
Abstract
Patient activation has been considered as a “blockbuster drug of the century.” Patients with mental disorders are less activated compared to patients with other chronic diseases. Low activation due to mental disorders can affect the efficiency of treatment of other comorbidities. Contextual factors are significantly associated with mental health care access and utilization. However, evidence of their association with patient activation is still lacking. Using data from the Health Tracking Household Survey 2007 and Area Health Resource File 2008, we examine the association between contextual factors and self-reported activation levels among patients with depression. We investigate two types of contextual factors—(a) site of usual source of care and (b) community characteristics, measured by mental health care resources availability, population demographics, and socioeconomic characteristics at the county level. Results show significant variation in activation levels by contextual factors. The availability of community mental health centers, lower proportion of foreign-born individuals, and higher income in the local community are associated with higher patient activation. Our results also show that depressed patients having a usual source of care at a physician’s office have significantly higher patient activation levels than those with a usual source of care in the emergency department or hospital outpatient clinics. Results suggest that primary care setting is critical to having a sustained relationship between patients and physicians in order to enhance patient engagement in mental health care. Interventions in communities with low income and high immigrant populations are necessary.
Approximately 1 in 10 adults have depression in the United States (Gonzalez et al., 2010). The cost of depression (the sum of health care costs and lost productivity) exceeds $105 billion annually (in 2010 dollars; Greenberg et al., 2003). Depression is a chronic disease that can be treated effectively through regular treatment, such as psychotherapy and pharmacotherapy (Norcross & Goldfried, 2005; U.S. Department of Health and Human Services, 1999). Compared to patients with other chronic diseases, patients with depression are less likely to be engaged in their treatment or adhere to their treatment plans (Cabassa, Hansen, Palinkas, & Ell, 2008; Hibbard & Cunningham, 2008; Rodriguez, Chen, & Rodriguez, 2010). Since depression is a common comorbidity of other diseases, such as heart disease, diabetes, and obesity (Katon, 2008; Katon et al., 2008; Rugulies, 2002; Zhao et al., 2011), lower activation as a result of depression may adversely affect the treatment of other diseases (Katon, 2008; Katon et al., 2008; Rugulies, 2002). Hence, improving patient activation, such as engaging patients and encouraging self-management in mental health care, is critical.
Patient activation is defined as a person’s ability and confidence to manage his or her health and health care (Hibbard et al., 2008; Hibbard, Mahoney, Stock, & Tusler, 2007). Higher levels of patient activation predict better treatment compliance and health outcomes (Alegría et al., 2008; Aujoulat, d’Hoore, & Deccache, 2007; Aujoulat, Marcolongo, Bonadiman, & Deccache, 2008; Cortes, Mulvaney-Day, Fortuna, Reinfeld, & Alegría, 2009; Cunningham, Hibbard, & Gibbons, 2011; Fitzsimons & Fuller, 2002; Johnson, 2011). Patient activation has been considered as a “blockbuster drug of the century” (Kish, 2012). Improving patient activation and engaging patients in their health care and decision making is the top priority of the Patient Centered Outcomes Research Institute, launched in 2010 through the Affordable Care Act (Barry, Weiner, Lemke, & Busch, 2012; Garfield, Zuvekas, Lave, & Donohue, 2011; Mullins, Abdulhalim, & Lavallee, 2012).
Research has been conducted extensively to improve patient activation (Handy, Boarnet, Ewing, & Killingsworth, 2002; Hibbard et al., 2007; Hibbard et al., 2008; Hibbard, Mahoney, Stockard, Mahoney, & Tusler, 2005; Ory, Kinney Hoffman, Hawkins, Sanner, & Mockenhaupt, 2003). Recent research also suggests the potential influence of contextual factors on individuals’ mental health care utilization (Cook, Doksum, Chen, Carle, & Alegría, 2013; Hibbard et al., 2008). The evidence of the association between contextual factors and patient activation, however, is still lacking. To bridge this gap, this study is designed to (a) conceptualize the impact of contextual factors on patient activation and (b) empirically examine the association of contextual factors and patient activation among patients with depression. Our evidence will advance the current literature on the understanding of the contextual components of patient activation.
Conceptual Framework
Our conceptual framework is adapted from the patient activation literature (see Figure 1; Hibbard et al., 2008; Jerant, Sohler, Fiscella, Franks, & Franks, 2011) and the Andersen behavioral model (Andersen, 1968, 1995; Davidson, Andersen, Wyn, & Brown, 2004).
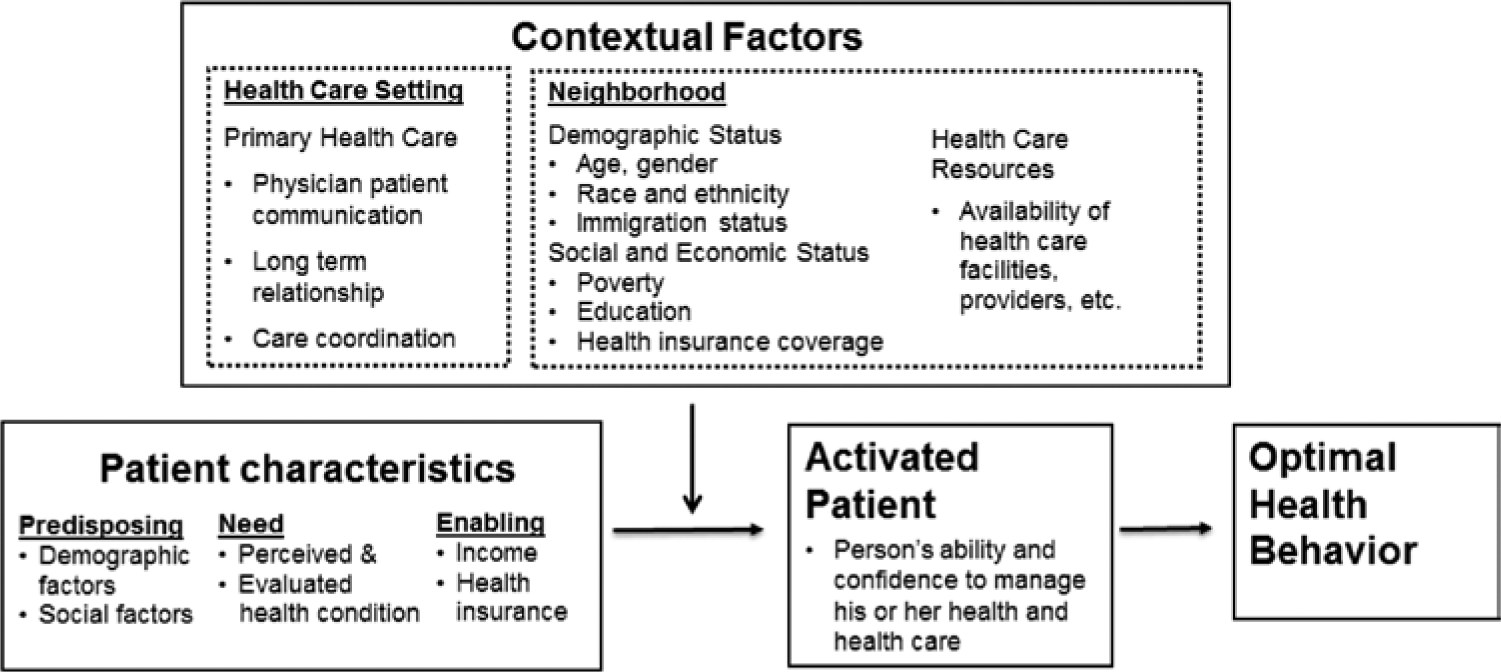
Conceptual framework.
Patient Characteristics
The literature shows that patient activation varies by patients’ demographic and socioeconomic characteristics (Cunningham et al., 2011; Hibbard et al., 2008). Racial and ethnic minorities, immigrants, people with lower income, less educational attainment, and worse self-reported health are less active compared to their counterparts (Hibbard et al., 2007; Hibbard et al., 2008). Health insurance coverage is also related to patient activation. Hibbard et al. (2008) showed that patients with Medicaid were less likely to be activated compared to patients covered by private health insurance. These factors related to patient activation are categorized by predisposing (demographic factors), need (health status), and enabling factors (income, education, health insurance, and other socioeconomic factors) according to the Andersen behavioral model (1968, 1995).
Contextual Factors
Davidson, Andersen, Wyn, and Brown (2004) improved the Andersen behavioral model by adding contextual factors. Jerant et al. (2011) also modeled contextual factors as critical attributes to patient activation. Contextual factors are defined as the environment in which patients receive health care (Cook et al., 2013). Specifically, we focus on two types of contextual factors (Hibbard et al., 2008): site of usual source of care and community characteristics. Site of usual source of care, such as a physician’s office or hospital emergency department (ED), reflects the relationship between physicians and patients, the major impact on patient activation (Alexander et al., 2012).
A continuous relationship with a physician is critical to sustaining a patient’s activation and involvement in their care (Haggerty et al., 2003). The primary health care setting, where health care is regularly delivered and illness is usually diagnosed, may relate to higher patient activation, compared to EDs and other sites of care, for a variety of reasons. Primary health care provides a better environment to improve patient–physician communication, cultivate patients’ trust, and sustain patients’ activation in their health care (Alexander et al., 2012). In addition, primary health care also plays a critical role in continuity of care, as well as care coordination, such as referring the patients to specialist visits or other appropriate health care services. The integrated mental health care model, advocating coordinated primary care and specialty care for mental health treatment, has been considered a core clinical feature to improve mental health care (Agency for Healthcare Research and Quality, 2013; SAMHSA-HRSA Center for Integrated Health Solutions [SAMHSA-HRSA], 2013). Our study provides national-level evidence of patient activation in the primary care setting.
The second contextual factor is the characteristics of the community. Hibbard (2009) noted the importance of improving patient activation at the community level. Community characteristics have been shown to be a critical component of people’s health (White, Haas, & Williams, 2009; Williams et al., 2012). Community health care resources and population characteristics are significantly associated with health care access and utilization (Benjamins, Kirby, & Bond Huie, 2004; Davidson et al., 2004; Dinwiddie, Gaskin, Chan, Norrington, & McCleary, 2013; Gaskin, Dinwiddie, Chan, & McCleary, 2012a, 2012b; Ludwig et al., 2012; Ory et al., 2003), including mental health care (Cook et al., 2013; Lee, 2009) and health care disparities (Gaskin et al., 2012a, 2012b; Kim et al., 2013).
Method
Data
The data for this analysis are from the Center for Studying Health System Change 2007 Health Tracking Household Survey (Hibbard et al., 2008; Strouse, Carlson, Hall, & Cybulski, 2009). The Health Tracking Household Survey is the first large, nationally representative survey to include patient activation measures to assess the level of activation in the civilian, noninstitutionalized U.S. population. The survey includes a 13-item patient activation measure in the consumer engagement section, composed of self-reported responses to questions regarding patients’ self-management of their own health. In addition to the activation questions, the survey also provides detailed data on demographics and socioeconomic status of the respondents, as well as their health care access, insurance coverage, and perception of their patient–physician relationship.
To estimate the association between community characteristics and patient activation, we link the Health Tracking Household Survey data with county-level data from the Area Health Resource File. The Area Health Resource File is a county-based data file and has more than 6,000 data elements for all counties in the United States, including number of physicians, community centers, and population demographic components within a particular county.
Measures of Patient Activation
We construct a patient activation index using the 13 patient activation measures as an overall indicator of patient activation for each respondent. These 13 questions (i.e., Patient Activation Measure-13) have been widely adopted in the literature (Cunningham et al., 2011; Hibbard et al., 2007; Hibbard et al., 2008). Specifically, the 13 items include respondents’ self-evaluations to the following statements: being active in their own health care, being responsible for managing their health condition, knowing prescription doses, doing follow-up treatments at home, understanding the cause of their health condition, knowing different treatment options, knowing how to prevent further problems, the ability to tell concerns to health provider, tell when need to get health care, act to prevent symptoms, maintain lifestyle changes, find solutions for new problems, and maintain lifestyle changes under stress. The answers to each of these questions are measured by Likert-type scales ranging from 1 (strongly agree) to 4 (strongly disagree). The activation index equals to the average score of the responses to these 13 questions (Cunningham et al., 2011; Greenberg et al., 2003). The index is then linearly transformed to a continuous scale, ranging from 1 to 100, with higher scores indicating higher activation levels.
Contextual Factor: Site of Usual Source of Care
Variables measuring access and the site of usual source of care are constructed from responses to the usual source of care questions. Respondents are asked whether there is a place that they usually go when they get sick or need health-related advice. Those who respond negatively to this question are considered to have no usual source of care. Respondents who answer affirmatively are further asked the type of places that they usually go to for care. We categorize these usual care sites as a physician’s office, a hospital outpatient clinic, a clinic or health center, an ED, and other places.
Contextual Factor: Community Characteristics
Our study includes supply and demand sides of the community contextual factors. The proxies for the available mental health care resources (the supply side) include the number of community mental health institutions and number of psychiatrists per 1,000 people at the county level. We control for percentages of the population who are foreign-born, are non-White, or have a college or higher degree, as well as the average community per capita income as proxies for the community demand factors. (Cook et al., 2013).
Other Independent Variables
Guided by the Andersen model of health services use and the conceptual framework developed in the patient activation literature (Andersen, 1968, 1995; Handy et al., 2002; Handy et al., 2005; Hibbard et al., 2005), we include the following population characteristics in our estimation model as well: age, sex, race/ethnicity, marital status, family size, education, income, health insurance (private coverage, uninsured, Medicare, Medicaid, or other public insurance), interview language, self-reported health status, and chronic diseases in addition to depression.
Analyses
We first summarize the sample characteristics and present the contextual factor measures by different levels of patient activation. Multivariable linear regressions are used to estimate the association between contextual factors and the patient activation index, controlling for all the listed covariates. Model 1 controls for the site of care; Model 2 controls for community characteristics; and Model 3 controls for both site of care and community characteristics. Our analyses use survey weights to generate nationally representative estimates. The survey weights adjust for the nonresponse rates based on age, gender, race and ethnicity, and education (Strouse et al., 2009). Detailed survey-weights calculations are discussed in the methodological report of the survey (Strouse et al., 2009).
Our data set includes 2,044 patients with self-reported depression. Among these respondents, 1,686 have valid measures of patient activation. We exclude respondents who reported “not applicable,” “don’t know,” or “refused” on more than 7 (out of 13) patient activation questions, and respondents who replied “strongly agree” or “strongly disagree” on all 13 patient activation questions (Hibbard & Cunningham, 2008). After dropping observations with missing values of other covariates, our final sample includes 1,670 adults age 18 years and older with a diagnosis of depression. Approval for the study was obtained from the institutional review board.
Results
Table 1 shows the summary statistics of patients with depression. The average score of activation among patients with depression is 72, significantly lower than that found in studies of the general population (Hibbard & Cunningham, 2008). The likelihood of strongly agree/agree with each of the 13 items ranged from 0.64, maintaining lifestyle changes under stress, to 0.95, doing follow-up treatment at home. The majority of the depressed patients in the sample are White, female, married, and have other chronic diseases, such as hypertension, arthritis, or diabetes.
Sample Statistics: Individuals with Diagnosed Depression (aged 18 and above; n = 1,670).
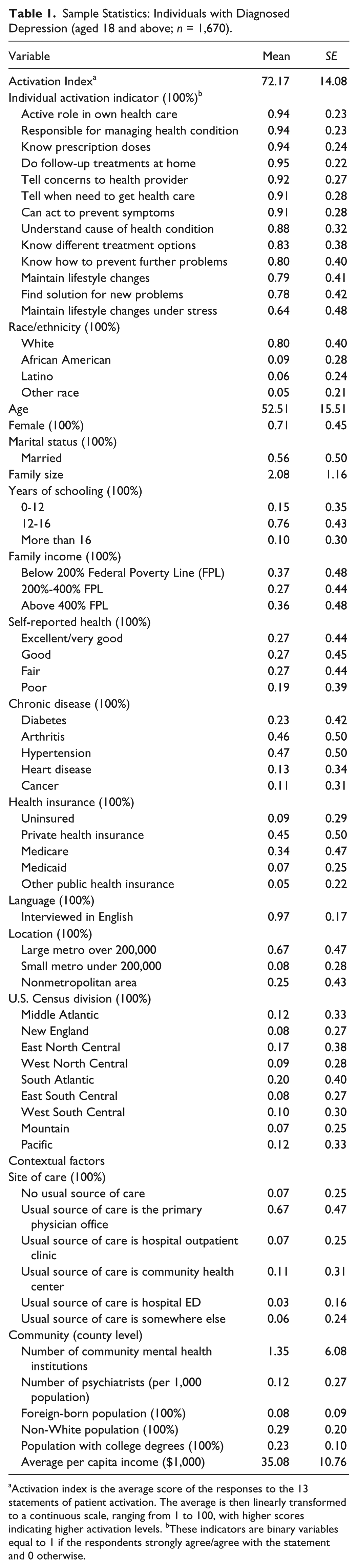
Activation index is the average score of the responses to the 13 statements of patient activation. The average is then linearly transformed to a continuous scale, ranging from 1 to 100, with higher scores indicating higher activation levels. bThese indicators are binary variables equal to 1 if the respondents strongly agree/agree with the statement and 0 otherwise.
Usual source of care in a physician’s office (67%, n = 1,117) is most common, followed by community health center (11%, n = 179), hospital outpatient clinic (7%, n = 111), somewhere else (6%, n = 101), and ED (3%, n = 43). Seven percent (n = 111) of patients report no usual source of care. On average, there are 1.4 community mental health institutions in each county and 12 psychiatrists per 10,000 population. The average percentages of foreign-born populations and non-Whites are 8% and 29% at the county level, respectively. On average, 23% of the population at the county level have college degrees or higher. The average per capita income is $35,000 at the county level.
Figure 2 shows the averages of contextual factors by 4 quantiles of the patient activation index. The first quantile, the lowest 25% of the patient activation index, ranges from 0 to 63.89, the second quantile, 25% to 50% of the index, ranges from 63.89 to 69.23 and so on. Results show that the available mental health care resources (i.e., the number of community mental health institutions and number of psychiatrists) are the lowest at the first (i.e., the lowest) quantile of patient activation index. In addition, the percentages of foreign-born populations and non-White populations are the highest in the first quantile. The percentages of populations with college or higher degrees and average per capita income were also the lowest in the first quantile.
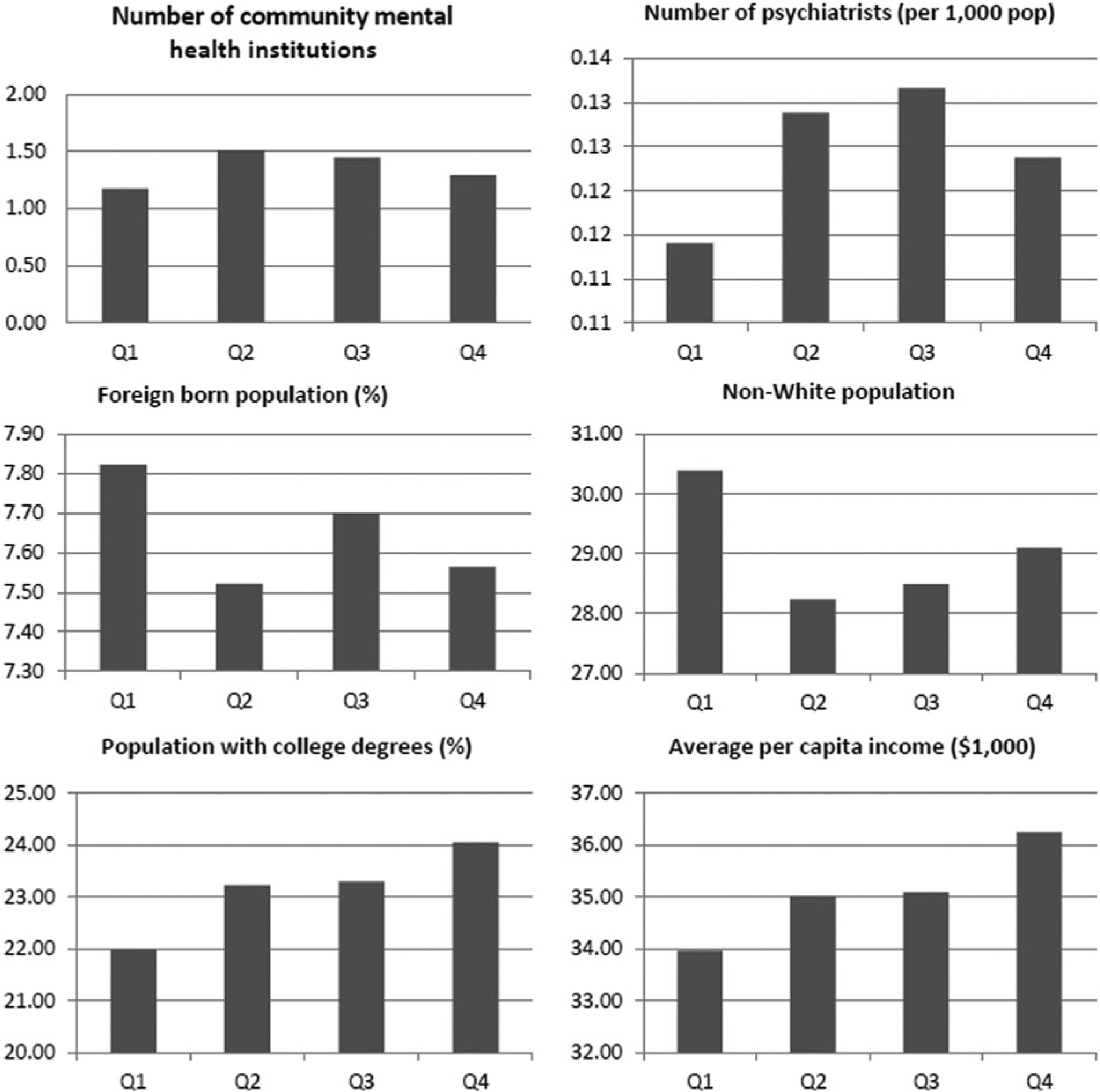
Averages of contextual factors at different ranges of patient activation index.
Table 2 shows the results for the multivariable linear regression with the continuous patient activation index as the outcome variable. Model 1 controls for the site of care. Model 2 controls for the community contextual factors, and Model 3 controls for both contextual factor measures. Models 1-3 also control for the covariates presented above. Results consistently show that compared to patients using physician’s offices as their usual source of care, patients using hospital outpatient clinics (coef = −3.59, p < .05, Model 3) or EDs (coef = −5.04, p < .05, Model 3) have a significantly lower activation index. The differences in patient activation in clinic health centers and physician offices are not significant in both Model 1 and Model 3.
Multivariable Regression: Factors Associated With Activation Index Among Patients With Depressiona.
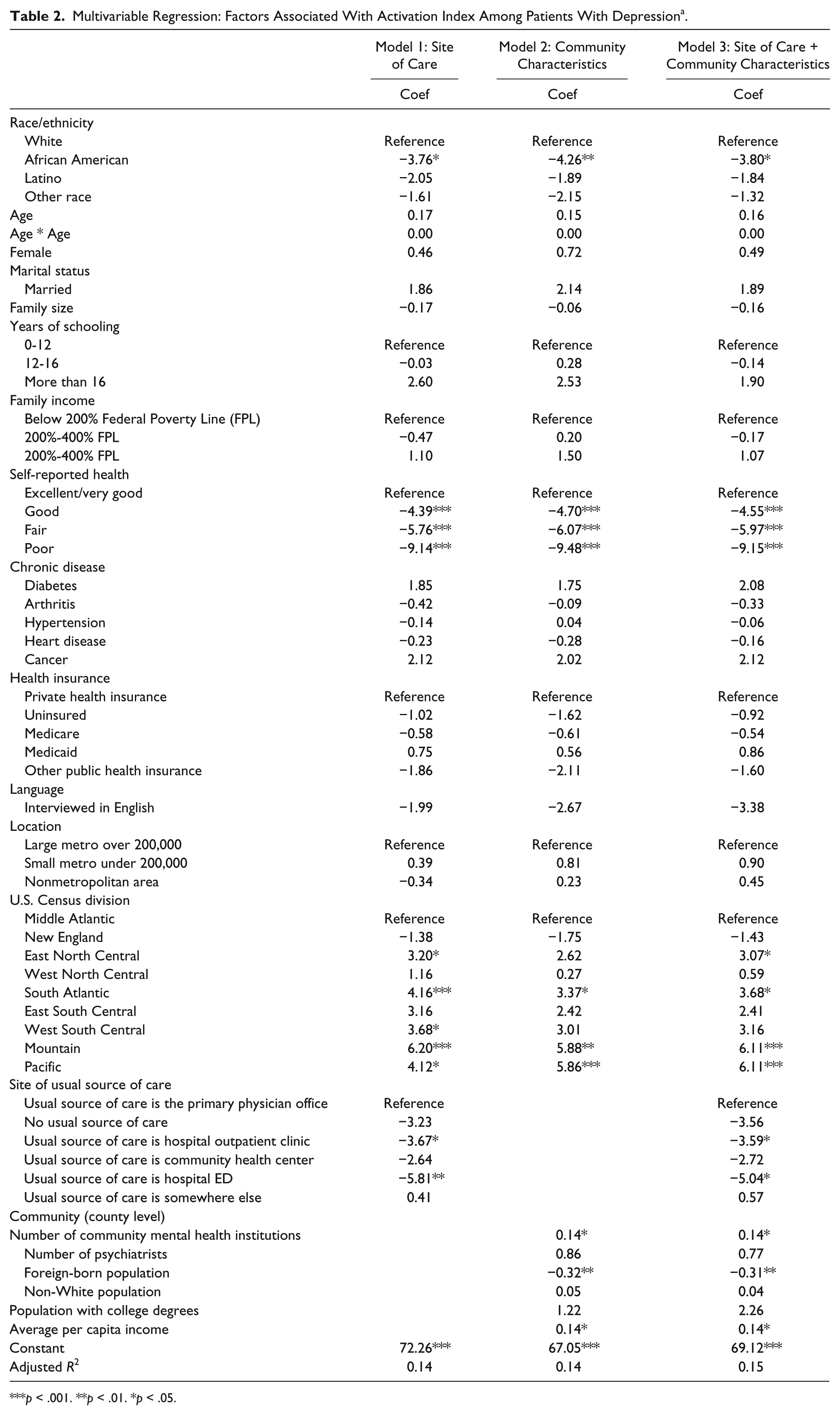
p < .001. **p < .01. *p < .05.
At the county level, more community mental health institutions (coef = 0.14, p < .05, Model 3), lower percentages of foreign-born populations (coef = −0.31, p < .01, Model 3), and higher per capita income (coef = 0.14, p < .05, Model 3) are associated with higher activation scores in both Model 2 and Model 3.
Among the covariates, race and ethnicity, self-reported health status, and U.S. Census Division are the only three categories significantly associated with patient activation index in our multivariable regression models. The activation index is not significantly associated with individual health insurance coverage, family income, or education, after controlling for other covariates.
Discussion
Among patients with mental disorders, patient engagement and self-management can significantly improve treatment compliance, which leads to better quality of life. Contextual factors, that is, the places and environment where consumers receive health care, have been shown as important predictors for health care utilization. To our knowledge, this is the first study that identifies the association of contextual factors and patient activation among patients diagnosed with depression, using a nationally representative data set.
Contextual Factor: Site of Care
Depressed patients who report a physician’s office or community clinic as their usual source of care have higher activation measures compared to those who report hospital outpatient clinics or the ED. Maintaining a continuous relationship with a regular physician is associated with patients’ willingness to share their concerns with their physicians and patients’ knowledge of their health conditions. Continuity provides an environment that improves communication, trust, and a sustained sense of responsibility (Haggerty et al., 2003). Additionally, primary health care can also coordinate health care in a cost effective approach (SAMHSA-HRSA, 2013).
Our results also show that patient activation in a community health center setting is comparable to that of a physician’s office. Community health centers usually serve as a safety net for vulnerable populations in the United States, such as low-income racial and ethnic minorities (Shi, Stevens, Wulu, Politzer, & Xu, 2004). Since minority patients report significantly lower activation, community health centers face challenges to maintain quality care and encourage patient activation. On the other hand, these centers are more likely to provide culturally competent care for underserved populations, and patients may be more likely to be engaged (Forrest & Whelan, 2000). Our finding is consistent with the literature that the quality of care received for treatment of chronic conditions in community health centers is comparable to that received in a physician’s office.
Contextual Factors: Community Characteristics
Community characteristics are significantly associated with patient activation. Our results show evidence that patient activation should be highly encouraged in communities with high ratios of foreign-born individuals. This finding is consistent with previous evidence of lower patient activation among immigrants (Cunningham et al., 2011). Policy should target these communities and design culturally competent health care to engage immigrants in their own health. These policies are critical given the rapid population growth rates of immigrants. Educational programs advocating patient activation among these groups might be effective (Hibbard et al., 2008). Results also show that average income of the neighborhood is positively associated with patient activation. This finding is consistent with evidence showing that neighborhood income has a positive effect on residents’ long-term well-being (Chow, Jaffee, & Snowden, 2003; Greenberg et al., 2013; Gresenz, Stockdale, & Wells, 2000).
The role of the place is critical in health care. Health care resources are considered a “community-level enabling variable” (Phillips, Morrison, Andersen, & Aday, 1998), a critical component of health care utilization (Dinwiddie et al., 2013; Gaskin et al., 2012a, 2012b). We find that the number of community mental institutions positively relates to higher patient activation. This finding may suggest that the community and primary care are critical to engage patients with mental disorders in their own health and health care. Our results also suggest that policy interventions targeting specific regions are needed, and such strategies can be effective to improve patient activation. The insignificant relationship of the supply of psychiatrists is consistent with the literature, which shows a weak relationship between the density of psychiatrists and psychologists on mental health care utilization (Gresenz et al., 2000; Stockdale, Tang, Zhang, Belin, & Wells, 2007).
It is worth noting the role of place in mental health care disparities (Gaskin et al., 2012a, 2012b). Residential segregation, for example, has been shown as a critical predictor for health services utilization (Gaskin et al., 2012a, 2012b; Lee, 2009; Park & Iceland, 2011; White et al., 2012; Williams et al., 2012). Although our study does not focus on residential segregation due to data limitations, future research should explore whether segregation relates to racial and ethnic disparities in activation.
Our study has several limitations. First, our study uses a cross-sectional design, which limits analysis of the causal relationship of contextual factors with the patient activation. Although we have tried to control as many factors associated with patient activation as shown in the literature and are available in our data set, unobserved factors related to patient activation, such as the availability of mental health care institutions, might have been omitted. Second, our results only apply to patients who have been diagnosed with depression. Since depression is highly underdiagnosed and undertreated, the activation levels among patients already diagnosed may have been overestimated. Third, since most of the respondents are interviewed in English, our study cannot accurately estimate the association between English proficiency and activation. Fourth, contextual factors are measured at the county level given the restrictions of our data set. It is likely that zip code or other sub-county level measures can reflect better community characteristics.
Implications for Policy
Patient activation has the potential to achieve the “triple aim” of reduced health care cost, improved health, and efficiency of the health care system. Improving patient activation has been enforced under major provisions of the Affordable Care Act, such as patient-centered medical homes and Accountable Care Organizations. Patients with mental disorders are less activated compared to patients with other chronic diseases. More important, mental disorders are comorbid with other chronic diseases. Low activation due to mental disorders can affect the efficiency of treatment of other comorbidities. Our study shows evidence of the importance of contextual factors related to patient activation among people with mental disorders.
Our study suggests that primary care setting is critical to having a sustained relationship between patients and physicians to engage patients in mental health care. Improving patient activation in hospital outpatient clinics and EDs is also critical. Physicians should assess symptoms of depression, even when depression is not the primary diagnosis. However, improving patient activation at hospital outpatient clinics and EDs can be a challenge, since individuals accessing primary care at these sites might be less active in the first place.
Community contextual factors, such as the availability of community mental health care institutions, are critical to encourage patients to play an active role in their own health care. Our findings suggest that interventions in communities with lower levels of income and high immigrant populations are necessary. Tailored policies targeted at such communities can be cost effective to engage residents in their own health, improving long-term well-being and reducing health disparities.
In sum, our results show evidence that the integration of primary care and behavioral health services can better address individual mental health needs. Tailored strategies work more effectively to promote patient activation by addressing the health care needs and preferences of the individuals and communities. These findings support the integrated care model advocated by SAMHSA-HRSA (SAMHSA, 2013).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.