cases) and records of a forensic psychiatric examination when such an examination had been carried out. On the basis of this information, a coding schedule was constructed, which included information on the victim, the offender, the type of violence, day of the week and time, where the offense took place, and so on (for a more thorough description, please see Appendix I in National Council for Crime Prevention, 2011). However, due to an ethical qualification made by the National Council for Crime Prevention, not all of the variables could be studied in the current analysis. For example, information regarding psychiatric diagnoses and contacts with the health care system are considered sensitive data in Sweden, and approval was therefore not granted to examine these variables.
Structural Data and Statistics
Data on the number of Swedish residents below the age of 15 were collected for each year from Statistics Sweden (http://www.scb.se/Statistik/LE/LE0101/2010A01B/EK/EK4_07.xls). An incidence rate ratio (IRR) was computed to analyze the trend in the number of child homicides per year using data from the Cause-of-Death register. IRR represents the change in the raw numbers of child homicides per 100,000 inhabitants, with the number of inhabitants aged below 15 being employed as the exposure variable, years as the linear predictor and the number of child homicide victims as the dependent variable, thus measuring change in incidence over time. An IRR of 0.9 means, in this case, a decrease of 10% in the incidence of child homicides, whereas an IRR of 1.1% means an increase of 10%. The Poisson regression was modeled in STATA and the other analyses were performed in SPSS.
Since it has been proposed as a factor that may be related to the trend in child homicides, data on the prescription of antidepressant medication in the general population were collected from the official statistics maintained by the National Board of Health and Welfare (2012). The cause-of-death data that are employed to validate the EHM data were collected from the Swedish national Cause-of-Death register. These data are compiled from forensic reports and are published by the National Board of Health and Welfare, that is, data on the numbers of deaths as a result of violence to a victim below the age of 15 were also collected from the Swedish National Cause-of-Death register. However, a major drawback associated with these data is that they do not include any information about the perpetrator.
Results
There were 62 cases of homicide against a child 0 to 14 years during the first EHM data periods examined (1990-1996; 9 per year) and 33 cases in the second period (2002-2008; 5 per year). These figures give a total of 95 homicide cases, with an overall rate of 0.42 child homicides per 100,000 children. The rate per 100,000 inhabitants below the age of 15 was .55 during 1990-1996 and .29 during 2002-2008. Only four of the cases during these years had not been solved, giving an overall clearance rate of 96%. The Poisson regression model analyzing 1990-2012 resulted in an overall annual decrease of 4% in child homicides during the time period (IRR = 0.96; 95% confidence interval [CI] = [0.93, 0.98]; p < .001).
Regarding context and the offender–victim relationship, 33% (n = 31) of the cases in the EHM data were intra-familial with suicide, 54% (n = 51) were intra-familial without suicide and 13% (n = 12) were extra-familial. This distribution corresponds relatively well to what Somander and Rammer (1991), who used the same classification, found in relation to child homicides in Sweden during the period 1971-1980. However, the proportion of cases in which the offenders were family members and committed suicide, the so called filicide–suicide cases, was higher (39% of all child homicides) in the Somander and Rammer material (1971-1980).
The Victims
There were 55 girls and 40 boys among the victims in the EHM data, with a mean age of 4.3 years. The largest decrease among the victims was found among victims older than 1 year but younger than 10 years (Table 1). Strangulation/suffocation was the most common method of killing followed by blunt force violence and sharp force violence. Less than one tenth of the victims had been killed using a gun. All types of violence had declined in absolute numbers with the exception of sharp force violence (Table 1).
Description of the 95 Child Homicides in Sweden 1990-1996 and 2002-2008.
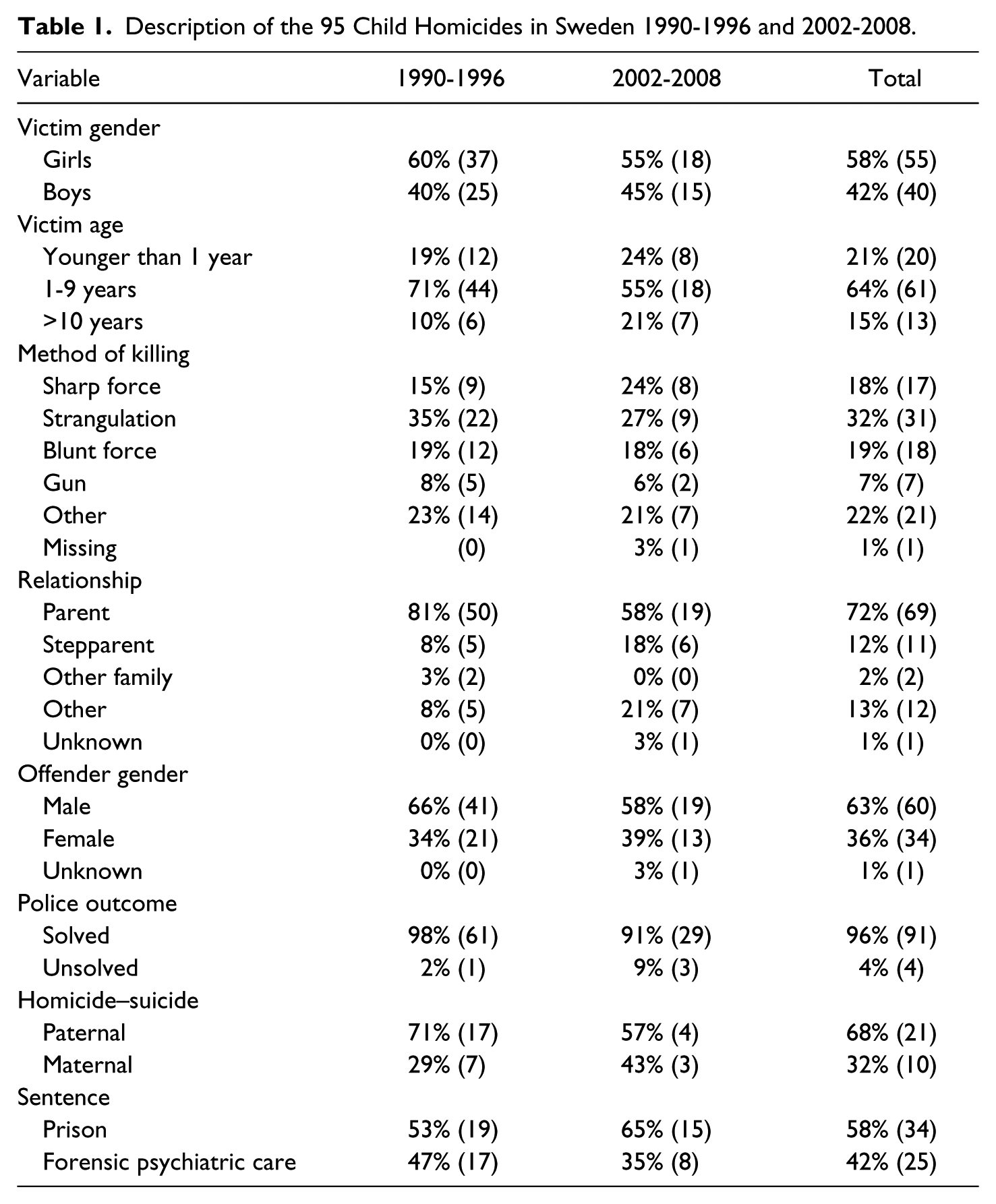
According to the EHM data, most of the children had been killed by a parent, although there was a decline in the number of such cases, from 50 victims (1990-1996) to 19 victims (2002-2008). Very few of the victims had been killed by an offender from outside the family (and only four of the offenders were strangers in the solved cases in the entire material for 1990-1996 and 2002-2008). However, no decline in the small numbers of child killings committed by persons outside the victim’s biological family was found from the 1990s to the 2000s.
The Offenders
Of the offenders in the EHM data, 60 were males and 34 females (in one case, the gender of the offender was unknown), with a mean age of 36 years (range = 15-63 years). The number of both female and male offenders decreased during the period examined, since there were 41 males and 21 females in the first of the two periods and 19 males and 13 females in the second. Altogether, the proportion of female offenders was roughly the same (34%-39%) in 1990-1996 and 2002-2008 as that found by Somander and Rammer (1991) for child homicides in Sweden during the period 1971-1980 (36%). In the first period, almost half of the offenders were sentenced to forensic psychiatric care and very few to life-imprisonment (n = 2; 5%). In the second period, however, both the number and proportion of offenders sentenced to life-imprisonment had increased (n = 5; 22%) and the proportion of offenders sentenced to forensic psychiatric care had declined.
Cases of Homicide–Suicide
Among the 62 offenders from the first period, 24 had taken their own life (39%). The corresponding figure for the second period was 7 of 33 offenders (21%). Altogether, 31 offenders (33%) had committed an act of filicide–suicide, of whom 21 were males (68%) and 10 females (32%) and this is in line with previous studies (NCI, 2009; Somander & Rammer, 1991). The results further show that between 1990-1996 and 2002-2008, there was a population-adjusted decrease of 72% in filicide–suicide offenders. There was a decrease among both mothers and fathers, although the decline was more pronounced among the fathers.
Discussion
A Decline in Child Homicides
The major finding of the study is that there has been an overall annual decrease of 4% in the number of child homicides in Sweden, and this decline is mainly due to a decline in the number of filicide–suicide cases. These cases do not account for all of the decrease but they are found to constitute the major cause. This study lends support to the increasing, and more conclusive, international empirical work that has noted a reduction in child homicides in most of the world’s industrialized nations (Bureau of Justice Statistics, 2010; Finkelhor & Jones, 2006; Lehti et al., 2012; Törö et al., 2010). The data from developing countries are more uncertain and more studies from different contexts are needed. Comparing the rate per 100,000 inhabitants, the number of child homicides seems to have declined in Sweden since the 1970s. Somander and Rammer (1991) report a rate 0.6 per 100,000 children in the 1970s. By comparison with the rate of child homicide of 0.29 in the second of the two periods examined in this study, this would imply a decrease of 50% in the rate of child killings in Sweden between the 1970s and the mid-2000s.
In contrast to the findings of a Finnish study on child homicides (Lehti et al., 2012), the current study found a decline in maternal filicide–suicides as well as in paternal filicide–suicides. One possible explanation for this difference is that the study by Lehti et al. analyzes changes between the 1960s and the 2000s, whereas the current study analyzes changes between the 1990s and the 2000s (thereby also involving smaller numbers than the Finnish study). The restriction of the current study’s focus to the most recent 20 years may have led to certain changes in the child homicide structure between the 1990s and the 2000s becoming more apparent. It is also possible that in Sweden, as well as in Finland, there might be different factors that explain the decrease in child homicides in the 1970s and the 1990s, respectively. However, the different time frames employed in the two studies do not rule out the possibility that there may also be actual differences in trends and explanations between the two countries.
Possible Factors Related to the Decrease
Since the decrease in child homicides in Sweden between the 1990s and the 2000s mainly concerns filicide–suicides (both maternal and paternal) involving victims aged 1 to 9 years, the proposed impact of an improved and expanded treatment of mentally ill parents seems relevant. Anti-depressant treatment in particular may be viewed as a factor that is likely to affect the specific type of child homicide that has decreased. It can be noted that the level of prescription of antidepressant medication in the general population increased in Sweden during the periods 1990-1996 and 2002-2008 (see Figure 2). In a related area of research, Swedish studies on suicide suggest an overall relationship between the prescription of antidepressant medication and a decline in suicides (Isacsson, 2000). This might imply that there is in fact a causal relationship between the increase in the prescription of antidepressant medication and the decline in child homicide in general, and the rate of filicide–suicide in particular. However, it is not possible on the basis of the data and methods employed in the current study to draw any further conclusions about the existence of a causal relationship between the increase in antidepressant medication and the decrease in child homicide.

Rate of child homicides (per 100,000) and number of daily doses of antidepressant medication per 100 inhabitants in Sweden 1990-1996 and 2002-2008.
As was noted earlier, another factor that may be of relevance to the decrease is an increase in the level of interventions from social and mental health services. Since the 1990s, Swedish legislation has been reformed in an effort to ensure that institutions that come into contact with children at risk of exposure to destructive acts will become more likely to intervene and report their concerns to social service agencies (Granath, 2012). It could be argued that this contextual factor, as with the increase in antidepressant medicine prescription, might be expected to affect filicide–suicides (both maternal and paternal) in particular—which, once again, constitute the type of the child homicide that has decreased the most since the 1990s. An increase in the level of interventions by social services, and the increase noted in the use of antidepressant medical treatment, may in fact be inter-related factors in relation to the decline noted in the child homicide rate.
Other, more cultural and family-gender oriented factors (greater acceptance of divorces and single mothers, the decriminalization of abortion, the medicalization of childbirth) that have been found to affect levels of child homicide in earlier studies covering the 1960s and 1970s (cf. Lehti et al., 2012; Somander & Rammer, 1991), may not be as relevant in relation to the decline found in the current study. The fact that the decline since the 1990s concerns both paternal and maternal filicide, and primarily victims aged 1 year or older, suggests that gender-oriented and family-structural changes, together with the further medicalization of childbirth, are unlikely to be important explanatory factors. Thus, it could be argued that the decline in child homicides in Sweden between the 1990s and 2000s may not be due to the same explanatory factors as the decline in child homicides in Sweden, and other countries, noted during the 1960s, 1970s, and 1980s.
The Proportion of Filicide–Suicides Remains Relatively High
Although decreasing, the rate of filicide–suicides in this sample is relatively high compared with other similar studies from comparable jurisdictions. For example, Nielssen, Large, Westmore, and Lackersteen (2009) found in their Australian study that 7 of 157 (4%) child homicide offenders committed filicide–suicide. This is a considerably lower figure than the 33% reported in this study. Regarding the structure of child homicide, there do not seem to have been any major changes since the 1970s. By comparison with Somander and Rammer’s (1991) results, we found quite similar proportions of cases of intra-familial (45% vs. 54%), intra-familial with suicide (39% vs. 33%), and extra-familial (16% vs. 13%) homicide. This finding supports the view that there has been no major change in the structure of child homicide in Sweden over the past 40 to 50 years.
Methodological Considerations
Unfortunately, there is no data set or register that holds information on the prescription of antidepressant medication among the parents of children aged 0 to 14 years. Such figures would provide an even better overall picture regarding the relationship between antidepressant medication and child homicides, and this is an issue that should be targeted by future research. The number of cases (n = 95) in the current study is somewhat small compared with many other studies. However, the figure is population-based and includes all cases within the jurisdiction of Sweden. In addition, the data are not merely register-based but also include additional information about the filicide–suicide cases, which has been argued to constitute a major methodological advantage (Friedman et al., 2005). Another strength of the current study is that the number of cases corresponds well to the population-based official Cause-of-Death register, even when the data are broken down into different sub-categories of child homicide. All in all, we would conclude that the overall picture presented by the study with regard to child homicide in Sweden is both valid and clinically fair.
Conclusion
There has been a decrease in child homicide in Sweden over the past 20 years, with the main decline being due to a reduction in cases of filicide–suicide among both mothers and fathers. The structural changes in child homicide in Sweden found in the 1990s and the 2000s lends support to earlier hypotheses that the decline is related to contextual factors such as the improved treatment of mentally ill parents (by means of an increase in the prescription of antidepressant medication, for example) and increased levels of interventions from social and mental health services. This underscores the view that although most violence toward children is driven by social factors (Fiala & LaFree, 1988; Hjern & Bremberg, 2002) and although cultural and social changes have had a major impact on child homicide rates since the 1960s, when examining lethal violence in modern North European societies such as Sweden, contextual, medical and psychiatric factors must also be taken into consideration. However, these factors do most certainly not explain the entire decline in child homicides in Sweden since the 1990s, and more research is needed on the causal relationship between various factors and variations over time in the rate of child homicides.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.