
Abstract
Extant health literacy research is unclear about the contribution of health literacy to health behaviors and is limited regarding women’s health issues. The primary purpose of this study is to investigate the association between health literacy and five health behaviors (Pap smear screening, annual physical checkup, smoking, checking food expiration dates, and monitoring physical changes) in women and to test whether the association is mediated by health knowledge. A national sample of 1,754 female adults in Taiwan was included in the study. Result showed that health literacy was positively and independently related to checking food expiration dates and monitoring physical changes, and that health literacy was not related to physical checkup and Pap smear screening. Interestingly, women with high health literacy were more likely to be a current smoker. Study findings suggest that efforts to improve health promotion behaviors in women should consider health literacy as an important factor and that the effect of health literacy on health prevention behaviors may vary by women’s access to care.
Keywords
Strong and consistent evidence shows that educational attainment affects an individual’s health-related behaviors (Arnold, Davis, & Berkel, 2001; Dewalt, Berkman, Sheridan, Lohr, & Pignone, 2004; Fong et al., 2007; LeVine, LeVine, Rowe, & Schnell-Anzola, 2004). Evidence accumulated over the past two decades suggests that health literacy, defined as an individual’s ability to obtain, process, and understand basic health information and services needed to make appropriate health decisions (Seldon, Zorn, Ratzan, & Parker, 2000), may be a stronger factor than educational attainment in explaining and predicting individual health behaviors and use of health services (Clement, Ibrahim, Crichton, Wolf, & Rowlands, 2009; Commission on Social Determinants of Health, 2008; Wolf, Parker, Ratzan, & Kris, 2008). It is also suggested that low health literacy may be indicative of disadvantaged social status that increases an individual’s exposure to unhealthy living conditions and social influences, thereby limiting the individual’s acquisition of appropriate health behaviors and practices (Lee, Arozullah, & Cho, 2004).
When examining health related behavior, health literacy researchers have mostly adopted a clinical orientation to focus on disease management behaviors among specific patient populations, for example, patients who have HIV/AIDS, diabetics, or hypertension (Gazmararian et al., 2006; Kalichman & Rompa, 2000; Morris, MacLean, & Littenberg, 2006; Osborn, Paasche-Orlow, Bailey, & Wolf, 2011). Moreover, evidence regarding the association between health literacy and health behaviors has been inconclusive. White, Jing, and Atchison (2008) linked health literacy to several health behaviors, including dental and vision check, cancer screening, flu shot, and osteoporosis screening. They found that the relationships varied by age groups. Several other studies reported that adequate health literacy enhanced the likelihood of good eating habits, regular exercise and cancer screening, and reduced the risk of smoking (Cho, Lee, Arozullah, & Crittenden, 2008; Scott, Gazmararian, Williams, & Baker, 2002; von Wagner, Knight, Steptoe,& Wardle, 2007). However, Wolf, Gazmararian, and Baker (2007) found adequate health literacy to be associated with an increased likelihood of smoking and alcohol consumption. The associations became nonsignificant once sociodemographic factors were included in the analysis.
In addition to the disease-specific orientation and inconsistent findings regarding the contribution of health literacy to health behaviors, health literacy research has paid limited attention to women’s health. Women are the “primary care doctor” and “family health officer” in most households and their heath behaviors influence significantly the health of their family members and loved ones (Hibbard & Pope, 1987; Keitel, 2000). In the United States, for example, women make around 80% of health care decisions for their families and they are the primary caregivers when a family member is ill (U.S. Department of Labor, 2010). The smoking behavior of mothers has been identified as a strong factor in the process of childhood socialization into smoking (Graham, 1987). Moreover, wives, more than husbands, are likely to influence the health of others in a marital relationship (August & Sorkin, 2010; Umberson, 1992).
Extant health literacy research on women has primarily focused on cancer screening and has found in general that health literacy is a significant factor. Davis et al. (1996) showed that low-literacy women, compared with their high-literacy counterparts, were less likely to receive mammography. Two United States studies found that inadequate health literacy was associated with a reduced likelihood of cervical cancer screening and follow-up examinations (Garbers & Chiasson, 2004; Lindau et al., 2002). Using data from the 2003 National Assessment of Adult Literacy in the United States, White et al. (2008) also found a significant link between health literacy and Pap smear and mammogram screenings among women of various age. Beyond cancer screening, there is a dearth of empirical evidence linking health literacy to women’s health behaviors.
To fill this gap, we used data on a nationally representative sample of women in Taiwan to investigate two research questions: (a) What is the association between health literacy and health promotion and prevention behaviors in women? (b) To what extent is the association between health literacy and health promotion and prevention behaviors mediated by health knowledge? In a recent article, Kondilis, Kiriaze, Athanasoulia, and Falagas (2008) observed an imbalance in the health literacy literature: Less than one third of the health literacy–related studies published between 1991 and 2005 were conducted in European countries and almost all the rest were in the United States. To our knowledge, health literacy research outside North American and European countries is even more limited. Efforts to understand the extent of health literacy problems and their consequences in other parts of the world have just begun, because of limited availability of health literacy assessment tools. Our research, therefore, would contribute to diversifying the knowledge basis of health literacy research.
Health Literacy, Health Knowledge, and Health Behaviors
Based on evidence of health literacy research and drawing on social cognition models of health, von Wagner, Steptoe, Wolf, and Wardle (2009) developed a comprehensive framework to explicate the relationships between health literacy and health actions. The framework identified several pathways and processes through which health literacy may affect health. Of particular relevance to our study, the framework considered health knowledge as a motivational factor that mediated the effect of health literacy on health behaviors, such as quitting smoking, healthy eating, and attending for screening.
Take cancer prevention as an example. Individuals with difficulty in comprehending printed health information—a basic health literacy skill—are unlikely to benefit from health education campaigns and acquire new cancer knowledge. Their beliefs about cancer prevention would be shaped predominantly by personal experience rather than state-of-the-art health advice. Thus, health literacy is expected to be positively associated with cancer prevention behavior and the association is mediated through health knowledge. In support of this expectation, several studies demonstrated that individuals with limited health literacy were disadvantaged by poor knowledge of cancer prevention services (Davis et al., 1996; Lindau et al., 2002) and that lack of knowledge about cancer prevention services was associated with negative beliefs about those services (Dolan et al., 2004). More direct evidence about the mediating effect of health knowledge was found in a study that employed path analysis to examine intermediate factor that linked health literacy to health status and health service utilization in a sample of Medicare enrollees in inner-city neighborhoods (Cho et al., 2008). The study found that health literacy had a positive effect only on disease knowledge, which in turn had a positive effect on health behavior.
A mediation model of health literacy, health knowledge and health promotion and prevention behaviors examined in the current study is depicted in Figure 1. According to Baron and Kenney (1986), testing of a mediation effect requires first the establishment of a relationship between the independent variable and the dependent variable and then decomposition of the relationship into a direct component (A) and an indirect, or mediated, component (B and C). Thus, four hypotheses were examined in the study:
Hypothesis 1: Health literacy is significantly and positively associated with health behaviors.
Hypothesis 2: Health literacy is significantly and positively associated with health knowledge.
Hypothesis 3: Health knowledge is significantly and positively associated with health behaviors.
Hypothesis 4: The association between health literacy and health behaviors becomes weaker or no longer significant when health knowledge is controlled for.
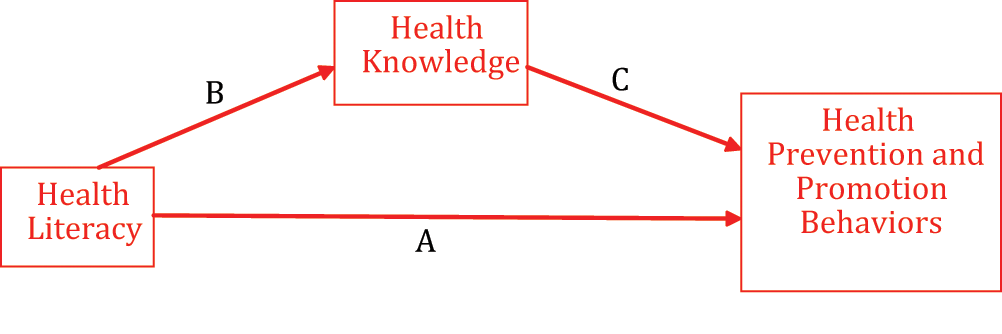
A mediation model of health literacy, health knowledge, and health behaviors
Method
Data for this study were obtained from a national survey conducted by the National Health Research Institutes (NHRI) in Taiwan in 2008-2009. The survey was to assess the level of health literacy in Taiwanese adults using the Mandarin Health Literacy Scale (MHLS; T.-I. Tsai, Lee, Tsai, & Kuo, 2011). The main results of the survey were reported in Lee, Tsai, Tsai, and Kuo (2010). The current study included only female adults.
The NHRI Survey of Health Literacy in Taiwan
The survey was conducted on Taiwanese adults, age 18 years and older, selected based on the Taiwanese household registration system and using a multistage stratified, probability-proportional-to-size sampling strategy (Liu et al., 2006). A total of 5,682 adults who met the initial inclusion criteria were sampled. The following procedures were employed in recruitment and data collection.
First, the 5,682 adults selected for the survey were contacted by mail or phone. The letter and the phone message explained the purpose of the survey and asked for their voluntary participation. Those who responded and agreed to participate were scheduled for an in-person interview to be conducted by a trained interviewer at the subject’s home or a location of his or her convenience. At the scheduled interview, the interviewer first explained the consent form—including the purpose of the survey, survey participants’ rights, risks and benefits of participation, and the plan to protect the confidentiality of survey participants—and obtained the signature of the subject if he/she agreed to the questionnaire interview. The interviewer then asked the subjects to read aloud a brief text to identify those who were illiterate or unable to read, because previous research suggested that illiterate subjects may feel embarrassed about not being able to read and may be uncomfortable taking a self-administered health literacy test (Parikh, Parker, Nurss, Baker, & Williams, 1996; Wolf et al., 2007). Those subjects (N = 365) who were unable to read were not asked to complete the self-administered health literacy test and received a score of zero. In all, Thirty-five subjects refused the MHLS test. The remaining adults took the test and were scored. All subjects, whether or not they took the test, answered all the remaining survey questions, administered by the interviewer, regarding their sociodemographic attributes, health behaviors, health knowledge, health status, and health care utilization. On average, the interview took approximately 40 minutes to complete.
Excluding nonresponders (subjects who refused or could not be reached after five attempts of phone or mail contact) and subjects who had uncorrectable vision and hearing problems, who were cognitively impaired, and who refused the MHLS test, the effective sample size was 3,526 adults and the response rate was 62.1%. Subjects participating in the survey were not statistically different from those who were excluded in terms of age, gender, and formal education. There were 1,754 female participants, who constituted the sample of this study.
Measurement
The MHLS is a reading test designed to assess health literacy in Mandarin Chinese that uses traditional Chinese characters—the standard writing in Taiwan (T.-I. Tsai et al., 2011). The scale contains 50 items, of which 33 test the comprehension of health-related texts and 17 assess numeracy skills. In a random sample of 323 Taiwanese adults, the scale was found to have a high correlation with years of formal education, suggesting high convergent validity. It was significantly associated with reading habit, health knowledge, and receipt of assistance in reading written health materials, indicating good predictive validity. Furthermore, it had high internal reliability (Cronbach’s α = .95) and split-half reliability (Spearman-Brown correction = .95). Based on the test score, range 0 to 50, respondents could be classified into three health literacy levels: inadequate (0-30), marginal (31-42), and adequate (43-50; Lee et al., 2010).
Three survey items were used to assess health promotion behaviors. Two of them asked respondents to reply on a 5-point Likert-type scale (1 = never, 2 = seldom, 3 = sometimes, 4 = often, and 5 = always) how frequently they paid attention to their physical changes (e.g., skin discoloration, weight change, abnormal growths) and checked the expiration dates on food labels when shopping for groceries. The third item inquired about the respondent’s smoking behavior. Based on the response, respondents were classified as “current smokers,” “former smokers,” and “nonsmokers.” Current smokers were those who smoked more than 100 cigarettes in their life and smoked in the past month. Former smokers were those who smoked less than 100 cigarettes in their life or those who smoked more than 100 cigarettes in their life and did not smoke in the past month. Nonsmokers were those who reported that they never smoked or had one or few puffs in their life. In the analysis, we merged “nonsmokers” and “former smokers” into the same group and created a dummy variable, smoking, that had a value 1 indicating “current smokers” and 0 indicating “noncurrent smokers.”
Health prevention behaviors were indicated by two survey items, which asked whether the respondent had an annual physical checkup and Pap smear screening in the past 2 years. The variables were coded 1 if the respondent answered “yes” and 0 if “no.” The National Health Insurance Program in Taiwan offers free annual physical checkup to people 40 years and older and Pap smear screening to women 30 years and older. Thus, we limited the analysis on physical checkup to women aged 40 years and older and the analysis on Pap smear screening to women aged 30 years and older.
The NHRI survey contained 10 questions that assessed the respondent’s health knowledge. The questions were designed based on printed health materials distributed by the Taiwanese government—Take Care of Yourself (Department of Health, 2006), Health 99 Education Resource (Bureau of Health Promotion, 2008)—and health information commonly seen in the mass media. A correct answer to each of the 10 questions was given 1 point. Exploratory factor analysis of the questions showed that six of them—regarding dengue fever transmission, health hazards of smoking, flu vaccination, hepatitis B transmission, prevalence of cardiovascular disease, and treatment of cold—were loaded on a common factor. Confirmatory factor analysis validated the result, showing that the one-factor model was a good fit for those six questions (χ2/df = 4.77, adjusted goodness-of-fit index = .98, normed fit index = .94, root mean square error of approximation = .03). On the basis of these results, we constructed a six-item index to measure health knowledge. The measure had satisfactory internal reliability (Cronbach’s α = .69). It was significantly correlated with education and health literacy, showing good criterion-related validity.
Several sociodemographic attributes were included as control variables. They were age, educational attainment (years of formal schooling), personal income, and residential location (metropolitan city, mid-size city, small city, rural/remote area).
Statistical Analysis
First, descriptive statistics (mean, SD, and percentage) were computed to describe the sociodemographic attributes of Taiwanese women included in the sample and to examine the levels of health literacy, health knowledge, and health behaviors of the sample. Second, correlation analysis were conducted to examine the bivariate associations between health literacy and health promotion and prevention behaviors, between health literacy and health knowledge, and between health knowledge and health promotion and prevention behaviors. Third, multivariate analysis using binomial logistic regression was conducted to examine whether health literacy was associated with health promotion and prevention behaviors, holding constant respondents’ age, educational attainment, personal income, and residential location.
The test of the mediation effect of health knowledge had to satisfy four conditions (Baron & Kenney, 1986): (a) a significant and positive association between health literacy and health promotion and prevention behaviors (Hypothesis 1), (b) a significant and positive association between health literacy and health knowledge (Hypothesis 2), (c) a significant and positive association between health knowledge and health promotion and prevention behaviors (Hypothesis 3), and (4) addition of health knowledge significantly reducing the association between health literacy and health promotion and prevention behaviors (Hypothesis 4). The bivariate and multivariate analyses described above provided the tests of the first three conditions. To examine the last condition, we entered health knowledge into the binomial logistic regression models to see if that would reduce the associations between health literacy and health promotion and prevention behaviors.
All statistical analysis was performed using the Statistical Analysis Software package, SAS version 9.1.
Results
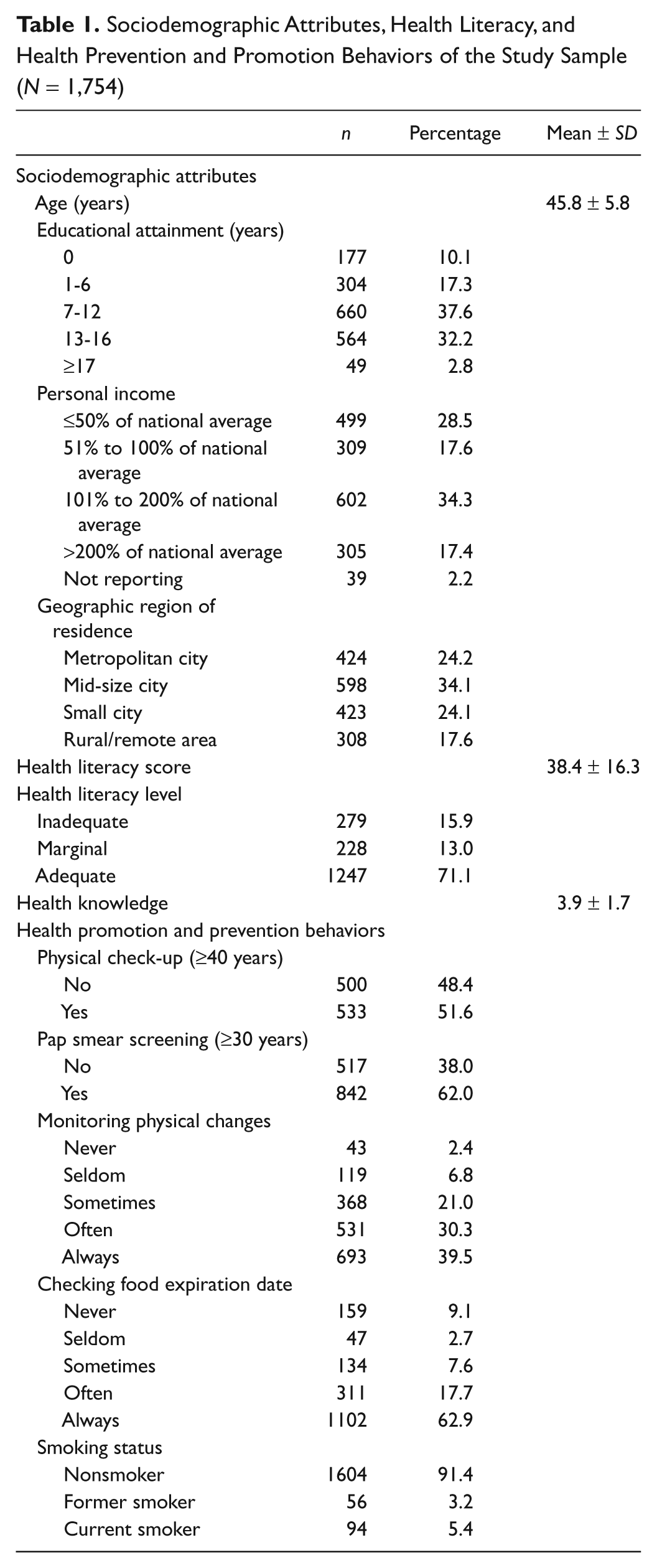
As shown in Table 1, the average age of the 1,754 women included in the study was 45.8 years. The largest group of the sample had 7 to 12 years of formal schooling (37.6%) and had income at 101% to 200% of the national average in 2007 (34.3%). The majority of women (58.3%) resided in metropolitan. The mean MHLS score was 38.4 (out of 50). Based on their MHLS score, 15.9% of women were considered to have inadequate health literacy, 13.0% marginal health literacy, and 71.1% adequate health literacy. The mean health knowledge score was 3.9 (out of 6). In terms of health prevention and promotion behaviors, 51.6% of women aged 40 years and older reported they had a physical checkup in the past 2 years; 62.0% of women aged 30 years and older reported they had a Pap smear test in the past 2 years; close to 70% of women reported they often or always paid attention to their physical changes; around 80% of women reported they often or always checked the expiration dates on food labels when grocery shopping; and 91.4% women were nonsmokers.
Sociodemographic Attributes, Health Literacy, and Health Prevention and Promotion Behaviors of the Study Sample (N = 1,754)
Results of the correlation analysis are presented in Table 2. In supporting Hypotheses 1 and 2, health literacy was significantly and positively associated with three health promotion and prevention behaviors—Pap smear screening (p < .001), monitoring physical changes (p < .05), and checking food expiration dates (p < .001)—and health knowledge (p < .001). Consistent with Hypothesis 3, health knowledge was also significantly and positively associated with Pap smear screening (p < .001), monitoring physical changes (p < .05), and checking food expiration dates (p < .001). Health literacy and health knowledge were not significantly associated with physical checkup and smoking status.
Correlations Among Health Literacy, Health Knowledge, and Health Promotion and Prevention Behaviors
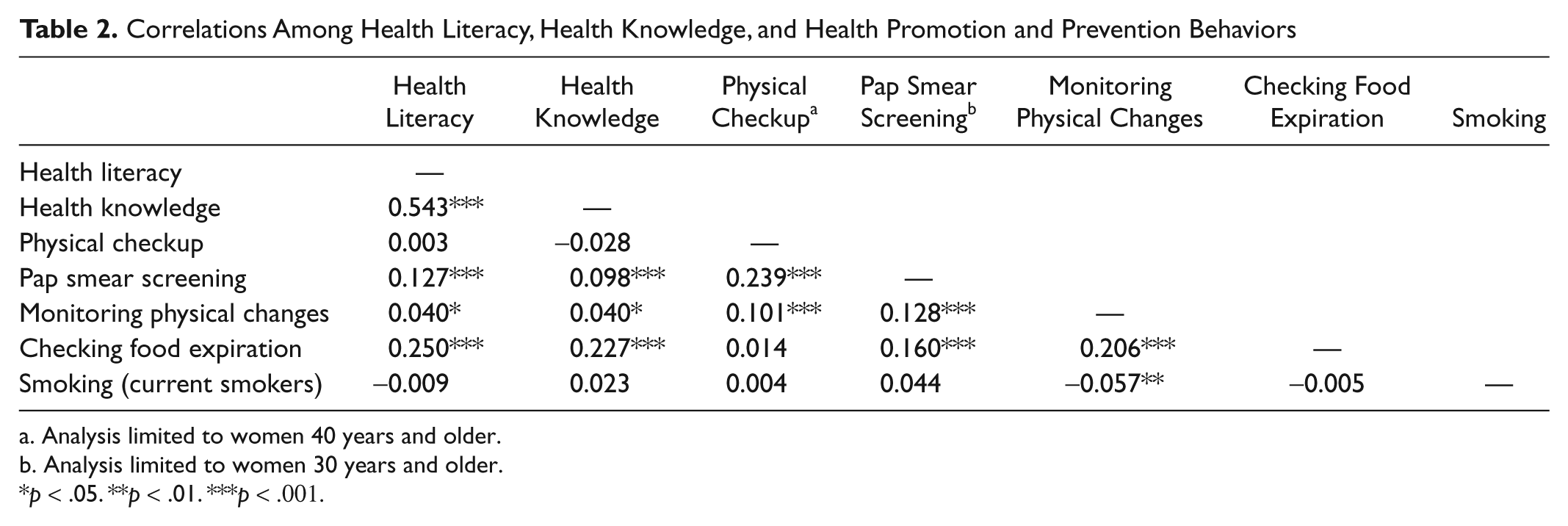
Analysis limited to women 40 years and older.
Analysis limited to women 30 years and older.
p < .05. **p < .01. ***p < .001.
Finally, binomial logistic regression was performed to see if health literacy was significantly associated with health promotion and prevention behaviors and if the addition of health knowledge would reduce the associations of health literacy with health promotion and prevention behaviors, holding constant age, education, income, and residence location. According to the results presented in Table 3, health literacy was significantly and positively associated with monitoring physical changes (odds ratio [OR] = 1.02; 95% confidence interval [CI] = 1.01-1.03), checking food expiration dates (OR = 1.03; 95% CI = 1.02-1.05), and smoking (OR = 1.03; 95% CI = 1.01-1.05). Addition of health knowledge did not change those significant associations, suggesting that health literacy had direct associations with those three health promotion and prevention behaviors among Taiwanese women. Health knowledge had significant and positive associations with monitoring physical changes (OR = 1.08; 95%CI = 1.00-1.17), but not with checking food expiration dates and smoking status.
Multivariate Logistic Regression Results

Note. OR = odds ratio; CI = confidence interval. Entries in bold font show data with statistical significance.
Discussion
This study is one of the few that are focused on health literacy in women. We found in a nationally representative sample of Taiwanese adults approximately 29% of women had inadequate and marginal health literacy. The rate was lower compared with results in previous studies (Garbers & Chiasson, 2004; Lindau et al., 2002). The difference may be because of three reasons. First, previous estimates were obtained from either a patient or an immigrant sample, which may be overrepresentative of women in disadvantaged social groups. Second, the literacy rate in Taiwan is 93.3%; the average length of education was 10.6 years among women aged 25 years and older; and 22.5% of the nation’s adults have a university degree (National Statistics, 2010). Thus, the majority of women may not have difficulty comprehending and using written health information. Third, the comparison may be imprecise because no similar tests have been developed to allow for international comparison.
The primary purpose of the study was to examine the association between health literacy and health promotion and prevention behaviors in women and to test if the association was mediated by health knowledge. We found health literacy to be significantly and positively associated with two health promotion behaviors—monitoring physical changes and checking food expiration dates. These findings were consistent with previous studies that linked health literacy to nutrition intake, physical activity, and dental checkup (von Wagner et al., 2007; White et al., 2008; Wolf et al., 2007). A common explanation of these positive relationships is that individuals with a higher level of health literacy are more knowledgeable of health matters and health risk factors and, therefore, are more likely to take health promotion measures (Gazmararian, Williams, Peel, & Baker, 2003; Lindau et al., 2002; Rothman et al., 2009). Surprisingly, we did not find health knowledge to be a mediator between health literacy and monitoring physical changes and checking food expiration dates, despite that health knowledge had significant and positive associations with those two health promotion behaviors. Does health literacy have a direct impact on health promotion behaviors? Are there important mediators—for example, health efficacy, social support—that are yet to be identified? Examination of these questions is important because it would suggest effective interventions to encourage health promotion behaviors in low health literacy women.
Also surprising was our finding that Taiwanese women with higher health literacy were more likely to be a current smoker. This was inconsistent with prior studies that showed either a negative or nonsignificant relationship between health literacy and smoking (Hibbard & Pope, 1987; von Wagner et al., 2007; Wolf et al., 2007). It is possible that smoking is generally and traditionally considered a taboo for women in Taiwanese society and that only those women who are young, who have high education, who live in urbanized areas, and who are employed and self-dependent—attributes that are related to high health literacy—are likely to acquire the habit (Y.-W. Tsai, Tsai, Yang, & Kuo, 2008). This explanation is partially supported by our analysis, which showed a significant and negative relationship between age and smoking and a significantly lower likelihood of smoking among women living in small cities and rural/remote areas. Our result of a significant and negative relationship between education and smoking, however, counteracts the explanation, suggesting that further research is needed to investigate women’s smoking behavior.
Contrary to previous studies (Garbers & Chiasson, 2004; Lindau et al., 2002), we did not find health literacy to be significantly associated with a physical checkup or Pap smear screening. A number of studies have pointed out that barriers to cervical cancer screening may include lack of knowledge, lack of access, and cultural and logistical factors (Arrossi, Ramos, Paolino, & Sankaranarayanan, 2008; Bazargan, Bazargan, Farooq, & Baker, 2004; Brown, 1996; Wong, Wong, Low, Khoo, & Shulb, 2008). These factors, as well as the interactions among them, may have differential effects on Western and Asian women. Alternatively, the National Health Insurance Program in Taiwan, which provides needed health care to approximately 98% of the nation’s population, may have effectively removed individual barriers to physical checkup and Pap smear services among women.
By examining health promotion and prevention behaviors in a population-based women sample, our study represented a significant departure from existing health literacy research that is mostly conducted in a specific patient group (e.g., HIV/AID, diabetes) or focused on disease-specific health behaviors. On the whole, our findings were consistent with previous research in supporting a strong association between health literacy and health knowledge. There was also evidence in our analysis that links health literacy to health promotion behaviors. However, the result that health knowledge did not mediate the relationship between health literacy and health promotion and prevention behaviors was unexpected. It stood in sharp contrast to the conceptualization of health literacy as a skill-based competency that transforms health information into knowledge and behaviors that contribute positively to health (Nutbeam, 2000; Zarcadoolas, Pleasant, & Greer, 2005). Is it possible that health knowledge, although long believed to be a critical factor in improving health outcomes and an integral part of health education campaigns, is not necessarily a prerequisite for change in health behaviors? If changing behaviors requires influencing individuals’ “minds” (knowledge) and “hearts” (emotion; Heath & Heath, 2010), could health literacy be also related to “the heart”—for example, confidence, self-worth, resolve, zeal—without which sustainable behavioral change is unlikely? To the extent these are plausible, our findings suggest that promotion of women’s health behaviors should go beyond the provision of health information and that health education should focus not just on knowledge but also on improvement in motivation, self-efficacy, and advocacy skills.
There were several limitations in our study. First, our ability to establish the causality between health literacy and health promotion and prevention behaviors was severely limited by the use of cross-sectional data in our analysis. Second, even though some research suggested a high degree of correspondence between patient self reports and medical records (Bush, Miller, Golden, & Hale, 1989), use of self-reported data on health promotion and prevention behaviors may raise concerns about validity and reliability. Third, our multivariate analysis included education as a covariate. To the extent that health literacy and education are highly correlated (r = .80 in our sample) and that they have similar health effects, our results may represent conservative estimates of the associations between health literacy and health promotion and prevention behaviors.
Conclusion
Women are the key consumers and disseminators of health information. Their health behaviors have an immediate impact on the health conditions of their family. Therefore, understanding women’s health literacy level and how health literacy influences women’s health behaviors are of utmost importance.
In this study, we found a sizeable proportion of women in Taiwan who had limited health literacy to fully function in the health care system. We also found health literacy to have direct associations with several health promotion behaviors among Taiwanese women. At the local level, our findings suggest health professionals in Taiwan should pay attention to women’s health literacy level so as to strengthen public health efforts that encourage women’s health behaviors. Globally, our study contributes to diversifying the knowledge base of health literacy and enhancing the focus of the research on women’s health issues. Our result that health literacy has a differential impact on health promotion and prevention behaviors also points to the importance of considering system-level factors as well as sociopolitical contexts in conducting health literacy research, which also promotes international comparison.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article.
This study was supported by the National Health Research Institutes in Taiwan (Grant Number: HP-097-PP-04 & HP-098-PP-23).