
Abstract
Background. Community collaboratives provide a means to build local capacity, reduce service fragmentation and duplication, maximize efficiency, and create synergies for systems change. But what are the collaborative practices that aging services providers and other stakeholders employ for system change and impact in evidence-based programming for older adults? Purpose. The aim of this study was to learn how aging and health collaborations created strategic partnerships to foster multisector systems change and pursue long-term goals and near-term activities to sustain and expand evidence-based health programming. Methods. Via a multiphase process, we identified eight geographically diverse, exemplar agencies that serve as the coordinators for various community collaborations. Using an interview protocol culled from the literature, we conducted on-site, in-depth interviews with leadership and partners. Results. Four creative strategies emerged across sites as contributing to the growth and sustainability of evidence-based health programming including engagement of nontraditional partners, development of new relationships with health care, building of innovative systems of structures and tools, and systematically working with vulnerable populations. Opportunities for future initiatives include enhancing linkages with health care, advocating for the value of evidence-based programming, supporting local program development and adaptation, and developing marketing strategies and business models. Conclusion. These eight organizations are leveraging their historic strengths and newly acquired expertise to extend health programming beyond established partners and funding silos. The four strategies and specific activities reflected in their work have laid a solid foundation for expanding and embedding future initiatives and positively impacting the health of older adults.
The increase in the proportion of older adults in the population (U.S. Census Bureau, 2008, 2010), combined with their burden of chronic conditions and age-associated geriatric syndromes (Centers for Disease Control and Prevention, 2012), has created a major challenge for aging services providers and their public health and health care partners in supporting older adult independence and engagement. Evidence-based or best practice health promotion programs offer a vehicle to deliver high-quality, tested programs at the community level to address these challenges and to promote healthy aging (Administration on Aging, n.d.). Unfortunately, such programs are not being adopted as widely as needed, resulting in fragmented and uneven program delivery (Center for the Advancement of Health, 2006). While there is a compelling need for accelerating the systematic uptake of health promotion programming, achieving widespread scaling cannot be accomplished through the efforts of largely autonomous organizations. Rather, organizations need to work in nontraditional ways, coordinating health care from multidisciplinary perspectives to extend beyond autonomous initiatives, and transcend the constraints that silos of funding can produce. Calling for a new approach focusing on collective impact, Crutchfield and McLeod-Grant (2012) contend that nonprofit organizations must mobilize their forces beyond their four walls to end isolation and systematically employ multisector, collaborative approaches.
Community collaboratives, defined as cross-sector alliances working together for a common aim, are emerging to address complex community health issues (Roussos & Fawcett, 2000). Such collaborations provide a means to build community capacity, reduce fragmentation and duplication in services, maximize the efficient use of resources, and ultimately, create synergies for systems change (Emshoff et al., 2007). Systems change is defined here as the intent to transform how community members rearrange the ways stakeholders interact with each other to coordinate care and manage financial resources (Scheirer, 2013). But how can the field of aging and health services galvanize their efforts with other community stakeholders to create such impact on practices, programs, and policies targeting older adult health?
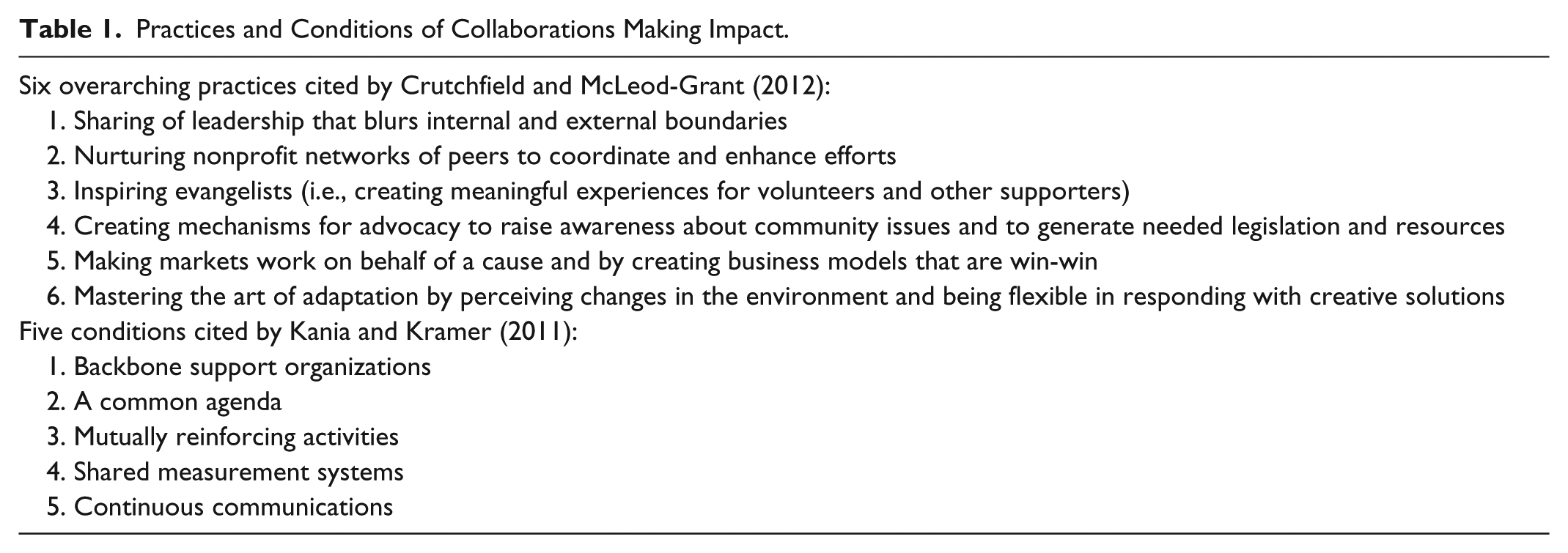
Drawing from the literature, we highlight in Table 1 the interrelated practices and conditions for creating and operating successful community-based collaboratives. In their research, Crutchfield and McLeod-Grant (2012) observed six overarching practices that blur boundaries to share leadership, coordinate efforts, inspire advocates and supporters, and maintain flexibility and adaptability in responding to external factors. Kania and Kramer (2011) enumerate five conditions to produce collective impact that emphasize the importance of a “backbone” organizations, that is organizations that take the lead to foster and coordinate mutuality in agendas, activities, measurement systems, and continuous communications. These overlapping constructs have been illustrated using various multisector collaborations addressing a range of community health and social issues; however, our review of the literature revealed no research or commentary featuring collaborations focusing on older adult health.
Practices and Conditions of Collaborations Making Impact.
Study Aims
To determine which of these collaborative practices are employed by advocates for systems change and impact in evidence-based programming for older adults, the National Council on Aging (NCOA) contracted with the University of North Carolina at Chapel Hill (UNC) to design and implement a multiphased evaluation of NCOA’s initiatives on self-management of chronic conditions. The goal of the study was to learn how evidence-based program collaborations created and leveraged their successes. Specific study aims were to identify (1) successful backbone or coordinating organizations and the types of multisector collaborations they fostered; (2) the strategies used to increase capacity both internally and externally across multiple sectors; (3) collaborative structures and engagement of the population; and (4) areas needing attention by funders, policy makers, and support organizations to further advance aging and health initiatives. This article summarizes our study process, tools, and findings.
Research Design and Methods
During the first phase of the study, the UNC/NCOA team planned an overall strategy to identify and report on exemplary regional- and community-level initiatives carrying out evidence-based programming for older adults. We conducted telephone interviews with 11 key informants using a 6-item telephone protocol with probes. Informants were selected based on representation from various sectors (e.g., federal and state government, philanthropy, national associations, regional/local health and aging services organizations), and their innovative leadership in the evidence-based program movement as identified by the NCOA staff. We asked these 11 informants to identify people who have been leaders in carrying out and supporting evidence-based health programming and why they are important to interview. The resulting list included key individuals from many sectors, but for this study we identified more than 40 people or organizations that were reported as being especially “successful” in leading evidence-based program collaborations.
To this list, we applied criteria at two levels. First, we selected organizations that were leading collaboratives that had experience with multiple evidence-based programs. Second, we sought diversity in: geographic location in the United States; organizational type (public and nonprofit; area agency on aging [AAA] and not an AAA); size of service area; population concentration of service area; and race and ethnicity of populations served. Using these criteria, we identified eight diverse agencies that serve as the coordinator for community collaborations. These eight agencies and their collaboratives are exemplars. During the course of this study, we learned that there are many other organizations across the nation leading similar community collaborations.
As we identified these agencies, we also reviewed the literature on successful community collaborations to understand the interplay of contextual factors and collaborative processes, and the types of systems changes achieved (e.g., shared decision making, shared financing, coordinated service delivery). Selected organizations who participated in site visits are listed in Table 2. The table also lists the Tier One evidence-based health promotion programs for older adults that were being delivered by each collaboration at the time of the study; some sites offered other health promotion programs not on Administration on Aging Tier One list. Tier One programs meet the most rigorous standards of criteria for level of evidence and capability for translation into the community, as designated by the Administration on Aging for its Title IIID Disease Prevention and Health Promotion Services. As a quality assurance strategy, the Administration on Aging goal is to move all Title IIID funded activities to the Tier One level (Administration on Aging, 2013). These organizations invited an array of collaborating partners to the site visit, including university research centers, various community-based aging and social service agencies, multicultural services, clinics, hospitals and health care systems, health insurers and quality improvement organizations, county health departments, state agencies, aging and disability resource centers, community advocacy groups, local YMCAs, and a cable television station.
Participating Study Sites and Tier One Evidence-Based Health Promotion Programs Offered.
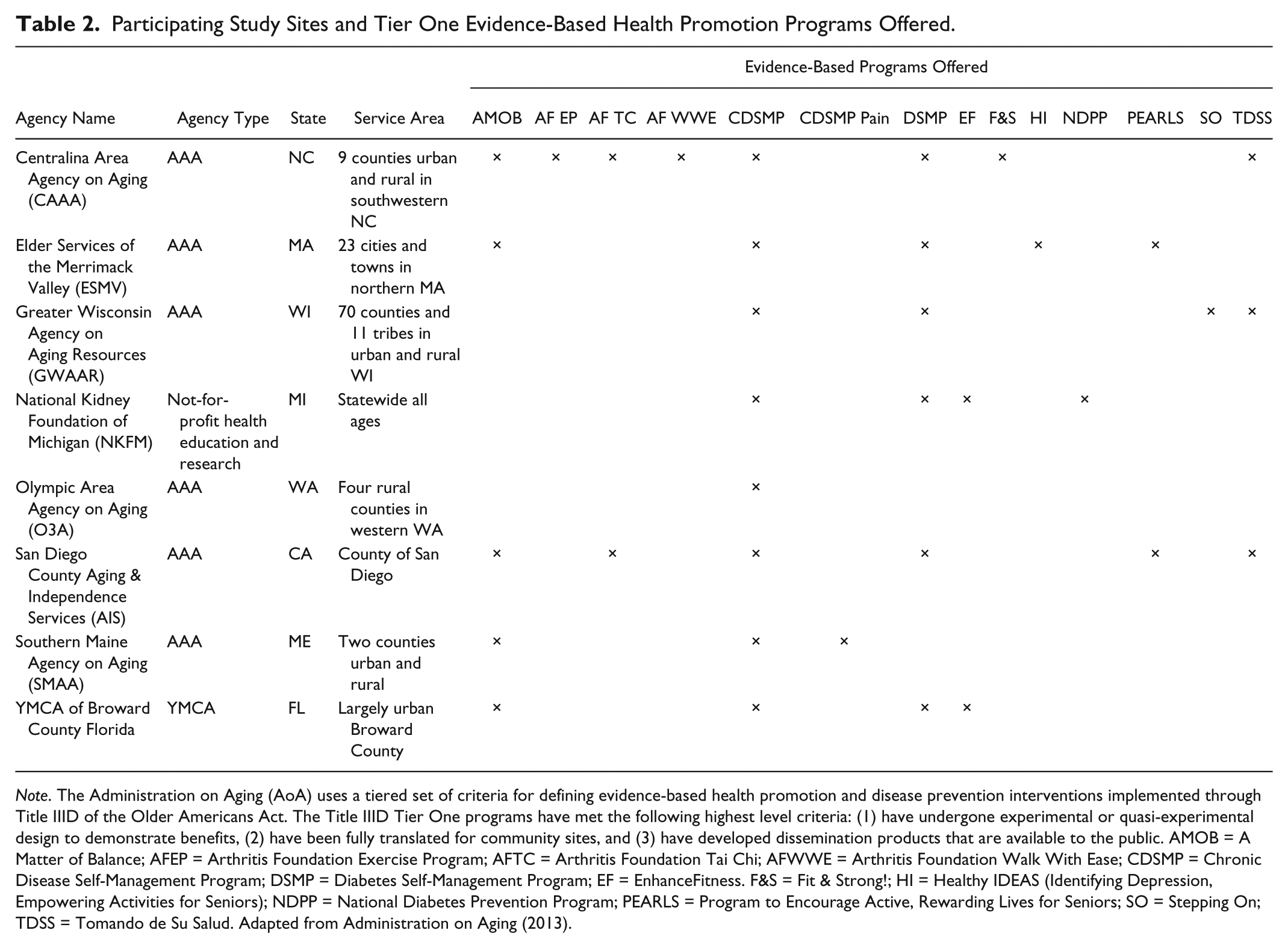
Note. The Administration on Aging (AoA) uses a tiered set of criteria for defining evidence-based health promotion and disease prevention interventions implemented through Title IIID of the Older Americans Act. The Title IIID Tier One programs have met the following highest level criteria: (1) have undergone experimental or quasi-experimental design to demonstrate benefits, (2) have been fully translated for community sites, and (3) have developed dissemination products that are available to the public. AMOB = A Matter of Balance; AFEP = Arthritis Foundation Exercise Program; AFTC = Arthritis Foundation Tai Chi; AFWWE = Arthritis Foundation Walk With Ease; CDSMP = Chronic Disease Self-Management Program; DSMP = Diabetes Self-Management Program; EF = EnhanceFitness. F&S = Fit & Strong!; HI = Healthy IDEAS (Identifying Depression, Empowering Activities for Seniors); NDPP = National Diabetes Prevention Program; PEARLS = Program to Encourage Active, Rewarding Lives for Seniors; SO = Stepping On; TDSS = Tomando de Su Salud. Adapted from Administration on Aging (2013).
As noted in Supplemental Table 1 (available online at heb.sagepub.com/supplemental), we created a site visit interview protocol integrating the factors, conditions and practices we noted in the literature, arrayed by the six domains identified by Crutchfield and McLeod-Grant, and including components of the RE-AIM framework (EFFECTIVENESS, ADOPTION, MAINTENANCE) that were most relevant to the interview focus (http://www.re-aim.org/). An additional domain was added to gather sites’ recommendations to support future success.
For the next phase of the study, our NCOA/UNC team scheduled one-day site visits with staff and collaborating partners. Prior to each site visit, we conducted conference calls with site leadership to discuss visit logistics (e.g., meeting duration, attendees, and materials to provide) and sent the interview protocol for their review. All eight sites agreed to participate. Two or more study team members participated in each site visit with one member serving as the lead interviewer. All study team members kept detailed notes which were later merged into summary reports and analyzed for cross-cutting themes and examples of collaborative practices. Each organization received a summary of findings for their specific site as well as the entire final project report. Findings were reviewed and validated by the site leads.
Results
Strategies for Growth and Sustainability
As expected, each site and its partners had a unique approach to building successful collaborations. Nevertheless, four creative strategies emerged across sites as transforming the growth and sustainability of evidence-based health programming, using a mix of science, grounded experience, advocacy, intentionally leveraging partnerships and successes, and steadfast commitment to impact. The four strategies are
Expanding program delivery networks beyond the aging services network
Creating mutually beneficial partnerships with health care
Building systems of structures and tools to support program expansion and culture change to make permanent impacts
Systematically engaging and empowering vulnerable populations.
We collected many site-specific examples for these strategies; however, we have selected only a few for illustrative purposes. Our intent was not to quantify the strength or variations of each strategy per site, but rather, to summarize overarching strategies that appear to be cross-cutting and feasible regardless of varying site contexts, processes, and resources.
Expanding Program Delivery Networks Beyond the Aging Services Network
To increase their reach and promote systems change, sites have developed new collaborations that extend beyond their established aging services partners. Elder Services of the Merrimack Valley (ESMV) created successful collaborations with nontraditional partners by highlighting mutual agendas and desired outcomes; building trust through systematic relationship building; and delivering on promises. ESMV launched the statewide Massachusetts State Disease Management Coalition to provide seed money to partnerships with the aim of aligning efforts in self-management programming. Initially, 13 organizations participated in one coalition, including Hebrew Senior Life, the largest provider of elder care (including health care, housing, and research) in the Boston area. ESMV has considerably expanded the model to provide technical assistance, support and activity coordination to six regional coalitions spanning the state.
We also found that regional foundations with missions broader than a healthy aging focus were instrumental in expanding delivery of evidence-based programs for the older adult population. For example, the National Kidney Foundation of Michigan (NKFM) is empowering and engaging diverse communities to improve health through evidence-based programs, and their partnering communities have expressed confidence that the foundation “is there for the long haul” after grant periods end. The YMCA of Broward County, Florida credits much of its success to the support and engagement of the Health Foundation of South Florida. The Health Foundation is taking a leadership role through its Healthy Aging Regional Collaborative in three southern Florida counties to build a sustainable infrastructure that can support the delivery of evidence-based programs to promote health and prevent disease and to work with grantees to improve organizational effectiveness and efficiency.
Creating Mutually Beneficial Partnerships With Health Care
The study sites reported a variety of ways they are engaging health care partners to expand their capacity to offer evidence-based programs and to uncover new public and private funding mechanisms. Working with MaineHealth, the largest health system in the state, the Southern Maine Agency on Aging is a founding partner of the Partnership for Healthy Aging, a nonprofit organization that enables the members to access data, extend capacity, and develop innovative approaches that strengthen and broaden health care collaborations. The Southern Maine Agency on Aging also embeds their own care managers within medical practices of health care organizations with the aim of enhancing the quality of medical care, coordinating services, and streamlining referrals to community-based health programming and community care. As a result of this embedding “organizations aren’t trying to go it alone now.”
ESMV has a long-standing relationship and shares staffing with Hebrew Senior Life, an organization providing health care and housing services. This mutually beneficial relationship has blurred organizational boundaries enabling ESMV to pursue funding opportunities for transitions in care, service coordination for medical homes, and reimbursement from Medicare for Stanford University’s Diabetes Self-Management Program. ESMV and Hebrew Senior Life also co-created and share leadership for the “Healthy Living Center of Excellence” to promote the integration of evidence-based health programs held in diverse community settings within the health care delivery system. One goal of this collaboration is providing “one stop shopping” for insurance companies to offer evidence-based programs to their members.
San Diego County Aging & Independence Services (AIS) “elevated its presence with the health care community” by presenting its work at a prestigious medical symposium in California. This led to AIS working with Sharp Rees-Stealy Medical Group (Sharp), an independent physician’s association, to offer evidence-based health promotion programs such as the Stanford Chronic Disease Self-Management Program. Sharp trains and pays its own employees to lead the program and allows AIS to recruit Sharp patients to attend the workshops.
Centralina Area Agency on Aging (CAAA) has built a strong partnership with Community Care Partners of Greater Mecklenburg, a network of more than 150 providers serving Medicaid enrollees. In an effort to gauge program impact, Community Care Partners is creating measurement and monitoring systems of evidence-based program participants to determine if they have fewer hospital readmissions and better health behaviors and outcomes. The organization also provides financial support to CAAA.
Building Systems of Structures and Tools to Support Program Expansion
All sites are employing a variety of innovative tools, resources, and processes to develop and sustain their healthy aging programming infrastructure and, in some cases, are applying these innovations to other program areas. For example, using a well-developed business model to drive network expansion, the YMCA of Broward County manages the logistics of program delivery in exchange for space and other facility services while participant fees accrue to the YMCA. This model of programming and financing has become a template for other YMCA programs and has spawned growth in programs targeted for middle-aged adults.
The Greater Wisconsin Agency on Aging Resources (GWAAR) facilitates connections between university researchers and community-based organizations through a structure called the Community Academic Aging Research Network. This GWAAR/Aging Research partnership allows the aging network to “better understand research and its benefits,” and helps accelerate program implementation and adaptations. This partnership assists in accelerating research to practice translation of healthy aging programming into community implementation. Additionally, GWAAR has created and implemented quality improvement processes and tools that are used throughout its networks.
To streamline coordination, increase fidelity, and track leaders and volunteers across their expansive network, CAAA created a comprehensive database and tracking system that has proven to be not only an effective marketing tool for engaging new partners, but also central to sustaining quality in how programs are planned, monitored and delivered. CAAA tells potential partners that they “just need to recruit people for the classes, and we will take care of everything else.” This database and strong infrastructure has allowed CAAA to support more than 200 trainers and leaders. Approximately 40% of their leaders are volunteers, and turnover is low; CAAA attributes this to their solid administrative support and robust infrastructure.
Olympic Area Agency on Aging serves a large, primarily rural service area that extends over the Olympic Peninsula and the entire length of Washington’s west coast. Olympic Area Agency on Aging has addressed the challenges of a dispersed population by establishing an organizational structure with 7 offices and 75 staff in its various geographic areas. They have inventively used print, radio and cable television programming to engage populations and market evidence-based community programming.
Systematically Engaging and Supporting Meaningful Involvement of Vulnerable Populations
Each of the sites was responsive to the demographics of its region by such efforts as being attentive to the growth of ethnic populations, reaching out to rural residents, and promoting programs to tribes. The NKFM focuses much of its programming on advocacy for diverse populations, particularly the African American community where kidney disease is more prevalent. Using a “population health” model that includes an aging focus, NKFM supports staffing and resources to leverage multisector coalitions in at-risk communities. These coalitions are comprised of minority-based organizations, businesses, community agencies, advocacy groups, local government, educational institutions, housing developments and others. Part of NKFM’s success is to “have people understand that they are part of something much bigger than the work of their own agencies—you aren’t an island doing the programs.”
Other study sites have extended their reach into the minority community by a variety of approaches. The San Diego County Aging & Independence Services partnership with Elder Multicultural Access and Support Services at the Union of Pan Asian Communities not only has extended reach to Asian, Arabic, African-American, and Hispanic elder populations, but it has also spawned grassroots ethnic-specific community initiatives to address older adult health and well-being. Olympic Area Agency on Aging emphasizes “working locally” with rural communities and nine federally recognized tribes to tailor programming for an integrated rural health system. Additionally, the YMCA of Broward County is working to meet the needs of its county’s diverse population by offering evidence-based programs in both English and Spanish for older adults at more than 30 sites.
Needs and Opportunities for Sustainment, Growth, and Advocacy
The eight sites were asked to provide input on what would be needed to sustain and expand their evidence-based programming. Sites identified the need for further attention to the following areas:
Enhance and institutionalize linkages with the health care system. Sites repeatedly said they needed assistance in developing, testing and disseminating effective referral systems between health care and community-based organizations, identifying and engaging physician champions to promote evidence-based programs and community partnerships, and creating and testing a common language and tools for marketing and communication.
Advocate for the importance of community-based evidence-based programming. Sites consistently stated the importance of educating stakeholders such as older adults and health care providers and insurers on the value of self-management, program benefits, and related cost savings. They sought help in providing updated, accurate and compelling data about older adult health issues and outcomes for evidence-based programs and in generating common data forms and/or web-based systems of program data entry. Additionally, they asked federal agencies, such as the Administration on Community Living, professional associations, and other national nonprofit organizations to focus their advocacy efforts for evidence-based health programming with other service systems, such as the Veteran’s Administration, Federally Qualified Health Centers, Centers for Medicare & Medicaid Services, prison systems, and university extension services.
Develop and share marketing strategies and business models. Sites proposed new initiatives focused on creating effective business models, understanding how other organizations are successfully partnering with health care, and providing opportunities to share effective strategies for promoting and disseminating evidence-based programs. Such capacity building might take the form of leadership development, shared learning networks, and/or consultation.
Support organic development and adaptation of evidence-based programming. As a way to keep evidence-based programming “vibrant and evolving,” sites requested assistance in accessing the best evidence, supporting flexibility in selecting and implementing health programming, and obtaining research support to conduct formative evaluation to tailor interventions to population needs and “make adaptation happen quickly.” Several sites advocated for new initiatives to address cultural differences and advance their efforts in working with diverse populations.
Discussion
This study addresses the gap in knowledge about how aging and health care organizations are innovatively fostering collaborations and shaping their successes. Key limitations of this study are the small number of study sites and the focus only on cross-cutting successes and not on variations in success or challenges. We note that the Centers for Disease Control and Prevention’s Principles of Community Engagement (2011) aligns the principles of engagement along a continuum—prior to beginning engagement, what is necessary for engagement to occur and what to consider for engagement to be successful over the long run, and provide concrete guidance for all parties involved about the “do’s” for creating effective collaborative activities. Hence, future research should compare variations in successful and less successful sites and also examine the temporal components of successful collaboration.
We found that these eight organizations are leveraging their historic strengths and newly acquired expertise to extend health programming outside their established partners and silos of funding, laying a foundation for expanding and embedding future initiatives. The four strategies and specific activities reflected in their work overlap with those components believed to produce successful collaborations and collective impact. For example, each site, to varying degrees, is addressing the fundamental conditions cited by Kania and Kramer (2011), by serving as a supportive backbone organization in establishing regional- or state-level multisector partnerships, setting mutual agendas, coordinating activities, and creating measurement systems. At the same time, each is carrying out many of the practices noted by Crutchfield and McLeod-Grant (2012) by sharing leadership, blurring organizational boundaries, nurturing networks and local level capacity, and advocating for and generating the resources needed to support programming. In these sites, at-risk populations were being encouraged and supported to address health issues within their own communities, which also provided opportunities for volunteers and other supporters to contribute significantly to community needs.
Moreover, these organizations provided insights into areas needing attention to sustain, grow, and advocate for evidence-based programming. Enhancing institutional linkages with the health care system, advocating for the importance of evidence-based programming, building marketing strategies and business models, and accelerating adaptation of evidence-based programming are all areas that policy-makers and funders could support to continue the systems change movement. However, we note that additional conditions beyond those enumerated by Kania and Kramer are needed to continue to support change within health programming for older adults into the future. The sites emphasized that successful systems change goes well beyond simply delivering programs; this effort requires considerable time, flexibility, and resources to engage nontraditional partners, develop new relationships with health care, build innovative systems of structures and tools, and systematically engage and empower vulnerable populations. Clearly, these organizations (and others like them across the nation) are well poised, moving beyond their four walls to enhance internal and external capacity. Their strategies are driven by local contexts and national priorities and sometimes inhibited by constraints or conditions tied to funding mandates. In these changing economic times, it is increasingly essential for funders and policymakers to support community leadership to be in the forefront of achieving systems change and galvanizing impact with limited resources to advance older adult health, engagement, and independence.
Footnotes
Acknowledgements
The authors wish to thank Dr. Basia Belza and Ms. Kristi Kulinski for their assistance in conducting the site visits and report preparation. We also wish to thank the eight sites and their partners that participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a grant from The Atlantic Philanthropies, Grant Number 14728.
Supplement Issue Note
This article is part of an open access supplement “Fostering Engagement and Independence: Opportunities and Challenges for an Aging Society,” published in SOPHE’s Health Education & Behavior. This supplement was supported by funding provided by the Centers for Disease Control and Prevention’s (CDC) National Center for Chronic Disease Prevention and Health Promotion, Healthy Aging Program (Cooperative Agreement #U38HM000454) via the Association of State and Territorial Health Officials, and from a grant provided by the Retirement Research Foundation. Views presented herein do not represent the official views of the CDC.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.